Microvascular fibular transfer for segmental bone defects and osteonecrosis · advanced
- Blood supply: the fibula is supplied by endosteal and periosteal vessels from the peroneal artery (a branch of the tibioperoneal trunk). Preserving this pedicle keeps the graft living, so it heals by primary bone union rather than creeping substitution.
- Harvest boundaries: preserve the proximal 6–8 cm (to protect the common peroneal nerve, lateral collateral ligament and biceps femoris) and the distal 6–8 cm (to preserve the distal tibiofibular syndesmosis and ankle mortise). Up to about 25 cm of diaphysis is harvestable.
- Protect the perforators: leave a 1–2 mm cuff of flexor hallucis longus (FHL) on the graft to shield the periosteal supply and septocutaneous perforators. Stripping the fibula bare denervates FHL and causes great-toe flexion contracture.
- Indications: large segmental long-bone defects greater than 6 cm (tumour resection, trauma, infection, congenital pseudarthrosis of the tibia) and pre-collapse femoral head osteonecrosis (Ficat/Steinberg I–II).
- The graft hypertrophies with loading (Wolff's law) over 6–18 months. Rigid fixation protects the microvascular anastomosis and promotes union; the Capanna technique (fibula inside an allograft shell) adds immediate stability for massive lower-limb defects.
When & Why
Indication. A free vascularised fibular graft (FVFG) is reserved for situations where a conventional, non-vascularised graft would predictably fail — because the defect is too large, or the recipient bed is poorly vascularised, irradiated, or scarred. It is used to biologically reconstruct segmental long-bone defects and to revascularise the pre-collapse femoral head. The three situations you reach for it:
Long-bone defects greater than 6 cm after intercalary or intra-articular tumour resection, severe open trauma with bone loss, radical debridement for chronic osteomyelitis or infected non-union, and congenital pseudarthrosis of the tibia.
Pre-collapse disease — Ficat/Steinberg Stage I–II, or early Stage III with minimal collapse (less than 2 mm) — typically in patients under 50 years, before the head has collapsed.
Poorly vascularised or irradiated tissue where non-vascularised graft revascularises poorly. The living fibula brings its own blood supply, heals by primary union, and hypertrophies under load.
Why vascularised beats non-vascularised. Because the graft stays living:
- It maintains osteocyte viability and heals by primary bone healing rather than creeping substitution.
- It undergoes rapid hypertrophy in response to mechanical stress (Wolff's law).
- It performs far better in poorly vascularised or irradiated recipient beds.
- It has a lower rate of late stress fracture and resorption. Consent. Counsel donor-site morbidity specifically — great-toe/FHL flexion contracture, common peroneal nerve palsy (foot drop), and ankle instability — and recipient-site risks: flap/anastomosis failure, non-union at the docking sites, and stress fracture of the graft before it hypertrophies. Setup. Supine with a sandbag under the ipsilateral buttock to internally rotate the leg slightly, on a radiolucent table. Exsanguinate and inflate a high thigh tourniquet. The procedure is long and is ideally run with two surgical teams working concurrently — one harvesting the fibula while the other prepares the recipient site — to minimise ischaemia time. Loupe magnification for the harvest; the operating microscope for the anastomosis.
The Operation
The goal is to harvest a length of living fibular diaphysis on its peroneal vascular pedicle, transfer it to the defect, secure it with rigid fixation, and re-establish blood flow by microvascular anastomosis. The lateral-leg exposure and pedicle isolation are the heart of the procedure — every later step depends on a clean, protected harvest.
Operative sequence
- Supine with a sandbag under the ipsilateral buttock to internally rotate the leg slightly; radiolucent table is essential.
- High thigh tourniquet, inflated after exsanguination.
- Two surgical teams work concurrently — one harvests the fibula while the other prepares the recipient site, to minimise ischaemia time.
- Make a longitudinal incision along the lateral aspect of the leg, along the line of the fibula.
- If a monitoring skin paddle is required (or to cover a soft-tissue defect), design it over the posterior intermuscular septum at the posterior border of the fibula to capture the septocutaneous perforators from the peroneal artery.
- Elevate the anterior skin flap and identify the intermuscular septum between the peroneals and the soleus.
- Retract the peroneal muscles anteriorly; identify and protect the superficial peroneal nerve as it exits the lateral compartment in the distal third of the leg.
- Perform an extraperiosteal dissection of the anterior fibula.
