Rare Benign Intraosseous Fibromatosis | Locally Aggressive | High Recurrence
- Desmoplastic fibroma is the intraosseous counterpart of soft-tissue desmoid tumour (aggressive fibromatosis)
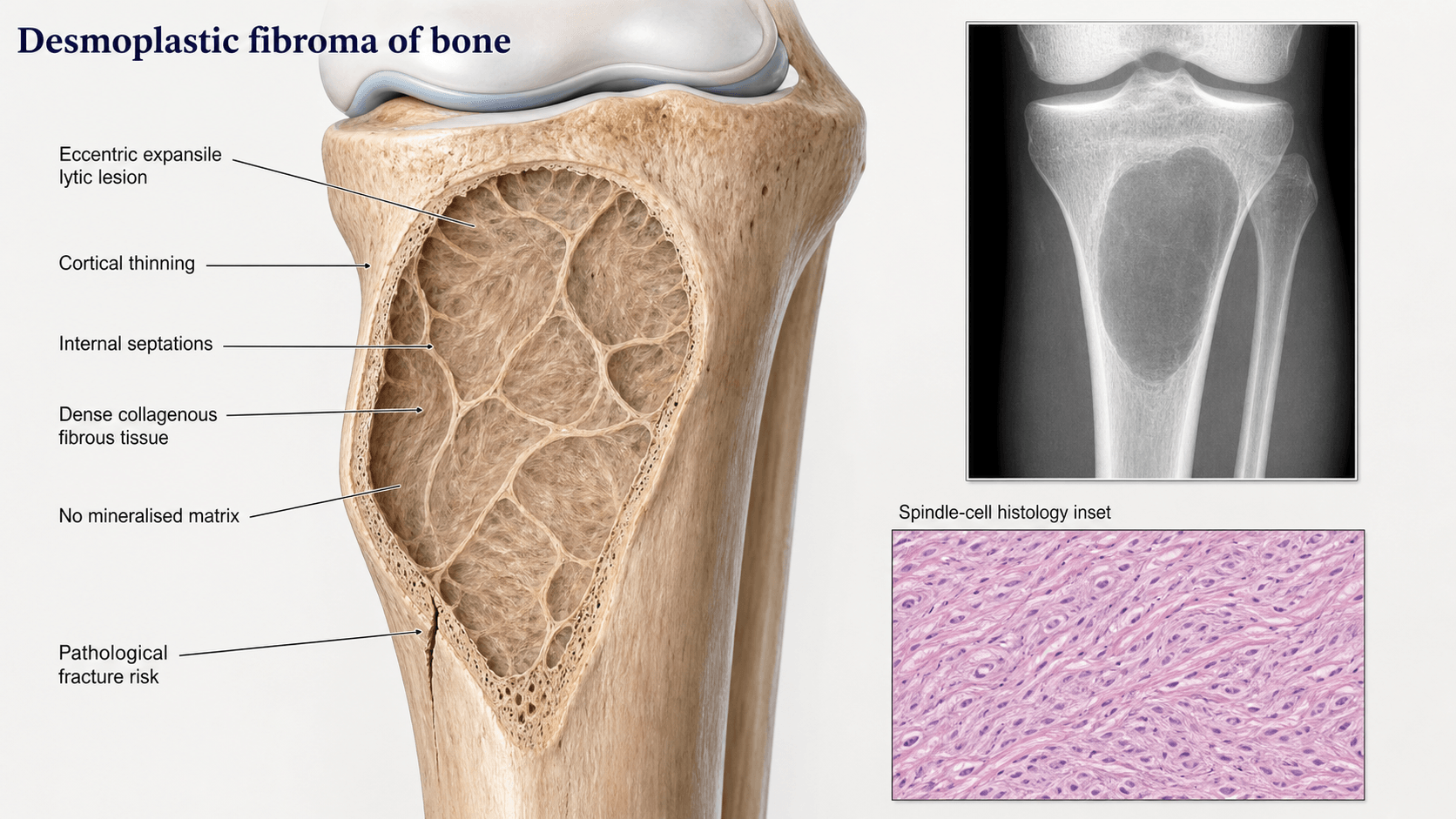
- Radiographically appears as a well-defined lytic lesion with internal trabeculation (honeycomb / soap-bubble)
- Histologically mimics low-grade fibrosarcoma but shows no cytological atypia, no mitoses, and no necrosis
- Intralesional curettage carries high recurrence (17-72%) — wide excision is the gold standard
- Must be differentiated from low-grade central osteosarcoma, fibrous dysplasia, and giant cell tumour
- “Think desmoplastic fibroma in a young patient with a lytic, trabeculated metaphyseal lesion
- “Histology: bland fibroblasts in abundant collagen, NO atypia, NO significant mitoses
- “Curettage alone has unacceptably high recurrence — always discuss wide excision
- “CT and MRI define cortical breakthrough and soft-tissue extension better than plain films
Benign but locally aggressive intraosseous fibromatosis. Clonal proliferation of myofibroblasts producing abundant collagen. Does not metastasise but destroys bone locally and recurs aggressively if inadequately excised.
