Avascular Tissue | Limited Intrinsic Healing | Repair Strategies
- Articular cartilage is avascular - no blood supply limits healing
- Partial thickness injuries do not heal due to no marrow access
- Full thickness defects heal with fibrocartilage (Type I collagen)
- Fibrocartilage is biomechanically inferior to hyaline cartilage
- Surgical strategies aim to restore hyaline-like tissue
- “Type II collagen in hyaline vs Type I in fibrocartilage repair
- “Chondrocytes have minimal mitotic activity in adults
- “Synovial fluid provides nutrition via diffusion
- “Subchondral bone breach necessary for any spontaneous repair
Cartilage Histology
Zonal Architecture

Avascular, aneural, alymphatic tissue. No blood supply means no inflammatory response or marrow-derived stem cells. Chondrocytes have minimal mitotic activity. Nutrition via synovial fluid diffusion only. Matrix turnover extremely slow.
Partial thickness injuries (above tidemark) have zero healing potential - cells cannot migrate, no inflammatory response. Full thickness injuries penetrating subchondral bone access marrow elements and form fibrocartilage repair tissue.
Repair tissue is fibrocartilage (Type I collagen) not hyaline (Type II). Fibrocartilage has inferior mechanical properties: less compressive stiffness, poor wear resistance, deteriorates over time under load.
All surgical interventions aim to restore hyaline-like tissue. Microfracture creates fibrocartilage. Osteochondral grafts (OATS) transplant true hyaline. ACI/MACI aim for hyaline-like regeneration with variable success.
Overview
Articular cartilage is a specialized connective tissue with unique properties optimized for load bearing and joint articulation. Its composition and structure provide excellent mechanical function but severely limit intrinsic healing capacity.
Clinical Significance
Cartilage injuries are common, affecting up to 60% of patients undergoing knee arthroscopy. The inability of cartilage to heal spontaneously leads to progressive joint degeneration and osteoarthritis. Understanding cartilage biology is essential for rational treatment selection.
Historical Perspective
Hunter's 1743 statement that "ulcerated cartilage is a troublesome thing, once destroyed it is not repaired" remains relevant. Modern surgical techniques attempt to overcome this biological limitation through various regenerative strategies.
Biology and Pathophysiology
Cartilage Structure and Composition
Articular cartilage consists of chondrocytes embedded in an extensive extracellular matrix (ECM). The ECM comprises approximately 95% of tissue volume and contains:
Collagen (10-20% wet weight): Predominantly Type II collagen arranged in zone-specific orientations. Provides tensile strength and tissue architecture. Type IX and XI collagens are also present in smaller amounts.
Proteoglycans (5-10% wet weight): Aggrecan is the major proteoglycan, bound to hyaluronic acid. Glycosaminoglycans (chondroitin sulfate, keratan sulfate) create negative charge attracting water.
Water (65-80% wet weight): Trapped by proteoglycan charge. Provides compressive stiffness through fluid pressurization.
Zonal Organization
- Depth from Surface
- 10-20%
- Collagen Orientation
- Parallel to surface
- Cell Shape
- Flat, elongated
- Function
- Shear resistance, joint lubrication
- Depth from Surface
- 40-60%
- Collagen Orientation
- Random/oblique
- Cell Shape
- Rounded
- Function
- Transition zone, shock absorption
- Depth from Surface
- 30%
- Collagen Orientation
- Perpendicular
- Cell Shape
- Columnar
- Function
- Resist compression, anchor to bone
- Depth from Surface
- Variable
- Collagen Orientation
- Into subchondral bone
- Cell Shape
- Hypertrophic
- Function
- Transition to subchondral bone
Why Partial Thickness Injuries Cannot Heal
Injuries confined to cartilage above the tidemark have no access to:
- Blood supply (no inflammatory cells)
- Bone marrow (no mesenchymal stem cells)
- Clotting factors (no fibrin scaffold)
Chondrocytes adjacent to injury have limited mitotic capacity and cannot migrate to fill defects. Proteoglycan depletion around the lesion rim leads to progressive degeneration.
