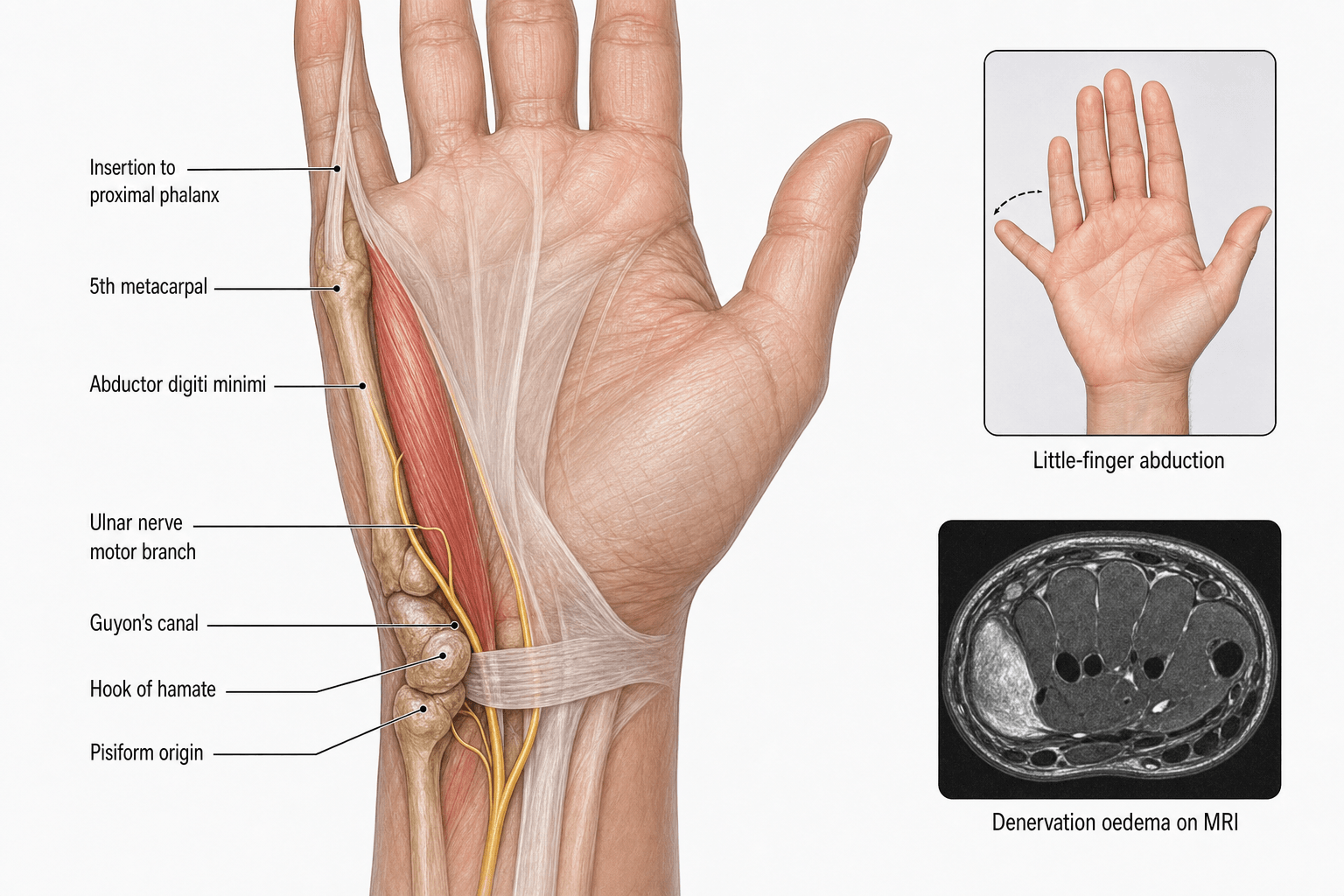
Ulnar Nerve | Pisiform Origin | MCP Abduction | Guyon Canal Landmark
- Deep branch of ulnar nerve (C8, T1) supplies the ADM
- Pisiform bone is the primary origin - key landmark
- Dual insertion to proximal phalanx AND extensor expansion
- Forms ulnar border of Guyon canal
- Wasting indicates ulnar nerve pathology at or proximal to wrist
- “Compare hypothenar eminences bilaterally for asymmetric wasting
- “Zone 2 compression = pure motor loss, no sensory deficit
- “Wartenberg sign paradox: ADM also ulnar-innervated but EDM abducts
- “ADM testing is key for localizing ulnar nerve lesions
Deep branch of ulnar nerve (C8, T1) supplies the ADM. Testing abduction of the little finger is a key clinical test for ulnar nerve function. Complete ulnar nerve palsy causes visible hypothenar wasting.
The ADM forms the ulnar border of Guyon canal. The ulnar nerve and artery pass through this tunnel. Compression here causes different patterns than cubital tunnel syndrome.
The ADM originates primarily from the pisiform bone, making this sesamoid bone clinically important. Pisiform fractures or excision may affect ADM function.
Inserts onto both the proximal phalanx base and extensor expansion. This dual insertion allows both MCP abduction and contribution to little finger extension.
Overview and Anatomical Location

The abductor digiti minimi is the most superficial and ulnar of the three hypothenar muscles. It forms the visible ulnar border of the hypothenar eminence when the hand is at rest. The muscle belly is readily palpable along the ulnar border of the palm and is an important clinical landmark for assessing ulnar nerve function.
