Infantile Cortical Hyperostosis | Self-Limiting | Classic Triad: Swelling, Bone Lesions, Irritability | Mandible Most Commonly Affected
- Self-limiting condition affecting infants under 6 months - resolves spontaneously by age 2 years
- Classic triad: soft tissue swelling, cortical bone lesions (hyperostosis), and irritability
- Mandible most commonly affected (70-90%), followed by clavicle and ulna - tibia rare
- Prostaglandin theory explains pathogenesis - elevated PGE2 levels found in affected infants
- Familial form associated with a recurrent COL1A1 mutation c.3040C-to-T (R836C / p.Arg1014Cys) on chromosome 17q21
- “Critical differential from non-accidental injury (NAI) - Caffey spares metaphyses, NAI involves metaphyses
- “Periosteal reaction is DIAPHYSEAL in Caffey disease, not metaphyseal as in NAI
- “No fractures in Caffey disease - fractures suggest alternative diagnosis
- “NSAIDs (indomethacin) are first-line treatment - supports prostaglandin theory
- “Mandible involvement is pathognomonic - rare in other paediatric bone conditions
Non-accidental injury (NAI) is the critical differential. Key differences: Caffey disease has DIAPHYSEAL periosteal reaction with NO fractures; NAI has METAPHYSEAL corner fractures and healing fractures of different ages. Mandible involvement favors Caffey disease.
Classic triad: (1) Soft tissue swelling over affected bone, (2) Cortical hyperostosis on X-ray, and (3) Irritability/pseudoparalysis. The triad is highly suggestive in an infant under 6 months with no history of trauma.
Mandible is affected in 70-90% of cases - this is nearly pathognomonic. Other common sites: clavicle (30-50%), ulna (30-40%), ribs, scapula. Tibia and femur are RARE. Spine and hands/feet are NOT affected.
Excellent prognosis - complete resolution by 2 years of age with no long-term sequelae. No treatment is curative; supportive care with NSAIDs for comfort. Recurrence is rare but can occur in familial forms.
- Caffey Disease
- Under 6 months
- NAI
- Any age
- Osteomyelitis
- Any age
- Scurvy
- 6-24 months
- Caffey Disease
- Low-grade or absent
- NAI
- Variable
- Osteomyelitis
- High fever
- Scurvy
- Absent
- Caffey Disease
- Mandible, clavicle, ulna
- NAI
- Metaphyses, ribs
- Osteomyelitis
- Metaphysis/diaphysis
- Scurvy
- Long bones, ribs
- Caffey Disease
- Diaphyseal periosteal reaction
- NAI
- Metaphyseal fractures
- Osteomyelitis
- Lytic lesion, sequestrum
- Scurvy
- Subperiosteal hemorrhage
- Caffey Disease
- None
- NAI
- Multiple, different ages
- Osteomyelitis
- Pathologic possible
- Scurvy
- Pathologic possible
- Caffey Disease
- Mildly elevated
- NAI
- Variable
- Osteomyelitis
- Markedly elevated
- Scurvy
- Normal
- Caffey Disease
- NSAIDs, observation
- NAI
- Safeguarding, MDT
- Osteomyelitis
- IV antibiotics, surgery
- Scurvy
- Vitamin C
- Caffey Disease
- Complete resolution
- NAI
- Variable
- Osteomyelitis
- Good with treatment
- Scurvy
- Excellent with treatment
Overview and Epidemiology
First Description. Caffey and Silverman first described this condition in 1945 as "infantile cortical hyperostosis." The familial autosomal dominant form was recognized later, and the COL1A1 gene mutation was identified in 2005. Understanding the history helps frame examination discussions.
- Peak age: Birth to 5 months (95% present before 6 months)
- Gender: Slight male predominance (1.5:1)
- Incidence: Rare, approximately 3 per 1000 live births
- Ethnicity: No racial predilection
- Familial: 10-20% have positive family history
- Self-limiting: Complete resolution by 2 years of age
- Duration: Acute phase 2-3 months, residual changes resolve over 6-12 months
- Recurrence: Rare in sporadic form, more common in familial
- Prognosis: Excellent - no long-term orthopaedic sequelae
Pathophysiology and Mechanisms
Prostaglandin-Mediated Pathogenesis
Elevated prostaglandin E2 (PGE2) levels have been found in affected infants and may explain the bone changes.