Misdiagnosis as low-grade osteosarcoma leads to unnecessary radical surgery or chemotherapy. Conversely, under-treatment with curettage alone leads to recurrence in up to 72 percent of cases.
Bland spindle cells in dense collagenous stroma. No nuclear atypia, no atypical mitoses, no necrosis. Features overlap with desmoid tumour of soft tissue. Beta-catenin nuclear staining is often positive.
Wide excision is gold standard. Curettage alone is associated with high recurrence (17-72 percent). Adjuvants (phenol, cryotherapy, cement) may improve curettage outcomes but evidence is limited.
- Diagnosis
- Lytic lesion with honeycomb trabeculation on X-ray
- Treatment
- Wide resection with negative margins
- Key Pearl
- Most common site overall is the mandible
- Diagnosis
- MRI shows cortical thinning, no soft-tissue mass
- Treatment
- Wide excision and reconstruction
- Key Pearl
- Long-bone lesions in metaphysis, respect growth plate
- Diagnosis
- Biopsy confirms bland fibroblasts, no atypia
- Treatment
- Re-resection with wide margins mandatory
- Key Pearl
- Recurrence signals inadequate initial margins
FAMEDesmoplastic Fibroma Site Distribution
Hook:Think FAME — Femur and Mandible are the hallmark sites for this rare entity!
BLANDHistology vs Mimics
Hook:BLAND histology keeps it benign — desmoplastic fibroma never shows cytological atypia!
Overview and Epidemiology
Desmoplastic fibroma of bone is the rarest primary bone tumour, accounting for less than 0.3 percent of all primary bone neoplasms. It is the intraosseous counterpart of the extra-abdominal desmoid tumour (aggressive fibromatosis). Although histologically benign and never metastasising, it is locally aggressive with a propensity for cortical destruction and local recurrence that mirrors low-grade malignancy. Misdiagnosis as fibrosarcoma or low-grade osteosarcoma can lead to overly aggressive treatment, while under-treatment with simple curettage leads to recurrence in the majority of patients.
- Incidence: Less than 0.3 percent of primary bone tumours
- Age: 10-30 years (peak in second decade), but ranges from childhood to elderly
- Sex: Roughly equal male-to-female distribution
- Over 300 cases reported in the literature as case reports and small series
- Local destruction: Progressive bone resorption, cortical expansion, pathological fracture
- Recurrence: 17-72 percent after intralesional treatment, under 10 percent after wide excision
- No metastasis: Benign biological behaviour — no distant spread
- Morbidity: Mainly from local destruction and surgical complications of wide resection
Pathophysiology
Desmoplastic fibroma is a clonal neoplastic proliferation of myofibroblasts that produce abundant type I and type III collagen. It represents the intraosseous counterpart of soft-tissue desmoid tumour (extra-abdominal fibromatosis). Molecular studies have identified mutations in the Wnt / beta-catenin pathway (CTNNB1 gene mutations) and APC gene alterations, the same pathways implicated in soft-tissue desmoid tumours. The lesion grows slowly but relentlessly, expanding and thinning the cortex, often producing a characteristic expansile lytic appearance. It does not metastasise but causes significant local bone destruction. The high local recurrence rate after incomplete excision reflects its infiltrative growth pattern at the tumour-bone interface.
