Achilles Avulsion | ORIF Required | Tension Band Wiring
- Achilles avulsion injury - posterior tuberosity is the Achilles footprint; displacement causes loss of push-off and a tented heel
- Skin is the emergency, not the bone - the displaced fragment tents posterior heel skin; pressure necrosis can occur within hours, so urgent reduction is mandatory
- Displacement drives prognosis - Carnero-Martin showed displacement of 2cm or more raises complications from 30% to 91% and soft-tissue compromise from 0% to 45%
- Insufficiency / Charcot fracture - common in elderly osteoporotic women and diabetics; low-energy mechanism, poor bone quality complicates fixation
- Sural nerve at risk in the posterolateral approach; protect it during exposure
- “The skin over the heel is the time-critical issue - tenting demands urgent reduction
- “Lee classification has 4 types; Beavis classification is NOT prognostic (Carnero-Martin)
- “Displacement (not fracture type) predicts complications and soft-tissue compromise
- “Always check Achilles power and screen for diabetes / osteoporosis
The displaced fragment tents posterior heel skin - In thin, elderly or diabetic patients, pressure necrosis can develop within hours. This is the time-critical issue, not the bone. Urgent reduction (closed or open) is mandatory to protect the soft-tissue envelope.
The posterior tuberosity is the Achilles footprint - Displacement causes loss of plantarflexion power, a positive Thompson-type picture and difficulty with single-leg heel raise. ORIF restores the lever arm and gastroc-soleus tension.
Magnitude of displacement drives prognosis - Carnero-Martin showed displacement greater than or equal to 2cm raised complications from 30% to 91% and soft-tissue compromise from 0% to 45%. The Beavis classification was NOT prognostic.
Think bone quality and Charcot - Many of these are insufficiency or Charcot (Brodsky 3B) avulsions in osteoporotic women and diabetics. Poor bone makes simple screw purchase fail; suture anchors, tension band and gastroc recession may be needed.
- Description
- Simple extra-articular avulsion (sleeve)
- Achilles fibres / mechanism
- All fibres; accidental trip / fall
- Typical patient
- Elderly women (commonest, 8/20)
- Description
- Beak fracture
- Achilles fibres / mechanism
- All fibres; often direct blow
- Typical patient
- Younger male
- Description
- Infrabursal avulsion, middle-third
- Achilles fibres / mechanism
- Superficial fibres only; fall
- Typical patient
- Younger male
- Description
- Beak with small superior triangular fragment
- Achilles fibres / mechanism
- Deep fibres; fall
- Typical patient
- Younger male
The morphological classifications (Lee, Beavis) describe the fracture but do not predict outcome. Carnero-Martin (J Foot Ankle Surg 2019) showed that displacement magnitude is the variable that drives complications and soft-tissue compromise, and proposed a displacement-based prognostic classification. In the exam, classify the morphology but manage by displacement and skin status.
Overview and Epidemiology
Calcaneal tuberosity fractures are rare but important injuries involving the posterior tuberosity of the calcaneus, which serves as the insertion site for the Achilles tendon. These fractures represent avulsion injuries and require ORIF if displaced to prevent loss of plantarflexion power and equinus contracture.
Definition
Calcaneal tuberosity fracture: Fracture of the posterior tuberosity of the calcaneus, which:
- Serves as insertion site for Achilles tendon
- Represents avulsion injury
- Causes loss of plantarflexion power
Achilles tendon insertion:
- Location: Posterior tuberosity of calcaneus
- Function: Plantarflexion and push-off
- Avulsion: Excessive tension causes avulsion with bone fragment
Epidemiology
- Incidence: Rare - approximately 1.3-2.7% of all calcaneal fractures (Lee 2012 found 20/764 = 2.6%)
- Age: Typically older adults; Carnero-Martin series mean age 57 years
- Gender: Female predominance (around 62% in Carnero-Martin), reflecting post-menopausal osteoporosis
- Comorbidity: Diabetes in roughly 1 in 5 (19% in Carnero-Martin); many are insufficiency or Charcot-related avulsions
- Mechanism: 71% low-energy (trip/fall) in Carnero-Martin; less commonly direct blow (Lee type II) or high-energy
- Associated injuries: Ipsilateral foot/ankle fractures; assess the whole hindfoot
Calcaneal tuberosity fracture = Achilles tendon avulsion - Tuberosity is insertion site for Achilles tendon. Avulsion causes loss of plantarflexion power and inability to push off. ORIF required if displaced to prevent equinus contracture.