- Elevated serum PGE2 levels in affected infants
- NSAIDs (indomethacin) are effective in symptom control
- PGE2 is known to stimulate osteoclast activity and periosteal bone formation
- Resolution of symptoms correlates with normalization of PGE2 levels
Elevated PGE2 leads to periosteal inflammation, which causes subperiosteal new bone formation, creating cortical thickening, and the clinical presentation of swelling and irritability follows.
This theory remains the most widely accepted explanation for sporadic Caffey disease.
Clinical Presentation
- Age: Under 6 months (typically 2-4 months)
- Onset: Acute onset of swelling and irritability
- Pain: Inconsolable crying, worse with handling
- Feeding: May refuse to feed if mandible involved
- Fever: Low-grade fever in 50% of cases
- Family history: Ask about affected siblings/parents
- Swelling: Firm, tender swelling over affected bone
- Mandible: Facial asymmetry, difficulty feeding
- Limbs: Pseudoparalysis of affected limb
- Skin: Overlying skin may be warm, not erythematous
- General: Irritable but systemically well
- No bruising: Important to note for NAI exclusion
Pseudoparalysis refers to apparent inability to move a limb due to pain, not true paralysis. The infant will not spontaneously move the affected limb but has intact neurological function. This is seen in Caffey disease, osteomyelitis, septic arthritis, and fractures. Always examine for underlying bone pathology.
Clinical Course of Caffey Disease
Acute onset of swelling, irritability, and low-grade fever. Parents often notice the infant is inconsolable.
Progressive bone changes visible on X-ray. Multiple bones may become involved sequentially. NSAIDs provide symptomatic relief.
Symptoms gradually improve. Swelling reduces. Irritability resolves. Radiographic changes begin to normalize.
Complete clinical and radiographic resolution. No long-term orthopaedic sequelae expected.
Imaging and Investigations
Plain Radiograph Findings
- Soft tissue swelling overlying bone
- Periosteal elevation may be subtle
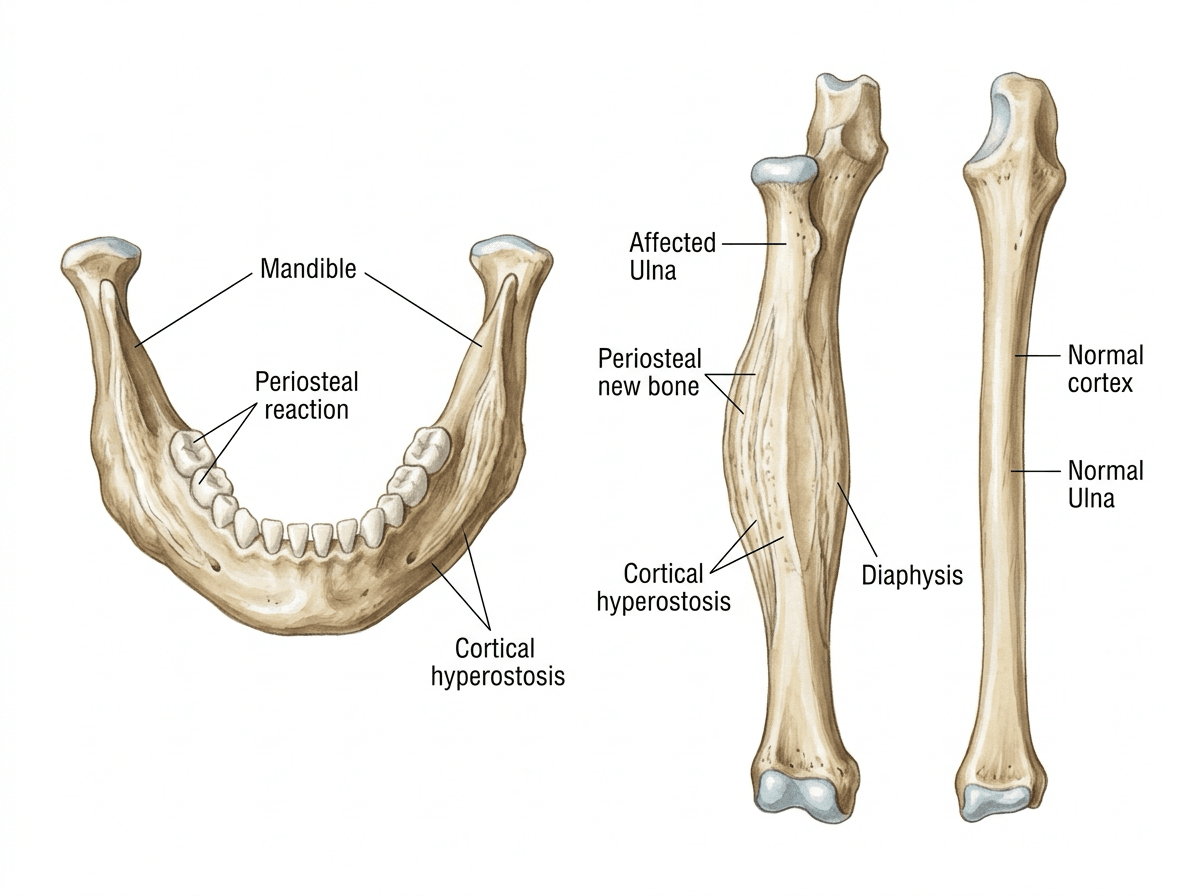
- Laminated or solid periosteal reaction along diaphysis
- Cortical thickening (hyperostosis)
- New bone formation is smooth and uniform
- May see "double cortex" appearance
- Gradual remodeling of thickened cortex
- Return to normal bone contour
- DIAPHYSEAL involvement (not metaphyseal)
- No fractures visible
