FGFR2 Acrocephalosyndactyly
- FGFR2: Two recurrent mutations - Ser252Trp and Pro253Arg.
- Hand: Complex syndactyly with bony fusion - the mitten hand.
- Thumb: Short, broad, with radial clinodactyly.
- Symphalangism: Stiff fingers (except little finger) limit outcome.
- Staged surgery: Release border digits and thumb first.
- “FGFR2 Ser252Trp and Pro253Arg
- “Upton classification of the Apert hand (I-III)
- “Allelic with Crouzon syndrome
- “Symphalangism is the main limit on function
Apert is a craniosynostosis syndrome. Raised intracranial pressure, hydrocephalus, obstructive sleep apnoea and a difficult airway take priority over the hands in infancy. The craniofacial and neurosurgical teams lead early care.
Even after perfect syndactyly release, the fingers stay stiff because of symphalangism (fused interphalangeal joints). Counsel families that the goal is a functional grasp and pinch, not normal fingers.
- Description
- Bony fusion of central digits - mitten hand
- Management
- Staged release, prioritise border digits
- Description
- Broad thumb with radial clinodactyly
- Management
- First web release, osteotomy for clinodactyly
- Description
- Stiff fused IP joints (spares little finger)
- Management
- Accept stiffness, optimise grasp
- Description
- Cutaneous toe webbing
- Management
- Usually conservative
APERTApert Syndrome Core Features
Hook:APERT - Acrocephaly, Proptosis, Excess FGFR2 fusion, Radial thumb, Total syndactyly.
Overview/Epidemiology
Apert syndrome (acrocephalosyndactyly type I) is one of the most recognisable craniosynostosis syndromes and the one with the most severe hand involvement.
- Genetics: Autosomal dominant. Caused by FGFR2 (Fibroblast Growth Factor Receptor 2) mutations.
- Birth prevalence: Roughly 1 in 65,000-80,000 live births.
- New mutations: Almost all cases arise as new (de novo) mutations; there is a strong paternal age effect.
- The orthopaedic angle: Apert is the syndrome where the hand surgeon plays a central role. The complex (bony) syndactyly is more severe than in any other common craniosynostosis syndrome.
Pathophysiology and Genetics
FGFR2 gain-of-function
According to PubMed, Wilkie and colleagues showed that essentially all Apert cases result from one of two adjacent missense mutations in FGFR2: Ser252Trp or Pro253Arg (Wilkie, Nat Genet 1995). These sit in the linker between the second and third immunoglobulin-like domains of the receptor.
- FGFR signalling normally coordinates suture and limb morphogenesis.
- The Apert mutations cause a gain of function - enhanced ligand binding and prolonged signalling.
- The result is premature fusion of cranial sutures (craniosynostosis) and abnormal fusion of the developing digital rays (syndactyly).
Allelic with Crouzon
Apert is allelic with Crouzon syndrome: both are caused by FGFR2 mutations, but Crouzon mutations affect the third Ig domain and produce craniosynostosis with normal limbs, whereas the Apert linker mutations produce craniosynostosis plus severe syndactyly (Wilkie, Nat Genet 1995).
Genotype-phenotype correlation
- The Ser252Trp mutation tends to produce more severe craniofacial disease (more cleft palate).
- The Pro253Arg mutation tends to produce more severe syndactyly of the hands and feet (Wilkie, Novartis Found Symp 2001).
Why almost every case is new and paternally derived
The overview notes that Apert is "almost always a new (de novo) mutation with a strong paternal age effect" - but the reason is never explained, and it is a high-yield genetics point. Apert is the textbook example of a "paternal age effect" disorder driven by selfish spermatogonial selection.
- The two recurrent FGFR2 mutations arise as new mutations on the paternally derived allele in essentially all cases - they occur during spermatogenesis, not oogenesis.
- These specific gain-of-function mutations give the mutant spermatogonial stem cell a selective growth/clonal advantage in the testis, so mutant clones expand and accumulate with the man's age ("selfish" selection, analogous to a benign tumour of spermatogonia).
- The result is that the risk rises with advancing paternal age, the mutation is paternal in origin, and the small number of mutable nucleotides explains why the same two substitutions recur across unrelated families.
This is why the recurrence risk for unaffected parents is very low (a sporadic de novo event), whereas an affected individual transmits it as autosomal dominant with a 50% risk - the distinction families need for counselling.
