Benign Fibroelastic Pseudotumour | Subscapular Tip | Classic Sarcoma Mimic on Imaging
- Location is the diagnosis - an ill-defined mass deep to serratus anterior at the inferior scapular angle is almost always elastofibroma dorsi
- Fat strands within muscle-like tissue on CT and MRI are the key imaging feature - biopsy is not needed when the appearance is classic
- Often bilateral and asymmetric - the contralateral side should always be checked
- Completely benign pseudotumour - it is widely regarded as a reactive lesion from repetitive friction, not a true neoplasm
- A 'wait and see' approach is appropriate - surgery is reserved for symptomatic lesions, not for diagnosis
- “Examiners use this lesion to test whether you panic and call every back mass a sarcoma - the location and fat strands let you diagnose it confidently
- “It is an incidental finding on chest CT and FDG-PET/CT - mild FDG uptake (SUVmax roughly 2) must not be mistaken for metastasis
- “Strong association with repetitive shoulder use and manual labour supports the reactive (pseudotumour) theory
- “Postoperative haematoma and seroma are the main surgical hazard - marginal excision, not radical resection, is the operation
Deep to serratus anterior at the inferior scapular angle. In the imaging literature roughly 98% sit in this exact plane. The location alone is almost diagnostic and is the single most testable fact.
Muscle-like tissue interlaced with strands of fat on CT and MRI. Interspersed fat is seen in around 90% of cases on MRI and is the feature that lets you avoid biopsy.
Do not reflexively call it a sarcoma. A true soft-tissue sarcoma rarely sits deep to serratus, rarely contains interspersed fat, and is far less likely to be bilateral.
No malignant potential. Asymptomatic lesions can be observed. Surgery (marginal excision) is for symptoms, with haematoma and seroma the main complications.
- Imaging Features
- Classic site plus fat strands on CT/MRI
- Management
- Reassure and observe - no biopsy
- Key Pearl
- Location and fat strands are diagnostic
- Imaging Features
- Classic site, lesion enlarges with arm elevation
- Management
- Discuss marginal excision if it limits function
- Key Pearl
- Mechanical symptoms drive the decision to operate
- Imaging Features
- No fat strands, invasion of muscle or bone, rapid growth
- Management
- Refer to a sarcoma unit for biopsy
- Key Pearl
- Atypical features mean do not assume elastofibroma
SAFEWhy It Is NOT a Sarcoma
Hook:SAFE - the four reassuring features that make elastofibroma a SAFE diagnosis rather than a sarcoma.
FLESHDifferential of an Infrascapular Mass
Hook:FLESH covers the soft-tissue lumps under the scapula - Elastofibroma is the one defined by its location and fat strands.
Overview and Epidemiology
Elastofibroma dorsi is a benign fibroelastic pseudotumour that arises in the connective tissue between the lower scapula and the posterior chest wall, deep to the serratus anterior. Its importance in exams and clinics is not its biology - which is entirely benign - but the fact that it is a classic mimic of a soft-tissue sarcoma and a frequent incidental finding on chest imaging. Recognising the pathognomonic location and the fat strands within muscle-like tissue lets you make a confident diagnosis and avoid unnecessary biopsy or alarm.
- Age: predominantly older adults, peak in the sixth to seventh decades (mean around 60 years)
- Sex: female predominance in most surgical series
- Laterality: frequently bilateral and asymmetric - always image both sides
- Association: repetitive shoulder use and manual labour
- Often incidental - found on chest CT or FDG-PET/CT done for another reason
- Symptomatic in roughly half of surgical cohorts
- Typical symptoms: a slow-growing swelling at the scapular tip, with snapping, clunking, stiffness or mild discomfort on shoulder movement
- Pain is usually mild; rapid growth or severe pain should prompt a rethink
On FDG-PET/CT series the reported prevalence of elastofibroma dorsi is around 1.7%, and the lesions are usually bilateral with mild-to-moderate FDG uptake (SUVmax roughly 1 to 4). This metabolic activity can be misread as nodal or metastatic disease - knowing the typical appearance prevents a cancer scare and unnecessary intervention.