- Gene
- CTNNB1 (beta-catenin)
- Frequency
- Commonly mutated
- Significance
- Nuclear beta-catenin staining on immunohistochemistry supports the diagnosis
- Gene
- APC
- Frequency
- Less frequent
- Significance
- Same pathway as CTNNB1 — may be associated with familial adenomatous polyposis
- Gene
- Trisomy 8, 20
- Frequency
- Reported in some cases
- Significance
- Non-specific but supports clonal neoplastic nature
Intraosseous origin: Begins within medullary cavity
Expansion: Slowly expands cortex from within
Cortical thinning: Progressive, may breach cortex
Soft-tissue extension: Possible in advanced cases but no true capsule
No mineralisation: Lesion itself produces no osteoid or matrix
Infiltrative margins: Tumour sends finger-like projections into surrounding bone
No capsule: Unlike benign cysts, no clear demarcation
Curettage leaves pockets: Residual tumour cells in bony interstices
Slow growth masks recurrence: May take 1-5 years to become radiographically evident
Adjuvants help but do not replace wide margins
Classification and Types
Classification by Anatomical Location
- Frequency
- Most common single site (over 20 percent)
- Typical Age
- 10-30 years
- Surgical Challenge
- Resection with margin, reconstruct with fibula graft
- Frequency
- Most common long bone
- Typical Age
- 10-25 years
- Surgical Challenge
- Wide excision, allograft or endoprosthesis
- Frequency
- Second most common long bone
- Typical Age
- 10-30 years
- Surgical Challenge
- Subcutaneous location aids surgical access
- Frequency
- Reported but uncommon
- Typical Age
- Young adult
- Surgical Challenge
- Difficult access, high morbidity of wide excision
- Frequency
- Rare but documented
- Typical Age
- Variable
- Surgical Challenge
- Neurological risk, en-bloc resection technically demanding
The mandible is the single most commonly reported anatomical site. In long bones, the metaphysis is the typical zone of origin, with extension into the diaphysis in larger lesions.
Clinical Assessment
- Pain: Slowly progressive, often mild for months
- Swelling: Gradually enlarging mass (especially mandible or tibia)
- Duration: Symptoms present for months to years before diagnosis
- Pathological fracture: May be the presenting event in weight-bearing bones
- Dental symptoms: Mandibular lesions — loose teeth, difficulty chewing
- Palpable mass: Bony-hard, non-tender or mildly tender
- No regional lymphadenopathy: Benign lesion, no nodal spread
- No systemic features: No weight loss, fever, or malaise
- Neurovascular status: Intact unless spine or pelvis involved
- Adjacent joints: Assess range of motion if near articular surface
Desmoplastic fibroma is so rare that it is almost never the first diagnosis considered for a lytic bone lesion. The key is recognising the combination of: young patient, well-defined lytic lesion with internal trabeculation, no matrix mineralisation, and no aggressive periosteal reaction. Always include it in the differential for a trabeculated lytic metaphyseal lesion in a young patient, especially in the mandible or femur.
- Key Features
- Lytic with honeycomb trabeculation, no matrix
- Discriminating Finding
- Bland fibroblasts in dense collagen, beta-catenin positive
- Confirmatory Test
- Biopsy with immunohistochemistry
- Key Features
- Lytic, may have subtle matrix, permeative margins
- Discriminating Finding
- Mild atypia, osteoid production by tumour cells
- Confirmatory Test
- Careful histological review, CT for subtle mineralisation
- Key Features
- Ground-glass matrix, long-bone involvement
- Discriminating Finding
- Woven bone spicules without osteoblastic rimming, GNAS mutation
- Confirmatory Test
- CT for matrix pattern, molecular testing
- Key Features
- Epiphyseal, extends to articular surface
- Discriminating Finding
- Osteoclast-like giant cells, RANKL overexpression
- Confirmatory Test
- MRI shows typical epiphyseal-metaphyseal location
- Key Features
- Expansile lytic, fluid-fluid levels
- Discriminating Finding
- Blood-filled spaces, no solid cellular stroma
- Confirmatory Test
- MRI shows fluid-fluid levels characteristic
- Key Features
- Eccentric metaphyseal, scalloped border
- Discriminating Finding
- Storiform fibrous tissue with giant cells, foamy histiocytes
- Confirmatory Test
- Usually incidental, regresses spontaneously
Low-grade central osteosarcoma is the most important differential. Both occur in young adults, both produce a lytic metaphyseal lesion, and both have bland spindle cells on histology. The critical difference is that low-grade osteosarcoma produces osteoid directly from tumour cells, even if subtle. Always request MDT review and ensure an experienced bone pathologist examines the biopsy, because misclassifying either direction leads to undertreatment or overtreatment.
