Surface Bone Tumour | Hands and Feet | High Local Recurrence | Benign but Mimics Malignancy
- Nora lesion is a benign surface-based osteocartilaginous proliferation most common in the hands and feet
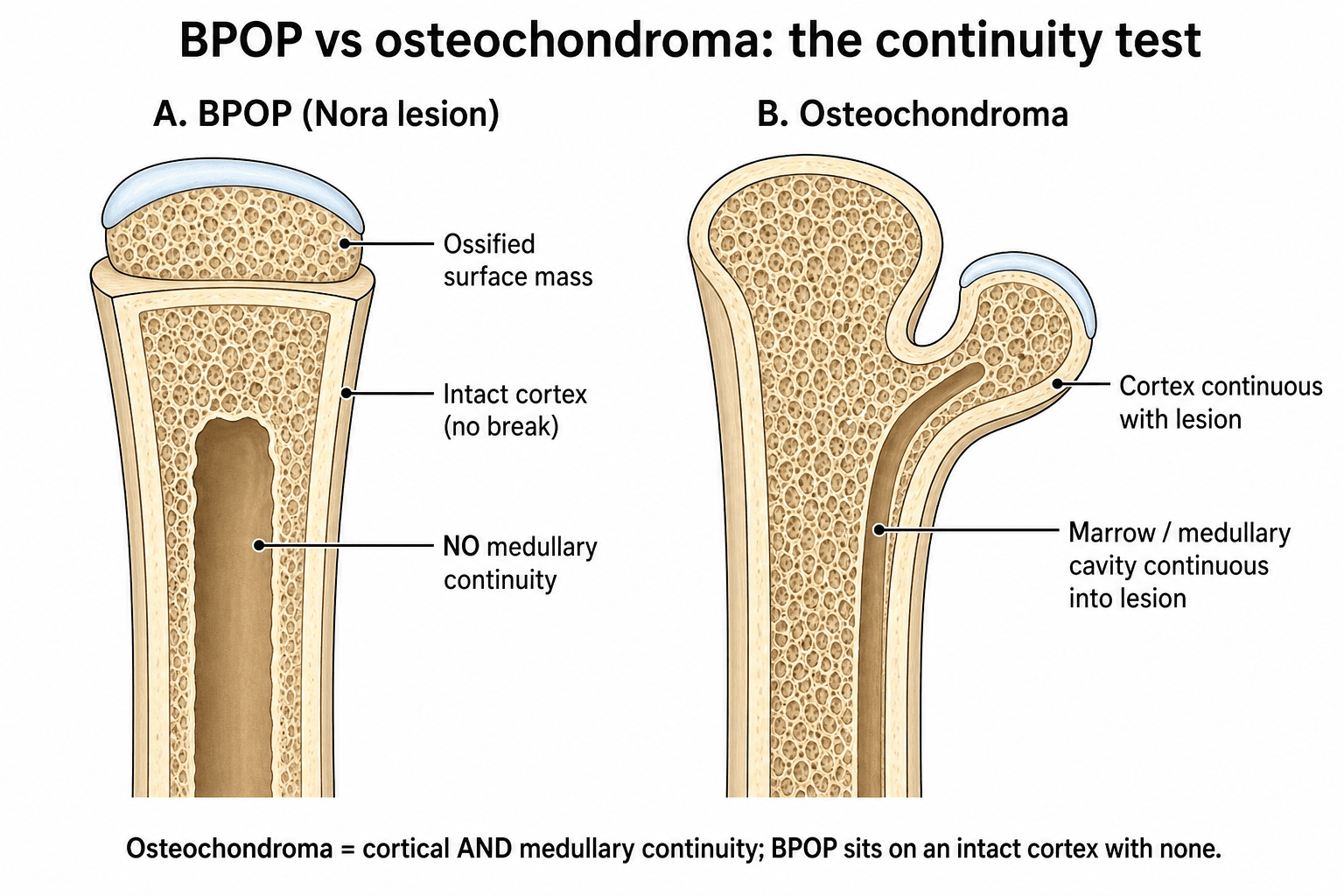
- No medullary continuity with the host bone (unlike osteochondroma) — the single most discriminating feature
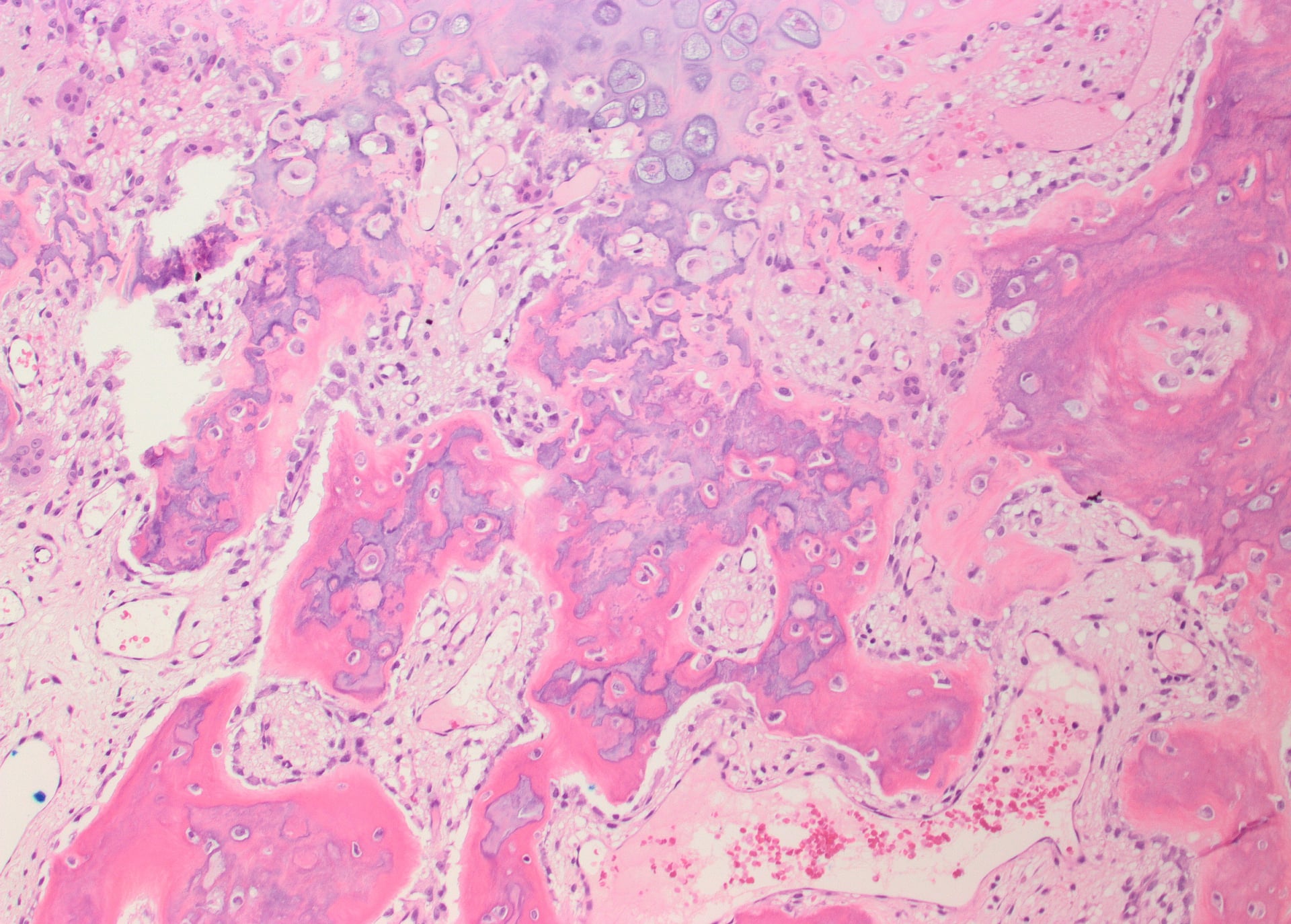
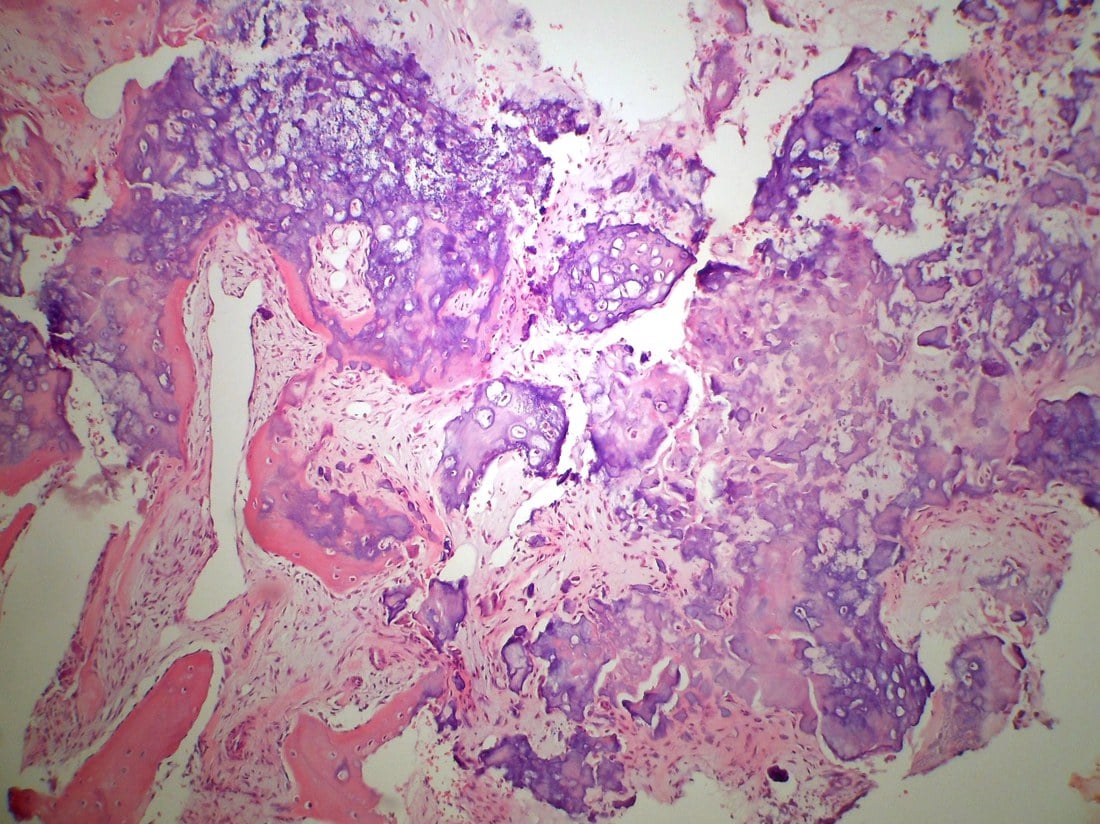
- Cartilage appears bizarre and hypercellular on histology, frequently mistaken for chondrosarcoma — overdiagnosis is a well-known pitfall
- Local recurrence rates of 50-70 percent after marginal excision, but no malignant transformation reported
- Treatment is marginal excision; re-excision for recurrence is curative
- “BPOP = no medullary continuity (unlike osteochondroma)
- “Hands and feet = think Nora lesion before parosteal osteosarcoma
- “Bizarre cartilage does NOT mean malignancy in this context
- “High recurrence is expected; counsel patients preoperatively
Bizarre parosteal osteochondromatous proliferation (BPOP). A benign reactive surface lesion of bone that produces a well-circumscribed mass of bone and cartilage attached to the cortex. First described by Nora et al. in 1983.
Hands and feet predominate. Phalanges (most common), metacarpals, metatarsals, and proximal/middle phalanges. Can occur in long bones but is far less common there.
Histologic mimicry of malignancy. Cartilage is hypercellular with enlarged, bizarre chondrocytes. Pathologists unfamiliar with BPOP may call it chondrosarcoma or parosteal osteosarcoma. Clinical-radiologic correlation is essential.
50-70 percent local recurrence after marginal excision. Recurrence is typically within 2 years. Re-excision is curative. No distant metastasis or malignant transformation has been reported.