Pathophysiology and Anatomy
Where It Sits
The lesion occupies the space between the inferomedial border of the scapula and the underlying ribs, lying deep to the serratus anterior and latissimus dorsi. Part of the mass is typically firmly attached to the periosteum of the ribs and the intercostal fascia, while its free surface blends with surrounding fat. This anatomical relationship explains both the mechanical symptoms (the mass is compressed and displaced as the scapula glides) and the surgical challenge of a deep, poorly defined plane.
Reactive Lesion, Not a True Tumour
The most widely accepted theory is that elastofibroma is a reactive pseudotumour caused by repetitive mechanical friction between the scapula and the chest wall, rather than a true clonal neoplasm. This fits the strong association with manual labour and repetitive overhead activity, the older age at presentation, and the frequent bilaterality. Degeneration and abnormal accumulation of elastic fibres follow chronic microtrauma.
Most accepted. Chronic friction between scapula and ribs triggers fibroblastic proliferation and abnormal elastic fibre production. Supported by the manual-labour association, the older age group and bilateral disease.
Genetic and degenerative contributions. Familial clustering and recurrent chromosomal copy-number changes have been described, suggesting that in some patients an intrinsic predisposition adds to mechanical wear.
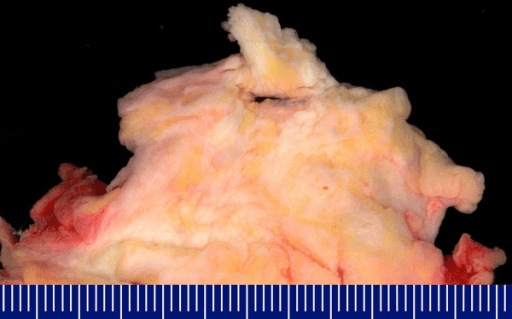
Histology
Macroscopically the lesion is a poorly circumscribed, firm, grey-white mass admixed with yellow mature fat. Microscopically the diagnostic feature is abnormal, coarse, branched and unbranched elastic fibres within a collagenous and fibrofatty stroma. These fibres can be highlighted with special stains (such as Weigert or Verhoeff-van Gieson elastin stains) and often have a beaded or globular ("chenille body") appearance. Immunohistochemistry typically shows CD34 and vimentin positivity, supporting a fibroblastic origin.
A reassuring histological point: elastofibroma shows no nuclear atypia, no high mitotic activity and no necrosis. The presence of any of these features should make the pathologist - and you - question the diagnosis and consider a true sarcoma.
Molecular Pathogenesis: Reactive Hyperplasia or Clonal Neoplasm?
The default framing above - a reactive friction pseudotumour rather than a true neoplasm - is the majority view, but it sits in tension with two observations the evidence base itself raises: familial clustering and recurrent chromosomal changes. Reconciling these is a favourite deeper viva probe, and the topic names both without developing either.
The Okinawa Endemic Cluster
The most striking evidence for a constitutional (genetic) contribution comes from Okinawa, Japan, where Nagamine and colleagues documented an extraordinarily high local frequency. In their landmark clinicopathological study of 170 cases (Cancer, 1982), many lesions arose on small offshore islands (Tonaki-jima, Aguni-jima), and a substantial proportion occurred within the same family lines - the 21 lesions from Tonaki Island showed clear familial occurrence, and 55 of the total cases clustered in related individuals. The authors concluded that elastofibroma was a reactive hyperplasia occurring against a constitutional predisposition - mechanical friction acting on a genetically susceptible background, rather than friction alone.
Genomic Findings and the Clonality Debate
Later molecular work has partly blurred the "purely reactive" label. Recurrent, non-random chromosomal copy-number changes and chromosomal instability have been described, and X-chromosome inactivation analyses have suggested that at least some lesions may be clonal - which would argue for a genuine, if extremely indolent, benign neoplasm rather than a pure reaction. Immunohistochemistry (CD34 and vimentin positivity) is consistent with a fibroblastic proliferation but does not settle the question. For exam purposes the safe, defensible position is that elastofibroma is best regarded as a benign fibroblastic pseudotumour driven by repetitive friction on a predisposed background, with the reactive-versus-neoplastic debate still unresolved.
