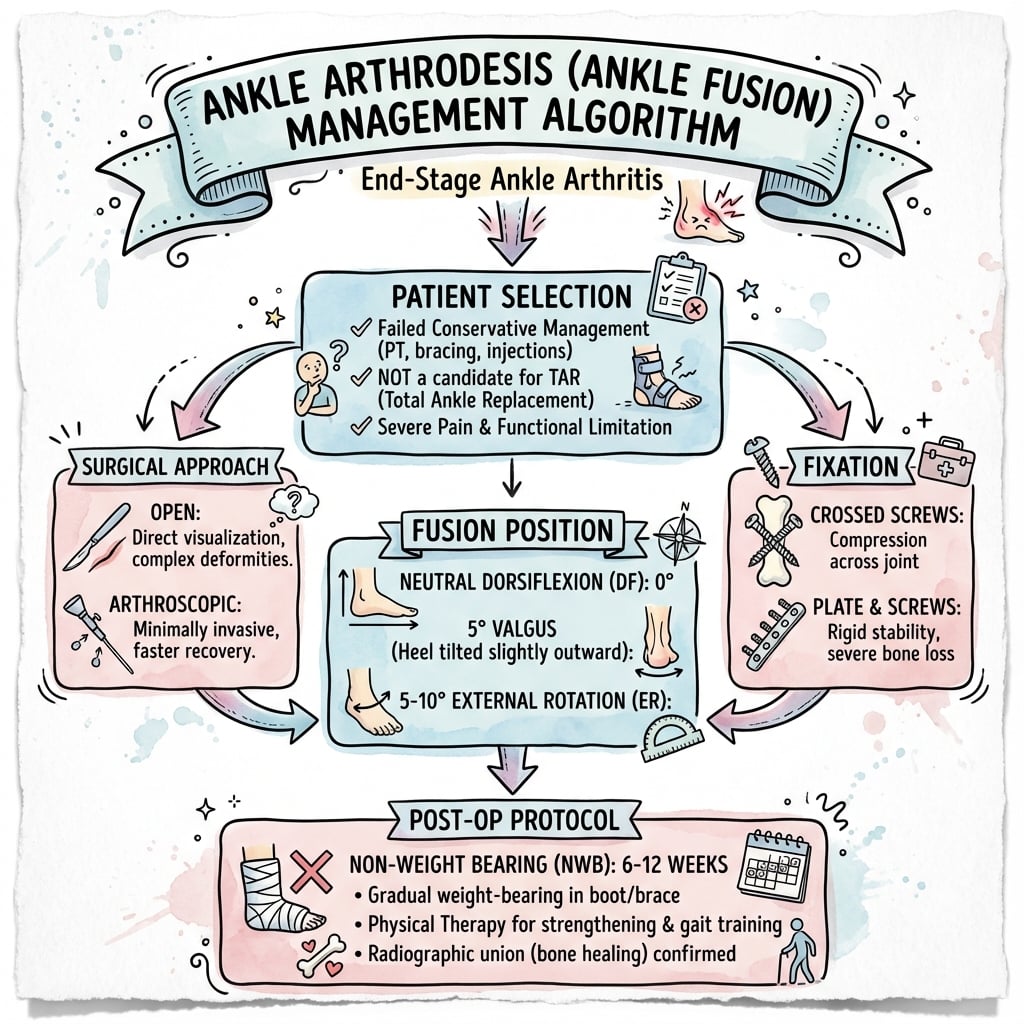
End-Stage Ankle Arthritis | Position Critical | Open vs Arthroscopic | Tibiotalocalcaneal Option
- Optimal position: Neutral dorsiflexion (5° plantar), 5° valgus, 5-10° ER (match contralateral)
- Arthroscopic: Faster recovery, similar union rates, best for non-deformed ankles
- Open: Better for deformity, bone loss, revision cases with bone grafting capability
- Union rate: 90-95% with optimal technique; malalignment increases nonunion 3-fold
- Compression critical: Minimum 250N compression across joint for reliable fusion
- “Position errors cannot be revised - get it right first time (5-5-5 rule)
- “Arthroscopic vs open debate settled: equivalent union, arthroscopic faster recovery
- “Tibiotalocalcaneal nail salvages failed ankle replacement and severe deformity
- “TARVA RCT: TAR and fusion give comparable 1-year outcomes - choice is patient-specific
Malalignment = guaranteed poor outcome. Sagittal position most critical: 5° neutral dorsiflexion (0-10° acceptable). Valgus 5° prevents varus collapse. External rotation must match contralateral side.
Post-traumatic arthritis number 1 (60% of cases). Also rheumatoid, avascular necrosis, failed ankle replacement, Charcot arthropathy. Age under 60 favors fusion over replacement.
Open vs arthroscopic not superior/inferior - patient-specific. Arthroscopic: faster recovery, less wound issues. Open: bone grafting, deformity correction, revision.
Minimum 250N compression across joint. Crossed screws provide rotation control. Plate adds compression and stability in osteoporotic bone or revision.