Apert is the classic paternal-age-effect disorder: the FGFR2 gain-of-function mutation arises de novo on the paternal allele and gives mutant spermatogonia a clonal growth advantage ("selfish spermatogonial selection"), so risk rises with paternal age and the same two substitutions recur. Counsel that unaffected parents have a very low recurrence risk, but an affected person transmits it autosomal-dominantly at 50%.
Classification Systems
Upton Classification of the Apert Hand
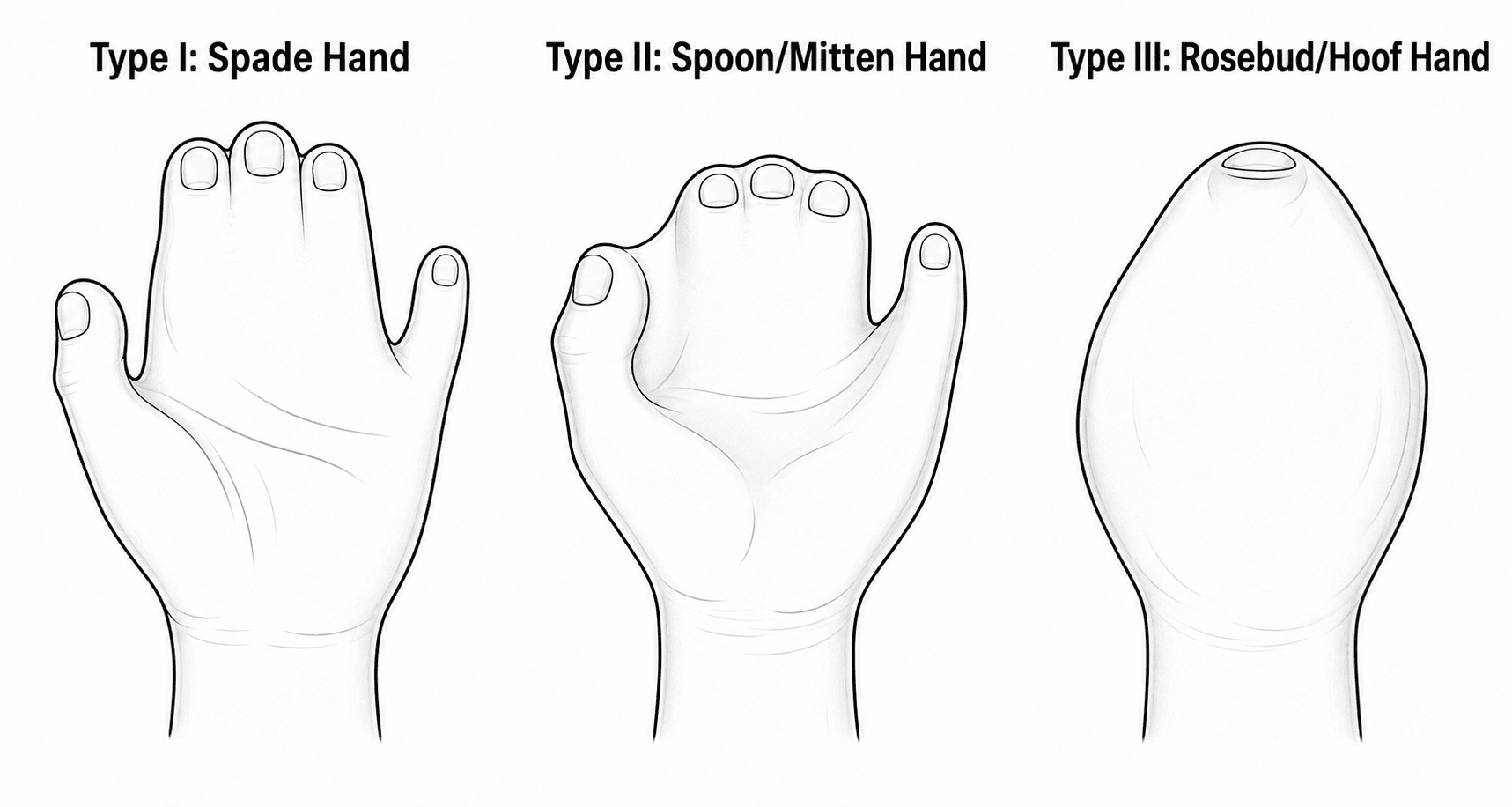
The most widely used scheme (Upton, Clin Plast Surg 1991) grades severity I to III:
- Type I - "spade" hand: Flattest, mildest. Central digits fused; the thumb and little finger are relatively spared, and the first and fourth web spaces are more developed.