- Nora Lesion (BPOP)
- Absent
- Osteochondroma
- Present (diagnostic)
- Parosteal Osteosarcoma
- Absent
- Nora Lesion (BPOP)
- Hands, feet (phalanges, MC/MT)
- Osteochondroma
- Metaphysis of long bones (knee, proximal humerus)
- Parosteal Osteosarcoma
- Distal femur posterior (long bones)
- Nora Lesion (BPOP)
- 2nd-3rd decades (range wide)
- Osteochondroma
- Adolescents (growth plate active)
- Parosteal Osteosarcoma
- 3rd-4th decades
- Nora Lesion (BPOP)
- Bizarre, hypercellular, but benign
- Osteochondroma
- Normal-appearing cartilage cap
- Parosteal Osteosarcoma
- Low-grade osteoid production
CARTDifferentiating BPOP from Osteochondroma
Hook:CART: Continuity, Anatomy, Radiologic border, Tumour behaviour — the four pillars for BPOP vs osteochondroma!
SAFEAvoiding the Malignancy Trap
Hook:SAFE: Site, Age, Florid spectrum, Expert path review — do not overcall malignancy!
Overview and Epidemiology
Nora lesion is rare but has a striking tendency to be misdiagnosed as chondrosarcoma or parosteal osteosarcoma on histology alone. The bizarre, hypercellular cartilage mimics malignancy, yet the lesion is entirely benign. Understanding this entity prevents catastrophic overtreatment — including unnecessary wide resection or amputation — particularly in the hands and feet where functional preservation is paramount.
- Age: 2nd and 3rd decades most common, but ranges from childhood to the elderly
- Sex: No strong sex predilection; slight female predominance in some series
- Incidence: Rare; exact incidence unknown, but account for a minority of surface bone lesions
- Sites: Phalanges of hands and feet (most common), followed by metacarpals and metatarsals; long bones less frequently
- Mass: Painless or mildly tender swelling on the surface of a bone in the hand or foot
- Growth: Slowly enlarging over months to years
- Functional impact: May cause mechanical irritation, deformity of adjacent digit, or limit motion
- History: Often no preceding trauma identified, though trauma has been proposed as a trigger
Pathophysiology
Nora lesion (BPOP) is classified as a reactive or pseudoneoplastic proliferation rather than a true neoplasm. It belongs to the spectrum of florid reactive periostitis and bizarre parosteal osteochondromatous proliferation. The exact aetiology is unknown, but proposed mechanisms include reactive changes from trauma or chronic irritation. The lesion produces mature bone and cartilage that grows on the cortical surface. The cartilage cap shows hypercellularity, enlarged chondrocytes, and bizarre nuclei that mimic chondrosarcoma — but there is no evidence of true malignant transformation. Molecular studies have demonstrated rearrangements of the type I collagen genes (COL1A1 and COL1A2), often as fusions with non-coding RNA genes (LINC-PINT, MIR29B2CHG), supporting a clonal but benign process.
- Features
- Well-formed bone and cartilage mass on cortex
- Location
- Phalanges, hands, feet
- Key Differentiator
- Most organized; mature bone with cartilage cap
- Features
- Fasciitis-like spindle cell proliferation with reactive new bone
- Location
- Phalanges, hands
- Key Differentiator
- Less organized bone; more spindle cell component
- Features
- Mature bone arising from distal phalanx under the nail
- Location
- Distal phalanx (great toe, thumb)
- Key Differentiator
- Specific distal phalangeal location; clinically distinct
The Reactive Surface-Lesion Spectrum and Turret Exostosis
BPOP sits within a family of reactive surface lesions of the small bones, and one classic member - turret exostosis - is worth knowing because it shares the same reactive pathogenesis and acral site.
Turret exostosis is a smooth, dome- or turret-shaped subperiosteal ossification on the dorsum (extensor surface) of a proximal or middle phalanx, arising from a post-traumatic subperiosteal haematoma that ossifies. Unlike BPOP it is a more mature, organised excrescence and often limits extensor tendon gliding and finger extension.
