Aggressive Fibromatosis | Locally Aggressive Benign | Surveillance-First Approach
- Desmoid tumors NEVER metastasize - benign but locally aggressive
- Active surveillance is first-line: 50% stabilize or regress spontaneously
- CTNNB1 mutation (beta-catenin) drives 85-90% of sporadic desmoids
- Positive surgical margins acceptable - function preservation priority
- Recurrence 20-40% even with complete excision
- “Nuclear beta-catenin staining is diagnostic (90% sensitive)
- “FAP-associated desmoids have APC mutations, not CTNNB1
- “MRI low-signal T2 bands (collagen) are pathognomonic
- “Do NOT re-resect positive margins - unlike sarcoma management
Zero metastatic potential - Despite being called "aggressive fibromatosis," desmoids are histologically benign. They infiltrate locally but NEVER metastasize to distant sites. This fundamentally changes management priorities compared to sarcomas.
50% stable or regress without treatment - Modern evidence supports active surveillance as first-line. Avoid overtreatment of tumors that may never progress. Surgery reserved for progressive symptomatic lesions.
Nuclear beta-catenin pathognomonic - CTNNB1 mutations cause nuclear beta-catenin accumulation. Nuclear (not cytoplasmic) staining confirms diagnosis. FAP-associated cases have APC mutations instead.
Function over margins - Positive margins acceptable to preserve nerve, vessel, or critical muscle. Unlike sarcoma, margin status does not affect survival. Recurrence manageable with surveillance or systemic therapy.
DESMOIDDesmoid Key Features
Hook:DESMOID summarizes the tumor: Does not spread, Surveillance first, Margins not critical!
Overview and Epidemiology
Desmoid tumors, also termed aggressive fibromatosis, are rare benign fibroblastic neoplasms characterized by monoclonal proliferation of myofibroblasts with locally infiltrative growth. Despite lacking metastatic potential, these tumors pose significant clinical challenges due to their unpredictable natural history, local aggressiveness, and high recurrence rates following surgical resection.
The paradigm for desmoid management has shifted dramatically over the past decade. Historical aggressive surgical approaches have been replaced by surveillance-first strategies, recognizing that approximately 50% of desmoids remain stable or spontaneously regress without intervention. This evolution reflects growing understanding of desmoid biology and the recognition that treatment-related morbidity may exceed disease-related morbidity in many patients.
Aggressive fibromatosis versus desmoid tumor: These terms are synonymous. "Desmoid" derives from the Greek "desmos" (band or tendon), reflecting the tumor's collagenous, band-like consistency. "Aggressive fibromatosis" emphasizes the locally aggressive behavior despite benign histology. Both terms appear in examination questions.
- Age: Peak 20-40 years, median 30 years
- Gender: Female predominance 2-3:1 overall
- Abdominal wall: Strong female bias (hormonal influence)
- Extremity: More equal gender distribution
- Extra-abdominal: 60% (shoulder, thigh most common)
- Abdominal wall: 25% (rectus, postpartum association)
- Intra-abdominal: 15% (mesentery, FAP-associated)
- Head/neck: 5% of extra-abdominal cases
Molecular Pathophysiology and Genetics
Wnt-Beta-Catenin Pathway
Desmoid tumorigenesis is driven by aberrant activation of the Wnt-beta-catenin signaling pathway through two distinct genetic mechanisms.
Sporadic Desmoid Tumors (85-90%)
CTNNB1 gene mutations (encoding beta-catenin) are the hallmark of sporadic desmoid tumors.
Molecular mechanism:
- Gene location: Chromosome 3p21
- Mutation sites: Exon 3, predominantly codons 41 (T41A) or 45 (S45F)
- Effect: Prevents beta-catenin phosphorylation and degradation
- Result: Nuclear beta-catenin accumulation
Pathway activation:
Normal state:
- Beta-catenin is targeted by destruction complex (APC-Axin-GSK3beta)
- Phosphorylation marks beta-catenin for ubiquitin-mediated degradation
- Cytoplasmic levels remain low
Mutant state:
- CTNNB1 mutation creates non-phosphorylatable beta-catenin
- Destruction complex cannot target mutant protein
- Beta-catenin accumulates and translocates to nucleus
- Nuclear beta-catenin binds TCF/LEF transcription factors
- Activates target genes promoting fibroblast proliferation
Genotype-phenotype correlation:
- T41A mutation: Associated with more aggressive behavior
- S45F mutation: May have better prognosis
- Codon 41 mutations: Higher recurrence risk in some studies
This molecular basis underlies nuclear beta-catenin immunostaining as diagnostic test.