Anatomical Position:
- Located on the ulnar side of the palm
- Forms the lateral boundary of the hypothenar eminence
- Lies superficial to the flexor digiti minimi brevis
- Parallel to the axis of the fifth metacarpal
- Most superficial of the hypothenar muscles
Compare both hypothenar eminences with the hand supinated and at rest. Asymmetric wasting strongly suggests ulnar nerve pathology. The ADM is the most obvious muscle to assess visually.
The hypothenar compartment is bounded superficially by the palmar aponeurosis and deeply by the fifth metacarpal. The ADM, along with the flexor digiti minimi brevis and opponens digiti minimi, fills this compartment and provides the fleshy prominence on the ulnar side of the palm.
Concepts and Principles
The abductor digiti minimi is best understood through five exam-critical concepts that recur in vivas and MCQs:
- Origin and identity - the most superficial and most ulnar hypothenar muscle, arising chiefly from the pisiform (a sesamoid within the flexor carpi ulnaris tendon); it forms the visible ulnar border of the hypothenar eminence and the ulnar wall of Guyon canal.
- Innervation - the deep branch of the ulnar nerve (C8, T1); the ADM is the first muscle supplied by the deep branch after the nerve bifurcates near the pisiform.
- Action - abduction of the little finger at the MCP joint, with secondary MCP flexion and a contribution to IP extension through its slip to the extensor expansion.
- Localising value - ADM wasting indicates an ulnar lesion at or proximal to the wrist; combining ADM with FCU, FDP 4-5 and sensory testing localises the level (wrist vs elbow), while preserved sensation with motor loss localises to the deep branch (Zone 2).
- Surgical landmark - the deep motor branch curves around the hook of hamate deep to the ADM origin, the relationship that governs Guyon canal decompression.
Origin and Insertion
Origin
The abductor digiti minimi has a complex origin from multiple structures on the ulnar side of the wrist:
- Pisiform bone - The main origin is from the medial and palmar surface of the pisiform, which is a sesamoid bone within the tendon of flexor carpi ulnaris
- Pisohamate ligament - The ligament connecting the pisiform to the hook of hamate
- Flexor retinaculum - The ulnar aspect of the transverse carpal ligament
- Hypothenar fascia - Deep fascia overlying the hypothenar compartment
- Primary Origin
- Pisiform bone
- Secondary Origin
- Pisohamate ligament, flexor retinaculum
- Primary Origin
- Hook of hamate
- Secondary Origin
- Flexor retinaculum
- Primary Origin
- Hook of hamate
- Secondary Origin
- Flexor retinaculum
Insertion
The muscle has a dual insertion providing both mechanical and functional advantages:
- Ulnar side of the base of the proximal phalanx of the little finger - This provides the primary abduction function at the MCP joint
- Ulnar edge of the extensor expansion (dorsal digital expansion) of the little finger - This allows contribution to finger extension, particularly at the IP joints
The dual insertion to both the proximal phalanx and extensor expansion means the ADM can both abduct the little finger at the MCP joint AND contribute to extension. This is why isolated ADM testing should be done with the MCP joint in slight flexion to eliminate extensor contribution.
Nerve Supply
Primary Innervation
The abductor digiti minimi receives its motor innervation from the deep branch of the ulnar nerve with root values from C8 and T1.
Pathway of the ulnar nerve to ADM:
- Ulnar nerve enters the hand through Guyon canal (ulnar tunnel)
- Divides into superficial and deep branches at the level of the pisiform
- Deep branch curves around the hook of hamate
- Immediately supplies the hypothenar muscles (ADM first)
- Continues deep into the palm to supply interossei and lumbricals 3-4
- Motor Supply
- Palmaris brevis only
- Sensory Supply
- Ulnar 1.5 digits (palmar)
- Motor Supply
- Hypothenars, interossei, lumbricals 3-4, adductor pollicis
- Sensory Supply
- None
Clinical Implications
Guyon Canal Syndrome Zones:

The site of compression in Guyon canal determines the clinical presentation:
- Zone 1 (proximal to bifurcation): Mixed motor and sensory loss including ADM weakness
- Zone 2 (deep branch only): Pure motor loss including ADM - no sensory loss
- Zone 3 (superficial branch only): Pure sensory - ADM spared
Zone 2 compression (deep branch only) causes weakness of all ulnar-innervated intrinsics including ADM BUT spares sensation. Classic causes include ganglion cysts, hook of hamate fractures, or cyclist's palsy. ADM testing is essential.
Differentiating Levels of Ulnar Nerve Lesion:
- FCU
- Weak
- FDP 4-5
- Weak
- Sensory
- Lost
- ADM
- Weak
- Interossei
- Weak
- FCU
- Normal
- FDP 4-5
- Variable
- Sensory
- Lost
- ADM
- Weak
- Interossei
- Weak
- FCU
- Normal
- FDP 4-5
- Normal
- Sensory
- Lost
- ADM
- Weak
- Interossei
- Weak
- FCU
- Normal
- FDP 4-5
- Normal
- Sensory
- Normal
- ADM
- Weak
- Interossei
- Weak
Blood Supply
Arterial Supply
The abductor digiti minimi receives its blood supply from multiple sources, primarily derived from the ulnar artery:
- Deep palmar branch of the ulnar artery - Main arterial supply to the muscle belly
- Ulnar artery - Direct branches as it courses through Guyon canal
- Deep palmar arch (anastomosis) - Contributes to the deep supply
- Muscular branches from surrounding vessels
Venous Drainage
Venous drainage follows the arterial supply:
- Venae comitantes accompanying the arterial branches
- Drain into the deep palmar venous arch
- Ultimately to the ulnar veins
Lymphatic Drainage
- Lymphatics follow the venous drainage
- Drain to epitrochlear nodes and then to axillary nodes
- Important in understanding spread of infection from the hypothenar region
The close relationship of the ulnar artery to the ADM within Guyon canal means that hypothenar hammer syndrome (repetitive trauma to the ulnar artery) can present with both vascular symptoms AND ADM weakness or wasting.