Investigations
Imaging Protocol
Views: AP and lateral of the affected bone — panoramic dental view for mandibular lesions
Look for: Well-defined lytic lesion, internal trabeculation (honeycomb), cortical thinning or expansion, no matrix mineralisation, no periosteal reaction
Clinical correlation: Plain films are often suggestive but not diagnostic — advanced imaging is always needed
Sequences: T1, T2, STIR, post-gadolinium T1 fat-sat
Findings: Low-to-intermediate T1 signal, low-to-intermediate T2 signal (reflecting fibrous collagen content), homogeneous gadolinium enhancement
Key assessment: Extent within medullary canal, cortical breakthrough, soft-tissue extension, relationship to neurovascular structures and joint
MRI pearl: The low T2 signal helps differentiate desmoplastic fibroma from other lytic lesions, which typically show high T2 signal
Indication: Best for assessing cortical integrity, internal trabeculation pattern, and matrix characteristics
Findings: Lytic lesion with coarse internal bony septa, cortical thinning, no mineralised matrix
Surgical planning: Defines the bony anatomy for resection and reconstruction planning, especially in the mandible and pelvis
Approach: Core needle biopsy preferred (adequate tissue for histology and immunohistochemistry)
Principles: Biopsy tract must be in the planned surgical field (excised en-bloc at definitive surgery)
MDT discussion: Biopsy should only be performed after imaging is complete and the case has been discussed at a multidisciplinary bone tumour meeting
Caution: Desmoplastic fibroma can be sampled inadequately — ensure sufficient tissue for specialist review
The low T2 signal on MRI is a distinguishing feature — most other lytic bone lesions (GCT, ABC, fibrous dysplasia) show high T2 signal due to fluid or cellular content. The low T2 in desmoplastic fibroma reflects its dense collagenous stroma. If you see a lytic bone lesion with low T2 signal and homogeneous gadolinium enhancement, think desmoplastic fibroma.
Management Algorithm
Enneking Surgical Margins (the language of resection)
Every treatment decision below is expressed in Enneking margin terms, so define them first. The margin is named by the plane of dissection relative to the tumour and its reactive zone.
- Plane of dissection
- Through the tumour (curettage, debulking)
- What is left behind
- Macroscopic and microscopic tumour
- Role in desmoplastic fibroma
- Curettage - high recurrence (17-72%); selected expendable sites only
- Plane of dissection
- Through the reactive zone / pseudocapsule (extracapsular but within the inflammatory zone)
- What is left behind
- Microscopic satellite/skip foci
- Role in desmoplastic fibroma
- Marginal excision - intermediate recurrence; when wide margins are anatomically impossible
- Plane of dissection
- Through normal tissue, removing the tumour with a cuff of normal tissue (intracompartmental)
- What is left behind
- Nothing locally (in the ideal case)
- Role in desmoplastic fibroma
- The GOLD STANDARD - recurrence under 10%
- Plane of dissection
- Removes the entire compartment containing the tumour
- What is left behind
- Nothing in that compartment
- Role in desmoplastic fibroma
- Rarely needed for a benign lesion; reserved for extensive disease
Wide Excision — Gold Standard
Goal: En-bloc resection with negative margins to minimise recurrence
Treatment Protocol
Staging: Complete local imaging (MRI + CT), systemic staging if diagnosis uncertain
MDT discussion: Bone tumour board to confirm diagnosis and surgical plan
Biopsy review: Confirm diagnosis with expert musculoskeletal pathologist before committing to wide excision
Reconstruction planning: Plan bone graft, allograft, or endoprosthesis at the same sitting
Margins: Wide margins (cuff of normal tissue around the lesion)
En-bloc resection: Do not violate the tumour capsule
Biopsy tract: Excise the entire biopsy tract en-bloc with the specimen
Reconstruction: Immediate reconstruction with structural allograft, vascularised fibula graft, or endoprosthesis depending on location and defect size
Functional rehabilitation: Guided by reconstruction type and anatomical site
Monitoring: Serial imaging at 3, 6, 12 months then annually for at least 5 years
Recurrence detection: MRI is the most sensitive modality for local recurrence
Wide excision reduces recurrence from 17-72 percent (curettage) to under 10 percent. For mandibular lesions, this means segmental resection with fibula free-flap reconstruction. For femoral or tibial lesions, it means en-bloc resection with intercalary allograft or vascularised fibula grafting. The morbidity of wide excision must be justified — that is why expert biopsy confirmation is mandatory before proceeding.
