Progressive Cartilage Loss | Biomechanical Overload | Non-operative to Total Knee Arthroplasty
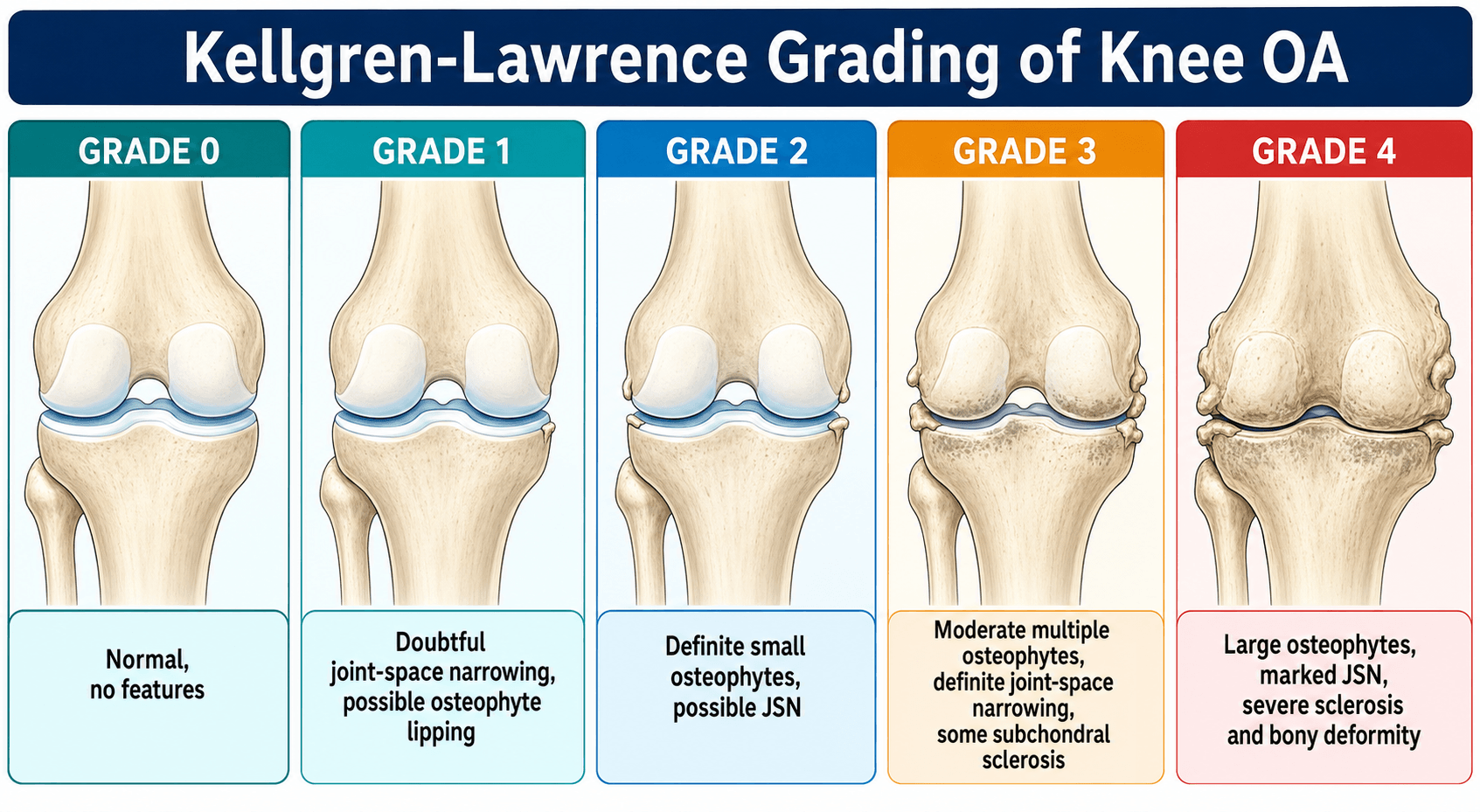
- Kellgren-Lawrence grading (0-4) guides treatment escalation
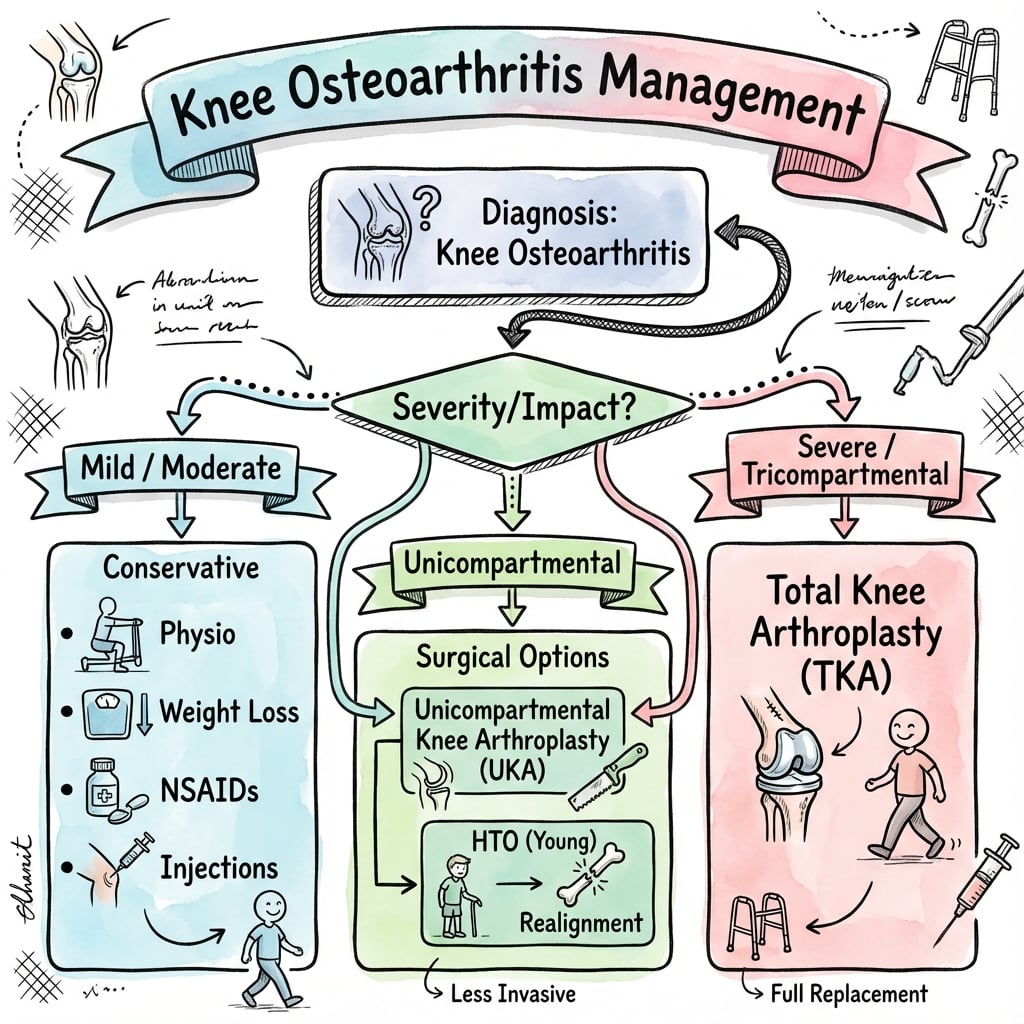
- Non-operative management is first-line for all patients: weight loss, physiotherapy, analgesia
- High tibial osteotomy (HTO) for young patients (under 60) with isolated medial OA and varus malalignment
- Unicompartmental knee arthroplasty (UKA) requires intact ACL, opposite compartment, and patellofemoral joint
- Total knee arthroplasty (TKA) is gold standard for end-stage tricompartmental OA failing conservative measures
- “Registry data (NJR, AJRR, AOANJRR): cemented TKA shows reliable long-term survivorship
- “Oxford Knee Score: validated patient-reported outcome measure (12-60 scale)
- “Mechanical axis: hip-knee-ankle alignment critical for HTO and TKA longevity
- “WOMAC score: Western Ontario McMaster Universities Arthritis Index - validated OA outcome tool
Progressive cartilage loss leads to three changes: 1) Subchondral sclerosis, 2) Osteophyte formation, 3) Joint space narrowing. Inflammatory cytokines (IL-1, TNF-alpha) drive chondrocyte apoptosis.
Kellgren-Lawrence (radiographic) versus Outerbridge (arthroscopic). K-L grades 0-4 based on osteophytes and narrowing. Outerbridge grades 1-4 based on cartilage surface changes at arthroscopy.
Age and compartment involvement determine surgery. Young (under 60) with isolated medial OA: HTO. Middle-aged with unicompartmental OA and intact ACL: UKA. Older or tricompartmental: TKA.
BMI greater than 30 = 4x risk. Every 5kg weight loss = 20% reduction in knee OA progression. TKA survivorship: approximately 95% at 10 years, 80-85% at 20 years (national registries).
- Radiographic Grade
- K-L Grade 1-2
- Treatment
- Non-operative: weight loss, PT, NSAIDs, injections
- Key Pearl
- Minimum 6 months trial before surgery
- Radiographic Grade
- K-L Grade 3 medial only
- Treatment
- High tibial osteotomy (HTO)
- Key Pearl
- Requires lateral compartment Outerbridge 0-1
- Radiographic Grade
- K-L Grade 3-4 single compartment
- Treatment
- Unicompartmental knee arthroplasty (UKA)
- Key Pearl
- Intact ACL mandatory, faster recovery than TKA
- Radiographic Grade
- K-L Grade 4
- Treatment