Function and Actions
Primary Actions
1. Abduction of the Little Finger at the MCP Joint
- The primary function is to move the little finger away from the ring finger in the plane of the palm
- Most effective when the MCP joint is in neutral or slight flexion
- Works against gravity when the forearm is supinated
2. Flexion of the MCP Joint
- Secondary function due to its palmar position relative to the MCP joint axis
- Contributes to power grip when the little finger wraps around objects
3. Extension of the IP Joints (Contribution)
- Through its insertion into the extensor expansion
- Helps extend the PIP and DIP joints when the MCP is stabilized
- Works synergistically with the extensor digitorum
Functional Testing
- Technique
- Spread fingers apart against resistance
- Interpretation
- Tests ADM and palmar interossei
- Technique
- Observe resting posture of little finger
- Interpretation
- Abducted little finger = weak interossei, unopposed ADM
- Technique
- Hold paper between extended fingers
- Interpretation
- Tests adduction (interossei), not ADM
The Wartenberg sign (abducted little finger at rest) indicates ulnar nerve palsy, but ADM is ALSO ulnar-innervated. The explanation: the EDM (radial nerve) has an ulnar slip that abducts the little finger when the interossei are weak. ADM is too weak to counteract this in ulnar palsy.
Grip Function
The ADM contributes to:
- Power grip - Helps wrap the little finger around objects
- Hook grip - Maintains finger position during sustained grip
- Precision handling - Fine adjustments of little finger position
In ulnar nerve palsy, loss of ADM function contributes to difficulty with tasks requiring little-finger positioning. Importantly, grip strength is a poor surrogate for intrinsic recovery: in long-term outcome data, grip recovered to around 83% of the uninjured side while isolated intrinsic (ulnar-innervated) strength recovered to only 26 to 37%, so dedicated little-finger abduction testing is required to detect residual ADM weakness.
Anatomical Relationships
Guyon Canal (Ulnar Tunnel)
The ADM has a critical relationship with Guyon canal:
- Roof: Palmar carpal ligament (volar carpal ligament) and palmaris brevis
- Floor: Flexor retinaculum and hypothenar muscles
- Ulnar wall: Pisiform bone and ADM origin
- Radial wall: Hook of hamate
- Ulnar nerve
- Ulnar artery
- Ulnar veins
- Fat
Guyon canal is ULNAR to the carpal tunnel and is NOT covered by the flexor retinaculum (transverse carpal ligament). The pisiform and hook of hamate are the key bony landmarks. Carpal tunnel release does NOT decompress Guyon canal.
Relationship to Other Hypothenar Muscles
- Abductor digiti minimi (most superficial, most ulnar)
- Flexor digiti minimi brevis (intermediate, more radial)
- Opponens digiti minimi (deepest, on fifth metacarpal)
When approaching the hypothenar region, the ADM is encountered first and must be protected or retracted to access deeper structures.
Relationship to the Fifth Metacarpal
The ADM lies ulnar to the fifth metacarpal shaft. In fifth metacarpal fractures (boxer's fractures), the muscle may be involved in:
- Soft tissue swelling
- Compartment syndrome (rare)
- Displacement forces
Classification
Guyon Canal Zone Classification
The Gross and Gelberman classification divides Guyon canal into three anatomical zones based on the relationship to the ulnar nerve bifurcation:
Zone 1 - Proximal Zone
- Location: Proximal to the bifurcation of the ulnar nerve
- Contents: Main trunk of ulnar nerve (motor and sensory)
- Clinical pattern: Mixed motor and sensory deficit
- ADM status: Weak (motor component affected)
Zone 2 - Deep Motor Zone
- Location: Around the hook of hamate, deep branch territory
- Contents: Deep motor branch only
- Clinical pattern: Pure motor deficit, sensation preserved
- ADM status: Weak (key finding - motor loss without sensory loss)
Zone 3 - Superficial Sensory Zone
- Location: Distal, superficial branch territory
- Contents: Superficial sensory branch only
- Clinical pattern: Pure sensory deficit, motor preserved
- ADM status: Normal (motor branch not affected)
This classification guides surgical decompression planning.