WIDERTreatment Approach
Hook:Go WIDER with your margins — inadequate excision is the number-one cause of recurrence!
Complications
- Incidence
- 17-72 percent after curettage, under 10 percent after wide excision
- Risk Factors
- Intralesional margins, infiltrative growth pattern
- Management
- Re-resection with wide margins — repeat imaging surveillance
- Incidence
- Variable, depends on lesion size and bone involved
- Risk Factors
- Large lesions, weight-bearing bones, cortical breakthrough
- Management
- Internal fixation at time of resection or curettage
- Incidence
- Depends on surgical approach and reconstruction
- Risk Factors
- Articular surface involvement, peri-articular surgery
- Management
- Early rehabilitation, physiotherapy-guided mobilisation
- Incidence
- Reported in skeletally immature patients
- Risk Factors
- Physeal involvement or damage during surgery
- Management
- Monitor growth, epiphysiodesis of contralateral limb if needed
- Incidence
- 15-25 percent of structural allografts
- Risk Factors
- Large allograft, poor host bone quality, infection
- Management
- Revision fixation, vascularised graft conversion
- Incidence
- Standard surgical risk, higher with allograft
- Risk Factors
- Large reconstructive procedures, prolonged operative time
- Management
- Antibiotic prophylaxis, aggressive treatment if occurs
Recurrence is the defining clinical challenge of desmoplastic fibroma. Unlike most benign bone tumours, it recurs aggressively after intralesional treatment. The time to recurrence ranges from months to years, mandating long-term surveillance for a minimum of 5 years after surgery. Each recurrence may require progressively more extensive surgery, reinforcing the importance of getting it right the first time with adequate margins.
Outcomes and Prognosis
- Recurrence Rate
- Under 10 percent
- Functional Outcome
- Good to excellent (dependent on site)
- Key Consideration
- Gold standard — higher initial morbidity but best long-term control
- Recurrence Rate
- 10-25 percent (estimated)
- Functional Outcome
- Good functional outcomes
- Key Consideration
- Acceptable when wide margins are anatomically impossible
- Recurrence Rate
- 50-72 percent
- Functional Outcome
- Good initially but recurrence common
- Key Consideration
- Acceptable only for expendable bones or extreme surgical morbidity
- Recurrence Rate
- 15-30 percent (varies by adjuvant)
- Functional Outcome
- Good functional outcomes
- Key Consideration
- Adjuvants improve local control but do not equal wide excision
Best prognosis: Wide excision with negative margins, small lesion size, accessible anatomical site (tibia, fibula)
Poor prognosis: Intralesional surgery, large lesions with cortical breakthrough, challenging anatomical sites (pelvis, spine), young age (more growth-related morbidity)
Key message: Desmoplastic fibroma never metastasises and never causes death from disease, but it can cause significant morbidity from local recurrence and surgical reconstruction. The prognosis for local control is overwhelmingly determined by the adequacy of the initial surgical margins.
