Comprehensive exam-focused review of wheelchair seating and positioning principles including pelvic positioning, pressure management, postural supports, and interface with orthopaedic surgery for patients with neurological conditions
- Neutral pelvic positioning is fundamental to proximal stability
- Posterior pelvic tilt leads to sacral sitting and kyphosis
- Pressure mapping guides cushion selection and positioning
- Hip surveillance protocols essential in non-ambulatory CP
- Spinal fusion timing considers seating and sitting balance
- “ASIS alignment determines pelvic position assessment
- “Windswept deformity: combined hip abduction and contralateral adduction
- “Obliquity creates asymmetric weight distribution
- “Interface pressure target: less than 32 mmHg capillary closure pressure
- “Multidisciplinary team essential: OT, PT, orthotist, surgeon
Wheelchair Seating and Positioning
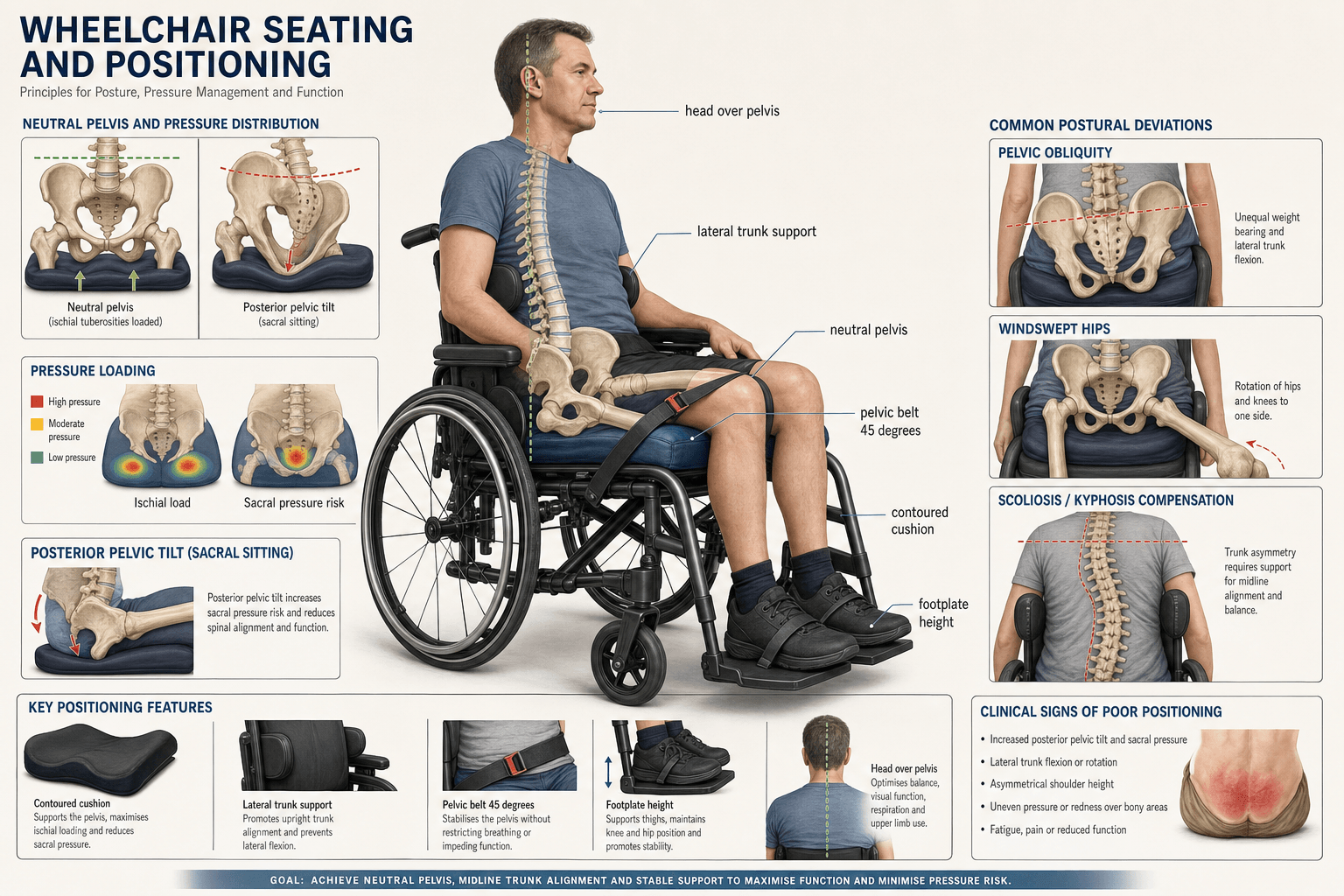
The pelvis is the foundation of seating. ASIS landmarks determine neutral versus posterior tilt. Posterior pelvic tilt causes sacral sitting, thoracic kyphosis, cervical hyperextension, and increased pressure on the sacrum and coccyx. Always assess pelvic position first.