- Total knee arthroplasty (TKA)
- Key Pearl
- Gold standard, 95% survival at 10 years
Overview and Epidemiology
Knee osteoarthritis (OA) is the most common articular disorder worldwide and a leading cause of disability in older adults. It represents a final common pathway of cartilage failure resulting from biomechanical stress exceeding the joint's repair capacity.
Knee OA is the leading indication for total knee arthroplasty worldwide and a top global cause of years lived with disability. Understanding the spectrum from early conservative management to advanced reconstructive options is essential for the Orthopaedic exam.
- Prevalence: approximately 10% symptomatic in adults over 60; radiographic OA far higher
- Global burden: knee OA affects an estimated 250-350 million people worldwide
- Gender: female to male ratio approximately 2:1, rising after menopause
- Age: incidence increases sharply after age 50
- Disability: a leading global cause of years lived with disability (GBD studies)
- Rising incidence: driven by ageing populations and the global obesity epidemic
- Workforce: major cause of work disability and early retirement in over 50s
- Surgical volume: TKA is among the most common elective orthopaedic procedures globally
Pathophysiology and Biomechanics
Modern understanding: Knee OA is an active disease process involving inflammatory cytokines (IL-1, TNF-alpha), matrix metalloproteinases (MMPs), and altered chondrocyte metabolism. It is not simple mechanical wear.
The Pathophysiological Cascade
Disease Progression
Chondrocyte stress: Mechanical overload or injury triggers cytokine release (IL-1, TNF-alpha). Chondrocytes increase MMP production, degrading collagen and proteoglycans. Cartilage softening (Outerbridge Grade 1-2).
Progressive loss: Fibrillation and fissuring of articular cartilage. Subchondral bone exposed in focal areas. Inflammatory mediators persist. Synovitis develops (secondary inflammation).
Subchondral sclerosis: Increased bone density as stress transfers to subchondral plate. Osteophyte formation at joint margins (attempt at stability). Bone marrow lesions (oedema on MRI).
Bone-on-bone: Complete cartilage loss. Severe subchondral sclerosis. Large marginal osteophytes. Joint space collapse. Deformity (varus/valgus). Subchondral cysts.