Guidelines, Registries & Global Practice
- Extremely rare with no geographic or ethnic predilection reported
- Over 300 cases documented in the published literature worldwide
- No large population-based registries exist due to tumour rarity
- Incidence data derived from referral centre case series rather than population cancer registries
- High-resource: Wide excision with advanced reconstruction (vascularised grafts, endoprostheses, free flaps) at specialist bone tumour centres
- Limited-resource: Curettage with local adjuvants may be the only feasible approach — referral to specialist centres when possible
- Universal principle: Diagnosis must be confirmed by biopsy and expert pathology review before any definitive surgery, regardless of resource setting
- Surgery: Desmoplastic fibroma management is concentrated in specialist orthopaedic oncology and maxillofacial units globally
- Diagnosis Emphasis
- Biopsy with expert pathology — MRI staging — MDT review mandatory
- Treatment Recommendation
- Wide excision gold standard — curettage only when resection causes unacceptable morbidity
- Follow-up
- Serial MRI for minimum 5 years
- Diagnosis Emphasis
- Core needle biopsy — nuclear beta-catenin IHC helpful — exclude low-grade osteosarcoma
- Treatment Recommendation
- En-bloc resection with wide margins — adjuvant cryotherapy or phenol when wide margins impossible
- Follow-up
- Long-term surveillance, MRI-based
- Diagnosis Emphasis
- Systematic biopsy protocol — CT and MRI staging
- Treatment Recommendation
- Wide excision preferred — extended curettage with adjuvants for selected cases
- Follow-up
- Radiographic surveillance annually for 5 years minimum
There is no dedicated international registry for desmoplastic fibroma. The evidence base consists entirely of retrospective case series and systematic reviews of published cases. No randomised controlled trials exist, and none are feasible given the tumour's extreme rarity. Treatment recommendations are therefore principle-based: confirm diagnosis with expert pathology, achieve the widest margins surgically possible, and monitor for recurrence with serial MRI.
In every suspected case of desmoplastic fibroma:
- Biopsy must be performed at a centre capable of definitive surgical management
- Imaging (MRI + CT) must be completed before biopsy
- Pathology must be reviewed by a specialist musculoskeletal pathologist
- MDT discussion must occur before committing to any surgical approach
- If wide excision cannot be performed locally, the patient must be referred to a specialist centre before any surgical intervention
A missed diagnosis of low-grade osteosarcoma (undertreated as desmoplastic fibroma) or an inadequate initial surgery (curettage where wide excision was feasible) are the two most significant management errors in this rare tumour.
Controversies & Areas of Uncertainty
Soft-tissue desmoid tumours respond to NSAIDs, hormonal therapy (tamoxifen), and tyrosine kinase inhibitors (imatinib, sorafenib). There are anecdotal reports of medical therapy for desmoplastic fibroma of bone, but no robust evidence. Given the molecular similarity (Wnt / beta-catenin pathway), these agents are biologically plausible but remain unproven in the intraosseous setting.
Radiotherapy has been used in soft-tissue desmoid tumours and has been reported sporadically for desmoplastic fibroma of bone when surgical resection is impossible. Concerns include radiation-induced sarcoma in a young patient population. Radiotherapy is not standard treatment and should only be considered in unresectable, progressive disease after MDT discussion.
The optimal balance between local control and functional morbidity is debated for anatomically challenging sites (pelvis, spine). Extended curettage with cryotherapy or phenol may achieve reasonable local control in selected cases, but evidence is limited to case reports and small series. Wide excision remains the standard when surgically feasible.
Recurrence has been reported up to many years after initial surgery. Most protocols recommend 5 years of surveillance, but there is no consensus on whether lifelong monitoring is warranted. The very late recurrence potential (similar to soft-tissue desmoid tumours) argues for extended follow-up in high-risk patients.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“An 18-year-old male presents with a 6-month history of progressive right knee pain. Plain radiographs demonstrate a well-defined lytic lesion in the distal femoral metaphysis with internal trabeculation producing a honeycomb pattern. There is cortical thinning but no cortical breakthrough. No periosteal reaction or soft-tissue mass is seen. MRI shows a lesion with low T2 signal and homogeneous gadolinium enhancement. Core needle biopsy shows bland spindle cells in a dense collagenous stroma with no mitoses, no atypia, and no osteoid production. What is your diagnosis and management plan?”