Interface pressure must remain below capillary closure pressure of 32 mmHg to prevent tissue ischaemia. Pressure mapping technology quantifies distribution. High-risk areas include ischial tuberosities, sacrum, coccyx, greater trochanters, and scapulae. Regular weight shifts essential.
Non-ambulatory children with CP have 60-90% risk of hip displacement. Seating systems cannot prevent hip subluxation but can accommodate existing deformity. Orthopaedic surveillance every 6-12 months essential. Surgery decisions affect seating requirements.
Neuromuscular scoliosis progresses in non-ambulatory patients. Spinal fusion typically extends to pelvis (L5/S1 or ilium). Post-fusion, sitting balance changes significantly. Seating reassessment mandatory after spinal surgery. Fusion timing considers skeletal maturity.
PPFCGoals of Seating
Hook:Think PPFC like Performance, Protection, Function, Comfort for the seated patient
Overview
Wheelchair seating and positioning is a critical component of care for patients with neurological conditions who are non-ambulatory or have limited mobility. The primary goals include maintaining optimal posture, preventing pressure injuries, maximising function, and promoting comfort. The pelvis serves as the foundation of the seating system, and neutral pelvic positioning is essential for proximal stability and distal function. Proper seating reduces the risk of secondary complications including pressure ulcers, scoliosis progression, hip subluxation, and respiratory compromise. A multidisciplinary approach involving occupational therapists, physiotherapists, orthotists, and orthopaedic surgeons is essential for optimal outcomes.
- Description
- Polyurethane or viscoelastic foam layers
- Advantages
- Lightweight, low cost, good stability
- Disadvantages
- Limited pressure relief, degrades over time, heat retention
- Best For
- Low risk patients, backup cushions
- Description
- Viscous gel in flexible container
- Advantages
- Excellent pressure distribution, good stability, durable
- Disadvantages
- Heavy, may leak, temperature sensitive
- Best For
- Moderate risk, stable posture
- Description
- Interconnected air cells (e.g., ROHO)
- Advantages
- Best pressure envelopment, adjustable, lightweight
- Disadvantages
- Requires maintenance, unstable base, puncture risk
- Best For
- High risk SCI, bony prominences
- Description
- Combination of foam, gel, and/or air
- Advantages
- Balances pressure relief and stability
- Disadvantages
- More complex, higher cost
- Best For
- Mixed needs, moderate-high risk
- Description
- Moulded to patient anatomy
- Advantages
- Optimal positioning, maximum control
- Disadvantages
- Expensive, difficult to adjust, accommodates growth poorly
- Best For
- Complex deformity, fixed postures
Pathophysiology and Biomechanical Principles
The Pelvic Foundation
The pelvis serves as the foundation of the seating system and the key to proximal stability. Proper pelvic positioning enables optimal trunk alignment, head control, and upper limb function. The pelvis should be positioned in neutral alignment, with the ASIS landmarks level and the pelvis neither excessively tilted anteriorly nor posteriorly. [1]
- ASIS and pubic symphysis in vertical plane
- Weight distributed evenly on ischial tuberosities
- Lumbar lordosis preserved
- Thighs parallel to seat surface
- Sacral sitting with increased sacral pressure
- Loss of lumbar lordosis
- Thoracic kyphosis compensation
- Cervical hyperextension for visual field
- Increased risk of pressure injuries
- Compromised respiratory function
Biomechanical Principles
The seated posture involves a kinetic chain from the pelvis through the spine to the head. Optimal positioning requires understanding of force distribution, pressure management, and postural alignment. [2]
Key biomechanical considerations:
- Seat depth affects thigh support and popliteal pressure
- Seat width affects lateral trunk support availability
- Seat-to-back angle affects posture and pressure distribution
- Footrest height affects thigh loading and pelvic position
- Armrest height affects shoulder positioning and transfers
Goals of Seating Intervention
- Maintain neutral pelvic position
- Preserve or improve spinal alignment
- Support head position for function
- Prevent or accommodate deformity
- Distribute forces over maximal area
- Reduce peak pressures at bony prominences
- Enable regular pressure relief activities
- Prevent tissue breakdown
- Facilitate upper limb reach and manipulation
- Enable safe swallowing and breathing
- Support communication and vision
- Allow mobility and environmental access