- Elevate the posterior skin flap and retract the soleus posteriorly.
- The flexor hallucis longus (FHL) muscle belly lies directly over the posterior fibula and carries the peroneal perforators — it is the key to the deep dissection.
- Measure and mark the required length of fibula, strictly preserving the proximal 6–8 cm (common peroneal nerve, lateral collateral ligament and biceps femoris insertion) and the distal 6–8 cm (distal tibiofibular syndesmosis and lateral malleolus).
- Pass curved retractors subperiosteally at each osteotomy site to protect the deep vessels.
- Cut with an oscillating saw or a Gigli saw.
- Place a bone hook in the proximal fibular segment and apply gentle lateral traction.
- Divide the interosseous membrane from anterior to posterior, roll the fibula laterally, and divide the tibialis posterior muscle.
- Identify the peroneal artery and venae comitantes proximally and distally; ligate the distal peroneal vessels.
- Dissect the FHL off the fibula, leaving a 1–2 mm cuff of muscle attached to protect the periosteal blood supply and the perforators.
- Trace the pedicle proximally to its origin at the tibioperoneal trunk to gain maximal pedicle length, ligating the muscular branches.
- Outside the zone of injury or radiation, isolate a healthy recipient artery and vein with good flow and healthy intima.
- Shape the fibular ends to fit the defect.
- Once the recipient site is ready, ligate the proximal peroneal vessels and note the ischaemia time.
- Flush the graft with heparinised saline if your local protocol requires it, then transfer it to the recipient site.
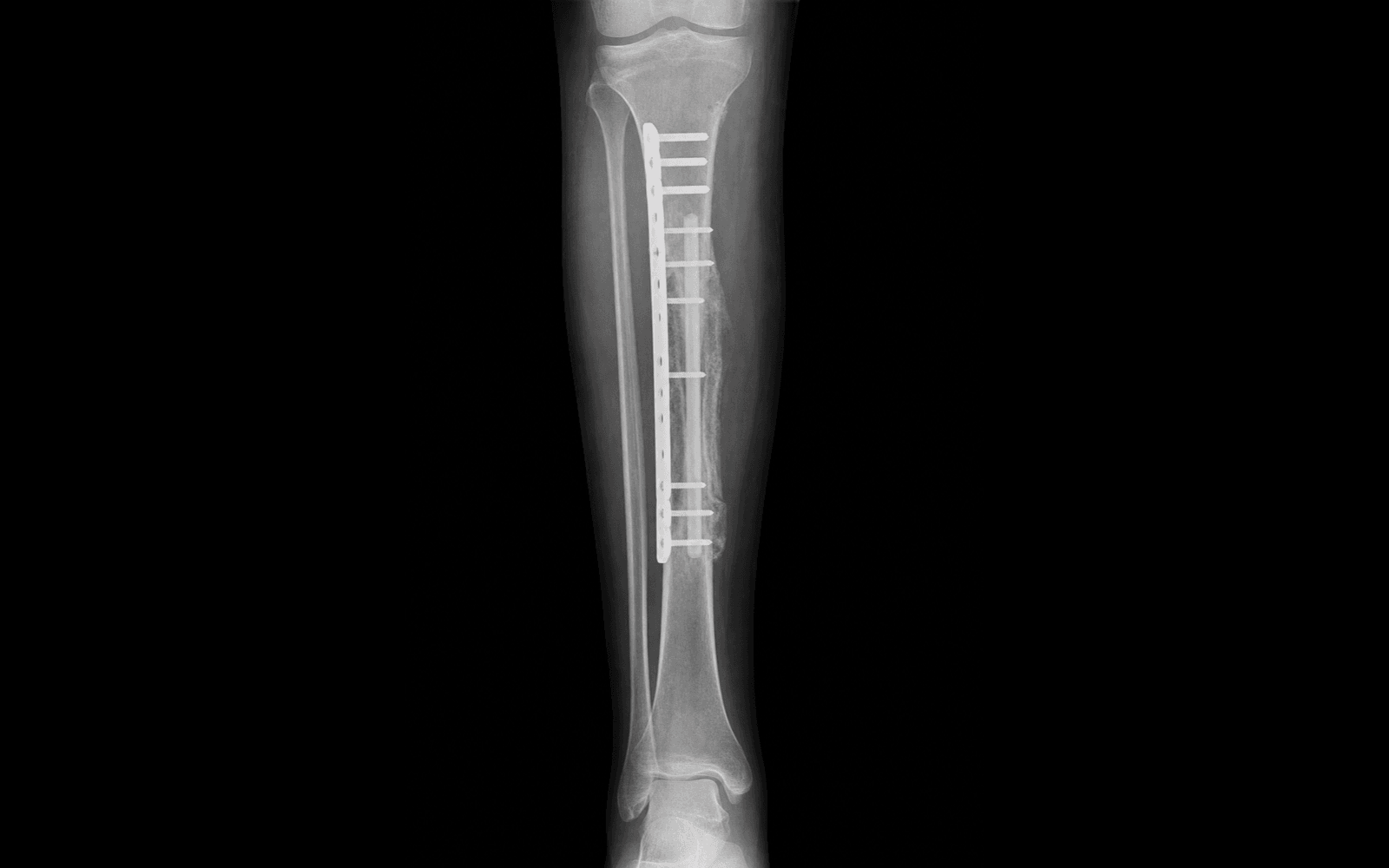
- Inset the graft. Rigid fixation is essential — typically a bridging locking plate or an intramedullary nail — to protect the microvascular anastomosis and promote union.