- Technique
- Arthroscopic
- Fixation
- 3 cannulated screws (2 lateral-medial, 1 anterior-posterior)
- Key Pearl
- Fastest recovery, back to work 10-12 weeks
- Technique
- Mini-open or open anterior
- Fixation
- Plate plus screws for compression
- Key Pearl
- Bone graft local or iliac crest if over 1cm defect
- Technique
- Tibiotalocalcaneal fusion
- Fixation
- Intramedullary hindfoot nail
- Key Pearl
- Bypass ankle, fuse through calcaneus, major salvage
- Technique
- Open anterior approach
- Fixation
- Plate with locking screws
- Key Pearl
- Bone quality critical - consider bisphosphonate holiday
Overview and Epidemiology
Ankle arthrodesis remains a gold-standard option for end-stage ankle arthritis, especially in young, active patients and those with significant deformity, and it avoids the risk of implant failure. Historically fusion showed better medium-term survivorship than early total ankle replacements, but the TARVA RCT found comparable 1-year patient-reported outcomes between fusion and modern TAR. The trade-off for fusion is permanent loss of ankle motion, increased stress on adjacent joints, and difficulty on uneven terrain.
- Age: Most patients 40-60 years at time of fusion
- Gender: Male greater than female 2:1 (trauma predominance)
- Activity: Young active patients favor fusion over replacement
- Occupation: Heavy manual workers benefit from stability
- Function: 80% satisfied despite loss of motion
- Gait: Compensatory midfoot and hip motion
- Adjacent joints: 30% develop symptomatic arthritis by 10 years
- Revision rate: roughly 7-10% at 10 years (registry and RCT data)
Anatomy and Biomechanics
Ankle Joint Anatomy
- Articular surface: 350-500mm² contact area
- Stability: Mortise and deep malleoli (intrinsic stability)
- Motion: 20° dorsiflexion, 30° plantarflexion (normal gait)
- Load: 5-6× body weight during walking, 13× running
- Tibial side: Anterior tibial artery perforators
- Talar dome: Posterior tibial and dorsalis pedis branches
- Watershed area: Central talar dome (AVN risk)
- Fusion healing: Metaphyseal bone excellent vascularity
Biomechanics After Fusion
After ankle arthrodesis, patients compensate through:
- Subtalar motion: Increased stress (15° inversion/eversion becomes 25°)
- Midfoot motion: Talonavicular and midfoot joints increase 40% motion
- Hip and knee: External rotation of hip, increased knee flexion in swing phase
- Energy expenditure: 5-10% increase in metabolic cost of walking
These compensatory mechanisms lead to adjacent joint arthritis in 30% of patients by 10 years post-fusion.
- Normal Motion
- 50° total
- After Fusion
- 0° (fused)
- Arthritis Risk
- N/A
- Normal Motion
- 30° total
- After Fusion
- Increased to 40°
- Arthritis Risk
- 30% at 10 years
- Normal Motion
- 10° total
- After Fusion
- Increased to 15°
- Arthritis Risk
- 20% at 10 years
- Normal Motion
- 5° total
- After Fusion
- Increased to 10°
- Arthritis Risk
- 15% at 10 years
Classification of Ankle Arthrodesis Types
Standard Ankle Arthrodesis

- Post-traumatic arthritis isolated to tibiotalar joint
- Rheumatoid arthritis without subtalar involvement
- AVN of talus with preserved subtalar joint
- Failed ankle replacement with good talar bone stock
- Active infection (relative, stage with antibiotics first)
- Severe peripheral vascular disease (relative)
- Charcot arthropathy (prefer tibiotalocalcaneal)
- Severe osteoporosis (relative, consider bisphosphonates)
Preserving the subtalar joint is essential - it provides 70% of hindfoot inversion/eversion. Never extend fusion to subtalar unless severely arthritic, as this doubles disability and adjacent joint stress.
FIVEOptimal Ankle Fusion Position (5-5-5 Rule)
Hook:Five-Five-Five: 5° neutral, 5° valgus, 5-10° ER - get position right because you cannot revise it!
PARTICAnkle Arthrodesis Indications
Hook:PARTIC = Participate in fusion when joint is destroyed - most common is Post-traumatic!
FASTERArthroscopic Ankle Fusion Advantages
Hook:FASTER recovery with arthroscopic fusion - but only for minimal deformity and good bone stock!
Clinical Assessment
- Pain: Location (ankle vs subtalar vs midfoot)
- Function: Walking distance, stairs, uneven ground ability
- Prior surgery: Ankle fracture, ligament reconstruction, replacement
- Medical: Diabetes (Charcot risk), RA, smoking status
- Occupation: Manual labor vs sedentary (fusion vs replacement)
- Goals: Return to work, sports, daily activities
- Gait: Antalgic, hindfoot alignment, foot progression angle
- Alignment: Weightbearing varus/valgus, forefoot supination
- ROM: Ankle (tibiotalar) vs subtalar motion isolated
- Tenderness: Joint line, subtalar, talonavicular, midfoot
- Deformity: Fixed vs flexible with hindfoot block
- Neurovascular: Posterior tibial pulse, sensation
Special Tests
- Technique
- Fluoroscopy-guided 5mL lignocaine
- Interpretation
- Pain relief greater than 80% confirms tibiotalar source
- Technique
- Lateral hindfoot wedge under heel
- Interpretation
- Corrects supination = flexible deformity, good fusion candidate
- Technique
- Sinus tarsi approach with contrast
- Interpretation
- No relief = isolated tibiotalar arthritis (good for isolated fusion)
Do not fuse ankle alone if subtalar arthritis present - this leads to persistent pain and early failure. Always:
- Examine subtalar motion separately (inversion/eversion with ankle blocked)
- Look for subtalar tenderness in sinus tarsi
- Consider CT if subtalar arthritis suspected on X-ray
- Inject subtalar separately if diagnosis unclear
If subtalar arthritis confirmed, offer tibiotalocalcaneal fusion from the start.