- Maximise sitting duration
- Reduce pain and fatigue
- Improve quality of life
- Promote participation in activities
Clinical Assessment and Pelvic Positioning
Assessment of Pelvic Position
Clinical assessment of pelvic position requires palpation of bony landmarks with the patient seated. The ASIS landmarks are the primary reference points for determining pelvic tilt and obliquity. [3]
Assessment technique:
- Patient seated on firm surface
- Palpate bilateral ASIS landmarks
- Determine relative position to assess tilt
- Compare ASIS heights to assess obliquity
- Assess rotation by comparing ASIS to PSIS planes
- Determine if deformity is fixed or flexible
Pelvic Tilt
- ASIS and pubic symphysis in same vertical plane
- Optimal for pressure distribution
- Preserves lumbar lordosis
- Goal for most seating interventions
- ASIS posterior to pubic symphysis
- Common in hypotonic patients
- Causes sacral sitting
- Increases sacral and coccygeal pressure
- May be fixed or flexible
- ASIS anterior to pubic symphysis
- Less common in wheelchair users
- May occur with hip flexion contracture
- Can cause increased lumbar lordosis
Pelvic Obliquity
Pelvic obliquity refers to asymmetric height of the ASIS landmarks in the coronal plane. One side of the pelvis is higher than the other. [4]
- Leg length discrepancy
- Hip contracture (adduction/abduction asymmetry)
- Scoliosis (pelvic obliquity secondary to spinal curve)
- Muscle imbalance (asymmetric tone)
- Fixed bony deformity
- Determine if flexible or fixed
- Flexible obliquity can be corrected with seating
- Fixed obliquity must be accommodated
- Unilateral seat elevation or contouring
- Consider orthopaedic intervention for severe fixed cases
Pelvic Rotation
Pelvic rotation occurs when one ASIS is anterior relative to the contralateral side in the transverse plane. This is often associated with windswept hip deformity.
Windswept deformity:
- Combined hip abduction on one side and adduction on the other
- Creates apparent limb length discrepancy when supine
- Associated with pelvic rotation and obliquity
- Common in non-ambulatory cerebral palsy
- Difficult to accommodate in seating systems
Differential Diagnosis: The Deteriorating Seated Posture
A common exam and clinic scenario is the patient whose sitting has "got worse." The differential is structural, not a single diagnosis — the value lies in distinguishing causes that respond to seating adjustment from those needing surgical or medical intervention.
- Key Clinical Clue
- Slides forward, sacral pressure, kyphosis
- Flexible or Fixed
- Often flexible early
- First-Line Action
- Open seat-to-back angle, add anterior pelvic support, solid seat base
- Key Clinical Clue
- Trunk collapse to one side, pelvic obliquity, rib-on-pelvis
- Flexible or Fixed
- Becomes fixed
- First-Line Action
- Lateral trunk supports; refer for spinal surveillance/fusion
- Key Clinical Clue
- Asymmetric hips, pain on transfer, windsweeping
- Flexible or Fixed
- Fixed if chronic
- First-Line Action
- Hip surveillance radiograph (migration percentage); orthopaedic referral
- Key Clinical Clue
- Cannot achieve 90-degree hip flexion; pelvis pulled into tilt
- Flexible or Fixed
- Fixed
- First-Line Action
- Accommodate with opened angles; consider soft-tissue release
- Key Clinical Clue
- Extensor thrust, variable posture, recent illness or pain
- Flexible or Fixed
- Dynamic
- First-Line Action
- Treat trigger (pain, UTI, constipation); tone management; dynamic seating
- Key Clinical Clue
- New behaviour change, guarding, posture worse when upright
- Flexible or Fixed
- Variable
- First-Line Action
- Identify and treat source before re-prescribing seating
- Key Clinical Clue
- Sagging upholstery, child has grown, worn cushion
- Flexible or Fixed
- n/a
- First-Line Action
- Re-measure and re-prescribe; replace worn cushion
ASIS CheckPelvic Position Assessment
Hook:Always Start Inspecting the ASIS to determine pelvic position
Investigations and Pressure Management
Pathophysiology of Pressure Injuries
Pressure injuries develop when sustained external pressure exceeds capillary closure pressure (approximately 32 mmHg), leading to tissue ischaemia and necrosis. Additional contributing factors include shear forces, friction, moisture, and nutritional status. [5]
- Impaired sensation (SCI, neuropathy)
- Impaired mobility
- Incontinence
- Malnutrition
- Cognitive impairment
- Previous pressure injury
- Bony prominences
- Muscle atrophy
- Ischial tuberosities (highest risk when seated)
- Sacrum and coccyx (especially with posterior pelvic tilt)
- Greater trochanters (lateral positioning)
- Spinous processes (kyphotic patients)