The tidemark separates calcified from non-calcified cartilage. Injuries above the tidemark (partial thickness) cannot heal. Only injuries penetrating through the calcified cartilage to subchondral bone can access marrow elements for any repair response.
Full Thickness Injury Response
When injury penetrates subchondral bone, the following sequence occurs:
- Hemorrhage and clot formation - fibrin scaffold forms
- Inflammatory response - macrophages and growth factors
- MSC migration - marrow-derived stem cells populate defect
- Fibrocartilage formation - cells differentiate into fibrochondrocytes
- Type I collagen production - inferior repair tissue forms
This repair tissue is biomechanically inferior: less stiff, poor wear resistance, and tends to degenerate over time.
Differential Diagnosis
A focal chondral defect is a clinical diagnosis of exclusion — several conditions mimic its presentation (mechanical knee pain, effusion, catching) and must be distinguished because management differs entirely.
- Key Distinguishing Feature
- Discrete injury event, well-defined lesion edges
- Imaging Hallmark
- Full-thickness defect with stable shoulders on MRI
- Implication for Repair
- Candidate for marrow stimulation, OAT or ACI
- Key Distinguishing Feature
- Adolescent/young adult, insidious onset
- Imaging Hallmark
- Subchondral bone fragment +/- separation; bone oedema
- Implication for Repair
- Subchondral bone must be addressed — favours OAT/OCA, not isolated microfracture
- Key Distinguishing Feature
- Older patient, multi-compartment, malalignment
- Imaging Hallmark
- Joint-space narrowing, osteophytes, bipolar wear
- Implication for Repair
- Contraindication to focal repair; treat as OA (osteotomy/arthroplasty)
- Key Distinguishing Feature
- Sudden onset, risk factors (steroids, alcohol)
- Imaging Hallmark
- Subchondral crescent sign, geographic marrow oedema
- Implication for Repair
- Requires osteochondral allograft or arthroplasty, not cell therapy
- Key Distinguishing Feature
- Joint-line pain, positive provocative tests
- Imaging Hallmark
- Meniscal signal reaching articular surface
- Implication for Repair
- Treat meniscus; an unaddressed tear undermines any cartilage repair
Before committing to any cartilage repair, confirm a stable, well-aligned, ligament-competent knee with intact menisci. Malalignment, instability or meniscal deficiency are the commonest reasons a technically good repair fails — they must be corrected concurrently (osteotomy, ligament reconstruction, meniscal repair/transplant).