Risk Factors
- Mechanism
- Germline APC mutation
- Relative Risk
- 10-20% lifetime risk
- Clinical Relevance
- Screen FAP patients, genetic counseling
- Mechanism
- Wound healing response trigger
- Relative Risk
- 30% of patients report
- Clinical Relevance
- Avoid unnecessary surgery in FAP
- Mechanism
- Hormonal influence (estrogen)
- Relative Risk
- 40% of abdominal wall cases
- Clinical Relevance
- Counsel postpartum women on surveillance
- Mechanism
- Hormonal factors suspected
- Relative Risk
- 2-3:1 female predominance
- Clinical Relevance
- Consider hormonal therapy (tamoxifen)
Pathology and Histology

Macroscopic Features
Desmoid tumors present as firm, poorly circumscribed masses:
- Consistency: Firm to rubbery, resembling scar tissue or keloid
- Margins: Infiltrative, no true capsule, irregular borders
- Cut surface: Whorled, glistening white-grey appearance (collagenous)
- Size: Variable, typically 5-15cm at diagnosis (can be larger)
- Fascial involvement: Common, tumor follows fascial planes
- Muscle infiltration: Invades between muscle fibers
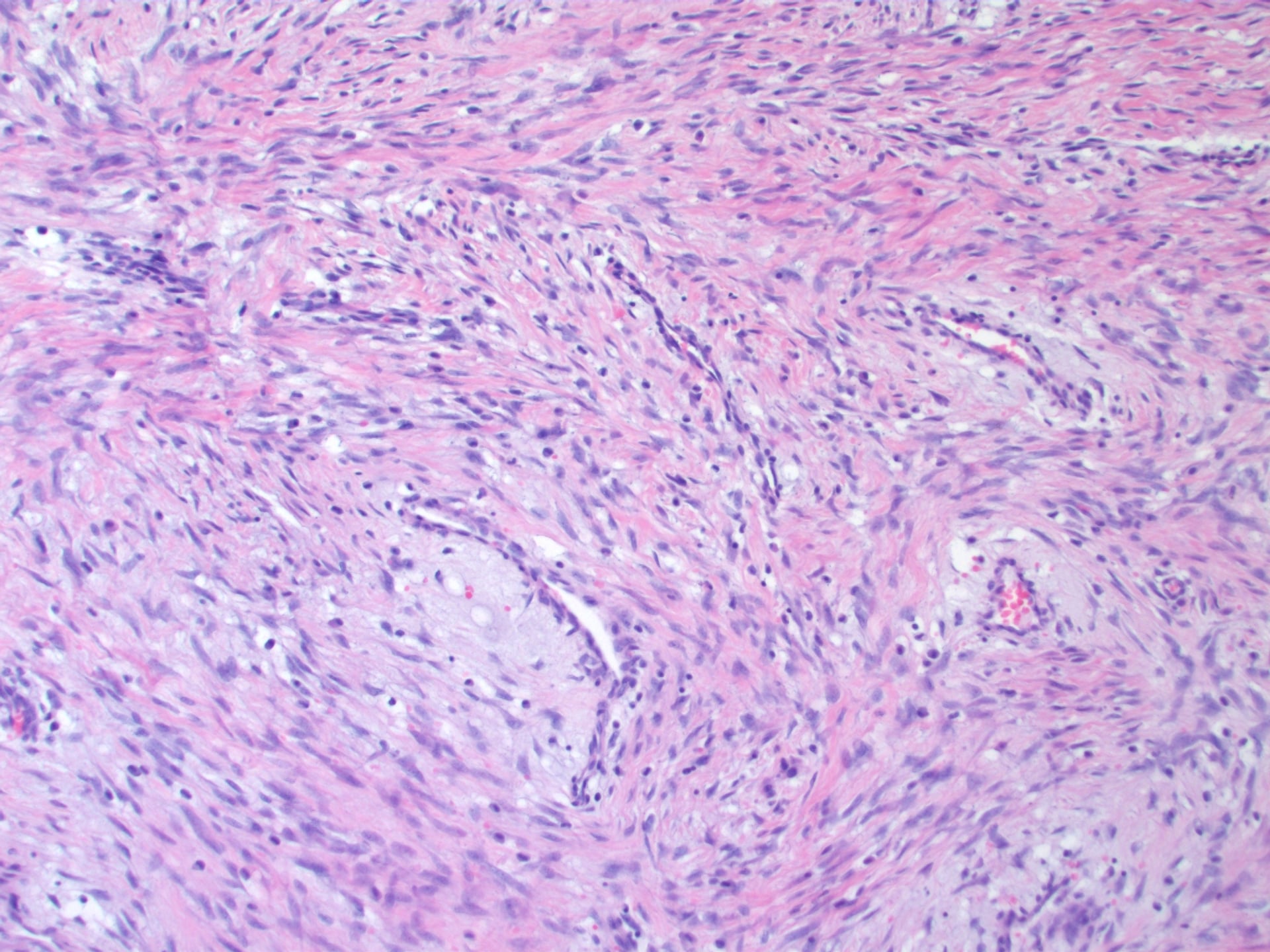
Microscopic Features
- Growth pattern: Infiltrative sweeping fascicles
- Margins: Irregular, invading adjacent tissues
- Architecture: Long bundles of fibroblasts in collagen
- Muscle invasion: Dissects between muscle fibers
- Vascularity: Variable, often hypovascular
- Cellularity: Uniform spindle cells (myofibroblasts)
- Cytology: Bland, minimal nuclear atypia
- Nuclei: Vesicular with small nucleoli
- Mitoses: Rare to absent (benign)
- Necrosis: Absent (key to exclude sarcoma)
- Collagen: Abundant, keloid-like in older lesions
Immunohistochemistry
Diagnostic markers:
- Expression
- Positive 85-95%
- Significance
- PATHOGNOMONIC - must be nuclear not cytoplasmic
- Expression
- Positive (variable)
- Significance
- Confirms myofibroblastic differentiation
- Expression
- Low (under 5%)
- Significance
- Confirms benign nature
- Expression
- Negative
- Significance
- Excludes smooth muscle tumor
- Expression
- Negative
- Significance
- Excludes neural tumor
- Expression
- Negative
- Significance
- Excludes solitary fibrous tumor
Nuclear (not cytoplasmic) beta-catenin staining is diagnostic:
- Cytoplasmic beta-catenin is non-specific (normal finding)
- Nuclear accumulation reflects Wnt pathway activation
- Seen in 85-95% of desmoid tumors
- Negative staining should prompt reconsideration of diagnosis
- Strongly positive nuclear staining is pathognomonic
BLANDHistology Differential Diagnosis
Hook:BLAND histology distinguishes desmoid from aggressive sarcoma!
