Reactive Giant Cell Lesion | Osteitis Fibrosa Cystica | The Great GCT Mimic | Treat the Parathyroid First
- Brown tumour is a reactive lesion, NOT a neoplasm - the end-stage of osteitis fibrosa cystica in hyperparathyroidism
- Histologically identical to giant cell tumour of bone - the diagnosis is made by BIOCHEMISTRY (raised PTH and abnormal calcium), not by the slide
- Always check serum calcium and PTH before treating any apparent giant cell lesion of bone
- Treat the parathyroid disease first - most brown tumours regress and remineralise after the PTH is normalised
- Secondary hyperparathyroidism from chronic kidney disease is now the most common cause worldwide
- “The brown colour comes from haemosiderin and vascularity, not melanin or chondroid
- “Subperiosteal resorption of the radial side of the middle phalanges is the classic radiological sign of hyperparathyroidism
- “A 'salt-and-pepper' skull and a generalised lytic lesion in a patient with renal failure should trigger a PTH check
- “Avoid en-bloc resection or aggressive curettage as a first step - it is the wrong operation for a reactive lesion
Brown tumour is histologically identical to giant cell tumour of bone. If you treat it as a GCT (denosumab, aggressive curettage, resection) you have done the wrong operation. Always check serum calcium and PTH before committing to surgery for any giant cell lesion of bone.
Brown tumour is the focal end-stage of osteitis fibrosa cystica - a reactive response to high PTH, not a clonal tumour. There is no metastatic potential. The "tumour" is a misnomer driven by its lytic, mass-like appearance.
Correcting the hyperparathyroidism (parathyroidectomy in primary/tertiary HPT, or medical control then surgery in secondary HPT) usually leads to regression and remineralisation of the lesion. Bone surgery is a second-line, anatomy-driven decision.
Primary (adenoma, high Ca + high PTH), secondary (CKD, low/normal Ca + very high PTH) and tertiary (autonomous gland after long-standing secondary HPT). The biochemistry pattern tells you which one you are dealing with and what to do about the gland.
- Typical Patient
- HPT (primary adenoma or CKD)
- Key Discriminator
- Raised PTH + abnormal calcium; often multiple lesions
- Management Direction
- Treat parathyroid disease first
- Typical Patient
- 20-40 years, skeletally mature
- Key Discriminator
- Normal PTH and calcium; epiphyseal, subarticular; solitary
- Management Direction
- Curettage + adjuvant or denosumab
- Typical Patient
- Under 20 years
- Key Discriminator
- Fluid-fluid levels; USP6 rearrangement; normal biochemistry
- Management Direction
- Curettage + adjuvant / embolisation
- Typical Patient
- Jaw, hands, feet
- Key Discriminator
- Normal biochemistry; reactive giant cells
- Management Direction
- Curettage
- Typical Patient
- Over 50 years
- Key Discriminator
- Known primary or paraprotein; aggressive features
- Management Direction
- Oncological / haematological pathway
Overview and Epidemiology
Definition
A brown tumour is a focal, tumour-like, lytic bone lesion that represents the localised end-stage of osteitis fibrosa cystica, the skeletal manifestation of hyperparathyroidism. Sustained excess parathyroid hormone (PTH) drives osteoclastic bone resorption; the resulting cavities fill with vascular fibrous tissue, osteoclast-type giant cells, reactive woven bone, microhaemorrhage and haemosiderin. The brown colour seen at operation comes from the haemosiderin and the rich vascularity, not from any pigment-producing cell.
The crucial point for the exam is that a brown tumour is a reactive process, not a true neoplasm. It has no metastatic potential, and it is histologically indistinguishable from giant cell tumour of bone, so the diagnosis depends on the biochemical context.
Why It Matters
- It is a classic giant cell tumour mimic - mislabelling it leads to the wrong operation.
- It can be the first presentation of otherwise occult hyperparathyroidism, including parathyroid carcinoma.
- It usually regresses after the parathyroid disease is treated, so the management priority is the gland, not the bone.