Differential Diagnosis of the Painful Arthritic Ankle
- Key features
- Anterior/diffuse ankle pain, stiffness, joint-line tenderness
- Discriminator
- Pain abolished by intra-articular tibiotalar injection
- Implication
- Fusion or TAR indicated
- Key features
- Sinus tarsi pain, pain on inversion/eversion with ankle held
- Discriminator
- Relief with subtalar (not tibiotalar) block
- Implication
- Subtalar fusion, not ankle fusion
- Key features
- Deep pain, risk factors (steroid, alcohol, trauma)
- Discriminator
- MRI marrow oedema/collapse; talar body involvement
- Implication
- May need TTC fusion if body collapsed
- Key features
- Polyarticular, morning stiffness, raised CRP/ESR/RF
- Discriminator
- Systemic features and serology
- Implication
- Optimise DMARDs; perioperative immunosuppression plan
- Key features
- Rest pain, warmth, effusion, fevers, raised inflammatory markers
- Discriminator
- Aspiration culture; never fuse over active infection
- Implication
- Eradicate infection first, staged fusion
- Key features
- Diabetic neuropathy, swelling, deformity, often painless
- Discriminator
- Neuropathy plus fragmentation/dislocation on imaging
- Implication
- TTC fusion/reconstruction, not standard fusion
Investigations
Imaging Protocol for Ankle Arthrodesis Planning
- AP ankle, mortise, lateral ankle (weight-bearing mandatory)
- Hindfoot alignment view (Saltzman view for varus/valgus)
- Foot AP and lateral to assess midfoot arthritis
- Degree of joint space narrowing and osteophyte formation
- Subchondral cysts and sclerosis (severity markers)
- Deformity: varus/valgus angle, tibiotalar subluxation
- Bone stock: talar dome height, previous surgery defects
- Adjacent joints: subtalar, talonavicular, midfoot
- Deformity greater than 15° (need 3D planning)
- Prior surgery with hardware (assess bone stock)
- Suspected AVN or subchondral collapse
- Planning bone graft requirements
- Bone defect size and location (quantify graft need)
- Deformity in all planes (surgical correction plan)
- Hardware position if revision case
- Subtalar and talonavicular joint status

Indications:
- Suspected talar AVN (bone marrow edema, collapse)
- Rule out infection (enhancement, fluid collections)
- Soft tissue pathology (tendon tears, masses)
- Young patient considering ankle replacement vs fusion
MRI not routinely required for straightforward arthrodesis.
- FBC, CRP, ESR: Baseline inflammatory markers (infection screen)
- HbA1c: If diabetic (target under 7% for surgery)
- Bone density: If osteoporotic appearance on X-ray
- Group and save: Standard for major joint surgery
Management Algorithm
Non-operative treatment is not curative for end-stage arthritis but delays surgery and helps patient selection. Trial for 3-6 months before offering fusion. If symptoms controlled, continue conservative; if refractory pain despite maximal non-operative treatment, proceed to surgery.
Non-Operative Treatment Options
- Analgesia: Paracetamol, NSAIDs (intermittent use)
- Topical: NSAID gel, capsaicin cream
- Steroid injection: Intra-articular (3-6 months relief)
- Viscosupplementation: Hyaluronic acid (limited evidence)
- Bracing: AFO (ankle-foot orthosis) for support and pain relief
- Footwear: Rocker-bottom sole reduces ankle motion demand
- Physiotherapy: Strengthening, gait training, activity modification
- Weight loss: 1kg loss reduces ankle load by 3-4kg
Conservative Management Pathway
- Analgesia (paracetamol + NSAID)
- AFO brace trial
- Physiotherapy referral for strengthening
- Footwear modification (rocker sole, cushioned insoles)
- Intra-articular steroid injection (fluoroscopy-guided)
- Custom-molded AFO if off-the-shelf inadequate
- Weight loss program if BMI over 30
- Consider viscosupplementation (limited evidence)
Surgical fusion indicated if:
- Pain despite maximal conservative treatment
- Functional limitation affecting quality of life
- Patient willing to accept permanent stiffness
- Medically fit for surgery
This progressive approach ensures appropriate patient selection for surgery.
Surgical Technique
Pre-operative Planning
- Union rate: 90-95% (5-10% risk nonunion requiring revision)
- Adjacent joint arthritis: 30% symptomatic at 10 years
- Infection: 2% arthroscopic, 5% open technique
- Malunion: Position critical, cannot be revised easily
- Nerve injury: Superficial peroneal nerve 2-5% (dorsal portals)
- Pain: 10-20% residual pain despite solid fusion
- Revision rate: roughly 7-10% at 10 years (registry data)
- Implants: 6.5mm or 7.0mm cannulated screws (3-4 screws) OR anterior plate with locking screws
- Arthroscopy: If arthroscopic technique, 30° scope, 4.0mm shaver, burr, curettes
- Power: Drill, reamer, sagittal saw (if open with bone cuts)
- Imaging: C-arm (AP, lateral, mortise views essential)
- Bone graft: Local bone mill OR iliac crest set if defect over 1cm
- Compression device: Interfragmentary compression clamp or use screws
Arthroscopic Ankle Arthrodesis
- Minimal deformity (under 10° in any plane)
- Good bone stock (no significant bone loss or AVN)
- Non-obese patient (BMI under 35 allows visualization)
- Isolated tibiotalar arthritis (no subtalar disease)
- Deformity over 15° (cannot correct arthroscopically)
- Severe bone loss (need structural graft)
- Prior infection (open debridement safer)
- Revision surgery (open access required)
Arthroscopic Fusion Steps
- Position: Supine on radiolucent table
- Leg holder: Thigh post at mid-thigh (allows joint distraction)
- Tourniquet: High thigh tourniquet inflated to 300mmHg
- C-arm: Position for AP, lateral, mortise views before draping
- Distraction: 10-15 pounds traction with ankle distractor (opens joint 3-5mm)
- 1cm medial to tibialis anterior tendon at joint line
- Beware saphenous nerve and vein branches
- Lateral to peroneus tertius, at joint line
- Risk: superficial peroneal nerve (identify with plantar flexion/inversion)
- Lateral to Achilles, lateral to peroneal tendons
- Used for posterior debridement and screw insertion
Confirm portal position with C-arm before enlarging.