Prognosis and Natural History
Prognostic Factors
- Favorable
- Extra-abdominal
- Unfavorable
- Intra-abdominal
- Favorable
- Younger (under 30)
- Unfavorable
- Older (over 40)
- Favorable
- Unifocal
- Unfavorable
- Multifocal (FAP)
- Favorable
- Negative
- Unfavorable
- Positive (modestly worse)
- Favorable
- Sporadic
- Unfavorable
- FAP-associated
- Favorable
- S45F (codon 45)
- Unfavorable
- T41A (codon 41)
Long-Term Surveillance
- Recurrence can occur decades after treatment
- Late progression after years of stability possible
- Lifelong monitoring recommended
- Years 0-2: MRI every 3-6 months
- Years 3-5: MRI every 6-12 months
- After 5 years: Annual MRI or clinical exam
Clinical Presentation
Extra-Abdominal Desmoid (60%)
- Painless slowly enlarging mass over months to years
- Discovered incidentally or noted by patient
- Firm, non-mobile mass fixed to underlying structures
- Pain in 30% if nerve compression develops
- Functional limitation if large or involves shoulder/thigh
- Shoulder girdle (deltoid, pectoralis, scapular muscles)
- Thigh (quadriceps, adductors)
- Chest wall, back, gluteal region
- Head and neck (rare, 5-10% of extra-abdominal)
- Prior trauma to area in 30% (sports injury, surgery)
- Slow growth typical (months to years)
- May have periods of rapid growth then stabilization
Abdominal Wall Desmoid (25%)
- Firm mass in anterior abdominal wall, usually rectus muscle
- Often in postpartum women (40% pregnancy-associated)
- History of cesarean section or prior abdominal surgery (30%)
- Usually painless, cosmetic concern predominates
- Carnett sign positive (pain increases with rectus contraction)
- Postpartum period (hormonal changes plus rectus trauma)
- Prior C-section or abdominal surgery
- Multiple pregnancies
- Female gender (strong association)
Intra-Abdominal Desmoid (15%)
- Abdominal pain, bloating, early satiety
- Bowel obstruction symptoms (if mesenteric)
- Palpable mass if large
- FAP history present in 50% of cases
- Small bowel obstruction (20-30%)
- Ureteric obstruction with hydronephrosis (10%)
- Portal vein compression (rare)
- Gastrointestinal bleeding (rare)
- 50% of intra-abdominal desmoids occur in FAP patients
- Often develop after colectomy (surgery triggers tumor)
- May be multifocal
- Leading cause of death in FAP after prophylactic colectomy
ALL patients with intra-abdominal desmoid should be screened for FAP:
- Family history of colorectal cancer or polyposis
- Personal history of colonic polyps
- Examination for extracolonic features: osteomas (skull, mandible), supernumerary teeth, CHRPE (congenital hypertrophy retinal pigment epithelium), epidermoid cysts
- Colonoscopy if suspicious
- Genetic testing for APC germline mutation if clinical suspicion
Physical Examination
- Firm to hard mass, non-tender unless nerve compression
- Poorly defined margins, infiltrative feel
- Fixed to underlying fascia or muscle, not freely mobile
- No overlying skin changes (unlike malignancy)
- No lymphadenopathy (benign tumor)
- Carnett sign: Pain increases with abdominal muscle contraction
- Distinguishes abdominal wall mass from intra-abdominal pathology
- Range of motion for extremity lesions
- Neurological examination if nerve compression suspected
- Vascular examination if proximity to major vessels
Investigations and Imaging
Magnetic Resonance Imaging (Gold Standard)
MRI is the investigation of choice for diagnosis, staging, and surveillance.
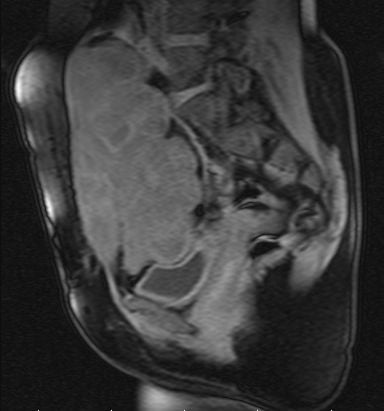
T1-Weighted Features
- Isointense to muscle (similar grey appearance)
- Poorly defined margins with irregular borders
- Infiltrates adjacent muscle (intramuscular extension)
- Fascia sign (tail sign): Tumor extends along fascial planes as linear tail
- Highly suggestive of desmoid tumor
- Reflects predilection for aponeurotic structures
- Relationship to neurovascular structures
- Extent of muscle involvement
- Bone contact (extraperiosteal, no invasion)
T1 sequences best for anatomical detail and surgical planning.