- Typical site
- Phalanges
- Key feature
- Fasciitis-like spindle-cell proliferation with reactive new bone (least organised)
- Behaviour
- Reactive; may recur
- Typical site
- Dorsum of proximal/middle phalanx
- Key feature
- Smooth dome of mature subperiosteal bone after a haematoma; limits extension
- Behaviour
- Reactive; lower recurrence than BPOP
- Typical site
- Phalanges, metacarpals, metatarsals
- Key feature
- Organised mature bone with a bizarre cartilage cap; no medullary continuity
- Behaviour
- Benign but recurs in 50-70%
- Typical site
- Distal phalanx (great toe, thumb)
- Key feature
- Mature bone under the nail
- Behaviour
- Benign; excise once mature
Some authors propose these represent stages of a single reactive process - florid reactive periostitis evolving through turret exostosis to BPOP - which helps explain their shared site, trauma association and overlapping histology. Whatever the precise relationship, the practical message is the same: an acral surface lesion in this spectrum is benign and treated by excision once mature, not as a sarcoma.
Turret exostosis is a smooth dome of mature bone on the dorsum of a phalanx after a subperiosteal haematoma, classically limiting finger extension. Excise once the lesion has matured, since early excision raises recurrence. It shares the reactive, acral, trauma-related background of BPOP.
NORANora Lesion Key Features
Hook:NORA: No medullary continuity, Osteocartilaginous, Recurs a lot, Acral sites!
Classification and Types
Radiographic Classification
- Typical Appearance
- Cortical surface of phalanges, metacarpals, or metatarsals
- Significance
- Acral predilection is the strongest clinical clue
- Typical Appearance
- Well-circumscribed mass of mature bone on the cortex
- Significance
- Well-defined borders suggest benignity
- Typical Appearance
- Absent — no connection between lesion and medullary canal
- Significance
- Key distinguishing feature from osteochondroma
- Typical Appearance
- May be visible as a radiolucent zone at the periphery
- Significance
- Cartilage is typically more prominent than expected for the size
- Typical Appearance
- Intact, may show slight cortical thinning or scalloping
- Significance
- Cortical destruction would raise concern for malignancy
The radiographic hallmark of Nora lesion is a well-circumscribed, surface-based osteocartilaginous mass on a short tubular bone (hand or foot) with no medullary continuity.
Parosteal Osteosarcoma: The Dangerous Mimic
Parosteal osteosarcoma is the malignant surface lesion that BPOP must never be confused with, and the differences are exam-critical. It is the commonest surface (juxtacortical) osteosarcoma, a low-grade tumour of slightly older patients (third to fourth decade), arising classically on the posterior metaphysis of the distal femur and other long bones - not the hands and feet.
- Parosteal osteosarcoma
- Long bones (posterior distal femur)
- Nora lesion (BPOP)
- Hands and feet (phalanges, MC/MT)
- Parosteal osteosarcoma
- Heavily ossified lobulated mass 'stuck on' the cortex with a radiolucent string/cleft sign
- Nora lesion (BPOP)
- Well-circumscribed acral surface mass, no medullary continuity
- Parosteal osteosarcoma
- Low-grade well-formed parallel bony trabeculae in a bland fibrous (spindle) stroma
- Nora lesion (BPOP)
- Mature bone with a bizarre hypercellular cartilage cap
- Parosteal osteosarcoma
- Low-grade malignant; can dedifferentiate to high-grade if neglected
- Nora lesion (BPOP)
- Benign; recurs but never metastasises
- Parosteal osteosarcoma
- Wide (limb-sparing) resection plus oncology MDT
- Nora lesion (BPOP)
- Marginal excision
Parosteal osteosarcoma is a low-grade surface osteosarcoma of the posterior distal femur with a radiolucent string (cleft) sign between tumour and cortex and bland low-grade osteoid in a fibrous stroma. It needs wide resection, not the marginal excision used for BPOP - so a surface lesion on a long bone, rather than a hand or foot, should raise it immediately.
Clinical Assessment
- Duration: Slowly growing mass over months to years
- Pain: Usually painless or mildly tender
- Trauma: May or may not recall preceding injury
- Function: May notice progressive deformity or limited range of motion of the digit
- Inspection: Firm, non-mobile mass on the surface of a phalanx, metacarpal, or metatarsal
- Palpation: Bony hard, fixed to the underlying bone, non-tender or mildly tender
- Overlying skin: Typically normal; no erythema or warmth
- Neurovascular: Intact distally; check for nerve compression if large lesion
The diagnosis of Nora lesion requires correlation of all three domains. Biopsy interpretation without knowledge of the radiologic appearance and clinical setting (young patient, hand/foot location, surface-based lesion) is the primary cause of misdiagnosis as sarcoma. Always ensure the pathologist has access to the imaging and clinical details before a final diagnosis is rendered.