Key Epidemiology
- Secondary hyperparathyroidism (chronic kidney disease) is now the most common driver worldwide, reflecting the global dialysis population.
- Primary hyperparathyroidism (usually a single parathyroid adenoma) is the classic textbook cause; brown tumours are now an uncommon presentation because primary HPT is detected earlier on routine calcium testing.
- Tertiary hyperparathyroidism (autonomous glands after long-standing secondary HPT) is a less common but recognised cause.
- Brown tumours are more frequent with more severe and longer-standing hyperparathyroidism.
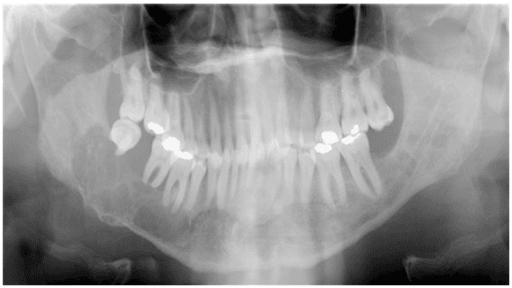
- Common sites include the pelvis, ribs, mandible/maxilla (jaws), femur and other long bones.
- Lesions may be solitary or multiple; multiplicity should raise suspicion of an underlying metabolic cause.
Pathophysiology and Pathology
The PTH-Osteoclast Axis
Parathyroid hormone is the master regulator of calcium. In excess it:
- Increases osteoclastic bone resorption (indirectly, via the RANKL pathway on osteoblastic stromal cells), liberating calcium and phosphate from bone.
- Increases renal calcium reabsorption and phosphate excretion.
- Stimulates renal 1-alpha-hydroxylase, raising active vitamin D and gut calcium absorption.
When PTH is persistently high, resorption outpaces formation. Generalised demineralisation produces osteitis fibrosa cystica; focal exuberant resorption with reactive repair produces the discrete brown tumour.
Biochemical Patterns by Type
The biochemistry both explains the disease and tells you the type:
- Calcium
- High
- Phosphate
- Low
- PTH
- High
- Typical setting
- Parathyroid adenoma (rarely carcinoma/hyperplasia)
- Calcium
- Low or normal
- Phosphate
- High
- PTH
- Very high
- Typical setting
- Chronic kidney disease, vitamin D deficiency
- Calcium
- High
- Phosphate
- Variable
- PTH
- Very high
- Typical setting
- Autonomous glands after long-standing secondary HPT
Alkaline phosphatase is typically raised, reflecting high bone turnover.
Histology
- Numerous osteoclast-type multinucleated giant cells
- A vascular, fibrous (spindle-cell) stroma
- Haemosiderin deposition and areas of old and recent haemorrhage
- Reactive woven bone and a background of generalised osteoclastic resorption
these features are indistinguishable from giant cell tumour of bone and overlap with giant cell reparative granuloma and the giant cell-rich variants of other lesions. The pathologist cannot reliably separate them on morphology alone - the diagnosis is confirmed by the biochemistry (raised PTH, abnormal calcium) and the clinical context.
Molecular Insight
Although classically considered purely reactive, molecular work shows that the giant cell-rich lesions of the jaws in hyperparathyroidism can harbour activating KRAS mutations with downstream MAPK/ERK pathway activation, placing them in the same RAS-driven spectrum as some histological mimics. This does not change the clinical message - treat the parathyroid disease - but it explains the close morphological overlap with other giant cell lesions.
Natural History After Parathyroid Treatment
What "Regression and Remineralisation" Actually Means
The management and prognosis sections repeatedly promise that brown tumours regress and remineralise once PTH is normalised, and the monitoring step tells you to follow biochemistry and serial imaging - but the topic never defines the timeline or how to read a lesion that fails to settle. This matters because it is exactly what an examiner asks next.
- Bone turnover falls quickly once PTH normalises; radiologically, the lytic lesion fills in and remineralises gradually over months, sometimes taking a year or more for a large lesion to sclerose fully.