- Type II - "spoon" or "mitten" hand: The palm becomes concave; the thumb is joined to the index by simple syndactyly.
- Type III - "rosebud" or "hoof" hand: Most severe. A tight central mass of fused digits with a single conjoined nail; the thumb is incorporated. Hardest to reconstruct.
IIIIIIUpton Hand Classification
Hook:Spade to Spoon to Rosebud - the hand gets tighter and harder to reconstruct from I to III.
Beyond the Hand: Progressive Proximal Upper-Limb Synostosis
The classification box flags "elbow and shoulder stiffness", the clinical exam says to "check elbow and shoulder range (often reduced)", and the complications list "reduced elbow/shoulder motion - proximal joint involvement" - but the topic never explains why. The Apert upper limb is abnormal proximally as well as distally: there is progressive synostosis and dysplasia of the elbow and shoulder, and it compounds the hand disability.
- Elbow - the hallmark is humeroradial (radiohumeral) synostosis: the radius and capitellum progressively fuse, so the elbow loses flexion-extension and, with it, the ability to bring the hand to the mouth and midline. (This is distinct from proximal radioulnar synostosis, which limits forearm rotation and is covered in its own topic.)
- Shoulder - glenohumeral dysplasia with a small, abnormally shaped glenoid/proximal humerus and progressive loss of abduction and elevation.
- Progressive - like the cranial sutures and the cervical spine, these joints are often mobile in infancy and stiffen with growth, so range of motion documented early may not last.
Why it matters:
- Problem
- Progressive humeroradial synostosis (loss of flexion-extension)
- Consequence / management
- Cannot reach mouth/midline; therapy to preserve function, derotation/positioning osteotomy only rarely
- Problem
- Glenohumeral dysplasia, restricted abduction/elevation
- Consequence / management
- Reduced overhead reach; compensatory strategies and therapy
- Problem
- Proximal stiffness ADDS to the stiff, reconstructed hand
- Consequence / management
- A child with a good reconstructed hand may still struggle to position it - set realistic goals
The clinical lesson is that the disability is a whole-limb problem: a technically excellent hand reconstruction can be undermined if the child cannot position the hand because the elbow and shoulder are stiff, so the proximal joints must be assessed and the family counselled accordingly. Surgery to the proximal joints is uncommon; therapy and adaptive strategies dominate.
Apert is not just a hand problem: the elbow and shoulder undergo progressive synostosis/dysplasia - classically humeroradial synostosis at the elbow (losing flexion-extension and hand-to-mouth reach) and glenohumeral dysplasia at the shoulder. These stiffen with growth and compound the hand disability, so assess the whole limb and counsel that positioning the hand may be as limiting as the hand itself. (Proximal radioulnar synostosis - forearm rotation - is the separate sibling topic.)
MITTENApert Hand Anatomy
Hook:Picture a MITTEN - one block of central fingers with the thumb tucked to the side.
Clinical Assessment
- Antenatal and birth history (craniosynostosis often diagnosed at birth or on prenatal ultrasound).
- Airway, feeding and sleep (obstructive sleep apnoea is common with midface hypoplasia).
- Developmental milestones and any features of raised intracranial pressure.
- Functional use of the hands - how the child grasps and pinches.
- Head and face: Acrocephaly (tall, turret skull), midface hypoplasia, hypertelorism, proptosis, flat facial profile.
- Hands: Define the Upton type. Assess the thumb (length, clinodactyly), the first web, and the conjoined central mass.
- Movement: Test interphalangeal motion - symphalangism means stiff joints. Check elbow and shoulder range (often reduced).
- Feet: Cutaneous toe syndactyly, broad great toes.
- Neurology: Screen for signs of cord compression if there is cervical fusion.


Investigations
- Hand and foot radiographs: Map the bony fusions, the conjoined nail, symphalangism and thumb anatomy - this drives the surgical plan.
- CT head: Suture fusion, ventricular size (hydrocephalus), midface anatomy for craniofacial planning.
- Cervical spine imaging: Apert is associated with progressive cervical vertebral fusion (commonly C5-C6), which matters for anaesthesia and neck positioning.
- MRI brain: For structural anomalies and ventriculomegaly when indicated.
- FGFR2 mutation testing confirms the diagnosis (Ser252Trp or Pro253Arg) and guides genetic counselling.