- For femoral head osteonecrosis, impact the fibula into a core-decompression tract reamed up the femoral neck into the necrotic segment (thoroughly debrided first).
- For massive lower-limb defects, use the Capanna technique — nesting the vascularised fibula inside a structural allograft shell for immediate mechanical stability while the fibula hypertrophies.
- Under the operating microscope, repair one artery and one or two veins using 8-0 or 9-0 nylon.
- Ensure the pedicle lies without kinking, twisting, or tension.
- Release the clamps and verify perfusion: the bone marrow should bleed, and the skin paddle (if used) should become pink with good capillary refill. Confirm flow with intra-operative Doppler.
- Close the recipient site over drains with the skin paddle visible. Close the donor leg; skin grafting may be required if the paddle was large. Do not close the fascia tightly — avoid a compartment syndrome.
Danger structures — what you protect at every step
Wraps around the fibular neck proximally. Resecting too far proximally — or excessive traction — endangers it. Always preserve the proximal 6–8 cm of fibula to protect the nerve and the lateral collateral ligament and biceps insertion.
The distal tibiofibular joint. Resecting the distal fibula destabilises the ankle mortise. Preserve the distal 6–8 cm to maintain the syndesmosis and lateral malleolus; consider a prophylactic syndesmotic screw if the harvest is borderline distal.
Runs closely along the posterior fibula, deep to FHL. It IS the graft's blood supply — injury during osteotomy or deep dissection destroys the transfer. Identify and protect it throughout; osteotomise only subperiosteally at the cut sites.
Caused by tethering, denervation, or ischaemia of the FHL belly (a cuff of which is left on the graft to protect the perforators). Prevent it with a minimal muscle cuff and early active and passive great-toe extension.
The fibular strut is initially weak compared with a femur or tibia and needs months to hypertrophy. Prevent it with rigid fixation (or a Capanna allograft shell for large lower-limb defects) and prolonged protected weight-bearing.
Highest risk in the first 72 hours. It leads to flap failure and graft necrosis. Prevent it with meticulous anastomotic technique, tension-free and unkinked vessel geometry, and careful post-operative monitoring of the skin paddle.
The peroneal artery and venae comitantes are the entire blood supply of the transfer. Identify the pedicle before any osteotomy, dissect it back to the tibioperoneal trunk for maximal length, and ligate the distal vessels first. Divide the proximal pedicle only once the recipient site, recipient vessels and fixation are all prepared, and note the ischaemia time. A skin paddle is invaluable — it gives you a visible, continuous monitor of perfusion after revascularisation.
Run the harvest and the recipient-site preparation concurrently so that ischaemia time is kept to a minimum. Have the recipient vessels isolated and the fixation planned before you divide the proximal pedicle — once it is cut, every minute of delay erodes graft viability.
A mobile graft thromboses its anastomosis and will not unite at the docking sites. Bridge the defect with a locking plate or an intramedullary nail. For massive lower-limb defects, the Capanna technique — a vascularised fibula nested inside a structural allograft shell — gives immediate load-bearing stability while the fibula hypertrophies, and it markedly reduces stress-fracture risk.