If an examiner presses on "reactive or neoplastic?", do not commit dogmatically. State that the dominant view is reactive (friction, manual labour, older age, bilaterality), that a genetic or constitutional element is real (the Okinawa familial cluster), and that recurrent chromosomal changes with possible clonality keep a low-grade neoplastic origin on the table. Naming the Okinawa familial series is a high-level touch that signals reading beyond the basics.
Extrascapular Elastofibroma: When It Is NOT Under the Scapula
The whole topic - correctly - hammers the subscapular location as pathognomonic and treats an atypical site as a red flag for sarcoma. The nuance that completes this picture is that elastofibroma itself is not exclusively subscapular: rare, histologically identical lesions occur at other pressure and friction points, and recognising them prevents both a missed benign diagnosis and an over-called sarcoma.
Documented Extrascapular Sites
Reported extrascapular locations follow the same logic - sites subjected to chronic mechanical friction or pressure over a bony prominence. In the Okinawa series, lesions were notably common in the infraolecranon (elbow) region, and multiple lesions involving the lateral thoracic wall and the ischial tuberosities were described. Further isolated case reports place elastofibroma at the greater trochanter, foot, hand, deltoid region and even the gastrointestinal tract. The unifying theme - friction over a bony point - is exactly what the reactive theory predicts, so their very existence is an argument for that mechanism.
Why This Matters Clinically
An extrascapular mass with elastofibroma-type imaging (muscle-like tissue interlaced with fat) does not automatically become a sarcoma - but because the site is atypical, the threshold for tissue diagnosis is lower than for a textbook subscapular lesion. Away from the pathognomonic subscapular plane you lose the location-based confidence that lets you skip biopsy, so the correct posture is to keep elastofibroma on the differential for a friction-site mass while confirming histology by planned image-guided biopsy through a sarcoma service before assuming benignity.
Two-part answer for a friction-site mass. First, yes - elastofibroma can occur outside the subscapular region; infraolecranon, ischial tuberosity, greater trochanter and other pressure points are documented. Second, away from the classic subscapular plane the pretest probability of elastofibroma falls sharply, so obtain a planned biopsy rather than diagnosing on imaging alone.
SCAPULAClassic Features of Elastofibroma Dorsi
Hook:SCAPULA - the lesion lives at the SCAPULA tip, and every letter is a feature an examiner can ask about.
Classification and Staging
Practical Clinical Categories
Elastofibroma has no formal malignancy-based staging system because it is benign. In practice it is categorised by symptom status and laterality, which is what actually drives management.
- Description
- Found on imaging for another reason
- Typical Finding
- Classic site and fat strands, no complaints
- Management Direction
- Reassure and observe
- Description
- Swelling with snapping, stiffness or discomfort
- Typical Finding
- Mechanical symptoms on shoulder movement
- Management Direction
- Consider marginal excision
- Description
- Lesions on both sides, often asymmetric
- Typical Finding
- Common - both sides should be assessed
- Management Direction
- Treat the symptomatic side; observe the other
Clinical Presentation
History
Most patients are older adults, often with a history of manual or repetitive overhead work. The typical complaint is a slowly enlarging lump at the lower part of the shoulder blade, sometimes noticed by chance or by a partner. When symptomatic, patients describe snapping, clunking, stiffness or mild discomfort as the arm is raised, because the mass is compressed between the scapula and ribs during movement. Pain, if present, is usually mild; severe or rapidly progressive pain is atypical and should raise concern.
Examination
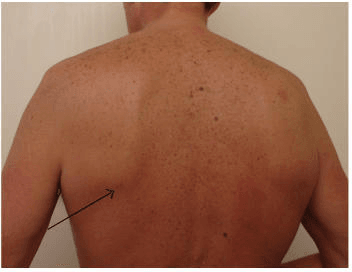
- A firm, ill-defined mass at the inferior pole of the scapula
- Becomes more prominent when the arm is adducted across the body or elevated, as the scapula slides over it
- Often non-tender; skin is normal with no overlying changes
- Reproduce the symptoms by asking the patient to elevate and lower the arm - listen and feel for snapping
- Always examine the contralateral scapula because bilateral lesions are common
- Shoulder range of movement is usually preserved but may feel mechanically restricted
The clue that distinguishes a deep scapular elastofibroma from a superficial lump is that it changes shape and becomes palpable with shoulder movement. Asking the patient to move the arm during examination is a simple, high-yield manoeuvre that examiners like to see.