Differential Diagnosis
Other FGFR-related craniosynostosis syndromes:
- Gene
- FGFR2
- Key Differentiator
- Severe complex (bony) syndactyly - mitten hand
- Gene
- FGFR2
- Key Differentiator
- Craniosynostosis with normal limbs
- Gene
- FGFR1/FGFR2
- Key Differentiator
- Broad, deviated thumbs and big toes; partial syndactyly
- Gene
- TWIST1
- Key Differentiator
- Ptosis, low frontal hairline, mild cutaneous syndactyly
- Gene
- RAB23
- Key Differentiator
- Autosomal recessive; polydactyly with syndactyly
Key Distinguishing Points:
- Apert: The most severe hand syndactyly (bony fusion, conjoined nail).
- Crouzon: FGFR2 like Apert, but limbs are normal - this is the classic contrast.
- Pfeiffer: Broad thumbs and big toes are the clue.
- Saethre-Chotzen: Milder, with ptosis and a low frontal hairline.
Management Algorithm
Multidisciplinary Sequence
- Infancy: Craniofacial and neurosurgical care comes first - protect the brain and airway. Posterior vault expansion (often distraction) and later midface advancement address the skull and face (Raposo-Amaral, J Craniofac Surg 2020).
- Hand surgery start: Syndactyly release usually begins around 6-12 months and aims to be largely complete by 2-4 years, before fine-motor skills mature (Roje, Acta Chir Plast 2012).
Surgical Techniques
Border-First, Staged Release
Indications: Complex syndactyly of the Apert hand.
Technique: Separate digits in stages, prioritising the border digits (thumb and little finger) at the first operations, then dividing the central conjoined mass with osteotomy and bone grafting as required (Roje, Acta Chir Plast 2012). Reconstruct each web commissure with a local flap and resurface the sides with full-thickness skin grafts.
Considerations: Each finger should only be released on one side at a time to protect its blood supply; multiple operations (often 4-6 per hand) are the norm (Salazard, Chir Main 2008).
Complications
Surgical Complications of Hand Reconstruction
- Frequency
- Uncommon if staged
- Risk Factors
- Releasing both sides of one digit at once
- Management
- Strict border-first staging; never release both sides simultaneously
- Frequency
- Variable
- Risk Factors
- Tension, infection, mobile child
- Management
- Re-graft, splinting, hand therapy
- Frequency
- Common over growth
- Risk Factors
- Growth of the child, scar
- Management
- Revision web release (about 16% in some series)
- Frequency
- High
- Risk Factors
- Severe (Upton III) hands, symphalangism
- Management
- Planned multiple stages
Functional and Long-Term Issues
- Why it Happens
- Symphalangism (fused IP joints)
- Implication
- Limits final motion despite good release
- Why it Happens
- Short thumb, stiff fingers
- Implication
- Pinch is rudimentary but usually functional
- Why it Happens
- Proximal joint involvement
- Implication
- Compensatory strategies, therapy
Perioperative and Anaesthetic Considerations
Critical considerations for any surgery in Apert syndrome:
- Difficult airway: Midface hypoplasia and a high-arched/cleft palate make intubation challenging - plan ahead.
- Cervical fusion: Progressive vertebral fusion (often C5-C6) limits safe neck extension - avoid forced positioning.
- Obstructive sleep apnoea: Common; optimise and monitor in the perioperative period.
- Raised intracranial pressure: Must be excluded/treated by the craniofacial team before elective limb surgery.
Clinical Relevance and Outcomes
Why It Matters for the Exam
Apert syndrome is the classic viva case linking genetics, craniofacial surgery and hand surgery. Examiners expect you to:
- Name the FGFR2 mutations and the link to Crouzon.
- Describe the Upton hand classification and the border-first, staged release principle.
- Explain why symphalangism caps the functional outcome.
Functional Outcomes
According to PubMed, even with expert staged reconstruction the goal is a functional, opposable hand with a rudimentary but useful pinch rather than normal fingers; symphalangism is repeatedly cited as the factor that "darkens" the functional prognosis (Salazard, Chir Main 2008). Early, specialist, staged surgery completed by 2-4 years gives the best functional and aesthetic results with acceptable revision rates (Roje, Acta Chir Plast 2012).
Counselling Families
- The hand will not look or move normally, but most children achieve independent grasp and pinch.
- Multiple operations are expected; this is a planned, staged journey, not a single fix.
- Care is lifelong and multidisciplinary (craniofacial, neurosurgery, hand, ENT, genetics, development).
Guidelines, Registries & Global Practice
Global Epidemiology
- Birth prevalence around 1 in 65,000-80,000; one of the more common craniosynostosis syndromes worldwide.
- Almost all cases are de novo FGFR2 mutations with a strong paternal age effect.