Clinical Significance
Assessment in Ulnar Nerve Palsy
The ADM is a key muscle for clinical assessment of ulnar nerve function:
- Compare hypothenar eminences bilaterally
- Look for wasting (flattening of the ulnar palm border)
- Note any asymmetry in muscle bulk
- Feel for muscle bulk with hand at rest
- Palpate during active abduction to confirm contraction
- Ask patient to spread fingers apart against resistance
- Observe abduction strength of the little finger specifically
- Grade power (MRC scale 0-5)
Pathological Conditions
1. Ulnar Nerve Palsy
- ADM wasting is an early sign of ulnar nerve pathology
- Loss of abduction power affects grip function
- May be isolated in Zone 2 Guyon canal compression
2. Dupuytren Disease
- The hypothenar area can be affected
- ADM may become contracted or tethered
- Can contribute to MCP flexion contracture of the little finger
3. Hypothenar Hammer Syndrome
- Repetitive trauma to the hypothenar eminence
- Can cause ulnar artery thrombosis
- May present with ADM dysfunction secondary to ischemia or nerve compression
4. Guyon Canal Syndrome
- Compression of ulnar nerve in the canal
- Causes vary: ganglion, anomalous muscles, hook of hamate fracture
- ADM weakness depends on zone of compression
Differential Diagnosis of Hypothenar Wasting / Little-Finger Abduction Weakness
- Distinguishing Features
- ADM + interossei weak, ulnar 1.5-digit sensory loss; FCU and FDP 4-5 normal
- Key Discriminator
- Sensory loss present but FCU/FDP spared = wrist-level
- Distinguishing Features
- ADM + all ulnar intrinsics weak, sensation fully preserved
- Key Discriminator
- Pure motor, no sensory loss - localises to deep branch
- Distinguishing Features
- ADM, interossei weak; FDP 4-5 and FCU often involved; dorsal ulnar sensory loss
- Key Discriminator
- Dorsal hand sensory loss + FDP/FCU weakness = elbow-level
- Distinguishing Features
- Weakness crosses median + ulnar territory (e.g. APB also weak); neck/arm pain, dermatomal sensory loss
- Key Discriminator
- Median-innervated thenar weakness too = root/plexus, not ulnar
- Distinguishing Features
- T1-predominant intrinsic wasting, Horner syndrome, medial arm pain
- Key Discriminator
- Horner / apical chest signs
- Distinguishing Features
- Painless wasting, fasciculations, no sensory loss, spreads beyond ulnar territory
- Key Discriminator
- Fasciculations + UMN signs + non-territorial spread
- Distinguishing Features
- Symmetrical, no sensory loss, normal nerve conduction
- Key Discriminator
- Bilateral, normal NCS, no denervation pattern
The ADM as a Transfer and Flap (Huber Opponensplasty)
The topic details the ADM's pisiform origin, its phalangeal and extensor-expansion insertion, and its supply from the deep branch of the ulnar nerve and the ulnar artery - but never notes that this is exactly the pedicle anatomy that makes the muscle a workhorse for reconstruction.
- Why the anatomy allows it. The ADM has a proximally-entering neurovascular pedicle (the deep ulnar nerve branch and an ulnar-artery branch enter near the pisiform), so the muscle can be islanded on that proximal pedicle, released from the pisiform origin, and rotated across the palm without devascularising or denervating it. Its superficial, ulnar-border position makes it easy to raise.
- The Huber (abductor digiti minimi) opponensplasty. The ADM is turned over roughly 180 degrees on its pedicle, tunnelled subcutaneously across the palm, and inserted onto the thumb (abductor pollicis brevis insertion / thumb MCP) to restore opposition. Its classic indication is congenital thumb hypoplasia (where it also adds a muscle belly to a deficient thenar eminence), and it is also used for low median nerve palsy.
- The ADM as a local muscle flap. The same reliable proximal pedicle lets the ADM be used as a small rotational muscle flap for soft-tissue coverage of the ulnar palm, wrist and Guyon-canal region (for example over an exposed ulnar neurovascular repair).
- The trade-off. Harvesting the ADM sacrifices little-finger abduction, which is well tolerated; the muscle's origin is released while its pedicle is protected. (The indications and step-by-step technique of the transfer are developed in the thumb-hypoplasia and tendon-transfers topics - the point here is that the muscle's own anatomy is what permits it.)
Q: Why can the abductor digiti minimi be used for a Huber opponensplasty? A: Its neurovascular pedicle (deep ulnar nerve branch + ulnar-artery branch) enters proximally near the pisiform, so the muscle can be islanded on that pedicle, released from the pisiform, and rotated ~180 degrees across the palm to the thumb to restore opposition - the classic reconstruction for congenital thumb hypoplasia (adding thenar bulk) and for low median nerve palsy. Losing little-finger abduction is well tolerated.
Palmaris Brevis and the Palmaris Brevis Sign
The topic repeatedly names the palmaris brevis - as part of the roof of Guyon canal and as the only muscle supplied by the superficial branch of the ulnar nerve - but never develops its function or its localising value.
- What it is. Palmaris brevis is a small, quadrilateral skin muscle of the hypothenar eminence, running transversely from the palmar aponeurosis/flexor retinaculum to the dermis of the ulnar palmar skin. It is the only motor muscle of the superficial (mainly sensory) branch of the ulnar nerve.
- What it does. On contraction it wrinkles/dimples the ulnar palmar skin, deepens the hollow of the palm and elevates the hypothenar eminence - improving cupping and grip - and it protects the underlying ulnar nerve and artery in Guyon canal.
- The palmaris brevis sign (localising value). Because palmaris brevis is supplied by the superficial branch, it is spared in a deep-branch (Zone 2) lesion: preserved hypothenar skin dimpling on little-finger resisted abduction, alongside weak ADM and interossei, points to a pure deep-branch lesion. Loss of palmaris brevis contraction instead implicates the superficial branch or the main trunk (Zone 1). (Isolated overactivity gives the rare palmaris brevis spasm syndrome.)
- Why it matters here. It complements the ADM in localising an ulnar lesion at the wrist: ADM weak + palmaris brevis preserved = deep-branch (Zone 2), tightening the zone diagnosis the topic builds around.