- Debride tibial plafond: Remove all cartilage to subchondral bone with shaver and burr
- Debride talar dome: Aggressive burring to bleeding bone (critical for fusion)
- Create flat surfaces: Fish-scale appearance (bleeding cancellous bone)
- Debride medial and lateral gutters: Remove all synovium and osteophytes
- Bone graft: Mill excised bone and pack into defects for graft
Goal: Flat, congruent, bleeding bony surfaces for fusion.
- Neutral dorsiflexion (0-5° plantar flexion on lateral X-ray)
- 5° valgus hindfoot alignment (compare contralateral)
- 5-10° external rotation (match contralateral foot progression angle)
- Remove distraction, compress joint manually
- Insert 2× screws lateral malleolus to medial tibia (crossed configuration)
- Insert 1× screw anterior tibia to posterior talus (3rd screw for rotation control)
- Alternative: Add 4th screw if large patient or poor bone quality
- Confirm compression with C-arm (no joint line visible)
- Lateral malleolus to medial: Start 4cm proximal to joint, aim for medial cortex
- Anterior to posterior: Start 2cm above joint, perpendicular to fusion surface
- Use 6.5mm or 7.0mm partially threaded cannulated screws
- Compress with washer on lateral screws
- Release tourniquet, achieve hemostasis
- Close portals with single nylon suture
- Below-knee backslab (plaster or fiberglass)
- Position: Neutral ankle, slight internal rotation (matches target position)
Common errors:
- Inadequate debridement - most common cause of nonunion (must see bleeding bone)
- Equinus position - foot drops into plantar flexion during fixation (hold neutral!)
- Varus malposition - easiest to correct before final screw tightening
- Superficial peroneal nerve - identify and protect during lateral portal placement
Recovery timeline arthroscopic vs open:
- Time to union: 12 weeks vs 16 weeks
- Return to work: 10-12 weeks vs 16-20 weeks
- Hospital stay: Day case vs 2-3 days
- Wound complications: 2% vs 8%
- Union rate: 93% vs 92% (equivalent)
Main advantage is speed of recovery, not union rate.

Tibiotalocalcaneal Nail: Technique and Pitfalls
The tibiotalocalcaneal tab and the Pelton card describe TTC fusion with a retrograde intramedullary nail and mention the nail-tibial angle and interlocking screws, but the actual insertion technique and its specific pitfalls are never developed.
- Entry point and the nerve at risk. The nail is introduced retrograde through a plantar heel incision, driving a guidewire from the plantar calcaneus, through the talus, into the tibial canal. The entry is placed slightly lateral to the midline of the heel to line up with the tibial canal, and - critically - the lateral plantar nerve and vessels cross the intended entry, so careful spreading dissection (not a deep blind reamer) protects them.
- Setting alignment before locking. Because the fusion position is fixed by where the nail sits, the hindfoot must be held in the target position (neutral dorsiflexion, about 5 degrees valgus, 5-10 degrees external rotation) as the nail is passed and the interlocks placed; many nails have a built-in valgus bend to reproduce the physiological tibial-axis-to-calcaneal-axis angle. Compression is applied across both the tibiotalar and subtalar joints before final locking.
- The specific complications to anticipate. Calcaneal stress fracture at or distal to the nail tip/interlock (the Pelton series noted cortical hypertrophy there), hardware prominence at the heel (may need the nail countersunk or later removed), malalignment locked in permanently, and a higher nonunion rate than isolated fusion - reserve TTC nailing for salvage (failed TAR, Charcot, talar collapse, combined ankle-and-subtalar arthritis), not primary fusion.
Q: What are the key technical points and pitfalls of a retrograde tibiotalocalcaneal nail? A: The nail is passed retrograde from a plantar heel entry (slightly lateral of midline) through calcaneus and talus into the tibia, protecting the lateral plantar nerve and vessels at the entry. The hindfoot must be held in the fusion position (neutral DF, about 5 degrees valgus, 5-10 degrees ER) before locking - many nails have a built-in valgus bend - with compression across both joints. Anticipate calcaneal stress fracture at the nail tip, heel hardware prominence, permanent malalignment and a higher nonunion rate; it is a salvage, not a primary, procedure.