Desmoid tumor MRI triad:
- Fascia sign: Tail extending along fascial planes (T1)
- Low-signal T2 bands: Collagen bundles (T2) - pathognomonic
- Heterogeneous enhancement: Cellular areas enhance, fibrous do not
These three features together are highly specific for desmoid tumor.
Other Imaging Modalities
- Limited role, may identify superficial lesions
- Hypoechoic mass with infiltrative margins
- Cannot adequately assess extent
- May guide core needle biopsy for superficial tumors
- Less useful than MRI for soft tissue characterization
- Role in intra-abdominal desmoids (bowel obstruction assessment)
- Can identify organ involvement
- May guide percutaneous biopsy
- Variable FDG uptake (not reliable for diagnosis)
- May be helpful for intra-abdominal cases
- Limited role in routine workup
Biopsy
- Confirm diagnosis before treatment (essential)
- Exclude malignancy (sarcoma differential)
- Obtain tissue for immunohistochemistry
- Image-guided (ultrasound or CT)
- Multiple cores (3-4) for adequate sampling
- 14-16 gauge needle
- Send for:
- H&E histology
- Nuclear beta-catenin immunostain
- Ki67 proliferation index
- Desmin, S100 (to exclude other diagnoses)
- Core needle biopsy: Greater than 90% diagnostic
- False negatives rare if adequate tissue obtained
- Repeat biopsy if non-diagnostic and suspicion high
- Violates oncologic principles if sarcoma
- Contaminates tissue planes
- Makes subsequent surgery more difficult
- Core needle biopsy is safe and diagnostic
- Cannot assume lipoma/benign based on imaging alone
- Must confirm benign nature before surveillance
- Sarcoma requires different surgical approach
A high-yield desmoid nuance: judging treatment success by tumour SIZE alone (conventional RECIST) underestimates benefit, because a desmoid can become biologically INACTIVE without shrinking.
- The key concept: as a desmoid "matures" to a quiescent fibrotic lesion, the MRI shows falling T2 signal (low-signal collagen replacing cellular high-signal tissue), reduced contrast enhancement, and usually loss of symptoms - even while the measured diameter stays the same. Stable size with falling T2 signal is a GOOD response; conversely, rising T2 signal/enhancement signals reactivation.
- So assess response by a combination of symptom/functional improvement and T2-signal/enhancement change, not size alone. This is why size-based RECIST is a poor endpoint for desmoid trials.
- Be patient: responses to systemic therapy and radiotherapy are slow (often months to a median of 6-12 months) and continue for years - do not declare failure early, and tumours may keep regressing after treatment stops.
Exam point: assess desmoid response by symptoms and T2-signal/enhancement (activity), not by RECIST size - a tumour can be controlled while unchanged in size.
Differential Diagnosis
- Key Distinguishing Features
- Nuclear atypia, mitoses, necrosis present; beta-catenin negative
- Definitive Test
- Biopsy with IHC
- Key Distinguishing Features
- Rapid growth (weeks), self-limited; USP6 rearrangement
- Definitive Test
- Clinical course, biopsy
- Key Distinguishing Features
- Sternocleidomastoid mass in infants, birth trauma
- Definitive Test
- Age, location, spontaneous resolution
- Key Distinguishing Features
- Subscapular mass in elderly, specific location, fat on MRI
- Definitive Test
- MRI shows fat intermixed with fibrosis
- Key Distinguishing Features
- Heterotopic ossification, trauma history, zonal phenomenon
- Definitive Test
- MRI/CT shows peripheral ossification
WATCH FIRSTManagement Algorithm
Hook:WATCH FIRST - the modern desmoid management philosophy!
Management Algorithm

Active Surveillance (First-Line)
Paradigm shift rationale:
The evolution from aggressive surgery to surveillance-first reflects recognition of desmoid natural history:
- 50% of desmoids remain stable or regress without intervention
- Surgery has high morbidity (functional loss, recurrence 20-40%)
- Treatment complications may exceed disease-related morbidity
- Benign nature (no metastasis) allows time for observation
- Progression after period of stability is manageable
Indications for active surveillance:
- Asymptomatic or minimally symptomatic
- No functional impairment
- No acute complications (obstruction, compression)
- Patient preference after informed discussion
- Understanding and acceptance of monitoring
- Any size (size not predictor of behavior)
- Stable on serial imaging
- Location where surgery would cause major morbidity
- Extra-abdominal location (better prognosis)
- First presentation (not recurrent)
Surveillance protocol:
Active Surveillance Schedule
Intensive monitoring:
- Clinical examination at each visit
- MRI every 3-6 months
- Assess size, signal characteristics, enhancement
- Document symptoms (pain, functional limitation)
- Photograph for clinical record
If stable:
- Continue clinical examination every 6 months
- MRI every 6-12 months
- Less frequent if clear stability pattern
- Patient education on warning signs
Long-term follow-up:
- Annual clinical examination
- MRI every 1-2 years or as clinically indicated
- Late growth possible (monitor indefinitely)
- Patient self-monitoring between visits
Surveillance continues indefinitely due to unpredictable late behavior.