Q: What is the palmaris brevis sign and how does it complement ADM testing? A: Palmaris brevis is a hypothenar skin muscle that dimples the ulnar palm and is the only muscle of the superficial ulnar branch. So in a deep-branch (Zone 2) lesion it is spared: weak ADM/interossei with preserved hypothenar skin dimpling localises to the deep branch, whereas lost dimpling implicates the superficial branch or the main trunk (Zone 1).
Investigations
Electrophysiology
- Motor studies recording from ADM are standard for ulnar nerve assessment
- Stimulate at wrist and below elbow
- Compare latency and amplitude to contralateral side
- Slowing across Guyon canal suggests canal compression
- Needle EMG of ADM can detect denervation changes
- Fibrillations and positive sharp waves indicate acute denervation
- Reinnervation potentials (polyphasic units) in recovery
- Normal Value
- Less than 3.5 ms
- Abnormal Finding
- Prolonged in distal compression
- Normal Value
- Greater than 6 mV
- Abnormal Finding
- Reduced with axonal loss
- Normal Value
- Greater than 50 m/s
- Abnormal Finding
- Slowed across lesion site
Imaging
- Can assess ADM muscle bulk and echogenicity
- Fatty infiltration suggests chronic denervation
- Dynamic assessment of nerve at Guyon canal
- Gold standard for muscle denervation assessment
- Acute denervation: T2 hyperintensity (edema)
- Chronic denervation: Fatty replacement on T1
Management
Conservative Management
- Mild symptoms with no motor weakness
- Early or intermittent compression
- Reversible causes (e.g., ganglion cyst observation)
- Activity modification (avoid prolonged gripping, cycling pressure)
- Wrist splinting in neutral position
- Ergonomic assessment for occupational causes
- NSAIDs for symptomatic relief
- Physiotherapy for nerve gliding exercises
Surgical Management
- Progressive motor weakness (ADM wasting)
- Failure of 3-6 months conservative treatment
- Fixed structural cause (hook of hamate fracture, space-occupying lesion)
- Severe or sudden onset palsy
- Guyon canal decompression (primary procedure)
- Excision of space-occupying lesion (ganglion, lipoma)
- Hook of hamate excision for nonunion or compression
- Neurolysis if intraneural fibrosis present
Motor recovery depends on duration and severity of compression. Early decompression within 3 months of symptom onset has better prognosis. ADM function typically recovers before intrinsic hand muscles due to shorter reinnervation distance.
Surgical Approaches
Guyon Canal Decompression
Compression of the ulnar nerve within Guyon canal confirmed by clinical examination and nerve conduction studies.
- Supine with arm on hand table
- Forearm supinated
- Tourniquet on upper arm
- Longitudinal incision along the radial border of the pisiform
- Extends distally toward the hook of hamate
- Alternatively, curvilinear incision following skin crease
- Incise skin and subcutaneous tissue
- Identify and protect the palmar cutaneous branch of the ulnar nerve
- Incise the palmar carpal ligament (roof of canal)
- Identify the ulnar nerve and artery within the canal
- Follow the nerve distally as it bifurcates
- Release the fibrous arch of the hypothenar muscles if compressing deep branch
- Identify the hook of hamate as key landmark
- The ADM origin may need to be partially released if the deep branch is compressed at this level
- Preserve as much muscle origin as possible
- The deep branch of the ulnar nerve runs beneath the ADM origin
- Close subcutaneous tissue and skin
- Bulky dressing with wrist in neutral
This section describes the surgical approach for Guyon canal decompression.
Complications
Surgical Complications
Nerve Injury
- Injury to deep branch of ulnar nerve during Guyon canal decompression
- Damage to palmar cutaneous branch causing sensory deficit
- Dorsal sensory branch at risk with proximal extension of incision
- Neurapraxia from excessive retraction (usually recovers)
Vascular Injury
- Ulnar artery laceration or thrombosis
- Haematoma formation compromising nerve recovery
- Hypothenar hammer syndrome exacerbation
Wound Complications
- Superficial or deep infection
- Wound dehiscence
- Hypertrophic or painful scarring
- Pillar pain (tenderness at incision margins)
Complications of Non-Treatment
Progressive Motor Loss
- Worsening ADM atrophy and weakness
- Involvement of all ulnar-innervated intrinsics
- Irreversible muscle fibrosis if denervation prolonged beyond 12-18 months
Functional Impairment
- Loss of fine intrinsic control (precision pinch, finger abduction/adduction) - the dominant functional deficit
- Difficulty with power grip and precision handling
- Clawing of ring and little fingers in advanced cases (intrinsic-minus posture)
Motor recovery is time-dependent. Decompression within 3-6 months of symptom onset has significantly better outcomes than delayed surgery. Chronic denervation beyond 18 months may result in permanent motor deficit despite technically successful decompression.