- Smooth periosteal reaction (not aggressive)
- Mandible involvement nearly pathognomonic
Always obtain X-rays of clinically affected areas plus skeletal survey if NAI is in the differential.
Differential Diagnosis
Non-Accidental Injury
This is the CRITICAL differential - missing NAI is a patient safety failure.
- Caffey Disease
- Under 6 months
- NAI
- Any age, peak 2-4 years
- Caffey Disease
- Diaphyseal periosteal reaction
- NAI
- Metaphyseal corner fractures
- Caffey Disease
- ABSENT
- NAI
- Multiple, different healing stages
- Caffey Disease
- Commonly involved (70-90%)
- NAI
- Rarely involved
- Caffey Disease
- Consistent with findings
- NAI
- Inconsistent or changing story
- Caffey Disease
- None
- NAI
- Bruises, burns, retinal hemorrhages
- Caffey Disease
- Normal family dynamics
- NAI
- Risk factors present
Red Flags for NAI:
- Delay in seeking care
- History inconsistent with injury pattern
- Multiple injuries at different stages
- Retinal hemorrhages
- Subdural hematoma
When in doubt, involve child protection services and perform a full skeletal survey.
Management
Supportive Care
- NSAIDs: Indomethacin or ibuprofen for pain relief and anti-inflammatory effect
- Paracetamol: For additional analgesia and fever control
- Gentle handling: Minimize manipulation of affected limbs
- 0.5-1 mg/kg/day divided into 2-3 doses
- Continue for 2-4 weeks then wean
- Monitor for GI side effects
The prostaglandin theory suggests elevated PGE2 drives the disease process. NSAIDs inhibit prostaglandin synthesis and provide both symptomatic relief and may shorten disease duration.
No role for antibiotics unless osteomyelitis cannot be excluded.
No role for corticosteroids - not proven beneficial and potential side effects.
Complications
Complications of Caffey Disease
Caffey disease is remarkably benign with few true complications:
- Feeding difficulties: If mandible severely affected
- Respiratory distress: Rare, if rib involvement is extensive
- Pseudoparalysis: Apparent limb weakness due to pain
- Bony asymmetry: Temporary cosmetic deformity during resolution phase
- Limb length discrepancy: Extremely rare, transient overgrowth reported
- Polyhydramnios
- Hydrops fetalis
- Stillbirth or early neonatal death (rare)
The key message is that postnatal sporadic Caffey disease has no significant long-term orthopaedic complications and complete resolution is expected.