Triggers for intervention:
Intervention considered if:
- Progressive growth on serial MRI (greater than 20% volume increase)
- Increasing symptoms (pain, functional impairment)
- Development of complications (nerve compression, vascular compromise)
- Bowel or ureteric obstruction (intra-abdominal)
- Patient anxiety despite stable disease (shared decision-making)
Patient counseling:
Key discussion points:
- Benign tumor, never spreads to other organs
- 50% chance tumor stays same or shrinks without treatment
- Surgery has risks: recurrence 20-40%, functional loss
- Monitoring is safe, active approach
- Can intervene anytime if tumor progresses
- Long-term commitment to surveillance required
Systemic Therapy
Indications
Systemic therapy reserved for:
- Unresectable tumors with documented progression
- Recurrent tumors not amenable to further surgery
- Symptomatic intra-abdominal desmoids
- Multifocal FAP-associated desmoids
- Patient preference to avoid surgery
First-Line Systemic Options
NSAIDs Plus Tamoxifen (First-Line)
- Low toxicity, oral administration
- Combination more effective than monotherapy
- Well-tolerated, suitable for long-term use
- First-line for many centers
- Sulindac (NSAID): COX-2 inhibition, anti-inflammatory
- Tamoxifen: Selective estrogen receptor modulator, anti-estrogenic
- Sulindac: 300mg daily (150mg twice daily)
- Tamoxifen: 20-40mg daily
- Continue for at least 12 months if responding
- Complete response: 5-10%
- Partial response: 20-30%
- Stable disease: 50%
- Progressive disease: 20-30%
- Overall disease control (CR + PR + SD): 70-80%
- Generally well-tolerated
- GI upset (10-20%): Nausea, dyspepsia
- Hot flashes from tamoxifen (30%)
- Thromboembolic risk with tamoxifen (rare)
- Endometrial hyperplasia (monitor with tamoxifen)
- MRI every 3-6 months
- Continue if stable or responding
- Consider discontinuation after 2 years if stable
- Restart if progression after stopping
NSAIDs plus tamoxifen is preferred first-line due to favorable toxicity profile.
Radiotherapy
Role and Indications
Radiotherapy is rarely used in modern desmoid management.
- Unresectable tumor failing systemic therapy
- Recurrent tumor not amenable to surgery or systemic therapy
- Symptomatic progression despite all other modalities
- Older patients (lower concern for late effects)
- Dose: 50-56 Gy in 25-28 fractions
- Conformal planning (IMRT or proton therapy)
- Minimize normal tissue exposure
- Daily fractionation over 5-6 weeks
- Local control: 70-80% at 5 years
- Response rate: 50-60% (shrinkage or stabilization)
- Median time to response: 6-12 months
- Acute: Skin reaction, fatigue
- Subacute: Fibrosis (3-12 months)
- Chronic: Joint stiffness, lymphedema, muscle atrophy
- Secondary malignancy risk: Radiation-induced sarcoma (rare, 0.5-1% at 10+ years)
Avoid radiotherapy in young patients if possible:
- Lifetime risk of secondary malignancy
- Radiation-induced sarcoma can occur decades later
- Functional impairment from fibrosis (joint stiffness, muscle atrophy)
- Reserve for older patients (over 50-60) with no other options
- Always discuss risks versus benefits thoroughly
Image-Guided Cryoablation
An increasingly used minimally-invasive option that this topic should include: image-guided percutaneous ablation - chiefly cryoablation - now sits between active surveillance and surgery for extra-abdominal desmoids.
- Mechanism: CT- or MRI-guided percutaneous probes generate lethal ice-balls that destroy the tumour, and the visible ice-ball allows real-time monitoring of the ablation zone (high-intensity focused ultrasound, HIFU, is an alternative non-invasive thermal option).
- Indications: progressive or symptomatic extra-abdominal desmoid, especially where surgery would be morbid; recurrent disease; an alternative to systemic therapy. It is repeatable and preserves the surgical and systemic options.
- Advantages: function-preserving, day-case, good symptomatic relief and local-control rates in published series.
- Cautions/limitations: large tumours need staged/multiple sessions; thermoprotection (hydro- or CO2-dissection, skin warming) is essential when the tumour abuts skin, bowel or a major nerve to avoid cryo-injury; it is not suited to intra-abdominal/mesenteric disease near bowel; and it requires interventional-radiology expertise.
Exam point: percutaneous cryoablation is a function-preserving, repeatable local treatment for symptomatic/progressive extra-abdominal desmoids, with thermoprotection of adjacent nerve, skin and bowel.