Biomechanical Factors
- Mechanism
- Shifts load medially, 3-4x increased medial stress
- Clinical Consequence
- Medial compartment OA progression, lateral thrust gait
- Mechanism
- Every 1kg body weight = 3-4kg knee force with walking
- Clinical Consequence
- 4x OA risk, accelerated progression
- Mechanism
- Loss of shock absorption and load distribution
- Clinical Consequence
- Post-meniscectomy OA in 30-50% by 10 years
- Mechanism
- Anteroposterior instability, altered kinematics
- Clinical Consequence
- 5-10x increased OA risk by 15 years post-injury
Classification Systems
Kellgren-Lawrence Radiographic Classification
The gold standard for grading knee OA severity on plain radiographs. Used globally for research and clinical decision-making.
- Radiographic Features
- Normal joint
- Clinical Correlation
- No symptoms
- Treatment
- Nil
- Radiographic Features
- Doubtful osteophytes
- Clinical Correlation
- Minimal symptoms
- Treatment
- Observation, activity modification
- Radiographic Features
- Definite osteophytes, possible narrowing
- Clinical Correlation
- Mild-moderate pain, stiffness
- Treatment
- Weight loss, PT, NSAIDs, injections
- Radiographic Features
- Moderate narrowing, multiple osteophytes
- Clinical Correlation
- Moderate pain, function limited
- Treatment
- Consider HTO/UKA if young, otherwise TKA
- Radiographic Features
- Severe narrowing, bone-on-bone, sclerosis
- Clinical Correlation
- Severe pain at rest, major disability
- Treatment
- TKA primary option
Grade 3: Moderate joint space narrowing (50% loss) with moderate osteophytes. Grade 4: Severe narrowing (bone-on-bone) with large osteophytes and subchondral sclerosis. The key difference is complete versus incomplete joint space loss.
Clinical Assessment
- Pain: Insidious onset, activity-related, worse with stairs/squatting
- Stiffness: Morning stiffness under 30 minutes (versus RA)
- Function: Walking distance, stairs, ADLs, night pain (severe)
- Mechanical symptoms: Locking (loose bodies), giving way (weakness)
- Risk factors: Obesity, previous trauma/surgery, occupation
- Gait: Antalgic, varus/valgus thrust, Trendelenburg
- Alignment: Standing mechanical axis (varus/valgus deformity)
- Effusion: Joint swelling, warmth (synovitis)
- Range of motion: Flexion (normal 0-135°), extension lag
- Stability: Varus/valgus stress, anterior drawer (ACL for UKA)
- Patellofemoral: Crepitus, tenderness, apprehension
Acute monoarthritis (septic arthritis, gout), systemic symptoms (fever, weight loss = malignancy/infection), rapid progression (inflammatory arthritis, avascular necrosis), young patient under 40 (secondary OA, metabolic disease). Investigate with bloods (ESR, CRP, urate) and consider aspiration.
Differential Diagnosis
- Discriminating Features
- Insidious, activity-related pain; morning stiffness under 30 min; mechanical symptoms
- Key Investigation
- Weight-bearing radiographs (narrowing, osteophytes, sclerosis)
- Discriminating Features
- Polyarticular, symmetrical; prolonged morning stiffness over 1 hour; warmth, systemic features
- Key Investigation
- RF, anti-CCP, ESR/CRP; erosive periarticular changes
- Discriminating Features
- Acute hot swollen joint; sudden onset; chondrocalcinosis (CPPD)
- Key Investigation
- Joint aspiration: negatively (urate) or positively (CPPD) birefringent crystals
- Discriminating Features
- Hot, exquisitely painful joint; fever; refusal to weight-bear; unwell
- Key Investigation
- Urgent aspiration (WCC, Gram stain, culture); ESR/CRP
- Discriminating Features
- Sudden severe pain (often older woman, SPONK); focal medial femoral condyle
- Key Investigation
- MRI (subchondral oedema, crescent sign) - normal early radiograph
- Discriminating Features
- Groin/thigh pain, limited hip rotation, normal knee exam
- Key Investigation
- Hip radiograph and examination
- Discriminating Features
- Mechanical locking, joint-line tenderness, often younger; OA may coexist
- Key Investigation
- MRI; correlate with weight-bearing radiographs
Outcome Measures
- Domains
- Pain and function (12 questions)
- Range
- 12-60 (12 best)
- Clinical Use
- Validated for pre/post-TKA comparison
- Domains
- Pain, stiffness, function (24 items)
- Range
- 0-96 (0 best)
- Clinical Use
- Gold standard for OA research
- Domains
- 5 subscales including QoL, sport
- Range
- 0-100 (100 best)
- Clinical Use
- Comprehensive, used in younger patients
Investigations
Imaging Protocol
Weight-bearing AP and lateral, skyline patella, long-leg alignment. AP shows joint space narrowing, osteophytes, sclerosis. Skyline assesses patellofemoral joint. Long-leg view: mechanical axis for pre-operative planning.
For unclear diagnosis, pre-HTO planning, or assessing meniscal/ligamentous status. Shows cartilage loss (grading), bone marrow oedema (subchondral lesions), meniscal tears, ACL integrity. Not routine for OA diagnosis.
CT-based alignment increasingly used for robotic TKA and complex deformity cases. Provides 3D reconstruction, precise mechanical axis, bone stock assessment.
Bloods: ESR, CRP (elevated in inflammatory arthritis), urate (gout), RF/anti-CCP (RA). Aspiration: If suspecting septic arthritis or crystal arthropathy. Cell count, Gram stain, culture, crystals.

Radiographic Severity Does Not Equal Pain (Pain Phenotypes)
The Kellgren-Lawrence EvidenceCard's own stated limitation is that it "correlates imperfectly with symptoms", and the topic notes that 10-15% of well-performed TKAs remain dissatisfied - but WHY radiographic grade and pain diverge, and what to do about it, is never developed.
- The discordance is real and large. Many people with K-L Grade 3-4 radiographic OA have little or no pain, while others with only mild radiographic change are severely symptomatic. Structural severity explains only a modest part of the pain.