Investigations
Imaging Protocol
Views: PA, lateral, and oblique of the affected digit/foot
Look for: Well-circumscribed surface bone mass, intact cortex, absence of medullary continuity, no soft tissue mass or aggressive features
Key sign: A surface-based osteocartilaginous mass on a short tubular bone without medullary connection is highly suggestive of BPOP
Indication: Confirm the absence of medullary continuity and better define the lesion-cortex interface
Findings: Mature bone mass on the cortical surface; no connection to the medullary canal; intact underlying cortex
Pre-op planning: Define the extent of the lesion for surgical excision planning
Indication: If there is concern for soft tissue extension, nerve/vessel involvement, or to differentiate from sarcoma
Findings: Well-defined surface lesion with cartilage cap signal characteristics; no marrow oedema or soft tissue mass
Important: MRI helps exclude the aggressive features expected in parosteal osteosarcoma
The single most important imaging feature to assess is medullary continuity. If the medullary canal of the host bone is continuous with the lesion, it is an osteochondroma, not a Nora lesion. CT is the best modality for confirming this. If medullary continuity is absent and the lesion is on a hand or foot bone, BPOP is the leading diagnosis.
Management Algorithm
Marginal Excision (Primary Treatment)
Goal: Complete excision of the surface mass with a narrow margin of normal tissue while preserving adjacent neurovascular structures and joint function
Surgical Protocol
Imaging review: CT to confirm surface location and plan approach
Biopsy: Consider pre-operative core needle biopsy only if diagnosis is uncertain; if radiologic appearance is classic for BPOP in a characteristic location, excision may proceed without prior biopsy
Consent: Counsel regarding 50-70 percent recurrence risk and possible need for re-excision
Approach: Direct approach over the mass, protecting neurovascular structures
Excision: Marginal excision — remove the mass with a thin cuff of surrounding tissue
Cortex: Smooth the underlying cortex; remove all visible lesion
Closure: Standard soft tissue closure; may need local tissue rearrangement if defect is large
Immobilization: Brief splinting for soft tissue healing (1-2 weeks for digits)
Mobilization: Early range of motion exercises once wound healed
Path review: Ensure musculoskeletal pathologist reviews specimen with clinical-radiologic correlation
Surveillance: Clinical and radiographic review at 3 months, 6 months, 12 months, then annually
Recurrence: Most recurrences occur within 2 years
Re-excision: If recurrence is detected, repeat marginal excision is the treatment
The key principle is marginal excision with careful follow-up. Wide resection or amputation is never indicated for Nora lesion. The high recurrence rate is expected and managed by re-excision. Over-treating due to misdiagnosis as sarcoma is the greatest iatrogenic harm.
Complications
- Incidence
- 50-70 percent
- Risk Factors
- Incomplete excision, location at joint-adjacent site
- Management
- Repeat marginal excision; curettage of the cortical base
- Incidence
- Reported in multiple case series
- Risk Factors
- Pathologist unfamiliar with BPOP, inadequate clinical info
- Management
- Always request expert musculoskeletal pathology review
- Incidence
- Variable, dependent on approach
- Risk Factors
- Multiple excisions, dorsal approach to digit
- Management
- Hand therapy, early mobilization, splinting
- Incidence
- Rare
- Risk Factors
- Large lesion, revision surgery, poor anatomy
- Management
- Careful dissection; loupe magnification for digital surgery
- Incidence
- Rare
- Risk Factors
- Large lesion weakening the cortex
- Management
- Protect digit during healing; internal fixation rarely needed
The most devastating "complication" of Nora lesion is iatrogenic: unnecessary wide resection or amputation performed because the lesion was misdiagnosed as chondrosarcoma or parosteal osteosarcoma. Multiple case reports in the literature document this scenario. Always ensure clinical-radiologic-pathologic correlation before committing to an aggressive surgical plan for any surface bone lesion in the hands or feet.