“A 24-year-old woman presents with a slowly enlarging right mandibular swelling 3 years after curettage of a lytic mandibular lesion at another institution. The original pathology was reported as a benign fibrous lesion. Current imaging shows a recurrent lytic lesion in the mandibular body with honeycomb trabeculation and buccal cortical breakthrough. Review of the original slides at your institution shows bland spindle cells in dense collagen with positive nuclear beta-catenin staining. What is the diagnosis and how would you manage the recurrence?”
Key Facts
- Rarest primary bone tumour — less than 0.3 percent of all bone tumours
- Intraosseous counterpart of soft-tissue desmoid tumour (aggressive fibromatosis)
- Peak age 10-30 years, mandible and femoral metaphysis most common sites
- Benign — never metastasises — but locally aggressive with high recurrence
Diagnosis
- X-ray: well-defined lytic lesion with honeycomb trabeculation, no matrix, no periosteal reaction
- MRI: low T2 signal (dense collagen), homogeneous gadolinium enhancement
- Biopsy: bland spindle cells in dense collagen, no atypia, no mitoses, no necrosis
- IHC: nuclear beta-catenin positive — CTNNB1 mutations on molecular testing
Critical Differential
- Low-grade central osteosarcoma: must exclude — shows osteoid production by tumour cells
- Fibrous dysplasia: ground-glass matrix, GNAS mutation, different histology
- Giant cell tumour: epiphyseal location, osteoclastic giant cells
- ABC: fluid-fluid levels on MRI, blood-filled spaces on histology
Treatment
- Wide excision = gold standard (recurrence under 10 percent)
- Curettage alone = unacceptable (recurrence 50-72 percent)
- Curettage with adjuvants (phenol, cryotherapy, cement) = 15-30 percent recurrence
- Reconstruction at time of resection: allograft, vascularised fibula, or endoprosthesis
Follow-up
- Serial MRI at 3, 6, 12 months then annually for at least 5 years
- Recurrence can occur years later — long-term vigilance required
- No role for chemotherapy or radiotherapy in standard management
- Medical therapy (NSAIDs, TKIs) unproven but biologically plausible for unresectable disease
Evidence Base and Key Trials
Desmoplastic fibroma of bone
- One of the largest single-institution case series from Mayo Clinic
- Confirmed the locally aggressive nature with high recurrence after intralesional treatment
- Wide excision recommended as the treatment of choice
- Histological criteria for distinguishing from low-grade fibrosarcoma and osteosarcoma emphasised
Desmoplastic fibroma of bone. A report of six cases
- Landmark Italian series from one of the world's largest bone tumour centres (Rizzoli Institute)
- Described the characteristic radiographic pattern of lytic lesion with internal trabeculation
- Reported recurrence rates stratified by surgical margin
- Emphasised the importance of differentiating from low-grade central osteosarcoma
Desmoplastic fibroma of bone: an immunohistochemical study including beta-catenin expression and mutational analysis for beta-catenin
- Demonstrated nuclear beta-catenin accumulation by immunohistochemistry in desmoplastic fibroma
- CTNNB1 mutations identified in a subset of cases
- Same molecular pathway as soft-tissue desmoid tumours confirmed
- Nuclear beta-catenin staining serves as a useful diagnostic adjunct
Desmoplastic fibroma of the bone. A report of two patients, review of the literature, and therapeutic implications
- Comprehensive literature review of desmoplastic fibroma cases up to 1996 with two new case reports
- Confirmed that intralesional curettage alone carries recurrence rates exceeding 50 percent
- Wide excision recommended as the treatment of choice whenever anatomically feasible
- Reviewed the clinical, radiographic, and histological spectrum of the disease
Desmoplastic fibroma of bone: A rare bone tumour
- Series from the Royal Orthopaedic Hospital Birmingham, a major UK bone tumour centre
- Highlighted the high local recurrence rate after intralesional treatment
- Recommended wide excision as the definitive treatment, with curettage reserved for expendable sites
- Emphasised the importance of specialist MDT management for this rare tumour