- Why pain and structure diverge. Pain in knee OA is multifactorial: synovitis and effusion, bone marrow lesions and subchondral bone change, and - importantly - central sensitisation (amplified central pain processing), alongside psychological factors (depression, anxiety, pain catastrophising) and low self-efficacy. A subgroup has a neuropathic-like / centrally-sensitised pain phenotype that responds poorly to a purely mechanical (structural) treatment.
- Why it matters clinically. Operating on a radiograph rather than on a symptomatic, structurally-concordant patient is a major cause of the dissatisfied TKA. Treat the patient, not the X-ray: correlate the radiographic pattern with the pain location and mechanical symptoms, screen for central sensitisation and psychological distress before surgery (e.g. pain-catastrophising and mood tools), and address the central component (education, exercise, duloxetine for a centrally-mediated component) rather than only escalating structural intervention.
Q: Why does radiographic OA severity correlate poorly with pain, and how does this change management? A: Structural grade explains only part of the pain - synovitis, bone marrow lesions, central sensitisation and psychological factors (depression, catastrophising) all contribute, and a centrally-sensitised pain phenotype responds poorly to mechanical treatment. So you treat the patient not the X-ray: confirm the pain is concordant with the structural disease, screen for central sensitisation and psychological distress before arthroplasty (a leading driver of the ~15% dissatisfied), and address the central component (education, exercise, duloxetine) rather than only escalating surgery.
Non-Operative Management
First-line for all patients, regardless of severity. Minimum 6-month trial before considering surgery. Multimodal approach combining weight loss, physiotherapy, pharmacological, and intra-articular therapies.
Weight Loss
Most effective non-operative intervention. Every 5kg weight loss = 20% reduction in OA progression risk.
- Mechanism: Reduces biomechanical load, decreases inflammatory adipokines (leptin)
- Evidence: 5% weight loss improves pain and function scores (NEJM 2013)
- Combined with exercise: Additive benefit versus either alone
Exercise and Physiotherapy
- Straight leg raises, isometric holds
- Eccentric loading (step-downs)
- Goal: Increase muscle force to offload joint
- Evidence: 20-30% pain reduction
- Low-impact: Swimming, cycling, walking
- Flexibility: Hamstring, IT band stretches
- Balance training: Reduces fall risk
- Frequency: 3-5x per week, 30-45 minutes
Physiotherapy provides sustained benefit with no adverse effects and is recommended for all patients.
WIPENon-Operative Management Steps
Hook:WIPE away the pain before considering surgery - Weight, Injections, PT, Education!
Management Algorithm
High Tibial Osteotomy (HTO)
Realignment procedure for young patients (under 60) with isolated medial OA and varus malalignment. Shifts load from medial to lateral compartment.
Indications (ALL must be met)
- Age: Under 60 years (biological age more important than chronological)
- Activity: Active, high-demand patient
- Compartment: Isolated medial OA (K-L Grade 3-4 medial, Grade 0-1 lateral)
- Alignment: Varus deformity (mechanical axis passes through medial compartment)
- Arc of motion: Flexion greater than 110°, extension lag less than 10°
- Patellofemoral: Minimal to no patellofemoral OA
- Ligaments: Stable knee (ACL/PCL intact)
- BMI: Ideally under 30 (obesity reduces survival)
Contraindications
- Inflammatory arthritis
- Tricompartmental OA
- Severe patellofemoral OA (Outerbridge Grade 3-4)
- Fixed flexion deformity greater than 15°
- Lateral compartment Outerbridge greater than Grade 2
- Medial bone loss (cannot achieve correction)
Technique Overview
Opening Wedge HTO (Medial)
Long-leg standing radiographs: Measure mechanical axis, calculate correction needed. Goal: Shift axis to 62% lateral (3-5° valgus). Calculate wedge size: 1mm wedge = 1° correction.
Longitudinal incision over proximal medial tibia. Protect superficial MCL. Expose metaphysis just distal to tibial tubercle.
Biplanar cut: Anterior cut from medial cortex directed laterally and posteriorly, stopping 1cm from lateral cortex (preserve hinge). Posterior cut 1cm posterior. Gradually open wedge with osteotomes/spreaders under fluoroscopy.
Locking plate (TomoFix, Puddu) with bone graft or substitute to fill wedge. Aim for mechanical axis passing through 62% of tibial plateau width (Fujisawa point). Confirm with fluoroscopy.
Undercorrection/overcorrection (10-15%, poor pre-op planning), delayed union/nonunion (5-10%, inadequate fixation/graft), lateral hinge fracture (5%, loss of correction), hardware irritation (20%, plate removal common), peroneal nerve palsy (1-2%, traction injury).
Outcomes
- Survivorship: 80% good-excellent at 10 years, 60-70% at 15 years
- Conversion to TKA: Does not compromise future TKA outcomes
- Patient satisfaction: High in appropriately selected patients
HTO buys time for young patients to delay arthroplasty by 10-15 years.
Surgical Technique
This section details the technical execution of the three main surgical interventions for knee OA: High Tibial Osteotomy (HTO), Unicompartmental Knee Arthroplasty (UKA), and Total Knee Arthroplasty (TKA).
Opening Wedge HTO Surgical Technique
Pre-operative Planning and Setup
Long-leg standing radiographs: Measure mechanical axis (centre of femoral head to centre of ankle). Calculate current varus deformity. Target correction: Shift mechanical axis to Fujisawa point (62% lateral, 3-5° valgus). Calculate wedge size: 1mm opening = approximately 1° correction. Example: 8° varus requires 10-11mm wedge to achieve 3° valgus.
Supine on radiolucent table. Tourniquet: High thigh (inflate to 300mmHg). C-arm: Position for AP and lateral fluoroscopy of proximal tibia. Bump: Under ipsilateral hip for neutral rotation.