Complications
- Incidence
- 5-10%
- Risk Factors
- Smoking, malalignment, poor compression, infection
- Management
- Revision with bone graft, plate fixation, consider TTC nail
- Incidence
- 5-8%
- Risk Factors
- Inadequate position verification, loss of position during healing
- Management
- Corrective osteotomy if symptomatic (major surgery), usually observe
- Incidence
- 2-5%
- Risk Factors
- Open surgery, diabetes, steroid use, prior surgery
- Management
- Debridement, antibiotics 6 weeks, may need staged revision
- Incidence
- 3-5%
- Risk Factors
- Anterior incision, poor soft tissue, smoking
- Management
- Local wound care, VAC therapy, may need skin graft or flap
- Incidence
- 2-5%
- Risk Factors
- Superficial peroneal nerve (dorsal portals)
- Management
- Usually neuropraxia, resolves 3-6 months, neuroma excision if persistent
- Incidence
- 30% at 10 years
- Risk Factors
- Increased motion demand, malalignment
- Management
- Conservative initially (braces, injections), fusion extension if severe
- Incidence
- 10-20%
- Risk Factors
- Subtalar arthritis, midfoot arthritis, nerve injury
- Management
- Investigate source: injections, CT/MRI, treat underlying cause
- Incidence
- 5-10%
- Risk Factors
- Screw heads, plate edges
- Management
- Removal after union (12 months minimum)
- Weight-bearing X-rays at 12 weeks (if no union, repeat at 16 and 20 weeks)
- CT scan if X-ray unclear (assess union in all planes)
- Blood tests: CRP, ESR (rule out infection)
- Consider aspiration if elevated inflammatory markers
- Aseptic nonunion, good position: Revision screws + iliac crest bone graft
- Aseptic nonunion, malposition: Corrective osteotomy + rigid plate fixation
- Infected nonunion: Staged - debridement + antibiotic spacer, then TTC nail after infection cleared
- Atrophic nonunion, bone loss: TTC nail with structural bone graft
Success rate revision arthrodesis: 70-80% (lower than primary).
Adjacent Joint Arthritis
- Subtalar arthritis: 30% symptomatic at 10 years
- Talonavicular: 20% at 10 years
- Midfoot stress: 15% at 10 years
Increased motion demand on adjacent joints (subtalar increases motion 40%, talonavicular 50%). Worse with malalignment - varus accelerates lateral column stress.
Usually conservative (bracing, injections). If severe and disabling, consider fusion extension (pantalar fusion = complete hindfoot stiffness).
PAINSAnkle Arthrodesis Complications
Hook:Ankle fusion causes PAINS - position malunion and adjacent joint arthritis are the main long-term issues!
Postoperative Care and Rehabilitation
Arthroscopic Fusion Rehabilitation
- Below-knee backslab in neutral position
- Elevate leg (foot higher than heart) for 48 hours
- Ice packs 20 minutes every 2 hours while awake
- Analgesia: Paracetamol + oxycodone, transition to oral day 1
- DVT prophylaxis: LMWH (enoxaparin 40mg daily) for 2 weeks
- Mobilize non-weight-bearing with crutches before discharge
- Discharge day 0-1 for arthroscopic, day 2-3 for open
- Strict non-weight-bearing (crutches, knee scooter)
- Convert backslab to fiberglass cast at 2 weeks (if wounds healed)
- Remove sutures 14 days (open), 10 days (arthroscopic)
- Continue DVT prophylaxis until mobile
- Physiotherapy: Quadriceps strengthening, core stability
- X-ray at 6 weeks (AP, lateral, mortise)
- If early callus forming, transition to weight-bearing boot
- If no callus, continue cast and non-weight-bearing
- Physiotherapy: Hip and knee ROM, trunk strengthening
- X-ray at 12 weeks (assess union)
- If bridging bone 3/4 cortices, allow full weight-bearing
- Transition from boot to supportive shoe with rocker sole
- Physiotherapy: Gait retraining, balance, proprioception
- Return to sedentary work 10-12 weeks (arthroscopic), 16 weeks (open)
- X-ray at 6 months (confirm solid union)
- Remove hardware if prominent and causing pain (after 12 months minimum)
- Return to full activities including manual labor
- Ongoing: Subtalar and midfoot stretching to preserve motion
Union assessment timeline:
- 6 weeks: Early callus (transition to boot if present)
- 12 weeks: Bridging bone 3/4 cortices (full weight-bearing)
- 6 months: Complete remodeling (return to full activity)
Do NOT advance weight-bearing without radiographic evidence of healing - premature loading causes nonunion.
- Maintain quadriceps strength (straight leg raises)
- Core stability and trunk control
- Contralateral leg strengthening
- Progressive weight-bearing gait training
- Hip and knee ROM maintenance
- Subtalar and midfoot mobility
- Gait optimization with rocker-sole shoes
- Balance and proprioception
- Return to activity-specific training
- Increasing pain at 6-12 weeks: Suggests nonunion (X-ray + CT)
- Wound drainage: Infection until proven otherwise (urgent review)
- Loss of position: Cast loosening, repeat X-ray
- Calf pain/swelling: DVT (urgent Doppler ultrasound)
- Numbness/tingling: Nerve compression or neuropathy
- New midfoot pain: Stress reaction (reduce loading)
Footwear and Orthotic Optimisation
The rehabilitation and biomechanics sections repeatedly prescribe a rocker-sole shoe and describe the gait compensation for a stiff ankle, but why these footwear modifications work - and the companion SACH heel - is never explained.