Investigations
Imaging Is the Key Test
The diagnosis is made by combining the clinical picture with cross-sectional imaging. Plain radiographs are usually unhelpful and may simply show a vague soft-tissue density.
- What It Shows
- Layered (fibrillar) mass deep to serratus anterior
- Strength
- Cheap, dynamic, good first test
- Limitation
- Operator dependent; can be mistaken for lipoma
- What It Shows
- Soft-tissue mass with attenuation like muscle interlaced with fat
- Strength
- Shows the diagnostic fat strands in most cases
- Limitation
- Fat strands missed in a minority - MRI then helps
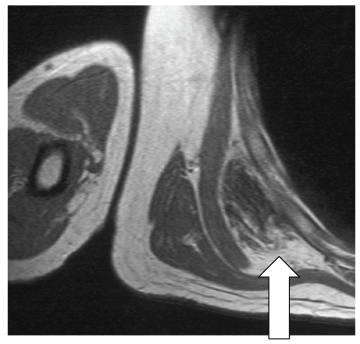
- What It Shows
- Muscle-like signal interlaced with fat on T1, deep to serratus
- Strength
- Best soft-tissue characterisation; confirms diagnosis
- Limitation
- Less available and more costly than CT or US
- What It Shows
- Mild-to-moderate uptake (SUVmax roughly 2)
- Strength
- Helps recognise it as an incidental benign finding
- Limitation
- Uptake can be mistaken for metastasis if unrecognised
The combination of a mass deep to serratus anterior at the inferior scapular angle with strands of fat interlaced through muscle-like tissue is, in the right clinical context, sufficient to diagnose elastofibroma dorsi without biopsy. On MRI interspersed fat is seen in around 90% of cases.
Role of Biopsy
When the location and imaging are classic, biopsy is unnecessary and most major series and reviews advise against it. Biopsy (image-guided core, performed through a planned route by a sarcoma service) is reserved for atypical lesions - wrong location, absent fat strands, rapid growth or invasion - where a true sarcoma cannot be excluded on imaging alone.
Management
The Overall Principle
Because elastofibroma is benign with no malignant potential, the modern default is a "wait and see" approach: confirm the diagnosis on imaging, reassure the patient, and reserve surgery for symptoms that interfere with daily life. Immediate surgery is no longer considered the standard treatment.
Management Pathway
Combine the clinical picture (older adult, scapular-tip mass, mechanical symptoms, manual-labour history) with cross-sectional imaging showing the classic site and fat strands. Check the other side.
For asymptomatic or minimally symptomatic lesions, reassure the patient that this is benign and offer clinical follow-up. No biopsy and no surgery are required.
For lesions causing pain, mechanical snapping or functional limitation, offer marginal (not radical) surgical excision through the deep subscapular plane.
Anticipate haematoma and seroma. Use careful haemostasis, suction drainage, quilting or obliteration of the dead space, and a compression dressing.
Complications
- Why It Happens
- Vascular deep bed and large dead space
- Management
- Usually conservative; evacuate if large or expanding
- Prevention
- Meticulous haemostasis, suction drainage
- Why It Happens
- Persistent dead space after excision
- Management
- Needle aspiration or compression; rarely re-drainage
- Prevention
- Dead-space obliteration, prolonged drainage, compression
- Why It Happens
- Collection or deep wound in an older patient
- Management
- Antibiotics; drainage if collection becomes infected
- Prevention
- Aseptic technique, avoid persistent collections
- Why It Happens
- Incomplete removal (uncommon)
- Management
- Re-excision if symptomatic recurrence is confirmed
- Prevention
- Complete marginal excision; the lesion rarely recurs
- Why It Happens
- Failure to recognise classic site and fat strands
- Management
- Review imaging; refer to sarcoma unit if truly uncertain
- Prevention
- Know the pathognomonic features - avoid needless biopsy and alarm
The most important safety caveat is to abandon the benign assumption if the lesion is atypical - wrong location, no fat strands, rapid growth, severe pain, or invasion of muscle or bone. In that situation refer to a bone-and-soft-tissue tumour service for assessment and image-guided biopsy before any surgery.