Postoperative Care
Immediate Postoperative Phase (0-2 weeks)
Wound Care
- Bulky dressing with wrist in neutral position
- Elevation to reduce swelling
- Wound check at 10-14 days, suture removal
- Keep wound clean and dry
Activity Restrictions
- No heavy gripping or lifting
- Avoid direct pressure on hypothenar region
- Gentle finger range of motion encouraged from day 1
- Light activities of daily living permitted
Early Rehabilitation Phase (2-6 weeks)
Hand Therapy
- Active and gentle passive range of motion exercises
- Scar massage once wound healed
- Nerve gliding exercises to prevent adhesions
- Oedema management techniques
Activity Progression
- Gradual return to light duties
- Avoid repetitive gripping activities
- Splinting rarely needed unless specific concerns
Late Rehabilitation Phase (6-12 weeks)
Strengthening
- Progressive grip strengthening exercises
- ADM-specific abduction exercises
- Functional task training
- Occupational therapy for work-specific requirements
Return to Activity
- Return to desk work typically 2-3 weeks
- Manual work 6-8 weeks depending on demands
- Return to cycling 8-12 weeks with ergonomic modifications
- Full motor recovery may take 6-12 months
Outcomes
Motor Recovery
Prognostic Factors
- Duration of symptoms (most important factor)
- Severity of preoperative weakness
- Presence of axonal loss on EMG
- Patient age and general health
- Aetiology of compression
Expected Outcomes by Timing
- Expected ADM Recovery
- Complete recovery expected
- Overall Prognosis
- Excellent
- Expected ADM Recovery
- Good recovery, may be incomplete
- Overall Prognosis
- Good
- Expected ADM Recovery
- Partial recovery likely
- Overall Prognosis
- Fair
- Expected ADM Recovery
- Limited recovery expected
- Overall Prognosis
- Guarded
Functional Outcomes
Grip and Intrinsic Strength
- Grip strength often recovers reasonably (around 80% of the contralateral side in long-term series) because it is dominated by extrinsic forearm flexors
- Isolated intrinsic (ulnar-innervated) muscle strength recovers far less completely (26 to 37% in long-term data), so apparent grip recovery overstates true ADM/interosseous recovery
- ADM function tends to recover before more distal intrinsic muscles owing to shorter reinnervation distance
- Meaningful motor recovery typically continues over 6 to 12 months post-decompression
Patient Satisfaction
- High satisfaction rates (greater than 85%) for early surgical intervention
- Sensory recovery (when applicable) often precedes motor recovery
- Pain relief typically rapid following decompression
- Return to work rates depend on occupational demands
Motor recovery follows the principle of reinnervation distance. ADM, being the first muscle innervated by the deep branch after bifurcation, typically shows the earliest and best recovery. More distal muscles (interossei, lumbricals) recover later and less completely.
Guidelines, Registries & Global Practice
Global epidemiology:
- Ulnar neuropathy is the second most common compressive upper-limb neuropathy worldwide after carpal tunnel syndrome; the great majority of ulnar lesions are at the elbow (cubital tunnel), with wrist-level (Guyon canal) compression being comparatively uncommon.
- In operative ulnar tunnel syndrome series the commonest causes are idiopathic and traumatic, followed by ganglion and other space-occupying lesions; coexistent carpal tunnel syndrome is frequent (up to ~70% in some series).
- Cyclist's palsy is a well-described occupational/recreational form of Guyon canal neuropathy: more than 90% of long-distance cyclists develop transient motor and/or sensory symptoms after a single multi-hundred-kilometre ride.
Side-by-side society guidance (no dedicated ADM/Guyon guideline exists - principles drawn from ulnar/peripheral nerve guidance):
- Position relevant to Guyon canal / ADM
- No standalone Guyon canal guideline; clinical diagnosis plus electrodiagnostic confirmation, imaging for suspected mass; surgery for confirmed compression failing conservative care
- Position relevant to Guyon canal / ADM
- Hand-surgery consensus: examine intrinsics (including little-finger abduction/ADM), confirm and localise with NCS/EMG, image to exclude space-occupying lesion before decompression
- Position relevant to Guyon canal / ADM
- Emphasises hook-of-hamate fracture and perilunate/CMC trauma as structural causes of deep-branch (Zone 2) palsy requiring fixation/excision plus decompression
- Position relevant to Guyon canal / ADM
- Supports nerve-conduction localisation and ultrasound/MRI for atypical or young patients to detect anomalous muscles or vascular causes
Compressive neuropathy decompressions are not separately captured by joint-replacement registries (NJR, AJRR, AOANJRR); evidence is therefore drawn from cohort and case series rather than registry data.
- High-resource settings: routine nerve conduction studies/EMG and high-resolution ultrasound or 3T MRI to localise the zone and identify ganglia, hook-of-hamate fractures, hypothenar hammer syndrome or an accessory ADM before surgery.
- Limited-resource settings: diagnosis rests largely on careful clinical examination (bilateral hypothenar comparison, ADM and first dorsal interosseous testing, Froment and Wartenberg signs); decompression may proceed on clinical grounds where electrodiagnostics are unavailable, with greater reliance on activity modification first.
Controversies and Areas of Uncertainty
Clinically Debated Points
1. Routine vs selective electrodiagnostics before decompression In well-resourced settings nerve conduction studies and EMG are standard to localise the zone, but they can be normal in early or purely deep-branch (Zone 2) compression - Akuthota et al. showed deep-branch latency prolongation with a normal ADM-recorded response. Some surgeons therefore proceed on strong clinical grounds when imaging shows a structural cause.
2. Significance of an accessory ADM Historically the accessory ADM was reported as a common cause of ulnar tunnel syndrome. Rixey et al. (3T MRI, n=396) found it in 25% of wrists but a true muscular type in only ~8%, all asymptomatic - so its causative role has been overstated and it should be implicated only when it is genuinely muscular and other causes are excluded.