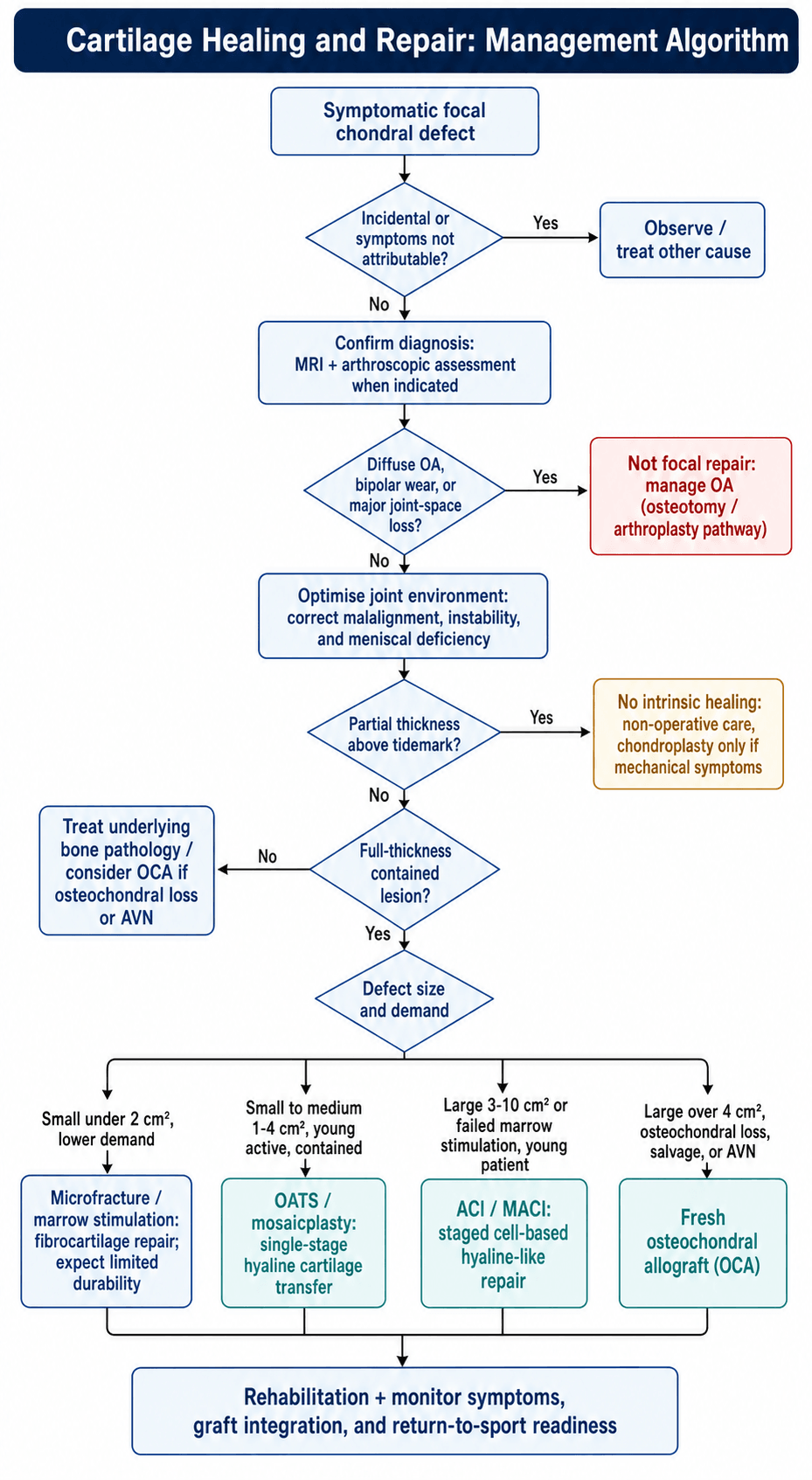
Management Algorithm
Rehabilitation After Cartilage Repair
The management algorithm ends with "rehabilitation, graft integration and return-to-sport readiness", and the durability data above hinge on it — yet cartilage-repair rehabilitation is decisive and easily overlooked, because repair tissue matures slowly and is vulnerable to premature loading.
- The maturation timeline drives everything. Repair tissue (fibrocartilage after marrow stimulation, hyaline-like after ACI/MACI) is soft and disorganised at first and remodels over roughly 12 to 18 months; rehabilitation protects it while it matures.
- Continuous passive motion (CPM) and early protected ROM. Salter's work established that CPM nourishes chondral repair tissue and promotes a more hyaline-like result than immobilisation, so early protected motion is standard after most cartilage procedures (within joint-specific limits).
- Weight-bearing is governed by the LESION LOCATION:
- Femoral condyle / tibial (weight-bearing) lesions — restricted/protected weight-bearing (touch or partial) for about 6 to 8 weeks with early full range of motion, so the repair is moved but not compressed.
- Patellofemoral (trochlea/patella) lesions — weight-bearing in extension is usually allowed, but flexion is restricted with a brace to keep shear/load off the patellofemoral repair during the vulnerable phase.
- Staged return to sport. Impact and pivoting sport are resumed deliberately late — commonly around 6 to 9 months after microfracture and 9 to 18 months after ACI/MACI or osteochondral procedures — because premature return is a leading cause of repair failure.
The single teaching point: match the weight-bearing and ROM restriction to the lesion location, and respect the long maturation window — a technically perfect repair fails if it is loaded too soon.
Q: How does weight-bearing after cartilage repair differ between a femoral condyle and a patellofemoral lesion? A: A weight-bearing (condylar/tibial) lesion is protected from compression — restricted weight-bearing for ~6 to 8 weeks with early full ROM. A patellofemoral lesion tolerates weight-bearing in extension but must have flexion restricted (braced) to unload the patellofemoral repair. Both need slow, staged return to sport over 6 to 18 months.