- Frequency
- Common if mandible affected
- Management
- Supportive feeding, soft nipple
- Frequency
- Common
- Management
- Resolves with disease
- Frequency
- Temporary
- Management
- Reassurance - resolves
- Frequency
- Rare
- Management
- Supportive care
- Frequency
- Rare
- Management
- Give with feeds, monitor
- Frequency
- Very rare (prenatal form only)
- Management
- Intensive prenatal management
Caffey on the Type I Collagenopathy Spectrum
The genetics tab and the Gensure study (below) note that COL1A1-Caffey carriers have connective-tissue features and that the mutation type differs from osteogenesis imperfecta, but the body never develops this.
- An arginine-to-cysteine substitution. The familial Caffey mutation replaces an arginine with a cysteine in the triple-helical domain (R836C / p.Arg1014Cys), introducing an unpaired cysteine and abnormal disulphide bonding - different from the glycine substitutions that typically cause osteogenesis imperfecta.
- A connective-tissue (EDS-like) phenotype. Affected individuals and obligate carriers can show joint hyperlaxity, hyperextensible skin and inguinal hernias - placing Caffey disease on the type I collagenopathy spectrum alongside osteogenesis imperfecta and the COL1A1/COL1A2 forms of Ehlers-Danlos syndrome (both covered in their own topics).
- Why it matters. The same gene produces very different diseases depending on the mutation, so a COL1A1-Caffey family may have relatives with mild connective-tissue laxity rather than classic Caffey - relevant to recognition and counselling.
Q: How does the COL1A1 Caffey mutation differ from osteogenesis imperfecta, and what else do carriers show?
A: Caffey's familial mutation is an arginine-to-cysteine substitution (R836C / p.Arg1014Cys) introducing an unpaired cysteine and abnormal disulphide bonding - unlike the glycine substitutions that typically cause OI. Affected individuals/carriers can have a connective-tissue (EDS-like) phenotype: joint hyperlaxity, hyperextensible skin and hernias - placing Caffey on the type I collagenopathy spectrum with OI and the COL1A1/COL1A2 forms of Ehlers-Danlos. Same gene, different mutation, very different disease.
SBIClassic Triad of Caffey Disease
Hook:SBI - Swelling, Bone changes, Irritability - think of the fussy baby with a swollen jaw!
MUCRSCommon Bones Affected in Caffey
Hook:MUCRS - Mandible leads, Ulna and Clavicle follow, Ribs and Scapula round out the list!
CAFFEY vs NAIDifferentiate Caffey from NAI
Hook:CAFFEY has no Fractures, affects Diaphysis, involves Mandible - NAI has Metaphyseal fractures!
The Prenatal (Lethal) Form: a Different Disease
The topic mentions a 'prenatal (severe) form' in the classification, complications and the Kamoun-Goldrat study, but never develops it as the distinct entity it is.
- Presents in utero. The rare prenatal (antenatal) form is detected on antenatal ultrasound, showing short, bowed long bones, cortical hyperostosis, polyhydramnios and sometimes hydrops fetalis.
- A different prognosis. Unlike the benign postnatal disease, the prenatal form is often severe and can be lethal (stillbirth or early neonatal death) and overlaps the osteogenesis imperfecta phenotype - so much so that it may first be diagnosed as severe OI.
- Same gene, sometimes. It can be caused by the same COL1A1 c.3040C to T variant, although some prenatal cases involve other genes - which is why recognising it matters: prognosis and counselling differ completely from postnatal Caffey disease.
Q: How does the prenatal form of Caffey disease differ from the classic postnatal form?
A: The rare prenatal/antenatal form is seen on antenatal ultrasound as short, bowed long bones plus cortical hyperostosis, polyhydramnios and sometimes hydrops fetalis; it is often severe or lethal (stillbirth or early neonatal death) - completely unlike the benign, self-limiting postnatal disease - and overlaps the osteogenesis imperfecta phenotype. It can be caused by the same COL1A1 c.3040C to T variant (some cases involve other genes). Recognising it matters because prognosis and counselling differ entirely.