- Scapulae (thin patients with high backrests)
Pressure Mapping Technology
Interface pressure mapping provides objective measurement of pressure distribution between the patient and seating surface. This technology uses sensor arrays to quantify pressure at multiple points and display results as colour-coded maps. [6]
- Cushion selection and comparison
- Positioning adjustment optimisation
- Identification of high-pressure areas
- Documentation for funding justification
- Patient and caregiver education
- Outcome measurement
- Peak pressure (maximum value at single point)
- Average pressure across contact area
- Pressure gradient (rate of change)
- Contact area (distribution of load)
- Pressure time integral (duration factor)
Cushion Selection Principles
Cushion selection depends on pressure injury risk level, positioning needs, transfer ability, lifestyle factors, and budget constraints. [7]
Selection considerations:
- Risk level (low, moderate, high, very high)
- Postural stability requirements
- Transfer method and frequency
- Weight and build of patient
- Continence status
- Maintenance capacity
- Environmental factors (temperature, moisture)
SIT TIGHTPressure Injury Risk Areas
Hook:Where you SIT TIGHT is where pressure injuries develop
Management and Postural Support
Seating System Types
- Flat surfaces at various angles
- Adjustable and versatile
- Suitable for flexible postures
- Lower cost
- Examples: solid seat insert, flat back support
- Shaped to patient anatomy
- Maximum contact and support
- Optimal for fixed deformities
- Higher cost and complexity
- Examples: custom-moulded back, seating simulator cast
Trunk Support Components
- Provide coronal plane stability
- Prevent or accommodate scoliosis
- Position varies with curve pattern
- May be fixed or swing-away
- Must not impede respiration
- Solid insert replaces sling upholstery
- Provides consistent postural support
- May be flat, contoured, or custom-moulded
- Height affects head control and comfort
- Angle affects pelvic position
Pelvic Positioning Devices
- Position pelvis in midline
- Prevent lateral migration
- May accommodate or correct obliquity
- Seat belt positioning (45-degree angle optimal)
- Subasis bar (padded bar below ASIS)
- Positioning belt systems
- Prevent forward sliding
- Pommel or medial thigh support
- Prevents adduction
- Abductor wedges for hip positioning
- Thigh guides for rotation control
Head Support Systems
- Poor active head control
- Fatigue with prolonged sitting
- Transportation safety
- Posterior head positioning
- Flat posterior support
- Contoured occipital support
- Circumferential support (complex needs)
- Dynamic headrests (allow movement)
Condition-Specific Seating Management
Seating Considerations in Cerebral Palsy
Cerebral palsy represents the most common cause of childhood physical disability, with 25-35% of affected individuals requiring a wheelchair for primary mobility. Seating needs vary significantly based on motor type (spastic, dyskinetic, ataxic, mixed) and functional level (GMFCS I-V). [8]
- May walk with assistive devices
- Wheelchair for longer distances
- Usually maintains sitting balance
- Linear seating often sufficient
- Focus on positioning for function
- Limited self-mobility
- Requires wheelchair for community
- May have some sitting balance
- May need moderate postural support
- Progressive scoliosis risk
- Dependent for all mobility
- Limited head and trunk control
- Maximum postural support required
- High risk for hip displacement
- Complex contoured seating often needed
- Prevalence in non-ambulatory: 60-90%
- Migration percentage monitoring essential
- Seating cannot prevent displacement
- Seating accommodates existing deformity
- Surgical intervention may be required
- Progressive in non-ambulatory patients
- Affects sitting balance and function
- Seating can support but not correct
- Spinal fusion may be indicated
- Post-fusion seating reassessment needed
Seating intervention in CP requires ongoing review due to growth, changing tone, and progressive deformity.
24-Hour Postural Management
The Hägglund evidence and the controversies call seating 'one arm of 24-hour postural management', but the body never explains what that means.
- Posture is managed across all 24 hours, not just in the chair. A dependent child spends the day sitting, the night lying (often the single longest posture, up to 10 to 12 hours), and ideally some time standing. A destructive or asymmetric posture in any of these - especially the many hours spent lying - drives the development of windswept hips, pelvic obliquity, scoliosis and hip subluxation.