Why Osteochondral Allograft Is Not Rejected
The OCA option above transplants fresh donor cartilage without HLA matching or immunosuppression — surprising for an allograft, and the reason ties straight back to this topic's central theme. Because articular cartilage is avascular, aneural and alymphatic, and its dense matrix physically shields the chondrocytes from the host immune system, the cartilage is relatively immunoprivileged and is not rejected the way a vascularised organ graft would be.
- Chondrocyte viability is the currency. The transplanted chondrocytes must survive to maintain the matrix, so graft viability declines with storage time — this is why fresh grafts are used within roughly 28 days, and a viability above about 70% is the commonly cited target for a usable graft.
- Screening, not matching. Donor grafts are screened for disease transmission and size/topography-matched to restore the joint contour, but they do not require blood-group/HLA matching or immunosuppression.
- What integrates and what does not. The bone portion is a non-living scaffold that the host revascularises and remodels by creeping substitution; the cartilage does not "heal in" but delivers immediate mature hyaline function — which is why OCA suits large or osteochondral defects, salvage and AVN, where the subchondral bone must also be replaced.
Q: Why can a fresh osteochondral allograft be implanted without HLA matching or immunosuppression? A: The avascular, dense cartilage matrix shields the chondrocytes from immune recognition, so cartilage is immunoprivileged. Only disease-transmission screening and size matching are needed. The catch is chondrocyte viability, which falls with storage — hence the fresh, within-~28-day, viability-above-~70% requirement.
Clinical Relevance and Repair Strategies
Microfracture
The most commonly performed cartilage repair procedure. Creates 3-4mm holes in subchondral bone at 3-4mm intervals to access marrow elements.
Mechanism: Bone marrow bleeding into defect provides MSCs, growth factors, and fibrin scaffold for repair tissue formation.
Repair tissue: Fibrocartilage (Type I collagen) with inferior biomechanical properties.
Indications:
- Smaller defects (under 2-4 cm squared)
- Contained lesions with stable shoulders
- First-line treatment in many centers
Outcomes: Good short-term results but deterioration at 5-8 years as fibrocartilage degenerates under load.
This technique remains widely used due to simplicity and low cost.
Comparison of Repair Techniques
- Defect Size
- Under 2-4 cm squared
- Repair Tissue
- Fibrocartilage (Type I)
- Stages
- Single
- Durability
- 5-8 years good results
- Defect Size
- Under 3-4 cm squared
- Repair Tissue
- Hyaline (transferred)
- Stages
- Single
- Durability
- Good long-term if matched
- Defect Size
- Over 4 cm squared
- Repair Tissue
- Hyaline (donor)
- Stages
- Single
- Durability
- Variable, depends on viability
- Defect Size
- 2-10 cm squared
- Repair Tissue
- Hyaline-like
- Stages
- Two
- Durability
- Good 10-15 year data emerging
Selection Criteria
Microfracture: First-line for smaller defects, low cost, single stage.
OATS: Smaller defects where hyaline desired, single stage, limited by donor.
ACI/MACI: Larger defects, younger patients, willing to undergo two surgeries.
OCA: Large defects, salvage, AVN, requires fresh tissue availability.
Guidelines, Registries & Global Practice
Global Epidemiology
Focal chondral or osteochondral lesions are found in roughly 60% of knee arthroscopies, with full-thickness (ICRS grade III-IV) lesions in around 5-11%. They are most common in active patients in the third and fourth decades, and a substantial minority are associated with concurrent ligament or meniscal injury — reinforcing that cartilage damage is rarely an isolated problem.
Side-by-Side Guidance
- Position
- ACI supported for defined defects with adequate evidence and governance; arthroscopic washout not recommended for OA
- Practical Emphasis
- Cell therapy concentrated in specialist centres with audit; resist its use in established OA
- Position
- Evidence-based work groups acknowledge multiple effective options but note limited high-level comparative data
- Practical Emphasis
- Shared decision-making; technique tailored to lesion size and patient demand
- Position
- Algorithm by defect size, depth, location and patient factors; address subchondral bone and joint environment
- Practical Emphasis
- Size-based selection (marrow stimulation small, OAT small-medium, ACI/OCA large)
- Position
- Emphasise treating malalignment, instability and meniscal deficiency concurrently
- Practical Emphasis
- A repair in a hostile joint will fail — correct the environment first
Registry & Resource Notes
- Dedicated cartilage registries (e.g. the German Cartilage Registry / KnorpelRegister DGOU and national procedure registries) track repair outcomes; unlike arthroplasty, cartilage procedures are not consistently captured in joint-replacement registries.