- Two recurrent mutations (Ser252Trp, Pro253Arg) account for the overwhelming majority of cases globally.
Side-by-Side Guidance
- Emphasis
- Brain and airway first; staged vault expansion (often posterior distraction) and midface advancement
- Emphasis
- Early, staged, border-first syndactyly release completed by 2-4 years; Upton classification to plan
- Emphasis
- FGFR2 confirmatory testing; counselling for de novo recurrence risk and 50% transmission risk
- Emphasis
- Anticipate difficult airway, cervical fusion and OSA in all procedures
Practice Variation
- High-resource settings: Specialist craniofacial units, distraction osteogenesis, multi-stage hand reconstruction and FGFR2 testing are available.
- Limited-resource settings: Diagnosis is clinical; care prioritises airway/feeding safety and the most functionally important hand release (thumb and first web) where full multi-stage programmes are not feasible.
- Family support organisations (craniofacial and Apert-specific groups) are valuable everywhere for psychosocial support and shared decision-making.
Controversies and Areas of Uncertainty
Timing and number of hand operations There is no single agreed protocol. Most centres favour an early, border-first, staged release completed by 2-4 years, but the exact age to start, the number of stages, and how aggressively to pursue a five-fingered hand in type III cases vary between units (Roje 2012; Theman/Upton 2018).
How far to go in the type III hand Central coalition osteotomy can create five digits in severe hands, but it requires more operations. Whether the extra aesthetic and functional gain justifies the additional surgery is a judgement made with each family (Theman/Upton 2018).
Feet Toe syndactyly is usually left alone because it rarely impairs function; routine separation is not recommended, and indications for foot surgery remain selective.
Genotype-guided counselling The Ser252Trp/Pro253Arg phenotype gradient (worse face vs worse hands) is real but not absolute, so genotype informs but does not dictate individual prognosis (Wilkie 2001).
MCQ Practice Points
Q: Which gene is mutated in Apert syndrome? A: FGFR2 - specifically the Ser252Trp or Pro253Arg mutations.
Q: Apert is allelic with which other craniosynostosis syndrome? A: Crouzon syndrome (also FGFR2, but with normal limbs).
Q: What is the hand hallmark of Apert syndrome? A: Complex (bony) syndactyly of the central digits - the spade or mitten hand.
Q: Which classification is used for the Apert hand? A: The Upton classification (types I spade, II spoon/mitten, III rosebud/hoof).
Q: What limits the functional outcome after syndactyly release in Apert? A: Symphalangism - the fused, stiff interphalangeal joints (the little finger is usually spared).
Q: What is the key safety rule when releasing Apert syndactyly? A: Never release both sides of a single digit at one operation - stage the release to protect the digital blood supply.
Self-Assessment Quiz
Additional Quiz Questions
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A newborn has a turret-shaped skull, midface hypoplasia and both hands fused into a single mass. What is the diagnosis and what are your immediate priorities?”
“A 1-year-old with Apert syndrome has a tight central mass of fused fingers with a single conjoined nail. How do you classify and plan the hand?”
“The anaesthetist asks what they should know before a hand operation in a 4-year-old with Apert syndrome. What do you tell them?”
GENETICS
- FGFR2 mutation
- Ser252Trp / Pro253Arg
- Autosomal dominant
- Allelic with Crouzon
CRANIOFACIAL
- Acrocephaly (turret skull)
- Midface hypoplasia
- Hypertelorism, proptosis
- Craniosynostosis
HAND
- Complex bony syndactyly
- Mitten/spade hand
- Short radial thumb
- Symphalangism (spares little finger)
CLASSIFICATION
- Upton I - spade
- Upton II - spoon/mitten
- Upton III - rosebud/hoof
- Drives surgical plan
SURGERY
- Staged, border-first release
- Open first web, fix thumb
- Never both sides of one digit
- Complete by 2-4 years
PERIOP
- Difficult airway
- Cervical fusion (C5-C6)
- OSA
- Exclude raised ICP first
Evidence Base
- Identified two adjacent FGFR2 missense mutations - Ser252Trp and Pro253Arg - in all 40 unrelated Apert cases studied
- Mutations sit in the linker between the second and third Ig domains of FGFR2
- Apert is allelic with Crouzon syndrome (third Ig-domain mutations, normal limbs)
- Reviewed the contrasting craniofacial vs limb severity of the two Apert mutations
- Ser252Trp tends to give more severe craniofacial disease; Pro253Arg more severe syndactyly
- Proposed alternative FGFR2 splice forms mediate the distinct cranial and limb effects