- A residual sclerotic or cystic focus can persist on imaging even after clinical and biochemical cure - a healed, remineralised lesion is not the same as a failed treatment.
- Serial biochemistry - calcium, phosphate, PTH and alkaline phosphatase - is the primary measure of success; falling PTH and normalising calcium confirm the gland is controlled.
- Serial imaging documents remineralisation and is reassuring when it tracks the biochemistry.
When a lesion does NOT regress - think inadequate parathyroid control, not aggressive tumour:
- Persistence or progression of a brown tumour after apparent treatment usually means the parathyroid disease is incompletely controlled rather than that the lesion is behaving like a neoplasm.
- Causes include a missed or ectopic adenoma, a supernumerary or residual gland after surgery, or under-treated secondary hyperparathyroidism in a dialysis patient. The response is to re-check the biochemistry and re-image the parathyroids (repeat ultrasound and sestamibi, with 4D-CT if needed), not to escalate to aggressive bone resection.
- Only a genuinely persistent, symptomatic lesion despite documented biochemical cure justifies bone-directed surgery (curettage and grafting, or fixation for mechanical failure).
Q: A brown tumour fails to remineralise months after parathyroid treatment. What is the most likely explanation? A: Incompletely controlled hyperparathyroidism - a residual or ectopic adenoma, a supernumerary gland, or under-treated secondary HPT - not aggressive local behaviour. Re-check calcium and PTH and re-localise the parathyroids before considering bone surgery.
Clinical and Exam Relevance
Why Examiners Love Brown Tumour
- It is the archetypal "do not be fooled" giant cell lesion - it tests whether you check biochemistry before operating.
- It links endocrinology, nephrology, radiology and orthopaedic oncology in one topic, ideal for a viva that crosses subspecialties.
- It rewards a candidate who states the principle clearly: treat the parathyroid disease first, operate on the bone only for mechanical or neurological reasons.
The One-Line Answer
If asked for the essence: "A brown tumour is a reactive giant cell lesion of hyperparathyroidism that is histologically identical to giant cell tumour of bone, so I would check the calcium and PTH, confirm and classify the hyperparathyroidism, and treat the parathyroid gland first - the lesion usually regresses, and I reserve bone surgery for fracture or neural compression."
Classification
Classifying the Lesion and Its Driver
By the underlying hyperparathyroidism (the most useful classification, because it dictates treatment of the gland):
- Mechanism
- Autonomous adenoma (85%), hyperplasia, rarely carcinoma
- Biochemistry
- High Ca, high PTH
- Gland treatment
- Parathyroidectomy / adenomectomy
- Mechanism
- Reactive gland response to CKD or vitamin D deficiency
- Biochemistry
- Low/normal Ca, high phosphate, very high PTH
- Gland treatment
- Medical control; parathyroidectomy if refractory
- Mechanism
- Autonomous gland after prolonged secondary HPT
- Biochemistry
- High Ca, very high PTH
- Gland treatment
- Parathyroidectomy
Clinical Presentation
How Patients Present
- Bone pain, often diffuse
- A palpable or radiologically detected lytic lesion
- Pathological fracture through weakened bone (a common orthopaedic presentation)
- Skeletal deformity in severe, long-standing disease
- Bones: bone pain, brown tumours, fractures
- Stones: renal calculi, nephrocalcinosis
- Abdominal groans: constipation, peptic ulcer, pancreatitis
- Psychic moans: fatigue, depression, poor concentration
- Proximal muscle weakness and hyperreflexia in severe disease
- A jaw swelling referred from a dentist or maxillofacial team that turns out to be the first sign of hyperparathyroidism.
- A dialysis patient with bone pain and a lytic lesion (secondary HPT).
- An apparent giant cell tumour that does not fit - multiple lesions, abnormal calcium, or renal failure.