Aftercare & Complications
Rehabilitation | Phase | Timing | Recipient limb | Donor leg & monitoring | |-------|--------|----------------|------------------------| | Early | 0–7 days | Elevate; avoid any pressure over the pedicle or skin paddle | Hourly skin-paddle checks (colour, capillary refill, Doppler signal) for the first 24–48 hours; LMWH for DVT prophylaxis (some centres add aspirin or dextran); encourage active ankle and toe motion, especially great-toe extension, to prevent FHL contracture | | Intermediate | 1–6 weeks | Strict non-weight-bearing | Progress the donor leg to full weight-bearing as tolerated; continue aggressive FHL and Achilles stretching; x-ray to confirm alignment and fixation | | Late | 2–12 months | Progress weight-bearing only as radiographic docking-site union and graft hypertrophy appear | The fibula takes 6 to 18 months to hypertrophy to match the recipient bone; high-impact activity is restricted until substantial hypertrophy is visible on imaging | Complications
- Incidence
- 5–10 percent
- Recognition
- Skin paddle turns pale (arterial) or congested and blue (venous); Doppler signal is lost
- Prevention & management
- Prevention: meticulous microsurgery, avoid pedicle tension or kinking, keep the patient well hydrated. Management: urgent return to theatre for exploration, thrombectomy and revision of the anastomosis
- Incidence
- 2–5 percent
- Recognition
- Foot drop with sensory loss over the dorsum of the foot
- Prevention & management
- Prevention: strictly preserve the proximal 6–8 cm of fibula and avoid excessive traction. Management: AFO and physiotherapy; explore the nerve if there is no recovery after several months
- Incidence
- 10–20 percent
- Recognition
- Inability to fully extend the great toe; clawing
- Prevention & management
- Prevention: leave only a small cuff of FHL on the graft and begin early active and passive toe stretching. Management: physiotherapy and splinting; surgical FHL lengthening in severe refractory cases
- Incidence
- less than 5 percent
- Recognition
- Lateral ankle pain, clinical instability, and mortise widening on x-ray
- Prevention & management
- Prevention: preserve the distal 6–8 cm; add a prophylactic syndesmotic screw if the harvest is borderline distal. Management: syndesmotic fixation, or ankle arthrodesis if severely symptomatic
- Incidence
- 15–30 percent
- Recognition
- New-onset pain at the recipient site with callus or a fracture line on x-ray
- Prevention & management
- Prevention: rigid initial fixation, the Capanna allograft shell for large lower-limb defects, and prolonged protected weight-bearing until hypertrophy occurs. Management: restricted weight-bearing and bracing; revision fixation or bone grafting if non-union develops
- Incidence
- 10–15 percent
- Recognition
- Persistent pain with no bridging trabeculae on imaging
- Prevention & management
- Prevention: rigid fixation, a viable graft, and meticulous debridement of the recipient bone. Management: autologous bone grafting and revision of fixation
Viva & Exam Focus
FIBULAFIBULA — harvest limits and anatomy
GRAFTGRAFT — indications for FVFG
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 25-year-old man requires reconstruction of a 10 cm mid-diaphyseal tibial defect following resection of an adamantinoma. You plan a free vascularised fibular graft. What are the key anatomical landmarks and limitations you must respect during the fibular harvest?”
“You are treating a 30-year-old patient with pre-collapse osteonecrosis (Ficat Stage II) of the femoral head and are discussing a free vascularised fibular graft. How does the procedure address the pathology, and what is the surgical technique?”