Surgical Management
Indications for Surgery
Surgery is now reserved for selected cases after failure of surveillance:
- Clinical Scenario
- Growth on serial MRI with pain or functional limitation
- Surgical Goal
- Complete macroscopic excision, accept positive margins
- Clinical Scenario
- Bowel obstruction, vascular compromise, severe pain
- Surgical Goal
- Debulking or complete resection, emergency surgery
- Clinical Scenario
- Cannot exclude sarcoma despite biopsy
- Surgical Goal
- Complete excision for definitive diagnosis
- Clinical Scenario
- Informed patient chooses surgery despite stable disease
- Surgical Goal
- Shared decision-making, counsel on recurrence risk
Surgical Principles (Function Over Margins)
Critical paradigm difference from sarcoma:
Unlike sarcoma surgery where wide margins are mandatory:
- Positive margins acceptable to preserve function
- No survival impact of margin status (benign tumor)
- Recurrence manageable with surveillance or systemic therapy
- Function preservation is priority
Intraoperative Margin Decisions
- Attempt preservation if greater than 1mm clearance possible
- If tumor encases nerve: Preserve nerve, accept positive margin
- Do NOT sacrifice major nerve for negative margin
- Functional loss from nerve sacrifice is permanent and devastating
- Dissect tumor off vessel if plane exists
- If tumor adherent: Preserve vessel, accept positive margin
- Vascular reconstruction possible but increases morbidity
- Accept positive margin rather than sacrifice vessel
- Non-critical muscle: Resection acceptable
- Functionally critical muscle: Preserve if possible
- Example: Preserve deltoid (shoulder function), can sacrifice sartorius
- Extraperiosteal resection if abutting bone
- Do not resect bone for margin (benign tumor)
- Rarely changes intraoperative management
- Positive margin often anticipated and accepted
- Document margin status for adjuvant therapy planning
Surgical decision-making prioritizes long-term function over margin status.
Outcomes After Surgery
- Negative Margins
- 20-30%
- Positive Margins
- 30-50%
- Management
- Higher with positive margins but many do not recur
- Negative Margins
- 30-40%
- Positive Margins
- 40-60%
- Management
- Late recurrence possible, lifelong surveillance needed
- Negative Margins
- Median 24 months
- Positive Margins
- Median 18 months
- Management
- Can occur decades later, unpredictable
- Negative Margins
- Variable by site
- Positive Margins
- Better if nerve/vessel preserved
- Management
- Function preservation improves quality of life
- Extra-abdominal: 20-40% recurrence
- Abdominal wall: 20-30% recurrence
- Intra-abdominal: 40-60% recurrence (worst prognosis)
- First-line: Active surveillance (same as primary tumor)
- Surgery if progressive and symptomatic (re-resection)
- Systemic therapy (especially if multiple recurrences)
- Radiotherapy (last resort)
Unlike sarcoma, positive margins do NOT mandate re-resection:
- Recurrence risk increases modestly (30-50% vs 20-30%)
- Many patients with positive margins never recur
- Re-resection adds morbidity without clear benefit
- Recurrence is manageable with surveillance or systemic therapy
- Function preservation more important than margin clearance
Examiners expect you to articulate this principle clearly.
Complications
Disease-Related Complications
- Incidence
- 20-30%
- Location
- Intra-abdominal desmoids
- Management
- Surgery, systemic therapy, nutritional support
- Incidence
- 10%
- Location
- Intra-abdominal/pelvic
- Management
- Stent, nephrostomy, systemic therapy
- Incidence
- 10-15%
- Location
- Extremity desmoids
- Management
- Surgery if progressive, pain management
- Incidence
- 30%
- Location
- Large extremity tumors
- Management
- Analgesia, physiotherapy, systemic therapy
Treatment-Related Complications
- Recurrence: 20-40% (highest complication rate)
- Wound infection: 10-15%
- Nerve injury: 5-10% (higher if tumor adherent)
- Functional impairment: 20-40% (shoulder, thigh)
- Abdominal wall hernia: 10% (if mesh reconstruction)
- NSAIDs/Tamoxifen: Minimal (GI upset, hot flashes)
- Sorafenib: Hand-foot syndrome 50%, diarrhea 30%, fatigue 40%
- Methotrexate/Vinblastine: Myelosuppression, nausea
- Fibrosis and joint stiffness: 40-50%
- Lymphedema: 10-20%
- Secondary malignancy: 0.5-1% (long-term)
Guidelines, Registries & Global Practice
Global Epidemiology
Desmoid-type fibromatosis is a rare tumour. Population-based and registry data give an estimated incidence of roughly 3 to 5 cases per million per year, with a female predominance and a peak in the third and fourth decades. According to PubMed, the prospective Dutch GRAFITI cohort and large referral-centre series confirm that the majority of patients managed with active surveillance never require active treatment, and that genotype (S45F CTNNB1) and tumour size predict the need for intervention (Schut et al., Ann Surg 2022; DOI). The defining molecular feature, CTNNB1 mutation in approximately 85% of sporadic cases, is consistent across international cohorts (Gronchi et al., Ann Oncol 2014; DOI).