- High-resource settings: full menu available — matrix-assisted ACI, fresh osteochondral allograft, and biologic augmentation in specialist centres.
- Limited-resource settings: marrow stimulation (microfracture/microdrilling) and osteochondral autograft dominate because they are single-stage, low-cost and need no cell-culture facility or tissue bank. Fresh allograft availability is constrained by tissue-banking infrastructure and short chondrocyte viability windows.
Controversies & Areas of Uncertainty
Subchondral plate perforation can produce intralesional osteophytes, subchondral cysts and bony overgrowth, and may compromise later procedures. Some surgeons now prefer subchondral-sparing nanofracture/microdrilling with smaller-diameter, deeper channels to reduce thermal necrosis and plate damage, but high-level comparative data remain limited.
The historical "2 cm squared" cut-off between microfracture and ACI is not firmly evidence-based. The SUMMIT RCT used a 3 cm squared threshold, while registries suggest microfracture underperforms even below 2 cm squared in high-demand patients. The true threshold is patient- and lesion-specific, not a fixed number.
Platelet-rich plasma and bone-marrow aspirate concentrate are widely used to "augment" marrow stimulation, but evidence is heterogeneous and largely low-level. No standardised preparation exists, and routine use is not yet supported by robust RCT data.
Many small, asymptomatic chondral lesions found incidentally at arthroscopy may never become symptomatic. Over-treatment is a genuine risk; the decision to intervene should be driven by symptoms attributable to the lesion, not by its mere presence on MRI.
MCQ Practice Points
Q: Why does articular cartilage have limited intrinsic healing capacity?
A: Articular cartilage is avascular, aneural, and alymphatic with low cellularity (chondrocytes comprise only 1-5% of tissue volume). Without blood supply, there is no inflammatory response or access to mesenchymal stem cells. Chondrocytes have limited proliferative capacity and are trapped in the dense ECM, unable to migrate to injury sites. This contrasts with bone which heals through vascular-mediated inflammation.
Q: What is the mechanism of cartilage repair with microfracture, and what type of repair tissue forms?
A: Microfracture creates 3-4mm deep holes through subchondral bone, allowing bone marrow blood and mesenchymal stem cells (MSCs) to access the chondral defect. A fibrin clot forms and MSCs differentiate into chondrocyte-like cells. However, the repair tissue is fibrocartilage (predominantly Type I collagen) rather than hyaline cartilage (Type II collagen), with inferior biomechanical properties and durability.
Q: What are the indications for OATS vs ACI/MACI for cartilage defects?
A: OATS (osteochondral autograft): Small contained defects (1-4 cm²), single lesion, young active patients. ACI/MACI: Larger defects (2-10 cm²), failed prior treatment, young patients. OATS provides immediate mature hyaline cartilage but is limited by donor site morbidity and available graft. ACI/MACI generates hyaline-like cartilage but requires two surgeries (harvest then implantation) and specialized cell culture facilities.
Q: What are the key differences between fibrocartilage and hyaline cartilage repair tissue?
A: Hyaline cartilage: Type II collagen (90-95%), proteoglycan-rich with organized columnar structure, superior compressive stiffness and durability. Fibrocartilage: Type I collagen predominates, disorganized fibrous structure, lower proteoglycan content, inferior biomechanical properties, prone to degeneration under repetitive loading. Clinical significance: Fibrocartilage repair (from microfracture) deteriorates after 2-5 years, while hyaline-like repair (from ACI/MACI) has better long-term durability.
Q: What is the "super clot" concept in cartilage repair?