Guidelines, Registries & Global Practice
Global epidemiology. Caffey disease is rare and likely under-reported. Historical estimates of roughly 3 per 1000 infants reflect an era of more frequent classic disease; the incidence has fallen markedly in recent decades and the condition is now an uncommon diagnosis worldwide. It occurs across all populations with no strong ethnic predilection and a slight male predominance. Sporadic disease far outnumbers the autosomal dominant COL1A1 form, which accounts for a minority of cases.
There is no dedicated registry or disease-specific society guideline for Caffey disease; management is consensus- and case-series-based. The decisive guideline framework in practice is child-protection / suspected-physical-abuse imaging, where named-society guidance differs in emphasis:
- Core recommendation
- Standardised full skeletal survey (with follow-up survey at 11-14 days) when abuse is suspected in under-2s
- Practical implication
- Repeat imaging detects evolving fractures and helps separate healing trauma from physiological/Caffey periostitis
- Core recommendation
- Appropriateness criteria recommend skeletal survey as first-line in suspected abuse under 2 years
- Practical implication
- Defines minimum mandatory views; reduces missed occult fractures
- Core recommendation
- Skeletal survey plus multidisciplinary child-protection assessment
- Practical implication
- Mandatory reporting where abuse cannot be excluded
- Core recommendation
- Caffey disease is a recognised differential of multifocal periosteal new bone
- Practical implication
- Diaphyseal smooth periosteal reaction, mandible involvement and absence of fractures favour Caffey over abuse
Registry note. Unlike arthroplasty or fracture care, Caffey disease has no implant or procedure registry; the evidence base is genetic cohorts (e.g. multi-family COL1A1 series) and case reports rather than registry survivorship data.
High- vs limited-resource practice variation.
- Well-resourced settings: ready access to high-quality skeletal survey, MRI to exclude osteomyelitis when uncertain, COL1A1 genetic testing and formal genetic counselling for familial cases, and rapid multidisciplinary child-protection input.
- Limited-resource settings: diagnosis rests on clinical pattern and plain radiographs; genetic confirmation may be unavailable, so reliance on the classic clinico-radiological triad and exclusion of mimics (osteomyelitis, scurvy, congenital syphilis, prostaglandin exposure) is greater. The reassuring, self-limited natural history makes conservative management with simple analgesia/NSAIDs broadly applicable.
Treatment is internationally consistent: supportive care with NSAIDs (commonly off-label) as first-line; antibiotics only if osteomyelitis cannot be excluded.
Controversies and Areas of Uncertainty
The prostaglandin hypothesis and the COL1A1 collagen-I hypothesis coexist but are not unified. Sporadic disease commonly lacks any detectable COL1A1 variant, and prenatal cases may be caused by other genes (e.g. IFITM5). It is unresolved how a structural collagen defect produces a self-limited, episodic inflammatory periostitis.
NSAIDs (indomethacin/ibuprofen) reliably help symptoms, but there is no randomised evidence that they shorten the disease or change bony outcome. Because the condition is self-limiting, apparent treatment "responses" may reflect natural resolution.
Frequently quoted figures (around 3 per 1000) derive from older series; the apparent fall in incidence may be real or may reflect reclassification and better recognition of mimics. Robust contemporary epidemiology is lacking.
Variable penetrance of the COL1A1 variant makes individual prognostication difficult, and a negative gene test does not exclude the diagnosis. How aggressively to pursue genetics in apparently sporadic cases is not standardised.