Implants: Locking HTO plate (TomoFix, Puddu, Arthrex), appropriate screws. Graft: Allograft or bone substitute (calcium phosphate, DBM). Instruments: Oscillating saw, osteotomes (graduated), spreaders, K-wires, power drill.
Surgical Steps
Longitudinal incision 6-8cm over proximal medial tibia, centred 4cm distal to joint line. Extend from tibial tubercle to posteromedial border. Protect: Saphenous vein and nerve (anterior to incision).
Identify superficial MCL (pes anserinus insertion). Subperiosteal dissection of superficial MCL anteriorly to expose medial tibial metaphysis. Mark osteotomy level: 3.5-4cm distal to medial joint line (below tibial tubercle). Protect posterior cortex: Pass a retractor posteriorly along posterior tibial cortex.
Anterior K-wire: From medial cortex (osteotomy start point) directed laterally and superiorly toward fibular head under fluoroscopy. Angle: Parallel to joint line on AP, slight posterior slope (5-7°) on lateral. Check: Wire exits lateral cortex 1cm distal to lateral joint line (preserves hinge).
Anterior cut: Oscillating saw along K-wire from medial cortex, stopping 1cm from lateral cortex (preserve lateral hinge). Posterior cut: Second cut 1cm posterior to first, parallel, also stopping 1cm from lateral cortex. Depth check: Fluoroscopy to confirm hinge preservation.
Sequential opening: Insert osteotomes into osteotomy gap, gradually open with increasing sizes (5mm, 8mm, 10mm). Spreaders: Use laminar spreaders for final opening. Monitor fluoroscopy: Check mechanical axis with electrocautery cable (hip to ankle). Target: 62% lateral. Check hinge: Ensure no lateral cortex fracture.
Plate application: Position locking HTO plate on medial tibia. Proximal screws: Insert 2-3 locking screws into proximal fragment. Bone graft: Pack allograft or substitute into wedge gap. Distal screws: Insert distal locking screws. Final imaging: Confirm alignment (mechanical axis), plate position, screw purchase.
Hemostasis: Release tourniquet, achieve hemostasis. Drain: Optional (most surgeons omit). Layer closure: Pes/superficial MCL, subcutaneous, skin. Dressing: Bulky dressing, hinged knee brace locked in extension.
Lateral hinge fracture (5%): Avoid by preserving 1cm lateral cortex, gradual opening, fluoroscopy monitoring. Undercorrection (10-15%): Meticulous pre-op planning, intra-op cable check of mechanical axis. Peroneal nerve palsy (1-2%): Avoid prolonged lateral retraction, gentle opening.
The opening wedge HTO requires precise planning and meticulous execution to achieve optimal alignment.
The Knee Adduction Moment (KAM)
The topic notes that lateral-wedge insoles "aim to reduce the knee adduction moment" and that varus malalignment increases medial load, but the KAM itself - the biomechanical driver that ties these together - is never explained.
- What it is. During the stance phase of gait the ground-reaction force passes medial to the knee joint centre, creating an external adduction (varus) moment that thrusts the knee into varus and concentrates load on the MEDIAL compartment. Its magnitude is the single best dynamic surrogate for medial-compartment load.
- Why it matters. A higher peak KAM (and the KAM impulse, the area under the curve over stance) predicts the presence, severity and radiographic PROGRESSION of medial knee OA, and is increased by varus malalignment, obesity and a wide-based gait.
- Every "unloading" treatment works through it. Each conservative and surgical measure for medial OA reduces the KAM or its effect: lateral-wedge insoles and valgus unloader braces shift load laterally; gait retraining (toe-out gait, medial knee thrust, lateral trunk lean, shorter stride) lowers the peak KAM; weight loss reduces the force that generates it; and high tibial osteotomy structurally moves the mechanical axis lateral (to the Fujisawa point), directly cutting the medial load. Understanding the KAM explains WHY these interventions are chosen for medial-compartment disease.
Q: What is the knee adduction moment and why is it central to medial knee OA? A: During gait the ground-reaction force passes medial to the knee, creating an external adduction (varus) moment that concentrates load on the medial compartment; a higher peak KAM (and KAM impulse) predicts medial-OA severity and progression. It is the common target of the medial-OA "unloading" toolkit - lateral-wedge insoles, valgus unloader braces, gait retraining, weight loss and high tibial osteotomy (which shifts the mechanical axis laterally to the Fujisawa point).
STORMRisk Factors for Knee Osteoarthritis
Hook:STORM batters the knee joint - Sex, Trauma, Obesity, Repetitive load, Malalignment!
PAINIndications for Total Knee Arthroplasty
Hook:PAIN drives the decision for TKA - refractory Pain, ADL limited, severe Imaging, No contraindications!
Complications
Periprosthetic joint infection (PJI) is the most serious complication requiring urgent recognition and treatment. Early acute PJI (under 4 weeks) is managed with debridement and implant retention (DAIR), while chronic PJI (over 4 weeks) requires two-stage revision.