Indications
- Segmental long-bone defects greater than 6 cm (tumour, trauma, infection)
- Pre-collapse femoral head AVN (Ficat/Steinberg I–II)
- Congenital pseudarthrosis of the tibia
Harvest boundaries
- Proximal 6–8 cm preserved — common peroneal nerve, LCL, biceps
- Distal 6–8 cm preserved — ankle syndesmosis, lateral malleolus
- Up to about 25 cm of diaphysis harvestable
Vascular anatomy
- Pedicle: peroneal artery and venae comitantes from the tibioperoneal trunk
- Endosteal supply (nutrient artery, middle third) plus periosteal (segmental) supply
- Skin paddle based on septocutaneous perforators along the posterior intermuscular septum
Technique
- Lateral approach between the peroneals and the soleus
- Subperiosteal dissection only at the osteotomy sites
- Leave a 1–2 mm FHL cuff to protect the perforators
- Rigid fixation protects the anastomosis and promotes union
- Capanna technique for massive lower-limb defects
Complications
- Microvascular thrombosis (5–10 percent) — needs urgent revision
- Common peroneal nerve palsy — from proximal over-resection
- Great-toe flexion contracture — FHL denervation or tethering
- Stress fracture before hypertrophy — protected weight-bearing
- Ankle instability — from distal over-resection
Background & Evidence
Surgical anatomy and blood supply. The fibula is a long, thin strut of cortical bone — non-weight-bearing in its proximal and diaphyseal regions but critical for ankle stability distally. Its diaphyseal blood supply comes entirely from the peroneal artery, a branch of the tibioperoneal trunk, which descends in the posterior compartment deep to the soleus and between tibialis posterior and FHL. A nutrient artery enters the middle third to give endosteal supply; multiple segmental periosteal and muscular branches supply the periosteum and overlying musculature; and septocutaneous perforators pass along the posterior intermuscular septum to the skin, allowing harvest of a vascularised skin paddle for post-operative monitoring. This dual endosteal and periosteal supply is what keeps a transferred fibula living and lets it heal by primary union. Compartments and the approach. The leg has three compartments — anterior (extensor digitorum longus, extensor hallucis longus, tibialis anterior), lateral (peroneus longus and brevis), and posterior (soleus, gastrocnemius, tibialis posterior, FHL). The lateral approach works the intermuscular plane between the peroneals and the soleus/FHL. The nerves at risk are the common peroneal nerve, which wraps around the fibular neck proximally, and the superficial peroneal nerve, which exits the lateral compartment in the distal third. Femoral head osteonecrosis — staging and the role of FVFG. Success is closely correlated with the stage at operation; the procedure works before collapse and fails once the head has collapsed.
- Definition
- No subchondral collapse on imaging
- Role of FVFG
- Best results; FVFG indicated in symptomatic patients under 50
- Definition
- Crescent sign or early collapse, with depression less than 2 mm
- Role of FVFG
- Offered in selected cases; counsel on a guarded outcome
- Definition
- Collapse greater than 2 mm, or joint-space loss
- Role of FVFG
- High failure rate; FVFG is generally not offered — consider arthroplasty
Key evidence. Vascularised fibular grafts achieve primary union in 70 to 90 percent of large defects. The Capanna technique — a vascularised fibula inside a massive structural allograft — provides immediate mechanical stability from the allograft and long-term biological viability from the fibula, significantly reducing the rate of stress fracture compared with FVFG alone. For femoral head AVN, FVFG reliably delays or prevents total hip arthroplasty in young patients with early-stage disease; head survival correlates with stage, and post-collapse heads (collapse greater than 2 mm) fail at high rates. Over 6 to 18 months the graft hypertrophies in response to loading (Wolff's law), which is why it is particularly suited to younger, active patients.
References
Treatment of osteonecrosis of the femoral head with free vascularized fibular grafting. A long-term follow-up study of one hundred and three hips.
- Long-term follow-up of 103 hips with osteonecrosis treated with FVFG
- Survival rate without THA was significantly higher for pre-collapse stages compared to post-collapse
- Established FVFG as a viable joint-preserving option for young patients with early AVN
A new reconstructive technique for intercalary defects of long bones: the association of massive allograft with vascularized fibular autograft. Long-term results and comparison with alternative techniques.
- Review of the combined massive allograft and vascularised fibular graft technique
- Demonstrates excellent immediate structural stability from the allograft and long-term biological viability from the fibula
- Significantly lower rate of stress fractures compared to isolated FVFG in lower limb reconstructions
Donor-site morbidity with use of vascularized autogenous fibular grafts.
- Detailed assessment of donor leg morbidity following fibular harvest
- Most common issues included great toe flexion weakness/contracture and mild ankle symptoms
- Confirmed the safety of the harvest provided proximal and distal anatomical boundaries are respected
Free vascularized fibular grafting-25 years' experience: tips, techniques, and pearls.
- Comprehensive review of 25 years of experience with vascularised fibular grafting techniques
- Highlights the superior healing and hypertrophy potential of vascularised bone compared to non-vascularised grafts in hostile recipient beds
- Outlines the critical importance of rigid fixation and meticulous microvascular technique
Revascularization of the femoral head in osteonecrosis.
- Comprehensive review of vascularised bone grafting techniques for femoral head osteonecrosis
- Demonstrates that FVFG reliably prevents collapse in pre-collapse AVN (Ficat Stage I-II) and provides sustained femoral head survival
- Outlines patient selection criteria: younger age, pre-collapse stage, and adequate remaining bone stock are the strongest predictors of success