3. ADM as a recording site in ulnar nerve conduction Recording the compound motor action potential from ADM is conventional, but because ADM is innervated immediately after the bifurcation, a deep-branch lesion distal to its take-off can spare the ADM response while the interossei are denervated. Recording additionally from the first dorsal interosseous improves sensitivity for distal deep-branch lesions.
4. Extent of ADM origin release at surgery There is no consensus on how much of the ADM origin (and the fibrous hypothenar arch) must be divided to decompress the deep branch; the aim is adequate release of the arch while preserving as much muscle origin and function as possible.
5. Grip strength as an outcome measure Grip strength recovers far better than isolated intrinsic strength after ulnar nerve injury (Schreuders et al.: ~83% grip vs 26-37% intrinsic), so grip is an unreliable surrogate and dedicated little-finger abduction (ADM) measurement is preferred for honest outcome assessment.
MCQ Practice Points
A: The pisiform bone. Secondary origins include the pisohamate ligament and flexor retinaculum. This is the most commonly tested anatomy fact about ADM.
A: The deep branch of the ulnar nerve (C8, T1). NOT the superficial branch - this is a common distractor. The ADM is the first muscle supplied after the nerve bifurcates at the level of the pisiform.
A: Zone 2 of Guyon canal (deep motor branch only). Zone 2 causes pure motor deficit with preserved sensation. Zone 1 would cause mixed motor and sensory loss. Zone 3 causes pure sensory loss with preserved motor function.
A: The ADM inserts onto both the ulnar base of the proximal phalanx AND the ulnar edge of the extensor expansion. This allows it to abduct the little finger at the MCP joint AND contribute to IP extension.
A: ADM wasting indicates ulnar nerve pathology AT or PROXIMAL to the wrist. It helps distinguish wrist-level compression (Guyon canal) from elbow-level compression (cubital tunnel) when combined with FCU and FDP testing. Both levels cause ADM wasting, but only elbow lesions affect FCU and FDP 4-5.
Key Numbers for MCQs
- C8, T1 - nerve root supply
- 3 - hypothenar muscles (ADM most superficial)
- 3 - Guyon canal zones (Gross & Gelberman)
- 26-37% - long-term intrinsic strength recovery after ulnar nerve injury (vs ~83% grip)
- 25% - prevalence of an accessory ADM on wrist MRI (true muscular type only ~8%)
At a Glance
The abductor digiti minimi (ADM) is the most superficial hypothenar muscle, originating from the pisiform and innervated by the deep branch of the ulnar nerve (C8-T1). It is essential for clinical assessment of ulnar nerve function, with wasting indicating pathology at or proximal to the wrist. Understanding Guyon canal zones is critical for localizing compression - Zone 2 causes pure motor loss including ADM weakness with preserved sensation.
FAOHypothenar Muscles - FAO
Hook:FAO - like the UN organization, these three muscles work together for small finger function. Superficial to deep order is Abductor, Flexor, Opponens.
ADMADM Origins - PPH
Hook:PPH - the Pisiform is the Primary origin for the Hypothenar ADM muscle.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 45-year-old cyclist presents with weakness of finger abduction and numbness of the little finger. How would you examine the hypothenar muscles and what anatomy is relevant?”
“A 52-year-old manual worker has clawing of the ring and little fingers, hypothenar and first dorsal interosseous wasting, but you are unsure whether the lesion is at the elbow or the wrist. How does the abductor digiti minimi help you, and how do you localise the lesion clinically?”
“You are decompressing Guyon canal for a confirmed ulnar tunnel syndrome. Describe the boundaries and contents of the canal, the relationship of the ADM, and the structures most at risk.”
Origin and Insertion
- Origin: Pisiform bone (primary), pisohamate ligament, flexor retinaculum
- Insertion: Ulnar base of proximal phalanx AND ulnar edge of extensor expansion
- Dual insertion allows MCP abduction AND IP extension contribution
- Most superficial and ulnar of the hypothenar muscles
Nerve Supply
- Deep branch of ulnar nerve (C8, T1)
- Nerve divides at level of pisiform into superficial and deep branches
- Deep branch curves around hook of hamate to reach ADM
- First muscle supplied by deep branch after bifurcation
Blood Supply
- Deep palmar branch of ulnar artery (primary)
- Direct branches from ulnar artery in Guyon canal
- Contributions from deep palmar arch
- Venous drainage via deep palmar venous arch to ulnar veins
Actions
- Primary: Abduction of little finger at MCP joint
- Secondary: MCP flexion due to palmar position
- Contribution to IP extension via extensor expansion insertion
- Functional: Power grip, hook grip, precision handling
Clinical Relevance
- Wasting indicates ulnar nerve pathology at or proximal to wrist
- Forms ulnar border of Guyon canal - key surgical landmark
- Zone 2 compression: pure motor loss, ADM weak, sensory spared
- Wartenberg sign paradox: ADM also weak but EDM abducts unopposed
Guyon Canal Zones
- Zone 1: Proximal to bifurcation - mixed motor and sensory loss
- Zone 2: Deep branch - pure motor (includes ADM), sensory spared
- Zone 3: Superficial branch - pure sensory, ADM function preserved
- Hook of hamate fracture classically causes Zone 2 compression
Evidence Base