Clinical Relevance and Exam Focus
Elastofibroma dorsi is a perfect viva trap: it is a back mass in an older patient that mimics a sarcoma. Candidates who default to "this is a sarcoma until proven otherwise" without recognising the pathognomonic location and fat strands look unsafe at one extreme, while candidates who biopsy or radically excise every classic lesion look over-aggressive at the other. The examiner is testing whether you can be confident and conservative when the picture is classic, yet appropriately cautious when it is not.
- Location - deep to serratus anterior at the inferior scapular angle
- Imaging - muscle-like tissue with interspersed fat strands
- Often bilateral - check the other side
- Benign pseudotumour - reactive, no malignant potential
- Manage by symptoms - observe if quiet, marginal excision if symptomatic
- Calling every classic lesion a sarcoma
- Biopsying a radiologically classic lesion
- Performing radical resection instead of marginal excision
- Forgetting to warn about haematoma and seroma
- Misreading FDG uptake as metastatic disease
Guidelines, Registries & Global Practice
Global Epidemiology
Elastofibroma dorsi is reported worldwide with a consistent profile: it predominantly affects older adults (peak in the sixth and seventh decades), shows a female predominance in most surgical series, and arises almost exclusively in the subscapular region. Although historically called rare, autopsy and cross-sectional imaging work shows it is far commoner than once thought - incidental imaging series report a prevalence of roughly 1.7% on FDG-PET/CT, with bilateral lesions in a large proportion of those patients. There is no dedicated tumour registry for this benign entity; epidemiology derives from radiology, pathology and orthopaedic-oncology case series rather than national implant registries.
Guideline Framework (Side-by-Side)
- Relevant guidance
- Listed among benign fibroblastic/fibrohistiocytic lesions
- Practical implication
- Confirms benign biology; histology not required when imaging is classic
- Relevant guidance
- Indeterminate or aggressive-appearing soft-tissue masses should be referred to a sarcoma unit before biopsy
- Practical implication
- Refer only atypical lesions; classic elastofibroma needs no referral
- Relevant guidance
- Diagnostic uncertainty or aggressive features trigger sarcoma-unit referral
- Practical implication
- A confidently diagnosed elastofibroma is managed locally
- Relevant guidance
- Latent benign soft-tissue lesions (Enneking stage 1) may be observed
- Practical implication
- Excision reserved for symptomatic lesions
No major society mandates routine biopsy or specialist referral for a radiologically classic elastofibroma dorsi.
- MRI readily available to characterise the lesion and confirm fat strands
- CT and PET/CT commonly identify it as an incidental finding during cancer staging
- Histology easily obtained when a symptomatic lesion is excised
- Ultrasound is an excellent, inexpensive first-line test for a subscapular mass
- The classic location plus a layered (fibrillar) appearance supports a confident working diagnosis
- Marginal excision with careful dead-space management treats symptomatic lesions where surgery is needed
Across FRCS (Tr and Orth), FRACS, EBOT, ABOS and DNB/MS exams, be ready to describe the pathognomonic subscapular location and the fat strands within muscle-like tissue on CT and MRI, to explain why this is a benign reactive pseudotumour rather than a sarcoma, and to justify a symptom-led approach - observation for quiet lesions versus marginal excision (with counselling about haematoma and seroma) for symptomatic ones.
MCQ Practice Points
Q: Where does elastofibroma dorsi characteristically arise? A: Deep to the serratus anterior at the inferior angle of the scapula, between the lower scapula and the posterior chest wall. This location is almost pathognomonic.
Q: What imaging feature allows a confident diagnosis without biopsy? A: Strands of fat interlaced through muscle-like soft tissue at the classic subscapular site, seen on CT or MRI (interspersed fat present in around 90% of cases on MRI).