- Incidence
- 1-2% (superficial 2-3%, deep 0.5-1%)
- Risk Factors
- Diabetes, obesity, RA, prolonged surgery, previous surgery
- Management
- Early (under 4 weeks): DAIR; Chronic (over 4 weeks): 2-stage revision
- Incidence
- 1-2% at 10 years, 5% at 20 years
- Risk Factors
- Malalignment, obesity, polyethylene wear, osteolysis
- Management
- Revision TKA with bone grafting if needed
- Incidence
- 0.5-1%
- Risk Factors
- Ligament imbalance, component malposition, flexion gap issues
- Management
- Mild: Brace, strengthen; Severe: Revise to constrained/hinge implant
- Incidence
- 5-10%, severe (ROM under 90°) 2-3%
- Risk Factors
- Pre-op stiffness, infection, haematoma, poor compliance
- Management
- Aggressive PT, manipulation under anaesthesia at 6-12 weeks
- Incidence
- 0.5-1% intra-op, 1-2% post-op
- Risk Factors
- Osteoporosis, trauma, anterior femoral notching, elderly
- Management
- ORIF if stable implant, revision if loose or poor bone quality
- Incidence
- 1-2% symptomatic (10-30% subclinical DVT)
- Risk Factors
- Immobility, malignancy, thrombophilia, prolonged surgery
- Management
- Prophylaxis (LMWH or aspirin per local VTE guidelines), early mobilisation, mechanical prophylaxis
- Incidence
- 10-15%
- Risk Factors
- Pre-op catastrophising, depression, unrealistic expectations
- Management
- Screen pre-op (HADS, PCS), manage expectations, consider psychology
- Incidence
- 0.1-0.5% (common peroneal, popliteal artery)
- Risk Factors
- Fixed flexion correction, valgus release, vascular disease
- Management
- Immediate recognition, vascular surgery consult if arterial
Complication-Specific Management
PJI Classification and Management
PJI Management Algorithm
Clinical: Pain, swelling, fevers, wound drainage. Bloods: FBC, CRP/ESR (elevated), blood cultures. Aspiration: Cell count (greater than 3,000 WCC, greater than 80% PMNs), Gram stain, culture, synovial alpha-defensin or leucocyte esterase.
DAIR procedure (Debridement, Antibiotics, Implant Retention): Aggressive irrigation (9L saline), debridement of infected tissue, polyethylene exchange, multiple tissue cultures (5-6 samples), empirical IV antibiotics (vancomycin plus cephalosporin), then culture-directed for 6 weeks total. Success rate: 60-80% if organism sensitive.
Stage 1: Explant all components, thorough debridement, antibiotic-impregnated cement spacer (vancomycin plus tobramycin), IV antibiotics 6 weeks, monitor inflammatory markers. Stage 2: Re-implantation after CRP/ESR normalised (typically 6-12 weeks), repeat aspiration to exclude persistent infection. Success rate: 85-90%.
Major criteria (1 sufficient): Sinus tract communicating with prosthesis, or purulence around prosthesis. Minor criteria (3+ required): Elevated CRP/ESR, elevated synovial WCC (greater than 3,000) or PMN (greater than 80%), positive cultures (2+), positive histology. Acute PJI (under 4 weeks) may have normal markers.
Early recognition and appropriate management of PJI is critical for implant salvage.
HTO-Specific Complications
- Incidence
- 5-10%
- Prevention
- Adequate fixation, bone graft/substitute, avoid smoking
- Management
- If delayed: Continue protected weight-bearing, bone stimulator; If nonunion: Revision fixation with bone graft
- Incidence
- 5%
- Prevention
- Gradual opening, fluoroscopy monitoring, preserve 1cm hinge
- Management
- If stable: Continue protected weight-bearing; If unstable: Revision fixation with lateral plate
- Incidence
- 10-15%
- Prevention
- Pre-op planning (long-leg views), intra-op fluoroscopy, cable method
- Management
- Undercorrection: Early OA progression, consider revision osteotomy; Overcorrection (greater than 8°): Lateral compartment overload
- Incidence
- 1-2%
- Prevention
- Avoid prolonged retraction, gentle valgus correction, pad fibular head
- Management
- Most resolve spontaneously (70-80%), supportive care (AFO, PT), explore if no recovery at 3 months
Postoperative Rehabilitation
Total Knee Arthroplasty Rehabilitation
TKA Rehab Timeline
Pain control: Multimodal analgesia (paracetamol, NSAIDs, opioids PRN, local infiltration). Mobilisation: Out of bed day 0-1 with physiotherapy. Weight-bearing as tolerated with frame/crutches. DVT prophylaxis: LMWH or aspirin (per local VTE guidelines such as NICE/AAOS/ACCP), graduated compression stockings, foot pumps. ROM exercises: Ankle pumps, quadriceps sets, passive knee flexion/extension.
Gait training: Progress to stick, wean to independent. ROM goals: 0-90° by discharge. Exercises: Active assisted flexion/extension, straight leg raises, quad sets. Wound care: Dry dressing, monitor for infection signs. Discharge planning: Home with OT assessment, outpatient PT arranged.
ROM goals: 0-110° by 6 weeks. Strengthening: Progressive resistance (theraband, weights), functional exercises (sit-to-stand, step-ups). Gait: Wean walking aids, normalise gait pattern. Milestones: Independent ADLs, stairs, car transfers. Review: 6-week clinic review, radiographs (AP, lateral).
ROM goals: 0-120° by 12 weeks. Activities: Return to low-impact exercise (swimming, cycling, golf). Avoid high-impact (running, contact sports). Strengthening: Gym-based program, endurance training. Return to work: Sedentary 6-8 weeks, manual 12+ weeks.
Plateau: Maximum improvement by 6-12 months. Surveillance: Annual review (clinical, radiographs if symptomatic). Activity: Encourage low-impact exercise, maintain quad strength. Precautions: Avoid high-impact sports lifelong.
Weight-bearing as tolerated immediately for cemented TKA. No restrictions. Uncemented or bone-grafted cases may have 6-week protected weight-bearing, but this is rare for primary TKA.
Rehabilitation is patient-driven with individualised goal-setting for best outcomes.
Outcomes and Prognosis
Predictors of Poor Outcome
- Effect on Outcome
- Unrealistic expectations = dissatisfaction
- Management Strategy
- Detailed counselling, realistic goal-setting
- Effect on Outcome
- Depression, catastrophising = poor pain relief
- Management Strategy
- Screen pre-op (HADS, PCS), optimise mental health
- Effect on Outcome
- Higher activity, higher revision rate
- Management Strategy
- Consider HTO/UKA, counsel about longevity
- Effect on Outcome
- Higher infection, mechanical failure
- Management Strategy
- Encourage pre-op weight loss, warn of risks
10-15% of TKA patients are dissatisfied despite well-performed surgery. Main drivers: pre-operative pain catastrophising, unrealistic expectations, psychological distress. Pre-operative screening and counselling are key.