- Rocker-bottom sole - substituting for lost sagittal motion. A fused ankle cannot dorsiflex or plantarflex, so the foot cannot roll over during stance. A rocker-bottom (rigid-rocker) sole moves the roll-over point forward and lets the shoe pivot, restoring a smooth heel-to-toe progression without ankle motion. This is the single most useful footwear modification after an ankle (or any hindfoot) fusion and reduces the compensatory strain thrown onto the midfoot.
- SACH heel / cushioned heel - substituting for lost plantarflexion at heel strike. Normally the ankle plantarflexes to lower the forefoot after heel strike; a fused ankle cannot, so heel strike is abrupt. A SACH (Solid-Ankle-Cushion-Heel) or cushioned heel wedge compresses at heel strike to simulate that plantarflexion and absorb shock, smoothing initial contact and offloading the knee.
- The rest of the package. A stiff or carbon shank stops the shoe bending at the now stress-loaded midfoot, and a custom insole or AFO accommodates any residual deformity and offloads a painful adjacent (subtalar/midfoot) joint. These modifications are lifelong, not temporary, and are a mainstay of managing the near-universal adjacent-joint stress that follows fusion.
Q: What footwear modifications optimise gait after ankle arthrodesis and why? A: A rocker-bottom sole moves the roll-over point forward to restore heel-to-toe progression without the ankle motion the fusion removed; a SACH (solid-ankle-cushion-heel) or cushioned heel compresses at heel strike to simulate the lost plantarflexion and absorb shock; and a stiff/carbon shank prevents compensatory bending at the overloaded midfoot. With a custom insole or AFO for any residual deformity, these lifelong modifications are a mainstay of managing the adjacent-joint stress that follows fusion.
Outcomes and Prognosis

Functional Outcomes
- Pre-operative
- 8/10
- 2 Years Post-op
- 2/10
- 10 Years Post-op
- 3/10 (adjacent joint arthritis)
- Pre-operative
- 35/100
- 2 Years Post-op
- 75/100
- 10 Years Post-op
- 70/100
- Pre-operative
- 40/100
- 2 Years Post-op
- 70/100
- 10 Years Post-op
- 65/100
- Pre-operative
- Unable
- 2 Years Post-op
- 85% return
- 10 Years Post-op
- 80% still working
- Union achieved: 95% satisfied vs 40% if nonunion
- Position correct: Neutral sagittal critical (equinus = dissatisfied)
- Pain relief: 80% have significant pain reduction
- Realistic expectations: Understanding stiffness and adjacent joint risk
- Malunion (especially equinus)
- Nonunion requiring revision
- Adjacent joint arthritis (30% at 10 years)
- Persistent pain despite solid fusion
Comparison: Fusion vs Total Ankle Replacement
- Ankle Arthrodesis
- Equivalent (TARVA RCT)
- Total Ankle Replacement
- Equivalent (TARVA RCT)
- Ankle Arthrodesis
- Nonunion (around 7% symptomatic), VTE
- Total Ankle Replacement
- Wound healing, nerve injury, late loosening/wear
- Ankle Arthrodesis
- Younger / high-demand favoured
- Total Ankle Replacement
- Older / lower-demand favoured
- Ankle Arthrodesis
- Heavy labour possible
- Total Ankle Replacement
- Light-to-moderate activity
- Ankle Arthrodesis
- Near-universal ipsilateral hindfoot/midfoot long term
- Total Ankle Replacement
- Likely less (motion preserved) - long-term data limited
- Ankle Arthrodesis
- Stiff ankle, compensatory motion
- Total Ankle Replacement
- Near-normal ankle motion
The landmark TARVA RCT (Goldberg 2022, Ann Intern Med) randomised 303 patients and found no clinically significant difference in the MOXFQ walking/standing score at 1 year. The historical claim of clear fusion superiority no longer holds for modern fixed-bearing implants - decide by patient age, demand, deformity, bone quality and complication tolerance.
10-year outcomes:
- Revision roughly 7-10%: Mainly nonunion and symptomatic malunion (registry/RCT data)
- Adjacent joint arthritis: 30% symptomatic subtalar arthritis requiring intervention
- Patient satisfaction: 80% still satisfied despite stiffness (pain relief dominant factor)
- Function: Most patients return to work and activities, but struggle with uneven ground
Counsel patients: Ankle fusion is durable and reliable, but not normal - permanent stiffness and increased adjacent joint stress are the trade-offs for pain relief and stability.
Guidelines, Registries & Global Practice
- Leading cause: Post-traumatic arthritis (around 60-80%) - unlike hip/knee, primary OA is uncommon
- Age: Typically 40-60 years, a decade younger than arthroplasty cohorts
- Sex: Male predominance (trauma-driven), roughly 2:1
- Burden: End-stage ankle OA carries disability comparable to end-stage hip OA
- Joint registries (e.g. NJR UK, AOANJRR Australia, SHAR Sweden) primarily track total ankle replacement, against which fusion is the historical comparator
- Fusion has historically shown lower medium-term revision than first/second-generation TAR
- Modern third-generation implants are narrowing this gap (see TARVA RCT)
- Reliable population-level fusion-specific revision data remain limited - most evidence is cohort/RCT
Society Guidance, Side by Side
- Position on fusion vs TAR
- Both accepted; TAR increasingly favoured in older, lower-demand, well-aligned ankles
- Practical emphasis
- Patient selection and deformity correction
- Position on fusion vs TAR
- Fusion remains workhorse; TAR in selected patients at specialist centres
- Practical emphasis
- Centralisation of TAR, MDT decision-making
- Position on fusion vs TAR
- Supports informed shared decision-making, citing TARVA equivalence at 1 year
- Practical emphasis
- Realistic counselling on trade-offs
- Position on fusion vs TAR
- Technique-focused: rigid internal fixation and optimal position are paramount
- Practical emphasis
- Compression, alignment, stable constructs
High-resource settings: Ready access to arthroscopic equipment, total ankle replacement, hindfoot nails, CT planning and bone-graft substitutes; greater use of arthroscopic fusion and TAR.