Q: How often is elastofibroma dorsi bilateral? A: Frequently - a large minority of cases (and a high proportion of incidental PET/CT cases) are bilateral and asymmetric, so always check the other side.
Q: What is the most accepted cause of elastofibroma dorsi? A: A reactive pseudotumour from repetitive mechanical friction between the scapula and chest wall, supported by the strong association with manual labour - it is not regarded as a true neoplasm.
Q: What is the dominant complication after surgical excision? A: Postoperative haematoma or seroma, reported in up to around 40% of cases, related to the large dead space; most resolve with conservative treatment.
Q: When is surgery indicated for elastofibroma dorsi? A: For symptomatic lesions (pain, snapping, functional limitation). Asymptomatic lesions are observed; immediate surgery for diagnosis alone is no longer standard.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 63-year-old retired carpenter is referred with a slowly growing firm lump under his right shoulder blade. It snaps when he reaches across his body. On examination there is an ill-defined mass at the inferior pole of the scapula that becomes more obvious when he elevates the arm. How would you approach this?”
“A 68-year-old woman being staged for breast cancer has a chest CT that reports bilateral soft-tissue masses deep to the serratus anterior at the scapular tips, with mild FDG uptake on her subsequent PET/CT. The oncology team is worried about metastases. How do you interpret this?”
“A 55-year-old man has a rapidly enlarging, painful mass near the lower scapula. Imaging shows a mass that is partly superficial to serratus anterior, contains no fat strands, and appears to invade adjacent muscle. A trainee suggests this is just an elastofibroma. How do you respond and what do you do?”
Key Facts
- Benign fibroelastic pseudotumour of the subscapular region
- Older adults (peak 6th-7th decade), female predominance
- Frequently bilateral and asymmetric - check both sides
- No malignant potential - reactive friction lesion
Pathognomonic Features
- Location: deep to serratus anterior at the inferior scapular angle (~98%)
- Imaging: muscle-like tissue interlaced with strands of fat (~90% on MRI)
- Dynamic mass - snapping or clunking with shoulder movement
- Mild-to-moderate FDG uptake (SUVmax roughly 2) - not metastasis
Clinical Presentation
- Often incidental on chest CT or PET/CT
- Symptomatic in roughly half - swelling, snapping, stiffness, mild pain
- Strong association with manual labour and repetitive shoulder use
- Mass more prominent on arm elevation or adduction across the body
Investigations
- MRI is the key test - confirms classic site and fat strands
- CT shows fat strands in most cases; MRI rescues CT-negative cases
- Ultrasound is a good inexpensive first test
- Biopsy only for atypical lesions (wrong site, no fat, rapid growth)
Management
- Asymptomatic: reassure and observe (wait and see)
- Symptomatic: marginal excision (not radical resection)
- Anticipate haematoma and seroma - drainage and dead-space control
- Excellent prognosis; recurrence rare after complete excision
Exam Pearls
- Location plus fat strands = diagnosis without biopsy
- Classic sarcoma mimic - be confident yet cautious
- Always check the contralateral scapula (often bilateral)
- Postoperative haematoma/seroma is the dominant complication
Evidence Base and Key Studies
Current Update on the Diagnosis, Management and Pathogenesis of Elastofibroma Dorsi
- Comprehensive review framing elastofibroma dorsi as an uncommon benign fibroblastic pseudotumour of the subscapular region in middle-aged and older adults
- MRI is the recommended first-line investigation, showing a lenticular soft-tissue mass with signal similar to skeletal muscle interlaced with strands of fat
- Biopsy is not necessary when all pathognomonic criteria are present
- A conservative wait-and-see approach is reasonable - immediate surgery is no longer the standard treatment
Imaging Diagnosis of Thoracic Elastofibroma Dorsi
- Retrospective review over 12 years identifying 409 suspected cases; typical imaging analysed in 310 lesions
- Classic location was a mass deep to the serratus anterior (98%) near the scapular tip (98%)
- Interspersed intralesional fat was present in 87% of CT and 90% of MRI studies; MRI showed fat in 88% of CT cases that lacked it
- True tumours were rarely deep to serratus (17%) or at the scapular tip (25%) and almost never contained interspersed fat