Side-by-Side Guideline Guidance
- Front-Line Strategy
- Active surveillance for most newly diagnosed tumours
- Surgery
- Reserved for progression; function over margins
- Systemic Therapy
- Sorafenib, nirogacestat, low-dose chemo, hormonal/NSAID for progression
- Evidence Basis
- Expert consensus + RCTs
- Front-Line Strategy
- Watchful waiting first-line; treat on documented progression
- Surgery
- Selective; avoid mutilating resection
- Systemic Therapy
- Stepwise escalation; refer to sarcoma unit
- Evidence Basis
- Level I-III
- Front-Line Strategy
- Observation acceptable for asymptomatic disease
- Surgery
- Resection if progressive/symptomatic and function preserved
- Systemic Therapy
- Sorafenib or nirogacestat category 1 for progression
- Evidence Basis
- Category 1-2A
- Front-Line Strategy
- Front-line wait-and-see algorithm
- Surgery
- Stepwise, anatomy-driven, referral-centre
- Systemic Therapy
- Treatment only on progression
- Evidence Basis
- Consensus (PMID 24325833)
Registry & Prospective Evidence
- Design
- 105 patients, active surveillance
- Key Finding
- Only 30% needed treatment at 3 years; 28% regressed
- Practice Impact
- Validates surveillance-first internationally
- Design
- 495 resected patients
- Key Finding
- Margin NOT predictive; site/age/size are
- Practice Impact
- Function-preserving surgery; selective systemic therapy
- Design
- 142 patients, nirogacestat vs placebo
- Key Finding
- ORR 41% vs 8%; 2-yr event-free 76% vs 44%
- Practice Impact
- First desmoid-specific approved agent
Practice Variation & Global Access
International practice has converged on a surveillance-first, multidisciplinary model coordinated through specialist sarcoma centres, though access to newer agents varies by jurisdiction. Suspected desmoid tumours should be discussed with a specialist sarcoma multidisciplinary team, with image-guided core needle biopsy arranged locally or at the referral centre. Tamoxifen is widely available and inexpensive, and nuclear beta-catenin immunohistochemistry is available through standard anatomical pathology services. Sorafenib and nirogacestat regulatory and reimbursement status differs between countries, so confirm local availability before counselling patients on systemic options.
- Histological diagnosis before treatment (biopsy mandatory)
- MDT discussion for complex cases
- Informed consent: Natural history (50% stable/regress), recurrence risk, margin philosophy
- Surveillance protocol clearly documented
- Positive margin accepted: Document reason (function preservation)
- Excising mass without biopsy (missed sarcoma)
- Aggressive surgery without trial of surveillance
- Nerve sacrifice for negative margins (unacceptable)
- Inadequate surveillance leading to late recurrence detection
MCQ Practice Points
Q: What is the diagnostic immunohistochemical marker for desmoid tumor? A: Nuclear beta-catenin - Nuclear (not cytoplasmic) accumulation of beta-catenin is seen in 85-95% of desmoid tumors and is pathognomonic. This reflects CTNNB1 mutation preventing beta-catenin degradation, leading to nuclear translocation and Wnt pathway activation. Cytoplasmic beta-catenin is non-specific.
Q: What is the first-line management for asymptomatic extra-abdominal desmoid tumor? A: Active surveillance - Modern evidence supports surveillance-first approach as 50% of desmoids remain stable or regress spontaneously without intervention. Surgery has high morbidity (recurrence 20-40%, functional loss) and should be reserved for progressive symptomatic tumors. MRI every 3-6 months for monitoring.
Q: A desmoid tumor is resected with positive margins. What is the appropriate next step? A: Active surveillance, do NOT re-resect - Unlike sarcoma, positive margins in desmoid do not mandate re-resection. Positive margins increase recurrence from 20-30% to 30-50% but many patients never recur. Function preservation is priority over margin clearance. Recurrence is manageable with surveillance or systemic therapy.
Q: What percentage of FAP patients develop desmoid tumors? A: 10-20% lifetime risk - Desmoid tumors occur in 10-20% of patients with familial adenomatous polyposis. These are typically intra-abdominal (mesenteric), often triggered by prior colectomy, and represent leading cause of mortality in FAP after prophylactic colectomy. APC germline mutation rather than CTNNB1 somatic mutation.
Q: What MRI finding is pathognomonic for desmoid tumor? A: Low-signal T2 bands - Low-signal bands on T2-weighted MRI represent dense collagen bundles and are highly specific for desmoid tumor. Combined with fascia sign (tail along fascia on T1) and infiltrative margins, these features are diagnostic. Heterogeneous enhancement due to mix of cellular and fibrous areas.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 32-year-old woman presents 6 months postpartum with a 6cm mass in the right rectus abdominis. Core biopsy shows bland spindle cells with nuclear beta-catenin positivity, consistent with desmoid tumor. MRI shows infiltration of rectus muscle. She is asymptomatic. How would you manage this patient?”
“During resection of a shoulder girdle desmoid tumor, you find that the tumor densely encases the axillary nerve. You can either preserve the nerve with positive margins or resect the nerve en bloc for negative margins. What do you do and why?”
“A 28-year-old woman with known FAP status post total colectomy 2 years ago presents with abdominal pain and intermittent small bowel obstruction. CT shows a 12cm mesenteric mass consistent with desmoid tumor. What is your management approach?”