- Defined the distal ulnar tunnel as a 4 to 4.5 cm region with three zones based on the ulnar nerve bifurcation
- All 39 cases of combined motor and sensory deficit localised to Zone 1; all 36 Zone 2 lesions caused intrinsic paralysis; Zone 3 lesions caused sensory deficit only
- Whether hypothenar muscles (including ADM) are affected in Zone 2 depends on the exact site of the lesion within that zone
- Combined deficits arose from compression deep to the nerve, pure sensory deficits from compression superficial to it
- 31 operatively treated ulnar tunnel syndrome cases: idiopathic in 14, trauma in 8, thrombosis in 2, synovial proliferation in 2, with single cases of hook of hamate prominence, schwannoma, fibrous band and ganglion
- Zone 1 was involved in 28 cases, Zone 3 in 19, Zone 2 in 6; 55% had compression spanning more than one zone
- 71% of cases were associated with concurrent carpal tunnel syndrome
- Symptoms improved after Guyon canal and/or pisohamate tunnel release in all cases
- 23 of 25 cyclists developed motor and/or sensory symptoms after a single 600 km ride
- Isolated motor symptoms occurred in 36% of hands, isolated sensory in 10%, combined motor-and-sensory in 24%
- Symptom rate was independent of cyclist experience level
- Gloves, correct bike fit and frequent hand-position changes were recommended as preventive measures
- Distal motor latency of the deep ulnar branch to the first dorsal interosseous was significantly prolonged after a 6-day, 420-mile ride
- Ulnar motor latency recorded from abductor digiti minimi and ulnar/median sensory studies did NOT change significantly
- Selective deep-branch (Zone 2 type) slowing was demonstrated, sparing the ADM-recorded response
- Carpal tunnel symptoms were also exacerbated in some cyclists
- More than 2 years after injury, grip strength recovered to 83% of the uninjured hand whereas intrinsic ulnar-innervated muscle strength (measured by the Rotterdam Intrinsic Hand Myometer) recovered to only 26-37%
- No significant correlation between intrinsic muscle strength and grip strength recovery
- Manual muscle testing and grip dynamometry overestimated recovery of the small hand muscles
- Selective intrinsic dynamometry (including little-finger abduction) detected residual ADM and interosseous weakness missed by routine tests
- An accessory abductor digiti minimi was present in 25% of 396 wrist MRIs, but a true contiguous muscular type in only 8%
- The majority (69%) were a small fascial-type slip proximal to Guyon canal arising from the distal antebrachial fascia
- All patients were asymptomatic with normal EMG and no significant nerve compression
- Only 1 of 98 accessory muscles had been identified prospectively on the original report
- Standard reference framework for ulnar tunnel anatomy, Gross-Gelberman zone classification and surgical decompression technique
- Recommends nerve conduction studies and cross-sectional imaging to identify a space-occupying lesion before surgery
- Decompression involves release of the volar carpal ligament, the fibrous arch of the hypothenar muscles and the deep motor branch around the hook of hamate
- Emphasises protecting the deep motor branch as it passes deep to the ADM origin
References
-
Gross MS, Gelberman RH. The anatomy of the distal ulnar tunnel. Clin Orthop Relat Res. 1985;(196):238-247. PMID: 3995823.
-
Murata K, Shih JT, Tsai TM. Causes of ulnar tunnel syndrome: a retrospective study of 31 subjects. J Hand Surg Am. 2003;28(4):647-651. doi:10.1016/s0363-5023(03)00147-3. PMID: 12877855.
-
Patterson JM, Jaggars MM, Boyer MI. Ulnar and median nerve palsy in long-distance cyclists. A prospective study. Am J Sports Med. 2003;31(4):585-589. doi:10.1177/03635465030310041801. PMID: 12860549.
-
Akuthota V, Plastaras C, Lindberg K, Tobey J, Press J, Garvan C. The effect of long-distance bicycling on ulnar and median nerves: an electrophysiologic evaluation of cyclist palsy. Am J Sports Med. 2005;33(8):1224-1230. doi:10.1177/0363546505275131. PMID: 16000656.
-
Schreuders TA, Roebroeck ME, Jaquet JB, Hovius SE, Stam HJ. Long-term outcome of muscle strength in ulnar and median nerve injury: comparing manual muscle strength testing, grip and pinch strength dynamometers and a new intrinsic muscle strength dynamometer. J Rehabil Med. 2004;36(6):273-278. doi:10.1080/16501970410033677. PMID: 15841605.
-
Schreuders TA, Selles RW, Roebroeck ME, Stam HJ. Strength measurements of the intrinsic hand muscles: a review of the development and evaluation of the Rotterdam intrinsic hand myometer. J Hand Ther. 2006;19(4):393-401. doi:10.1197/j.jht.2006.07.024. PMID: 17056399.
-
Rixey A, Wenger D, Baffour F, Kakar S, McKenzie G. Accessory abductor digiti minimi muscle, less muscular than thought: an update on prevalence, morphology, and review of the literature. Skeletal Radiol. 2021;50(8):1687-1695. doi:10.1007/s00256-021-03728-5. PMID: 33533963.
-
Singh JP, Pun B, Chhabra A, Saraswat V. A novel case of ulnar nerve compression neuropathy with co-existing accessory flexor carpi ulnaris and accessory abductor digiti minimi. Skeletal Radiol. 2025;54(2):373-377. doi:10.1007/s00256-024-04739-8. PMID: 38949678.
-
Standring S, ed. Gray's Anatomy: The Anatomical Basis of Clinical Practice. 42nd ed. Edinburgh: Elsevier; 2021.
-
Wolfe SW, Pederson WC, Kozin SH, Cohen MS, eds. Green's Operative Hand Surgery. 8th ed. Philadelphia: Elsevier; 2022.