Anatomy and Pathophysiology
Calcaneal Tuberosity Anatomy
Posterior tuberosity of calcaneus:
- Location: Posterior aspect of calcaneus
- Function: Insertion site for Achilles tendon
- Size: Large, prominent posterior projection
- Blood supply: Branches from posterior tibial artery
Achilles tendon insertion:
- Location: Posterior tuberosity of calcaneus
- Function: Plantarflexion and push-off
- Width: 1.5-2cm at insertion
- Avulsion: Excessive tension causes avulsion with bone fragment
Sural nerve:
- Location: 1-2cm posterior to lateral malleolus
- Function: Sensory to lateral foot
- Risk: At risk in posterior approach
Pathophysiology
Injury mechanism:
- Sudden plantarflexion: Eccentric contraction of gastrocnemius-soleus
- Excessive tension: Achilles tendon experiences excessive tension
- Avulsion: Tendon avulses from tuberosity with bone fragment
- Low-energy / insufficiency: Often in osteoporotic or diabetic (Charcot) bone where minor force avulses a weakened tuberosity
Why displacement matters:
- Loss of function: Displacement causes loss of plantarflexion power
- Equinus contracture: Proximal migration causes equinus
- Push-off weakness: Inability to push off affects gait
Why ORIF required:
- Restore function: Anatomic reduction restores plantarflexion
- Prevent contracture: Prevents equinus contracture
- Early motion: Stable fixation allows early motion
Classification Systems
Lee Classification (Clin Orthop Surg 2012)
Derived from 20 tuberosity fractures (of 764 calcaneal fractures), correlating surgical and MRI findings:
Type I - Simple extra-articular avulsion ("sleeve"):
- Most common (8/20); typically elderly women after a trip/fall
- All Achilles fibres involved
Type II - Beak fracture:
- Often a direct blow to the bone
- All Achilles fibres involved; skin over apex at risk
Type III - Infrabursal avulsion, middle-third:
- Caused by a fall; only superficial Achilles fibres involved
- Diagnosis often needs MRI to localise
Type IV - Beak with small superior triangular fragment:
- Caused by a fall; deep Achilles fibres involved
- MRI helps confirm fibre involvement
Morphology guides exposure but not prognosis.
Clinical Assessment
History
Symptoms:
- Posterior heel pain: Pain in posterior heel
- Loss of plantarflexion: Unable to push off
- Swelling: Localised to posterior heel
- Difficulty walking: Pain with weight bearing
Mechanism:
- Sudden plantarflexion
- Fall
- Direct trauma to heel
Physical Examination
Inspection:
- Swelling in posterior heel
- Ecchymosis (may be delayed)
- Deformity (proximal migration of fragment)
Palpation:
- Tenderness over calcaneal tuberosity
- Gap at fracture site (if displaced)
- Achilles tendon continuity (may be disrupted)
Range of Motion:
- Loss of active plantarflexion
- Passive plantarflexion may be limited
- Equinus deformity (if displaced)
Special tests:
- Active plantarflexion: Unable to perform (loss of power)
- Thompson test: May be positive (Achilles dysfunction)
- Straight leg raise: May be limited (pain)
Loss of active plantarflexion is key finding - Patient unable to push off or perform single-leg heel raise. This indicates Achilles dysfunction and requires ORIF if displaced. Always inspect the posterior heel skin for blanching or tenting - this is the urgent issue.