Outcomes and Prognosis
- Treatment
- Marginal excision
- Expected Outcome
- Cured; normal function restored
- Long-term Function
- Full digital/hand function preserved
- Treatment
- Re-excision
- Expected Outcome
- Cured in most cases after second procedure
- Long-term Function
- Good function; minor stiffness possible
- Treatment
- Repeat marginal or en bloc excision
- Expected Outcome
- Eventually cured; no malignant transformation
- Long-term Function
- May have cumulative stiffness from repeated surgery
- Treatment
- Wide resection or amputation
- Expected Outcome
- Unnecessary functional loss
- Long-term Function
- Preventable with expert pathology review
Nora lesion is universally benign. No case of malignant transformation has ever been reported. The main morbidity is local recurrence (50-70 percent), which is managed with re-excision. The main risk is misdiagnosis leading to overtreatment. Prognosis for function is excellent when managed correctly.
Guidelines, Registries & Global Practice
- Rare worldwide: No population-based incidence data; reported across all continents
- No ethnic predilection: Cases reported in diverse populations
- Age distribution: Most common in 2nd and 3rd decades but ranges from adolescents to the elderly
- Acral predilection: The hand and foot predominance is consistent across all reported series globally
- High-resource: CT or MRI for characterization, musculoskeletal pathology review, hand/foot surgeon excision
- Limited-resource: Plain radiographs often sufficient for diagnosis; excision by any trained orthopaedic surgeon
- Universal principle: The diagnosis is primarily clinical-radiologic; pathology review confirms but should not be interpreted in isolation
- Key message: In any resource setting, avoid misdiagnosis as sarcoma by correlating clinical, radiographic, and histologic findings
- Diagnostic Emphasis
- Intermediate/benign surface lesion; bizarre cartilage is characteristic
- Treatment
- Marginal excision; re-excision for recurrence
- Key Message
- BPOP is a recognized entity; do not confuse with osteochondroma or parosteal osteosarcoma
- Diagnostic Emphasis
- Clinical-radiologic-pathologic correlation essential; biopsy if uncertain
- Treatment
- Marginal excision by tumour-trained surgeon
- Key Message
- Surface lesions of hands/feet warrant specialist path review
- Diagnostic Emphasis
- CT to confirm no medullary continuity; MRI if sarcoma concern
- Treatment
- Marginal excision; MDT discussion if diagnosis uncertain
- Key Message
- Do not overtreat; BPOP recurs but never metastasizes
- Diagnostic Emphasis
- Histology mimics chondrosarcoma; clinical context essential
- Treatment
- Excision with narrow margins; never wide resection
- Key Message
- Misdiagnosis is the greatest risk — educate pathologists
The evidence for BPOP is derived entirely from case series, case reports, and review articles. There are no randomized trials and no prospectively validated diagnostic criteria. The diagnosis rests on the combination of characteristic acral location, absence of medullary continuity on imaging, and typical (though alarming-appearing) histology with benign clinical behaviour.
Every orthopaedic surgeon and pathologist should know Nora lesion because:
- It is the most commonly overdiagnosed as sarcoma among surface bone lesions
- Unnecessary amputations and wide resections have been reported due to this misdiagnosis
- The single most discriminating feature is no medullary continuity on CT
- A surface bone mass on a hand or foot in a young patient with no medullary continuity should prompt consideration of BPOP before sarcoma
Controversies & Areas of Uncertainty
BPOP has historically been considered a reactive process, but molecular studies showing clonal gene rearrangements (COL1A1, COL1A2) suggest it may be a benign neoplasm. The distinction has no practical impact on management but is of academic interest.
Some authors recommend biopsy before excision if there is diagnostic uncertainty; others argue that classic radiologic features are sufficient to proceed directly to excision. No consensus exists, and practice varies by institution and surgeon experience.
Marginal excision is universally recommended, but the extent of cortical curettage or smoothing at the base is variable. Some surgeons advocate more aggressive local treatment of the cortical bed to reduce recurrence, but evidence is anecdotal.
Most recurrences occur within 2 years, but late recurrences have been reported. There is no consensus on the optimal duration of follow-up. Most authors recommend clinical and radiographic review for at least 2-3 years post-operatively.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 24-year-old woman presents with a slowly enlarging, painless firm mass on the radial aspect of the proximal phalanx of her right middle finger. It has been present for 18 months. Plain radiographs show a well-circumscribed bony mass arising from the cortical surface of the proximal phalanx. There is no connection between the lesion and the medullary canal. The underlying cortex is intact. What is your diagnosis and management?”