- The three arms complement each other. Twenty-four-hour postural management combines supportive seating by day, night-time (sleep-system) positioning to hold symmetrical, supported lying, and standing (standers) for weight-bearing, hip development, bone density and stretch. The chair alone cannot protect body shape if the child lies windswept for half the day.
- Why it matters. The preferred lying posture is associated with the direction of scoliosis and windsweeping (Agustsson), so managing lying and standing - not seating in isolation - is what plausibly preserves body shape, even though the supporting evidence is largely low-level.
Q: What is 24-hour postural management, and why is seating only one part of it?
A: Posture must be managed across all 24 hours - the dependent child sits by day, lies at night (often the longest single posture, about 10 to 12 hours), and ideally stands (in a stander). A destructive or asymmetric posture in any of these - especially the many hours lying - drives windswept hips, pelvic obliquity, scoliosis and hip subluxation. So 24-hour postural management combines supportive seating (day) + night-time/sleep-system positioning (symmetrical supported lying) + standing (weight-bearing, bone density, hip development, stretch). The chair alone cannot protect body shape if the child lies windswept for half the day - the preferred lying posture correlates with the direction of scoliosis and windsweeping. The evidence is largely low-level but it is the accepted framework.
Complications and Surgical Interface
Hip Surveillance and Management
Non-ambulatory children with cerebral palsy are at high risk for hip displacement, with prevalence of 60-90% in GMFCS levels IV and V. Hip surveillance protocols recommend regular clinical and radiographic monitoring. [11]
- Clinical hip examination every 6 months
- Anteroposterior pelvis radiograph annually (minimum)
- Migration percentage calculation
- Acetabular index measurement
- Assessment of hip pain and function
- Less than 30%: observation, continue surveillance
- 30-50%: increased surveillance, consider soft tissue surgery
- More than 50%: high risk for dislocation, consider reconstruction
- Dislocated: salvage procedures may be needed
- Soft tissue releases may improve positioning
- Bony procedures require healing before seating
- Post-operative seating assessment needed
- Accommodating versus corrective approaches
Spinal Surgery Considerations
Neuromuscular scoliosis is progressive in non-ambulatory patients and frequently requires surgical intervention. Spinal fusion significantly impacts seated posture and function. [12]
- Progressive curve despite bracing
- Curve magnitude affecting function
- Pelvic obliquity causing sitting imbalance
- Respiratory compromise from curve
- Pain related to deformity
- Upper level depends on curve pattern
- Lower level typically to pelvis in neuromuscular
- L5/S1 or iliac fixation common
- Preserves versus sacrifices lumbar motion
- Sitting balance goals influence levels
- Loss of compensatory spinal motion
- Fixed spine requires seat angle matching
- Improved pelvic alignment often achieved
- May need new seating system
- Function may improve or decline
Limb Procedures and Seating
Orthopaedic procedures on the limbs affect positioning requirements and seating prescription.
- Hip flexion contracture release may improve sitting angle
- Knee flexion contracture affects footrest positioning
- Foot deformity correction improves footplate placement
- Limb length discrepancy affects pelvic position
- Elbow and wrist positioning for function
- Hand support needs at armrest level
- Splinting integration with seating
Multidisciplinary Team
Core Team Members
- Seating and positioning assessment
- Functional upper limb evaluation
- Equipment prescription
- Home and school environment assessment
- Activities of daily living training
- Physical assessment and mobility
- Postural management programmes
- Respiratory physiotherapy
- Strengthening and stretching
- Gait training when applicable
- Fabrication of custom seating components
- Orthotic devices for positioning
- Technical expertise in materials
- Fitting and adjustments
- Maintenance and repairs
- Complex seating solutions
- Power mobility systems
- Electronic access devices
- Environmental controls
- Technical problem-solving
- Hip surveillance and surgery
- Spinal deformity management
- Contracture correction
- Bone health management
- Coordination with seating team
- Medical oversight of rehabilitation
- Spasticity management
- Pain management
- Coordination of care
- Prescription authority
Assessment Process
- Medical history and diagnosis
- Physical examination (range of motion, tone, posture)
- Current equipment evaluation
- Functional assessment
- Goals identification with patient/family
- Environmental considerations
- Trial of positioning options
- Angle adjustments
- Cushion comparisons
- Component testing
- Pressure mapping
- Photography documentation
Tilt-in-Space versus Recline
The topic prescribes 'tilt-in-space or recline' for several conditions but never explains how the two differ.