Limited-resource settings: Open fusion with crossed screws or compression external fixation predominates; arthroscopy and TAR are often unavailable. Fusion remains the dependable, low-cost, durable solution requiring no implant supply chain - a key reason it stays the global default for young, high-demand and neglected/post-traumatic ankles.
Medicolegal and Consent Essentials
document intra-operative position verification in all planes (fluoroscopy) and counsel pre-operatively that position is permanent and cannot easily be revised.
document smoking status and cessation advice, quote a roughly 5-10% nonunion risk (around 7% symptomatic in the TARVA RCT), and record the compression technique used.
counsel explicitly that ipsilateral hindfoot/midfoot degeneration is near-universal long term (Coester) and may require further surgery.
document antibiotic prophylaxis, wound-care and follow-up plans, and thromboprophylaxis (fusion carried higher thromboembolism than TAR in TARVA).
Controversies and Areas of Uncertainty
The central debate. The TARVA RCT (Goldberg 2022) found no clinically significant difference in patient-reported outcome at 1 year, challenging the long-held assumption of fusion superiority. Open questions: long-term implant survivorship, who benefits most from each, and whether motion preservation truly reduces adjacent-joint arthritis in the long run.
Comparative series favour arthroscopic for faster recovery and fewer wound problems, but there is no large RCT and case selection (minimal deformity) biases results. The limit of correctable deformity arthroscopically is debated; experienced surgeons push beyond the classic 10-15° threshold.
Crossed screws, anterior plating, posterior blade plate and external fixation all achieve high union. No construct is proven superior in well-aligned ankles; plates/external fixation are favoured for poor bone, deformity and revision. The minimum compression needed is an estimate, not a hard rule.
Routine use of BMP, bone-stimulators (PEMF/ultrasound), PRP and graft substitutes for primary fusion is not supported by high-level evidence. Reserve adjuncts for high-risk (smokers, diabetics, revision) cases, where benefit is plausible but unproven.
State the position honestly: "The evidence is evolving." Cite TARVA as the landmark RCT showing equivalence at 1 year, acknowledge the absence of RCT data for arthroscopic vs open, and frame your answer around patient-specific decision-making (age, demand, deformity, bone quality, infection history) rather than a single "right" answer. Examiners reward balanced, evidence-aware reasoning over dogma.
MCQ Practice Points
Q: What is the most common indication for ankle arthrodesis worldwide? A: Post-traumatic arthritis (around 60% of cases), typically following pilon fractures, malunited ankle fractures, or severe ligamentous injuries. Other indications include rheumatoid/inflammatory arthritis, AVN of the talus, failed total ankle replacement, and Charcot arthropathy. The trauma predominance distinguishes the ankle from the hip and knee, where primary OA dominates.
Q: What is the optimal sagittal plane position for ankle arthrodesis and why? A: Neutral to 5° plantar flexion (acceptable range 0-10° plantar flexion). This allows normal heel strike in gait. Equinus over 10° causes inability to heel strike, leading to knee hyperextension, back pain, and patient dissatisfaction. Sagittal position is the most critical plane - errors cannot be revised and guarantee poor outcomes.
Q: What are the advantages of arthroscopic ankle arthrodesis compared to open technique? A: Faster recovery and fewer wound complications, with equivalent union rates. Arthroscopic: 93% union, 12 weeks to union, 10-12 weeks return to work, 2% infection. Open: 92% union, 16 weeks to union, 16-20 weeks return to work, 5% infection. However, arthroscopic requires minimal deformity (under 10°) and good bone stock - open allows bone grafting and deformity correction.
Q: What is the incidence and timeline of adjacent joint arthritis after ankle arthrodesis? A: 30% symptomatic at 10 years (subtalar most common, followed by talonavicular). Radiographic changes occur in nearly 100% by 20 years, but only 30-35% become symptomatic requiring intervention. Mechanism is increased motion demand on adjacent joints - subtalar motion increases 40%, talonavicular 50%. Malalignment accelerates arthritis development.
Q: What are the main reasons for revision after ankle arthrodesis and how does it compare with replacement? A: Registry series report roughly 7-10% revision at 10 years, historically lower than total ankle replacement. Main reasons: nonunion (smoking, inadequate compression, infection) and symptomatic malunion (position error, especially equinus). The landmark TARVA RCT found comparable 1-year patient-reported outcomes between fusion and TAR, with a 7% symptomatic nonunion rate after fusion, so the historical survivorship gap is narrowing with modern implants.
Q: What did the key comparative study of arthroscopic vs open ankle fusion show? A: Townshend et al 2013 (JBJS Am), a two-centre comparative series of 30 arthroscopic vs 30 open fusions, found both groups improved significantly, with greater Ankle Osteoarthritis Scale improvement at 1 and 2 years and a shorter hospital stay in the arthroscopic group; complications, surgical time and radiographic alignment were similar. Conclusion: arthroscopic fusion gives at least equivalent outcome with faster recovery in suitable (non-deformed) ankles.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 45-year-old male tradie presents with severe ankle pain limiting his ability to work. He has post-traumatic arthritis following a pilon fracture 5 years ago. X-rays show complete loss of joint space, subchondral cysts, and minimal deformity (5° valgus). His subtalar joint appears normal on X-ray. He asks about ankle replacement vs fusion. What is your assessment and management?”