Differential Diagnosis
- Key feature
- Posterior heel pain, weak push-off, tented skin
- Discriminator
- Bony fragment displaced proximally by Achilles
- Imaging
- Lateral radiograph shows avulsed fragment
- Key feature
- Sudden 'kick', palpable gap in tendon
- Discriminator
- Positive Thompson test, NO bony fragment
- Imaging
- Ultrasound/MRI show tendon gap, normal bone
- Key feature
- Chronic posterior heel pain, no trauma
- Discriminator
- Gradual onset, no avulsed fragment
- Imaging
- Enthesophyte, calcification, no acute fracture
- Key feature
- Higher-energy, hindfoot swelling
- Discriminator
- Fracture line enters posterior facet; skin at apex at risk
- Imaging
- CT shows joint involvement and Bohler angle loss
- Key feature
- Insidious heel pain, osteoporosis/diabetes
- Discriminator
- No discrete displaced fragment, positive squeeze
- Imaging
- MRI marrow oedema; subtle on radiograph
Investigations
Standard X-ray Protocol
Lateral view (best view):
- Shows calcaneal tuberosity
- Assess displacement
- Proximal migration of fragment
Axial view (Harris view):
- Shows tuberosity from below
- Assess displacement
AP view:
- May show fracture
- Less reliable than lateral
Key point: Displacement greater than 2mm requires ORIF.
Management Algorithm
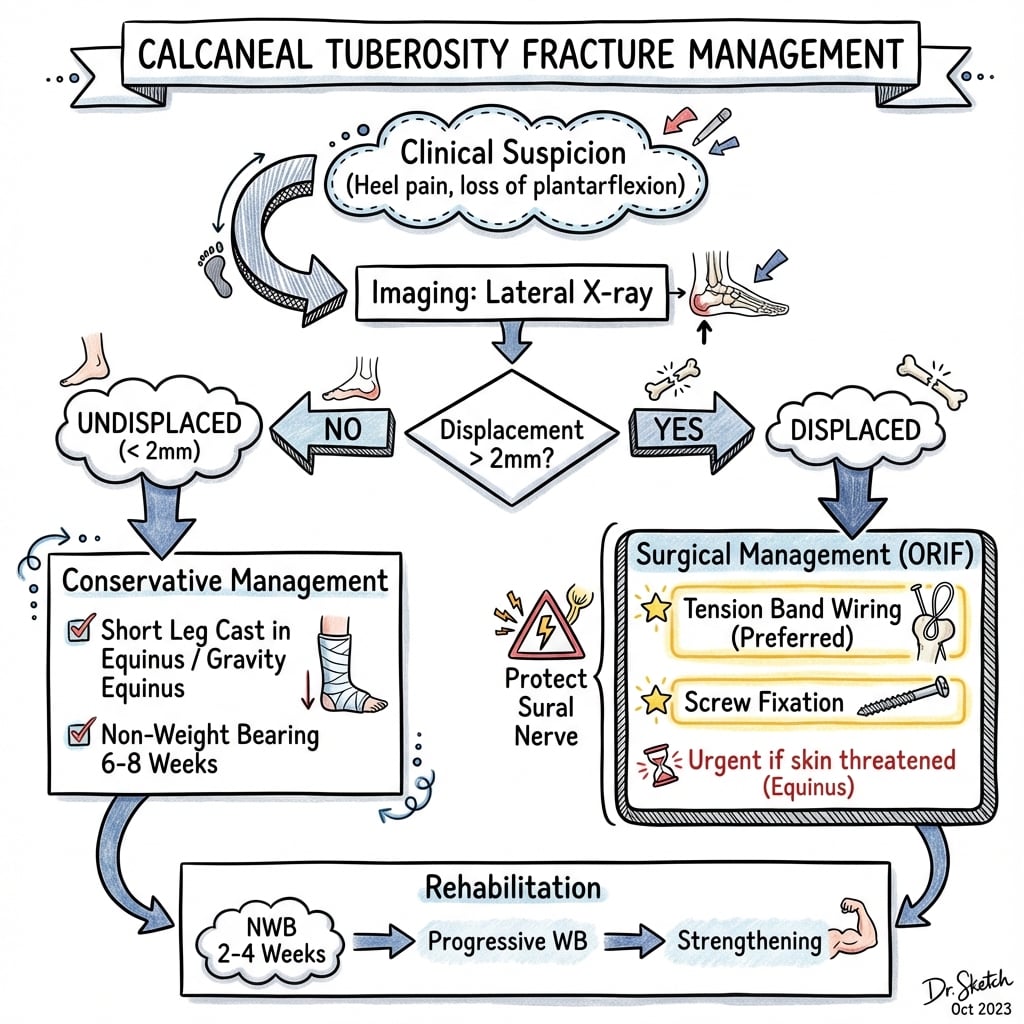

Management Pathway
Calcaneal Tuberosity Fracture Management
Loss of active plantarflexion is key finding. X-rays show calcaneal tuberosity fracture. Assess displacement - greater than 2mm requires ORIF.