- Tilt-in-space keeps the angles, changes the orientation. It tilts the whole seat and back as a fixed unit around a pivot, so the hip and knee angles are preserved while the person's orientation to gravity changes. It is the workhorse for pressure relief (shifting load off the ischial tuberosities onto the back and posterior thigh), rest, fatigue and gravity-assisted head/trunk control - and it does this without shear because the body moves as one.
- Recline opens the hip angle. The backrest reclines relative to the seat, extending the trunk on the thighs. It is useful for intermittent hip-angle change, toileting/catheterisation and comfort, but it shears the skin over the sacrum as the back slides, and in some patients opening the hip angle triggers an extensor thrust that pushes them forward out of the chair.
- So they are not interchangeable. For routine pressure relief in a patient at skin risk, tilt (angles preserved, no shear) is preferred; recline is added for specific needs, often combined with tilt to limit shear.
Q: What is the difference between tilt-in-space and recline, and when is each used?
A: Tilt-in-space tilts the whole seat and back as a unit around a pivot, preserving the hip and knee angles while changing orientation to gravity - the workhorse for pressure relief (load off the ischial tuberosities), rest and head/trunk control, without shear (the body moves as one). Recline opens the seat-to-back (hip) angle by reclining the backrest relative to the seat - useful for intermittent hip-angle change, toileting and comfort, but it shears the sacral skin as the back slides and can trigger an extensor thrust that pushes the patient forward. For routine pressure relief in a skin-at-risk patient, tilt is preferred; recline is added for specific needs, often combined with tilt.
Guidelines, Registries & Global Practice
Wheelchair seating need is driven by the global burden of cerebral palsy (roughly 2-3 per 1000 live births, the commonest cause of childhood physical disability), traumatic and non-traumatic spinal cord injury (global incidence on the order of 250,000-500,000 new cases per year), and progressive neuromuscular disease (Duchenne muscular dystrophy ~1 in 3500-5000 male births). Access to appropriate seating varies enormously between high-resource and limited-resource settings.
Side-by-Side Guidance
- Focus
- Wheelchair provision
- Core Recommendation
- 8-step service-delivery model (assess, prescribe, fit, train, follow-up); appropriate manual wheelchairs for less-resourced settings
- Focus
- CP hip displacement
- Core Recommendation
- GMFCS-stratified clinical and radiographic surveillance using migration percentage; refer when migration percentage rises or exceeds ~30-40%
- Focus
- Pressure injury
- Core Recommendation
- Risk assessment, individualised support surface, repositioning/weight-shift, skin inspection, nutrition
- Focus
- Neuromuscular
- Core Recommendation
- Anticipatory powered mobility with tilt/recline, scoliosis and respiratory surveillance
- Focus
- Seating standards
- Core Recommendation
- Clinician-led assessment, trial, pressure mapping and documentation before complex prescription
Registry and Surveillance Evidence
Population registers, rather than implant registries, drive practice here. The Swedish CPUP and the Victorian (Australian) CP registers generated the GMFCS-stratified hip-displacement data (Soo et al.) and the surveillance-reduces-surgery evidence (Hägglund et al.) that underpin worldwide hip surveillance programmes now adopted in the UK, Scandinavia, Australia and beyond.
High- vs Limited-Resource Practice
- High-resource settings: multidisciplinary seating clinics, pressure mapping, custom-moulded and powered tilt/recline systems, formal hip surveillance programmes, and third-party funding for complex assistive technology.
- Limited-resource settings: emphasis on appropriate, durable, locally maintainable manual wheelchairs (WHO model), simpler postural supports, and caregiver training; custom seating, pressure mapping and powered mobility are frequently unavailable, raising pressure injury and deformity risk. The clinical principles (neutral pelvis, pressure distribution, regular repositioning) remain universal even where the technology does not.
Controversies and Areas of Uncertainty
Wheelchair seating is an area where strong physiological rationale often outruns high-level trial evidence. Examiners reward candidates who can state what is genuinely established versus what is consensus or extrapolation.
- Does seating prevent hip displacement in CP? No. Postural management and abduction positioning are widely used, but evidence that day seating prevents hip migration is weak; the Soo cohort and current surveillance practice treat hip displacement as a natural-history problem managed by radiographic surveillance and surgery, not by the chair. Seating accommodates, it does not protect the hip.
- The 32 mmHg "capillary closure" target. The figure derives from Landis's 1930 nailfold capillary measurements and is widely quoted, but real interface pressures over the ischium routinely exceed it without ulceration, and tissue tolerance varies with shear, time, perfusion and individual factors. Treat 32 mmHg as a teaching benchmark, not an absolute threshold; deep-tissue injury may begin at the muscle-bone interface independent of surface pressure.