Guidelines, Registries & Global Practice
Global Epidemiology
Knee OA affects an estimated 250-350 million people worldwide and is a leading cause of years lived with disability (Global Burden of Disease studies). Burden is rising fastest in low- and middle-income countries, driven by ageing and the obesity epidemic. The medial compartment is most commonly affected, reflecting the physiological varus tendency and higher medial joint load.
Side-by-Side Guideline Comparison
- OARSI
- Core, strongly recommended
- NICE (UK)
- Core (offered to all)
- ACR (US)
- Strongly recommended
- AAOS (US)
- Strong evidence
- OARSI
- Recommended (knee)
- NICE (UK)
- First-line before oral
- ACR (US)
- Strongly recommended
- AAOS (US)
- Recommended
- OARSI
- Conditional (comorbidity-dependent)
- NICE (UK)
- Lowest dose, shortest time
- ACR (US)
- Strongly recommended
- AAOS (US)
- Strong evidence
- OARSI
- Conditional, short-term
- NICE (UK)
- May be offered for flares
- ACR (US)
- Conditionally recommended
- AAOS (US)
- Limited / inconclusive
- OARSI
- Not recommended / uncertain
- NICE (UK)
- Not recommended
- ACR (US)
- Conditionally against
- AAOS (US)
- Cannot recommend
- OARSI
- Not recommended
- NICE (UK)
- Not recommended
- ACR (US)
- Not addressed as OA Rx
- AAOS (US)
- Strong evidence against
Across OARSI, NICE, ACR and AAOS the core treatment is the same: structured exercise, weight management and education, with topical or oral NSAIDs as adjuncts. All major bodies advise against routine viscosupplementation, glucosamine/chondroitin and arthroscopic washout/debridement for established OA.
- Convergent survivorship: TKA approximately 94-96% at 10 years across NJR, AJRR, AOANJRR, Nordic registries
- Cemented fixation: durable and most common worldwide
- Patellar resurfacing: lower revision for anterior knee pain
- UKA: higher revision than TKA, strongly surgeon-volume dependent
- Younger age: consistently higher revision across all registries
- High-resource: robotic/navigated TKA, day-case arthroplasty, enhanced recovery, formal VTE pathways
- Limited-resource: prioritise exercise/weight loss and analgesia; HTO retains a strong role (joint-preserving, lower implant cost)
- Access: arthroplasty capacity, implant cost and rehabilitation availability vary widely
- Antibiotic prophylaxis: first-generation cephalosporin (e.g. cefazolin) at induction is near-universal
- Informed consent: Specific risks (infection 1-2%, revision 5% at 10 years, DVT/PE, stiffness, persistent pain 15%, nerve injury 0.5%), alternatives (non-operative, HTO, UKA), and expected outcomes (80-85% satisfaction)
- Pre-operative optimisation: Document BMI, smoking status, diabetes control (HbA1c), dental clearance
- Surgical planning: Long-leg alignment radiographs, templating, implant selection rationale
- Complications: Early recognition and management of PJI, DVT/PE, stiffness
- Failure to trial conservative management: Minimum 6 months non-operative recommended
- Infection: Delayed recognition, inadequate antibiotic prophylaxis
- Persistent pain/dissatisfaction: Unrealistic patient expectations, inadequate pre-operative counselling
- Neurovascular injury: Rare but devastating, document pre- and post-operative neurovascular status
Thorough documentation and realistic pre-operative counselling are medicolegal essentials.
Controversies and Areas of Uncertainty
Traditional mechanical alignment (neutral hip-knee-ankle) is challenged by kinematic alignment, which restores the patient's pre-arthritic joint line. RCTs show comparable short-term outcomes; long-term survivorship and the limits of acceptable deformity remain unresolved.
Robotics improve alignment accuracy and component positioning, but a clear benefit in long-term survivorship, function or revision over conventional instrumentation is not yet proven, and cost is substantial.
UKA offers faster recovery and more natural kinematics but carries higher registry revision rates, largely explained by surgeon volume and lower revision threshold. The TOPKAT trial found both cost-effective with comparable patient outcomes.
For young, active patients with isolated medial OA and varus, the choice between joint-preserving HTO and UKA remains debated and is driven by alignment, activity demands, age and patient preference.
Viscosupplementation, PRP and stem-cell therapies are widely marketed but supported by heterogeneous, often low-quality evidence; major guidelines do not endorse routine use. Repeated corticosteroid may accelerate cartilage loss.
Whether to always, never or selectively resurface the patella is long-debated. Registry data favour resurfacing for lower revision due to anterior knee pain, but selective approaches report good results.
MCQ Practice Points
Q: A 55-year-old with isolated medial compartment OA, intact ACL, passively correctable varus and Outerbridge 0-1 in the lateral and patellofemoral compartments is the ideal candidate for which procedure? A: Medial unicompartmental knee arthroplasty (UKA), provided the Oxford criteria are met (intact ACL, correctable deformity, preserved opposite and patellofemoral compartments). A younger, very active patient with significant varus malalignment may instead be better served by high tibial osteotomy.
Q: What is the key radiographic difference between Kellgren-Lawrence Grade 3 and Grade 4 knee OA? A: Grade 3: Moderate joint space narrowing (50% loss) with multiple osteophytes. Grade 4: Severe narrowing (bone-on-bone contact) with large osteophytes and marked subchondral sclerosis. The distinction is complete versus incomplete joint space loss.
Q: What fixation method has the most robust long-term registry track record for primary TKA? A: Cemented fixation has durable, well-documented survivorship across major joint registries (NJR, AJRR, AOANJRR) and remains the most common fixation worldwide. Modern cementless designs are improving but historically showed higher early revision, particularly in older, osteoporotic patients.
Q: What is the target mechanical axis correction for opening wedge high tibial osteotomy? A: Fujisawa point: 62% of tibial plateau width from medial to lateral, corresponding to 3-5° valgus overcorrection. Undercorrection (less than 3°) associated with early failure. Overcorrection (greater than 8°) risks lateral compartment OA.