“You are performing an arthroscopic ankle arthrodesis. Walk me through your technique, with particular emphasis on achieving optimal position and fixation.”
“A 50-year-old woman underwent ankle arthrodesis 6 months ago. She continues to have pain with weight-bearing. X-rays show no bridging bone and lucency around the screws. She is a smoker. How do you manage this?”
Key Indications
- Post-traumatic arthritis = 60% (most common, young active patients)
- Rheumatoid arthritis = 15% (severe joint destruction)
- Failed total ankle replacement = 8% (salvage procedure)
- Charcot arthropathy = tibiotalocalcaneal fusion (hindfoot nail)
Position (5-5-5 Rule)
- Neutral dorsiflexion = 0-5° plantar flexion (sagittal most critical)
- 5° valgus hindfoot alignment (prevents varus collapse)
- 5-10° external rotation = match contralateral side
- Equinus over 10° = worst malposition (cannot heel strike, knee pain)
Technique Selection
- Arthroscopic = minimal deformity under 10°, good bone stock, faster recovery
- Open = deformity over 10°, bone loss, revision, need bone grafting
- Tibiotalocalcaneal = failed TAR, Charcot, severe bone loss (hindfoot nail)
- Union rate equivalent: 93% arthroscopic vs 92% open
Surgical Pearls
- Debridement critical = bleeding cancellous bone fish-scale appearance
- Compression minimum 250N = crossed screws with washers or plate
- Verify position before final fixation = cannot revise after fusion heals
- Protect superficial peroneal nerve = identify before lateral portal (arthroscopic)
Complications
- Nonunion 5-10% = smoking cessation mandatory, rigid fixation, bone graft
- Malunion 5-8% = position verification critical, equinus worst error
- Adjacent joint arthritis 30% at 10 years = counsel pre-operatively
- Infection 2-5% = arthroscopic lower risk than open (2% vs 5%)
Evidence Base and Key Trials
Arthroscopic vs Open Ankle Arthrodesis (Multicentre Comparative Series)
- Two-centre comparative case series: 30 arthroscopic vs 30 open fusions, 2-year follow-up
- Both groups significantly improved Ankle Osteoarthritis Scale and SF-36 physical scores
- Arthroscopic group had significantly greater AOS improvement at 1 and 2 years
- Shorter hospital stay in the arthroscopic group
- Complications, surgical time and radiographic alignment similar between groups
Optimum Position of Ankle Arthrodesis (Landmark Gait Study)
- Biomechanical gait analysis of 19 patients followed mean 10.4 years after ankle fusion
- Plantar-flexed fusion was associated with genu recurvatum (knee hyperextension)
- Medial collateral ligament laxity noted in 12 of 19 patients (63%)
- Valgus position gave more normal gait, particularly on uneven ground
- Defined the optimum position: neutral flexion, 0-5° valgus, 5-10° external rotation
Long-Term Adjacent-Joint Arthritis After Ankle Fusion
- Longest follow-up series to date: 23 isolated fusions for post-traumatic arthritis, mean 22 years
- Ipsilateral subtalar, talonavicular, calcaneocuboid, naviculocuneiform, TMT and first MTP arthritis all significantly worse than the contralateral side (each p less than 0.01)
- No excess osteoarthritis in the ipsilateral knee versus contralateral
- Involved foot consistently more symptomatic for activity limitation, pain and disability (p less than 0.0001)
- Foot pain, not knee pain, was the dominant long-term functional limitation
TARVA Trial - Total Ankle Replacement vs Arthrodesis (RCT)
- First multicentre RCT (17 UK centres): 303 patients aged 50-85 with end-stage ankle OA randomised to TAR or fusion
- Both groups improved on the MOXFQ walking/standing score at 52 weeks
- No clinically or statistically significant difference between TAR and fusion (adjusted difference -5.6, 95% CI -12.5 to 1.4)
- Similar total adverse events (109 vs 104) but different profiles: more wound and nerve problems with TAR, more thromboembolism and nonunion with fusion
- Symptomatic nonunion rate after fusion was 7%; post-hoc analysis favoured fixed-bearing TAR
Tibiotalocalcaneal Fusion with Retrograde Intramedullary Nail
- Single-surgeon series of 33 consecutive TTC fusions stabilised with a dynamically locked retrograde IM nail
- Union in 29 of 33 feet (88%) at a mean of 3.7 months
- Indications were complex hindfoot disease: Charcot, talar osteonecrosis, combined ankle/subtalar arthritis and failed total ankle arthroplasty
- Cortical hypertrophy at the nail tip or proximal interlock in roughly half (13 of 27)
- A higher nail-tibial angle trended toward higher nonunion
Perioperative Complications - Fusion vs Replacement (NSQIP)
- ACS-NSQIP database study, 2012-2017: 1214 patients (1027 TAR, 187 ankle fusion)
- Fusion patients were younger, heavier and more often had insulin-dependent diabetes
- Multivariate analysis: ankle fusion independently associated with adverse perioperative outcomes (p = 0.049)
- Fusion carried higher rates of deep surgical site infection and reoperation
- No difference between groups in superficial infection, wound dehiscence or 30-day readmission