- Air versus gel versus foam. The Brienza RCT shows specified skin-protection cushions beat plain foam, but it does not establish superiority of any one skin-protection technology. Cushion choice remains individualised to risk, posture, transfer technique and maintenance capacity rather than dictated by trial data.
- Standing programmes and 24-hour postural management. Biologically plausible for bone density, contracture and comfort, but supporting evidence is largely low-level; intensity and dosing remain uncertain.
- Timing of neuromuscular spinal fusion. Tension between operating early (better pulmonary reserve, more flexible curve) and delaying for skeletal growth; no consensus threshold, decisions are individualised around curve magnitude, FVC trajectory and pelvic obliquity.
- Powered versus manual mobility in young children. Early powered mobility may aid development and participation, but concerns about cost, safety and deconditioning mean practice varies widely.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 10-year-old child with spastic quadriplegic cerebral palsy (GMFCS level V) is referred for wheelchair seating assessment. The parents report increasing difficulty with positioning and skin redness over the sacrum. On examination, there is a posterior pelvic tilt when seated, thoracolumbar scoliosis, and bilateral hip flexion contractures of 30 degrees. How would you approach this patient?”
“A 25-year-old male with T6 complete spinal cord injury from a motorcycle accident 6 months ago is transitioning from rehabilitation to community living. He has had no pressure injuries during rehabilitation but you are asked to optimise his seating for community use. What are the key considerations and how would you prescribe an appropriate cushion?”
“A 14-year-old boy with Duchenne muscular dystrophy has progressive scoliosis now measuring 55 degrees. He has been wheelchair-dependent for 2 years. His respiratory function is declining with FVC of 60% predicted. The spinal surgeon is considering posterior spinal fusion. How does seating assessment inform surgical planning, and what changes do you anticipate post-operatively?”
Goals of Seating (PPFC)
- Posture: maintain alignment, prevent deformity
- Pressure: distribute load, prevent injury
- Function: optimise upper limb use, mobility
- Comfort: ensure tolerance, quality of life
Pelvic Position
- Pelvis is foundation of seating system
- ASIS landmarks determine tilt and obliquity
- Neutral: ASIS and pubic symphysis vertical
- Posterior tilt: sacral sitting, kyphosis, increased pressure
- Obliquity: unequal ASIS heights, asymmetric loading
Pressure Management
- Capillary closure pressure: approximately 32 mmHg
- High-risk areas: ischial tuberosities, sacrum, trochanters
- Pressure mapping: objective cushion comparison
- Weight shifts every 15-30 minutes in SCI
- Cushion types: foam, gel, air, hybrid, custom
Cushion Selection
- Foam: low cost, limited relief, good stability
- Gel: good pressure relief, heavy, stable
- Air: best envelopment, maintenance required, unstable
- Hybrid: balances pressure relief and stability
- Match to risk level and functional needs
Seating System Types
- Linear (planar): flat surfaces, adjustable, versatile
- Contoured (custom): shaped to anatomy, maximum support
- Solid seat insert replaces sling upholstery
- Lateral trunk supports for scoliosis
- Pelvic guides and positioning belts for control
Condition-Specific Considerations
- CP: hip surveillance, scoliosis management, GMFCS level
- SCI: pressure prevention paramount, sensation absent
- DMD: progressive weakness, respiratory needs, scoliosis
- All: ongoing review essential
Orthopaedic Interface
- Hip displacement: 60-90% in non-ambulatory CP
- Seating accommodates but cannot prevent displacement
- Spinal fusion changes sitting balance significantly
- Post-surgical seating reassessment mandatory
- Hip flexion contractures require opened seat-to-back angle
Multidisciplinary Team
- OT: seating assessment, prescription, function
- PT: physical assessment, mobility, respiratory
- Orthotist: custom fabrication, fitting, repairs
- Orthopaedic surgeon: hip and spine surgery
- Rehabilitation physician: coordination, spasticity
Evidence Base
Hip Displacement in Cerebral Palsy (Victorian Cohort)
- Overall hip displacement incidence 35% across the birth cohort
- 0% at GMFCS I versus 90% at GMFCS V (linear gradient)