Examination
- Local tenderness or a firm swelling over the lesion
- Signs of the underlying disease (e.g. features of chronic kidney disease)
- Neurological assessment if a spinal lesion is suspected
Red Flags That Should Prompt a PTH Check
- A giant cell lesion in an unusual location for GCT (e.g. rib, jaw, multiple bones)
- Multiple lytic lesions
- A patient with renal failure or known hypercalcaemia
- Any giant cell lesion before a definitive operation is planned
Investigations
Biochemistry - The Key to the Diagnosis
This is the single most important investigation. A giant cell lesion of bone must have calcium and PTH checked before treatment.
- Brown tumour (HPT)
- High (primary/tertiary) or low/normal (secondary)
- Giant cell tumour
- Normal
- Brown tumour (HPT)
- Low (primary) or high (secondary)
- Giant cell tumour
- Normal
- Brown tumour (HPT)
- Raised (often markedly)
- Giant cell tumour
- Normal
- Brown tumour (HPT)
- Raised (high turnover)
- Giant cell tumour
- Usually normal
- Brown tumour (HPT)
- Often abnormal (secondary HPT)
- Giant cell tumour
- Normal
- Brown tumour (HPT)
- May be low (drives secondary HPT)
- Giant cell tumour
- Normal
Imaging
Plain Radiographs
- Well-defined, expansile lytic lesion, often with a thinned cortex
- May be solitary or multiple
- Pathological fracture may be present
- Subperiosteal resorption on the radial side of the middle phalanges - the classic hallmark
- Acro-osteolysis (terminal tuft resorption)
- Salt-and-pepper skull - granular mixed lucency and sclerosis
- Generalised demineralisation and insufficiency fractures
- Rugger-jersey spine (alternating sclerotic bands) in renal osteodystrophy
The brown tumour on its own is non-specific; it is the combination with these background signs and the biochemistry that points to the diagnosis.
Biopsy - Use With Caution
Biopsy shows giant cell-rich tissue but cannot distinguish brown tumour from giant cell tumour. If hyperparathyroidism has not been considered, a biopsy may even mislead towards an aggressive tumour diagnosis. The correct sequence is to check calcium and PTH first; biopsy is reserved for cases where the diagnosis remains uncertain after biochemistry, ideally in a specialist bone-tumour centre.

Management
Principle: Treat the Gland First
The cornerstone of management is correcting the hyperparathyroidism. Once PTH normalises, the bone turnover falls and the great majority of brown tumours regress and remineralise, often without any direct bone surgery.
- 11. Recognise and confirm
For any giant cell lesion of bone, check serum calcium, phosphate, PTH, ALP and renal function.
Raised PTH with abnormal calcium confirms a brown tumour rather than a true tumour.
- 22. Classify the hyperparathyroidism
Determine whether the cause is primary (adenoma), secondary (CKD) or tertiary.
The type dictates how the parathyroid gland is treated.
- 33. Treat the parathyroid disease
Primary/tertiary: parathyroidectomy. Secondary: control phosphate, give vitamin D analogues and calcimimetics.
PTH normalises; proceed to parathyroidectomy in secondary HPT if medically refractory.
- 44. Address the bone only if needed
Reserve bone surgery for impending or actual pathological fracture, neural compression, or a persistent symptomatic lesion.
Most lesions need no direct bone surgery once the gland is treated.
- 55. Monitor regression
Follow biochemistry and serial imaging after PTH control.
Expect remineralisation of the brown tumour over months.
Treating the Hyperparathyroidism
Surgical Cure of the Gland
- Parathyroidectomy (focused adenomectomy or exploration of all four glands depending on localisation) is the definitive treatment.
- Pre-operative localisation with ultrasound and sestamibi guides a focused approach.
- After successful surgery, calcium and PTH fall; watch for transient hypocalcaemia and, with large skeletal burden, hungry bone syndrome (rapid skeletal uptake of calcium).
- The brown tumours typically remineralise over the following months.
- Always exclude hyperparathyroidism before operating on a giant cell lesion - operating on an undiagnosed brown tumour is a classic error.