“A 30-year-old man underwent excision of a surface bone lesion from his third metatarsal 14 months ago. The original pathology report described 'bizarre parosteal osteochondromatous proliferation consistent with Nora lesion.' He now presents with a recurrent mass at the same site. Radiographs show a similar-appearing surface bone mass. The patient is anxious that the lesion may be malignant. How do you manage this?”
Definition & Key Features
- Benign surface osteocartilaginous proliferation of hands and feet
- No medullary continuity with host bone (vs osteochondroma)
- Bizarre hypercellular cartilage on histology mimics chondrosarcoma
- First described by Nora et al. in 1983
Diagnosis
- Clinical: young patient, painless surface mass on a digit/hand/foot bone
- Radiologic: well-circumscribed surface mass, no medullary continuity on CT
- Pathologic: mature bone with bizarre cartilage cap, no mitoses or permeation
- Mandatory clinical-radiologic-pathologic correlation
Differential Diagnosis
- Osteochondroma: has medullary continuity (the key difference)
- Parosteal osteosarcoma: long bones, tail/wrapping sign, low-grade osteoid
- Periosteal chondroma: purely cartilaginous, no bone in the mass
- Florid reactive periostitis: more spindle cell, less organized bone
Treatment & Recurrence
- Marginal excision is the definitive treatment — never wide resection
- 50-70 percent local recurrence rate, typically within 2 years
- Re-excision for recurrence is curative in most cases
- No malignant transformation has ever been reported
Critical Exam Pitfalls
- Do not misdiagnose as chondrosarcoma based on histology alone
- Do not perform wide resection or amputation for BPOP
- Always check for medullary continuity — present = osteochondroma, absent = BPOP
- Hands and feet + surface mass + young patient = think BPOP first
Evidence Base and Key Trials
Bizarre parosteal osteochondromatous proliferations of the hands and feet
- Original description of 35 cases (ages 14-74) of a distinct clinicopathologic entity
- Surface-based osteocartilaginous lesions confined to proximal phalanges, metacarpals and metatarsals, with bizarre, binucleate chondrocytes mimicking chondrosarcoma
- Local recurrence in roughly half the series (18 of 35), with at least 8 lesions recurring more than once
- Behaviour as a malignant tumour is very rare or non-existent despite the concerning histologic appearance
Bizarre parosteal osteochondromatous proliferation of bone (Nora's lesion)
- Largest early series — 65 cases (ages 8-73, mean 33.9): 36 hand, 10 foot and 17 long-bone, establishing that BPOP also affects long bones
- Distinctive blue (basophilic) tinctorial quality of the lesional bone is a helpful diagnostic clue
- Recurrence in approximately 55 percent (of the 40 with follow-up); no metastasis in any case
- Hypercellular cartilage with bizarre chondrocytes can be mistaken for parosteal osteosarcoma — regarded as a form of heterotopic ossification
Identification of COL1A1/2 Mutations and Fusions With Noncoding RNA Genes in Bizarre Parosteal Osteochondromatous Proliferation (Nora Lesion)
- COL1A1 and COL1A2 mutations identified in BPOP, along with fusions involving noncoding RNA genes
- Molecular findings support a clonal neoplastic process rather than a purely reactive proliferation
- These genetic alterations are distinct from those found in osteochondroma (EXT1/EXT2) and parosteal osteosarcoma
- Molecular testing may serve as an adjunct diagnostic tool in challenging cases
Bizarre parosteal osteochondromatous proliferation (Nora's lesion) in the hand
- Single-institution hand series — 10 cases of BPOP over 21 years versus only 1 hand osteochondroma, underscoring its relative frequency at this site
- Radiographs showed a well-marginated, uniformly dense surface mass without disruption of the host bony architecture
- Only 1 recurrence in their series — far below the literature's high rates — attributed to excising the pseudocapsule and underlying periosteum and decorticating any abnormal host cortex
- Correct diagnosis requires integration of clinical, radiographic, and histologic findings