- Relative risk versus GMFCS II: III 2.7, IV 4.6, V 5.9
- Justifies GMFCS-based surveillance and resource allocation
Skin-Protection Cushions Prevent Pressure Ulcers (RCT)
- N = 232; 6-month follow-up across 12 nursing homes
- Ischial ulcers 0.9% (skin-protection) vs 6.7% (foam), P = 0.04
- Combined ischial plus sacral ulcers 10.6% vs 17.6% (NS)
- Cushion type and correct fit both matter for prevention
Reliability of Interface Pressure Map Interpretation
- Visual pressure-map ranking reliable vs numerical data
- Significant intra- and inter-rater agreement (P less than 0.001)
- Reliable across operator experience levels and surfaces
- Validates pressure mapping as a routine assessment tool
Fusion to the Pelvis for Cerebral Palsy Scoliosis
- N = 287; scoliosis 76 to 25 degrees (68% correction)
- Pelvic obliquity 17 to 5 degrees (71% correction)
- Deep infection ~6%, 3 perioperative deaths
- 96% caretaker-reported satisfaction
GMFCS Predicts Sitting and Standing Performance
- N = 562 (total population, ages 3-18)
- Adaptive seating use 42% overall, rising with GMFCS
- 99% could sit and 96% could stand with supports
- GMFCS strongly predicts seating/positioning needs
Population Surveillance Reduces CP Orthopaedic Surgery
- Surgery for contracture/torsion fell 40% to 15% (P = 0.0019)
- Range of motion improved in non-ambulant children
- Severe contractures largely prevented
- Surveillance plus early tone/posture management is effective
Standards of Care in Duchenne Muscular Dystrophy
- Multidisciplinary, anticipatory model alters natural history
- Powered mobility with tilt/recline after loss of ambulation
- Scoliosis and respiratory surveillance integral to seating
- Coordinated care improves function and longevity
References
-
Letts M, Rang M. Seating and positioning for children with cerebral palsy. In: Pediatric Orthopaedics. 3rd ed. Saunders; 1997:1112-1145.
-
Hobson DA, Tooms RE. Seated lumbar/pelvic alignment. A comparison between spinal cord-injured and noninjured groups. Spine. 1992;17(3):293-298.
-
Holmes KJ, Michael SM, Thorpe SL, Solomonidis SE. Management of scoliosis with special seating for the non-ambulant spastic cerebral palsy population. Clin Biomech. 2003;18(6):480-487.
-
Ágústsson A, Sveinsson Þ, Pope P, Rodby-Bousquet E. Preferred posture in lying and its association with scoliosis and windswept hips in adults with cerebral palsy. Disabil Rehabil. 2019;41(26):3198-3202.
-
National Pressure Ulcer Advisory Panel and European Pressure Ulcer Advisory Panel. Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline. National Pressure Ulcer Advisory Panel; 2014.
-
Stinson MD, Porter-Armstrong AP, Eakin PA. Pressure mapping systems: reliability of pressure map interpretation. Clin Rehabil. 2003;17(5):504-511.
-
Brienza D, Kelsey S, Karg P, et al. A randomized clinical trial on preventing pressure ulcers with wheelchair seat cushions. J Am Geriatr Soc. 2010;58(12):2308-2314.
-
Rodby-Bousquet E, Hägglund G. Sitting and standing performance in a total population of children with cerebral palsy: a cross-sectional study. BMC Musculoskelet Disord. 2010;11:131.
-
Consortium for Spinal Cord Medicine. Pressure ulcer prevention and treatment following spinal cord injury: a clinical practice guideline for health-care professionals. J Spinal Cord Med. 2001;24(Suppl 1):S40-101.
-
Bushby K, Finkel R, Birnkrant DJ, et al. Diagnosis and management of Duchenne muscular dystrophy, part 2: implementation of multidisciplinary care. Lancet Neurol. 2010;9(2):177-189.
-
Soo B, Howard JJ, Boyd RN, et al. Hip displacement in cerebral palsy. J Bone Joint Surg Am. 2006;88(1):121-129.
-
Tsirikos AI, Lipton G, Chang WN, Dabney KW, Miller F. Surgical correction of scoliosis in pediatric patients with cerebral palsy using the unit rod instrumentation. Spine. 2008;33(10):1133-1140.
-
Hägglund G, Andersson S, Düppe H, Lauge-Pedersen H, Nordmark E, Westbom L. Prevention of severe contractures might replace multilevel surgery in cerebral palsy: results of a population-based health care programme and new techniques to reduce spasticity. J Pediatr Orthop B. 2005;14(4):269-273.
-
Rodby-Bousquet E, Hägglund G. Sitting and standing performance in a total population of children with cerebral palsy: a cross-sectional study. BMC Musculoskelet Disord. 2010;11:131.
-
World Health Organization. Guidelines on the Provision of Manual Wheelchairs in Less-Resourced Settings. Geneva: WHO; 2008.