Key Definition
- Benign fibroblastic tumor - NEVER metastasizes (0% metastatic potential)
- Locally aggressive with infiltrative growth pattern
- Also called aggressive fibromatosis
- Unpredictable: 50% stable/regress, 20-30% progress
Molecular Genetics (High Yield)
- CTNNB1 mutation 85-90% (sporadic) - exon 3, codons 41/45
- APC mutation 5-10% (FAP-associated) - germline
- Both cause nuclear beta-catenin accumulation via Wnt pathway
- Nuclear beta-catenin IHC diagnostic (90% sensitive, pathognomonic)
Location Distribution
- Extra-abdominal 60% (shoulder, thigh most common)
- Abdominal wall 25% (rectus, postpartum women)
- Intra-abdominal 15% (mesentery, FAP-associated)
- FAP-desmoids: intra-abdominal, multifocal, worse prognosis
MRI Triad (Pathognomonic)
- T1: Fascia sign (tail along fascial planes)
- T2: Low-signal bands (collagen bundles) - diagnostic
- Post-contrast: Heterogeneous enhancement (cellular areas enhance)
Management Algorithm
- First-line: Active surveillance (50% stable/regress)
- MRI every 3-6 months, intervene if progressive/symptomatic
- Surgery: Function over margins, positive margins acceptable
- Systemic: NSAIDs/tamoxifen first-line, sorafenib if fail
- Radiotherapy: Last resort (secondary malignancy risk)
Surgical Philosophy
- Function preservation PRIORITY over negative margins
- Positive margins acceptable (unlike sarcoma management)
- Do NOT sacrifice major nerve/vessel for margins
- Do NOT re-resect positive margins (recurrence manageable)
- Recurrence 20-40% regardless of margin status
Natural History
- 10-20% spontaneous complete regression
- 50% stable disease without treatment
- 20-30% progressive growth requiring treatment
- Recurrence after surgery: 20-40% at 5-10 years
FAP-Associated Features
- 10-20% of FAP patients develop desmoids
- Intra-abdominal location (mesentery), multifocal
- Triggered by abdominal surgery (colectomy)
- Leading cause of death in FAP after prophylactic colectomy
- Systemic therapy first-line (surgery triggers more tumors)
Exam Pearls
- NEVER metastasizes - benign but locally aggressive
- Nuclear (not cytoplasmic) beta-catenin diagnostic
- Surveillance first-line - avoid overtreatment
- Positive margins acceptable - function priority
- Unpredictable behavior - can regress spontaneously
Evidence Base and Key Studies
Front-Line Conservative Approach (Fiore, IGR/INT)
- 142 desmoid patients (Institut Gustave Roussy and Istituto Nazionale Tumori) managed front-line without surgery or radiotherapy
- 83 patients had a deliberate wait-and-see policy, 59 had front-line medical therapy
- 5-year progression-free survival 49.9% (wait-and-see) vs 58.6% (medical therapy), not significantly different (P=0.32)
- Similar results for primary and recurrent disease; no clinical variable independently predicted PFS
- All progressing patients were subsequently salvaged safely
Prognostic Nomogram - Margin Not Predictive (Crago, MSKCC)
- 495 patients resected for primary or recurrent desmoid; 100 of 439 with complete gross resection recurred (23%)
- 5-year local recurrence-free survival 69% overall; abdominal wall tumours best at 91%
- On multivariate analysis recurrence was driven by extremity site, young age and large size - NOT by microscopic margin (R1)
- Adjuvant radiotherapy did not improve local recurrence-free survival
- Nomogram of size, site and age (concordance 0.70) validated in an international multi-institutional dataset
Sorafenib for Progressive Desmoid Tumors (Phase 3, Alliance A091105)
- Double-blind randomised placebo-controlled trial, 87 patients with progressive, symptomatic or recurrent desmoids
- 2-year progression-free survival 81% sorafenib vs 36% placebo (HR 0.13, 95% CI 0.05-0.31, P less than 0.001)
- Objective response rate 33% sorafenib vs 20% placebo before crossover
- Most common grade 1-2 events: rash 73%, fatigue 67%, hypertension 55%, diarrhoea 51%
- Median time to response approximately 9.6 months on sorafenib
Nirogacestat (Gamma-Secretase Inhibitor) - DeFi Phase 3
- International double-blind randomised placebo-controlled trial, 142 adults with progressing desmoid tumours
- 2-year event-free likelihood 76% nirogacestat vs 44% placebo (HR for progression/death 0.29, 95% CI 0.15-0.55, P less than 0.001)
- Objective response rate 41% vs 8% (complete response 7% vs 0%)
- Significant improvements in pain, symptom burden and quality of life
- Common events: diarrhoea 84%, nausea 54%, fatigue 51%; 75% of women of childbearing potential had ovarian dysfunction (usually reversible)
Prospective Active Surveillance - GRAFITI Trial
- Nationwide Dutch multicentre prospective cohort, 105 patients with non-intra-abdominal desmoid on initial active surveillance
- At 3 years cumulative incidence of starting active treatment was only 30%; progression-free survival 58%
- During surveillance 28% regressed, 32% were stable; 40% had initial progression that frequently later stabilised or regressed
- Tumour 5 cm or larger (HR 2.38) and S45F CTNNB1 mutation (HR 6.24) predicted need for active treatment
- Most patients never required active treatment
Italian-French Sarcoma Group Position Paper (Consensus Guidance)
- Joint position paper of the Italian and French Sarcoma Groups proposing a stepwise algorithm for sporadic desmoid-type fibromatosis
- Endorses a front-line wait-and-see approach with treatment reserved for documented progression
- Confirms approximately 85% CTNNB1 prevalence and the central role of Wnt/beta-catenin signalling
- Emphasises individualised, anatomy-driven decisions and mandatory referral-centre counselling
- Recognises the absence of an evidence-based single standard of care