Q: What are the leading reasons for revision TKA in national registries? A: Aseptic loosening, infection, instability and unexplained pain dominate revision indications across registries. Loosening is often multifactorial (malalignment, polyethylene wear, osteolysis). Infection is the most feared and a leading cause of early revision.
Q: What is the approximate 10-year cumulative revision rate for primary TKA in major registries? A: Approximately 4-6%, meaning roughly 94-96% implant survivorship at 10 years across the NJR, AJRR and AOANJRR. This excellent long-term performance underpins patient counselling worldwide.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 58-year-old female presents with 2-year history of progressive left knee pain. Worse with stairs and prolonged walking. BMI 32. Radiographs show Kellgren-Lawrence Grade 2 medial compartment OA. How would you manage this patient?”
“A 45-year-old male tradesman presents with isolated medial knee pain. Active, plays social sport. Radiographs show K-L Grade 3 medial OA with 8° varus alignment on long-leg views. Lateral compartment and patellofemoral joint appear normal. He has failed 12 months of conservative management. What are your surgical options and how would you decide?”
“A 68-year-old male is 4 weeks post-TKA. He presents with increasing pain, swelling, and fevers (38.2°C). Wound has purulent discharge. How would you assess and manage this patient?”
Key Anatomy
- Medial compartment most commonly affected (70% cases)
- Subchondral sclerosis, osteophytes, joint space narrowing = radiographic OA triad
- Mechanical axis: Hip-knee-ankle alignment, 180° normal (varus/valgus deformity shifts load)
- ACL integrity mandatory for UKA (loss = instability)
Classification
- Kellgren-Lawrence: Grade 0 (normal) to Grade 4 (bone-on-bone)
- Grade 1-2 = conservative, Grade 3 = consider surgery if young, Grade 4 = TKA
- Outerbridge (arthroscopic): Grade 1 (softening) to Grade 4 (exposed bone)
- K-L radiographic versus Outerbridge arthroscopic (not 1:1 correlation)
Treatment Algorithm
- All patients: Weight loss (5-10% body weight), PT (quad strengthening), analgesia (paracetamol, NSAIDs), injections
- Young (under 60), isolated medial OA, varus: HTO (80% survival 10 years)
- Middle-aged, unicompartmental, intact ACL: UKA (95% survival 10 years)
- Older, tricompartmental, K-L Grade 4: TKA (95% survival 10 years, gold standard)
Surgical Pearls
- HTO target: 3-5° valgus (Fujisawa point 62%), 6 weeks non-weight-bearing
- UKA requires intact ACL, opposite compartment Outerbridge 0-2, correctable deformity
- TKA: cemented fixation (durable registry survivorship), resurface patella, mechanical axis neutral
- Weight-bearing as tolerated immediately post-TKA (cemented)
Complications
- PJI: 1-2% (early under 4 weeks = DAIR, chronic over 4 weeks = 2-stage)
- Aseptic loosening: 1-2% at 10 years (malalignment, polyethylene wear)
- Stiffness: 5-10% (MUA at 6-12 weeks if ROM under 90°)
- Dissatisfaction: 15% (manage expectations, screen for psychological factors)
Evidence Base and Key Trials
WOMAC Validation Study
- Validated the Western Ontario and McMaster Universities Arthritis Index (WOMAC) within a double-blind RCT of two NSAIDs in hip and knee OA
- Three subscales (pain, stiffness, physical function) met criteria for validity, reliability and responsiveness
- Disease-specific instrument designed for evaluative OA clinical trials
- Widely adopted as a reference outcome measure for hip and knee OA
Intra-articular Triamcinolone vs Saline (McAlindon RCT)
- Double-blind RCT: 140 patients (K-L grade 2-3) randomised to triamcinolone 40 mg vs saline every 12 weeks for 2 years
- Triamcinolone caused significantly greater cartilage volume loss than saline (-0.21 vs -0.10 mm)
- No significant difference in knee pain between groups at 2 years
- Does not support repeated corticosteroid injection for symptomatic knee OA
Kellgren-Lawrence Radiographic Classification
- Original description of the 5-grade (0-4) radiographic system for osteoarthrosis
- Grading based on osteophytes, joint space narrowing, sclerosis and bony deformity
- Became the international reference standard for radiographic OA severity
- Adopted by the WHO for epidemiological OA studies
National Joint Replacement Registries (Global)
- TKA 10-year cumulative revision rate approximately 4-6% across major registries
- Cemented fixation shows durable survivorship and remains the most common worldwide
- Patellar resurfacing reduces revision for anterior knee pain
- UKA carries higher revision than TKA (approximately 10-13% at 10 years), strongly surgeon-volume dependent
- Younger age (under 55) is consistently associated with higher revision rates
IDEA Trial: Intensive Diet and Exercise for Knee OA
- Single-blind RCT: 454 overweight/obese adults (BMI 27-41) with knee OA over 18 months
- Arms: diet plus exercise vs diet alone vs exercise alone
- Diet plus exercise produced the greatest pain reduction, best function and quality of life
- Diet groups achieved greater weight loss, lower IL-6 and reduced knee compressive force versus exercise alone
RCT of Total Knee Replacement vs Nonsurgical Treatment (MEDIC)
- RCT: 100 patients with moderate-to-severe knee OA eligible for TKA
- TKA plus 12 weeks nonsurgical care vs 12 weeks nonsurgical care alone
- At 12 months TKA gave greater KOOS4 improvement (adjusted difference 15.8 points)
- TKA carried more serious adverse events (24 vs 6); 74% of nonsurgical patients had not undergone TKA by 12 months
TKR After HTO vs Primary TKR: Meta-analysis
- Systematic review and meta-analysis: 11 studies, 2,170 TKR procedures
- No significant difference in KSS or HSS scores between TKR-after-HTO and primary TKR
- Survivorship at mean 7.2 years: 95% (post-HTO) vs 97% (primary) for any-cause revision
- A previous HTO does not negatively influence future TKR outcomes, though conversion is technically harder