- After parathyroidectomy in patients with a large skeletal burden, anticipate hungry bone syndrome with profound, prolonged hypocalcaemia requiring aggressive calcium and vitamin D replacement.
- In secondary HPT, do not rush to bone surgery - optimise the metabolic disease first.
Complications and Prognosis
Complications
- Pathological fracture through weakened bone
- Neural compression from spinal or skull-base lesions
- Deformity and functional impairment in severe, long-standing disease
- Renal stones and nephrocalcinosis, progressive renal impairment
- Cardiovascular and soft-tissue calcification (especially in CKD)
- Severe hypercalcaemia and its systemic effects
- Hungry bone syndrome after parathyroidectomy
- Standard surgical risks if bone-directed surgery is undertaken
- Recurrence or persistence of brown tumours if the parathyroid disease is inadequately controlled
Prognosis
- The lesion itself is benign and reactive with no metastatic potential.
- With successful control of hyperparathyroidism, most brown tumours regress and remineralise, and the prognosis is excellent.
- Persistent or recurrent lesions usually reflect incompletely treated parathyroid disease rather than aggressive local behaviour.
- The overall outlook is determined largely by the underlying cause (e.g. the renal disease in secondary HPT, or the rare parathyroid carcinoma in primary HPT).
Spinal Brown Tumour and Neural Compression
An Uncommon but High-Stakes Site
The classification and complications sections both flag axial lesions with neural compression as a surgical urgency, but the specifics deserve their own treatment because a spinal brown tumour is the scenario most likely to force early bone surgery and the one most often mislabelled.
- Vertebral brown tumours are rare but, when present, an expansile lytic lesion of a vertebral body, pedicle or lamina can encroach on the cord or nerve roots.
- The presentation overlaps exactly with an aggressive tumour - a young or middle-aged adult with an expansile destructive vertebral lesion - so it is repeatedly misdiagnosed as giant cell tumour, aneurysmal bone cyst or metastasis and biopsied or resected before anyone checks the biochemistry.
- Localised spinal pain, often with radicular pain (radiculopathy) from root involvement.
- Myelopathy or cauda equina features (weakness, sensory level, sphincter disturbance) when the canal is compromised - these mandate urgent imaging and a decision about decompression.
- The neurological emergency is treated on its own merits: urgent MRI, then decompression and stabilisation where there is progressive deficit or instability, exactly as for any compressive vertebral lesion.
- The metabolic driver is still corrected in parallel - even after decompression, normalising the parathyroid disease is what allows the residual lesion to remineralise and prevents recurrence. In the reported cervical case, a young man had a C6 lesion treated initially as an osteoclastoma (giant cell tumour); only persistently high calcium and PTH revealed primary hyperparathyroidism, and the bone recovered after parathyroidectomy once the underlying disease was addressed.
The exam-safe sequence therefore is: if there is a neurological deficit, decompress and stabilise the spine now, but check calcium and PTH before and after so that the true diagnosis is not missed and the gland is treated to consolidate the result.
Q: A young adult has an expansile lytic vertebral lesion with radicular pain and a biopsy reading "giant cell-rich lesion." What must you not forget? A: Check serum calcium and PTH. A spinal brown tumour of hyperparathyroidism looks and reads identically to giant cell tumour; decompress and stabilise if there is neurological deficit, but treat the parathyroid disease to allow remineralisation and prevent recurrence.
Guidelines, Registries & Global Practice
Global Epidemiology
- Brown tumours are uncommon and becoming rarer in primary hyperparathyroidism in high-income settings, because routine calcium testing detects the disease before severe bone involvement develops.
- Secondary hyperparathyroidism from chronic kidney disease is now the leading driver globally, tracking the worldwide growth of the dialysis population.
- Common sites across populations include the pelvis, ribs, jaws and long bones; lesions may be solitary or multiple.