A: The super clot involves augmenting the basic microfracture blood clot with biologics to improve repair tissue quality. Components may include: PRP (growth factors), bone marrow aspirate concentrate (BMAC) for additional MSCs, hyaluronic acid scaffold for cell retention, and fibrin glue for clot stability. The goal is to create an enhanced biologic environment that promotes differentiation toward hyaline-like cartilage rather than fibrocartilage.
At a Glance
Articular cartilage has virtually no intrinsic healing capacity due to being avascular, aneural, alymphatic, and having chondrocytes with minimal mitotic activity. Partial thickness injuries (above tidemark) cannot heal—no blood supply means no inflammatory response or marrow-derived stem cells. Full thickness injuries penetrating subchondral bone access marrow elements and form fibrocartilage (Type I collagen), which is biomechanically inferior to native hyaline cartilage (Type II collagen). Surgical repair strategies aim to restore hyaline-like tissue: microfracture produces fibrocartilage, OATS transplants true hyaline, ACI/MACI aims for hyaline-like regeneration, and osteochondral allograft provides fresh hyaline cartilage for large defects. Cartilage is 65-80% water with chondrocytes comprising only 5% of tissue volume.
AAAAWhy Cartilage Cannot Self-Repair
Hook:Four As = Four reasons cartilage cannot heal!
WATERCartilage Composition
Hook:WATER composition allows cartilage to bear load!
MOCHACartilage Repair Options
Hook:MOCHA - order your cartilage repair like coffee, from simple to complex!
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“Explain why articular cartilage has poor intrinsic healing capacity and how this influences treatment strategies.”
“A 28-year-old footballer has a 2.5 cm squared full thickness cartilage defect on the medial femoral condyle. What are your treatment options?”
“The literature is full of cartilage repair studies. How would you critically appraise the evidence, and what does it tell you about choosing between microfracture and cell-based repair?”
Why Cartilage Cannot Heal (AAAA)
- Avascular - no blood supply
- Aneural - no nerve supply
- Alymphatic - no lymphatics
- Amitotic - minimal cell division
Composition (WATER)
- Water 65-80%
- Aggrecan (proteoglycan)
- Type II collagen
- ECM 95% of volume
- Rare cells (chondrocytes 5%)
Repair Tissue Comparison
- Hyaline = Type II collagen (native)
- Fibrocartilage = Type I collagen (repair)
- Fibrocartilage biomechanically inferior
- Deteriorates under load over time
Treatment Options (MOCHA)
- Microfracture - marrow stim, fibrocartilage
- OATS - autograft, hyaline, single stage
- Cell-based (ACI/MACI) - hyaline-like
- Hyaluronic scaffolds - matrix-assisted
- Allograft (OCA) - large defects
Evidence Base
- Multicentre RCT: 80 patients with a single femoral condyle defect randomised to ACI or microfracture
- Both groups improved significantly vs baseline at 2 and 5 years
- Satisfactory results in 77% of patients in both arms at 5 years — no significant difference between techniques
- Failures rose from 1-2 at 2 years to 9 (23%) per arm at 5 years; one-third had early radiographic OA at 5 years
- No correlation between histological repair quality and clinical outcome; younger patients did better
- RCT of 144 patients with symptomatic defects 3 cm squared or larger (Outerbridge III-IV), mean lesion 4.8 cm squared
- KOOS pain and function improved significantly more with MACI than microfracture at 2 years (p=0.001)
- Treatment failures (non-responders): MACI 12.5% vs microfracture 31.9% (p=0.016)
- MRI/histology repair tissue quality good in both arms with no significant structural difference
- 5-year follow-up of the SUMMIT RCT; 128 of 144 patients continued (65 MACI, 63 microfracture)
- Superiority of MACI over microfracture in KOOS pain and function maintained at 5 years (p=0.022)
- Activities-of-daily-living advantage persisted (p=0.007); QOL and other symptoms favoured MACI but lost significance
- MRI defect fill improved in both arms with no significant between-group structural difference
- Systematic review of 28 studies, 3122 patients (6 RCTs), mean follow-up 41 months
- Microfracture reliably improves knee function within the first 24 months
- Reports on durability of that improvement were conflicting, with possible functional deterioration
- Smaller defects, younger age and good macroscopic repair quality predicted better outcomes