Exam Cheat Sheet
Definition
- Infantile cortical hyperostosis
- Self-limiting periosteal new bone formation
- Under 6 months age
- First described Caffey and Silverman 1945
Classic Triad
- Soft tissue Swelling
- Bone lesions (hyperostosis)
- Irritability
- SBI mnemonic
Common Bones
- Mandible 70-90% (pathognomonic)
- Clavicle 30-50%
- Ulna 30-40%
- Ribs, scapula less common
- Tibia rare, spine/hands NEVER
Pathophysiology
- Prostaglandin theory (elevated PGE2)
- COL1A1 mutation (familial form)
- Chromosome 17q21
- Autosomal dominant with variable penetrance
Caffey vs NAI
- Caffey: DIAPHYSEAL periosteal reaction
- NAI: METAPHYSEAL corner fractures
- Caffey: NO fractures
- NAI: Multiple fractures different ages
- Caffey: Mandible common
- NAI: Mandible rare
Investigations
- X-ray: diaphyseal periosteal reaction
- ESR/CRP: mildly elevated
- Skeletal survey if NAI concern
- Genetic testing for familial form
Management
- NSAIDs (indomethacin) first-line
- Supportive care
- NO antibiotics unless osteomyelitis suspected
- Parent education and reassurance
Prognosis
- Excellent - complete resolution
- Self-limiting by age 2 years
- No long-term orthopaedic sequelae
- Recurrence rare (more common familial)
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 3-month-old infant presents with a 1-week history of irritability and swelling over the left jaw. The parents are concerned the baby is crying excessively. What is your approach?”
“A 4-month-old infant presents with swelling of the left arm and irritability. X-ray shows periosteal reaction along the ulna. The emergency physician is concerned about non-accidental injury. How do you proceed?”
“A 2-month-old infant is diagnosed with Caffey disease. The mother mentions her brother had 'something similar as a baby.' How does this affect your management?”
Evidence Base
Original Description by Caffey and Silverman
- First comprehensive description of infantile cortical hyperostosis
- Identified classic triad of swelling, bone changes, irritability
- Noted predilection for mandible and clavicle
- Described self-limiting natural history
COL1A1 Gene Mutation Discovery (Autosomal Dominant Caffey)
- Genome-wide linkage in a large family mapped autosomal dominant Caffey to chromosome 17q21 (LOD 6.78)
- Identified a recurrent COL1A1 missense variant c.3040C-to-T (historically R836C in triple-helical numbering, now reported as p.Arg1014Cys)
- Same variant in 3 unrelated families but absent in over 300 control chromosomes; not found in 2 prenatal cases
- Carriers showed joint hyperlaxity, hyperextensible skin and hernias, extending the COL1A1 disease spectrum
Allelic Heterogeneity of COL1A1 in Caffey Disease
- COL1A1 sequenced in 28 families with suspected Caffey disease
- Recurrent p.(Arg1014Cys) variant found in 23 families; a novel p.(Arg918Cys) variant in 5 families
- Both arginine-to-cysteine substitutions lie in the triple-helical domain of the proalpha1(I) chain
- Confirms allelic heterogeneity and that a subset of clinically typical cases lack any detectable COL1A1 variant
Prostaglandin-Induced Cortical Hyperostosis (Pharmacological Mimic)
- 10 neonates with cyanotic heart disease developed cortical hyperostosis after prolonged PGE1 infusion (9-195 days)
- Long bones, ribs, scapulae and clavicles involved, radiographically indistinguishable from Caffey disease
- Serum alkaline phosphatase rose and tracked with hyperostosis; changes were dose- and duration-dependent
- Hyperostosis regressed after prostaglandin therapy was stopped
Prenatal (Lethal) Cortical Hyperostosis with COL1A1 Mutation
- Early-onset prenatal cortical hyperostosis is typically severe and often lethal, unlike the benign postnatal form
- Prenatal ultrasound showed short, bowed long bones; postmortem radiographs showed hyperostosis of long bones, ribs and mandible
- A heterozygous COL1A1 missense variant (c.3040C-to-T) was found in fetal tissue
- Shows the COL1A1 variant can also underlie lethal prenatal disease, overlapping the osteogenesis imperfecta phenotype
Clinico-Radiological Review (Self-Limited Collagen-I Disorder)
- Comprehensive review framing Caffey disease as the first known self-regressive collagen I-related disorder
- Soft-tissue swelling with periosteal hyperostosis, mandible being a characteristic site of facial swelling in infants
- Differential diagnosis of infantile facial/bone swelling and the radiological pattern that distinguishes it
- Surgical correction may rarely be needed for residual facial or mandibular asymmetry
These studies form the evidence base for diagnosis, pathophysiology and the critical differential from non-accidental injury in Caffey disease.