Side-by-Side Guidance and Consensus
- Position relevant to brown tumour
- Define surgical criteria for primary HPT (including overt skeletal disease such as brown tumours/osteitis fibrosa cystica) - these patients should undergo parathyroidectomy
- Position relevant to brown tumour
- Frame management of secondary HPT - control phosphate and calcium, use active vitamin D and calcimimetics, and consider parathyroidectomy for refractory disease
- Position relevant to brown tumour
- Lists brown tumour/osteitis fibrosa cystica among the giant cell-rich differential, emphasising correlation with biochemistry
- Position relevant to brown tumour
- Recommend pre-operative localisation (ultrasound, sestamibi) and parathyroidectomy as definitive treatment of primary and tertiary HPT
Where guidance genuinely differs, the divergence is in the threshold for parathyroidectomy in secondary HPT (earlier surgery in some centres versus prolonged medical therapy with calcimimetics in others), not in the principle that the parathyroid disease drives the lesion.
Registry and Trial Evidence
- No implant joint-registry (NJR/AJRR/AOANJRR) tracks brown tumour, because management is metabolic and reconstruction (when needed) is fixation or grafting rather than arthroplasty.
- Evidence is built from case series and multicentre retrospective cohorts (e.g. CKD-MBD oral/maxillofacial series) and from the parathyroid disease trials underpinning calcimimetic and surgical practice.
High- vs Limited-Resource Practice
- Typical pathway
- Early calcium screening, PTH assays, sestamibi/ultrasound localisation, calcimimetics and timely parathyroidectomy - severe brown tumours are now uncommon
- Typical pathway
- Later presentation with advanced osteitis fibrosa cystica and large or multiple brown tumours; reliance on plain films and clinical diagnosis; access to calcimimetics and parathyroid surgery may be limited
Any giant cell lesion of bone warrants serum calcium and PTH before definitive treatment - this simple step prevents the classic error of treating a brown tumour as a giant cell tumour.
Endocrinology, nephrology, radiology and orthopaedic oncology should jointly manage these patients, since the cure lies with the parathyroid disease rather than the bone lesion.
Memory Aids
BROWNBROWN - Core Features of Brown Tumour
Hook:A BROWN tumour is not brown trouble - check the biochemistry before you reach for the curette
BSGMBones, Stones, Groans, Moans - Hyperparathyroidism
Hook:Bones, stones, abdominal groans, and psychic moans - the classic quartet of hypercalcaemia
LYTICLYTIC - Radiology of Hyperparathyroidism
Hook:The bone reads LYTIC - lytic tumours, phalangeal resorption and a salt-and-pepper skull
MCQ Practice Points
Q: What is the single most important investigation before treating an apparent giant cell tumour of bone? A: Serum calcium and PTH. A brown tumour of hyperparathyroidism is histologically identical to giant cell tumour, so biochemistry - not histology - makes the distinction.
Q: Is a brown tumour a true neoplasm? A: No. It is a reactive, tumour-like lesion - the focal end-stage of osteitis fibrosa cystica - with no metastatic potential.
Q: What is now the most common cause of brown tumours worldwide? A: Secondary hyperparathyroidism from chronic kidney disease, reflecting the large dialysis population.
Q: What is the classic radiographic sign of hyperparathyroidism on hand films? A: Subperiosteal resorption on the radial side of the middle phalanges, often with acro-osteolysis and a salt-and-pepper skull.
Q: What is the first-line treatment of a brown tumour? A: Treat the hyperparathyroidism (parathyroidectomy in primary/tertiary HPT; medical control then surgery in refractory secondary HPT). Most lesions then regress; bone surgery is reserved for fracture or neural compression.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 45-year-old is referred with a solitary expansile lytic lesion of the proximal femur. The biopsy report says 'giant cell-rich lesion'. How would you approach this?”
“What exactly is a brown tumour, and why is it called that?”
“A patient on long-term dialysis has bone pain and multiple lytic lesions. What is happening and how would you manage it?”
“A patient with confirmed primary hyperparathyroidism and several brown tumours undergoes successful parathyroidectomy. On day one they become profoundly hypocalcaemic with tetany. What is going on and how do you manage it?”
Definition & Nature
- Focal end-stage of osteitis fibrosa cystica in hyperparathyroidism
- Reactive giant cell-rich lesion - NOT a neoplasm, no metastatic potential
- Brown colour from haemosiderin and vascularity
- Histologically identical to giant cell tumour of bone
Causes (Biochemistry)
- Primary HPT: adenoma - high Ca, low phosphate, high PTH
- Secondary HPT: CKD - low/normal Ca, high phosphate, very high PTH (commonest cause)
- Tertiary HPT: autonomous gland - high Ca, very high PTH
- Alkaline phosphatase raised (high turnover)
Imaging
- Expansile lytic lesion, solitary or multiple
- Subperiosteal resorption (radial side of middle phalanges) - hallmark
- Acro-osteolysis, salt-and-pepper skull, rugger-jersey spine
- Bone scan can mimic metastases (trap)
Management
- Treat the parathyroid disease FIRST - lesions regress
- Primary/tertiary: parathyroidectomy
- Secondary: phosphate control, vitamin D, calcimimetics; surgery if refractory
- Bone surgery only for fracture or neural compression
Pitfalls
- Never operate on a giant cell lesion without checking calcium and PTH
- Do not treat a brown tumour as a giant cell tumour
- Watch for hungry bone syndrome after parathyroidectomy
- Multiple lytic lesions - think metabolic cause, not just metastases
One-Line Answer
- Reactive giant cell lesion of hyperparathyroidism
- Diagnosis is biochemical (raised PTH, abnormal calcium)
- Treat the gland first; the lesion remineralises
- Operate on bone only for mechanical or neurological reasons
Evidence Base
Contemporary Overview of Brown Tumour of Hyperparathyroidism
- Brown tumour is the focal end-stage of osteitis fibrosa cystica driven by excess parathyroid hormone
- It is a reactive giant cell-rich lesion, not a true neoplasm, and lacks metastatic potential
- Diagnosis rests on the biochemical and clinical context because histology overlaps with giant cell tumour
- Management is directed at the underlying hyperparathyroidism, with lesion regression expected after PTH control
KRAS Mutations and MAPK/ERK Activation in Brown Tumours of the Jaws
- Targeted sequencing of 13 jaw brown tumours found activating KRAS mutations in 7 cases
- Phospho-ERK1/2 staining confirmed MAPK/ERK pathway activation in lesional mononuclear cells
- FGFR1 and TRPV4 were wild-type, distinguishing the mutational pattern from some mimics
- Places brown tumours within the RAS-driven spectrum of giant cell lesions of the jaws
Oral and Maxillofacial Manifestations of CKD-Mineral and Bone Disorder
- 21 patients with CKD-MBD; 13 had brown tumour of hyperparathyroidism, mostly in the mandible
- Mean PTH was markedly raised (around 1500 pg/mL) with high alkaline phosphatase
- Brown tumours produced well-defined radiolucencies; renal osteodystrophy gave a ground-glass appearance
- Treatment combined vitamin D, calcium, dialysis, parathyroidectomy and transplantation, with lesion resolution in several patients
Cervical Spine Brown Tumour Misdiagnosed as Giant Cell Tumour
- A 29-year-old with an expansile lytic C6 lesion was initially treated as a giant cell tumour
- Persistently high calcium and PTH revealed primary hyperparathyroidism from a parathyroid tumour
- Serum calcium and PTH normalised and the bone recovered after parathyroid surgery
- Authors recommend checking calcium and PTH whenever a giant cell tumour is considered
Bone Disease in Primary Hyperparathyroidism
- Severe primary hyperparathyroidism produces osteitis fibrosa cystica with brown tumours and cysts
- Radiographic hallmarks include subperiosteal resorption, salt-and-pepper skull and phalangeal erosions
- Bone mineral density is typically very low but is reversible after parathyroidectomy
- Marked hypercalcaemia with raised PTH and renal involvement characterises symptomatic disease