If non-displaced (less than 2mm) and intact extensor mechanism, conservative treatment with cast and non-weight bearing for 6-8 weeks. Success rate 85-90% (rare).
If displaced (greater than 2mm) or loss of plantarflexion, ORIF required. Tension band wiring preferred - converts tensile force to compression, allows early motion. Success rate 80-90%.
Tension band wiring preferred - K-wires or screws with figure-8 wire. Converts tensile force from Achilles to compression at fracture site. Allows early motion and weight bearing. Success rate 80-90%.
ORIFTreatment Decision
Hook:ORIF: ORIF Required if displaced, Insertion site, Fixation with tension band!
Surgical Technique

Tension Band Wiring Technique (Preferred)
Indications:
- Most calcaneal tuberosity fractures
- Displaced fractures
- Allows early motion
Approach:
- Posterior midline or posterolateral approach
- Expose tuberosity
- Protect sural nerve
Technique:
- Exposure: Posterior approach, expose tuberosity, protect sural nerve
- Reduction: Anatomic reduction of fragment to calcaneus
- K-wires: Two parallel K-wires (2.0-2.5mm) from tuberosity into calcaneus
- Tension band: Figure-8 wire (1.2-1.25mm) around K-wires and through Achilles
- Tensioning: Tension wire to convert tensile force to compression
- Verification: Confirm reduction and hardware position fluoroscopically
Advantages:
- Converts tensile force to compression
- Allows early motion
- Biomechanically favorable
- High union rate
Tension band wiring is preferred technique.
Complications
- Incidence
- 5-10%
- Risk Factors
- Posterior approach
- Prevention/Management
- Protect nerve, identify early
- Incidence
- 10-15%
- Risk Factors
- Delayed treatment, inadequate fixation
- Prevention/Management
- Early ORIF, adequate fixation
- Incidence
- 10-15%
- Risk Factors
- Inadequate reduction, delayed treatment
- Prevention/Management
- Anatomic reduction, early treatment
- Incidence
- 5-10%
- Risk Factors
- Inadequate fixation, displacement
- Prevention/Management
- Rigid fixation, bone graft if needed
- Incidence
- 20-30%
- Risk Factors
- Tension band wires
- Prevention/Management
- Bury wires, remove if symptomatic
Sural Nerve Injury
5-10% incidence:
- Cause: Posterior approach, nerve at risk
- Prevention: Identify and protect sural nerve (1-2cm posterior to lateral malleolus)
- Management: Neuroma excision if symptomatic
Equinus Contracture
10-15% incidence (if untreated):
- Cause: Proximal migration of fragment, delayed treatment
- Prevention: Early ORIF, adequate fixation
- Management: Stretching, serial casting, or surgical release
SURALComplications
Hook:SURAL: Sural nerve risk, Unable to push off, Risk of equinus, Achilles dysfunction, Loss of strength!
Postoperative Care
Immediate Postoperative
- Immobilisation: Short leg cast or boot
- Weight bearing: Non-weight bearing initially (2-4 weeks)
- ROM: Ankle ROM exercises early (if stable fixation)
- PT: Plantarflexion strengthening
Rehabilitation Protocol
Weeks 0-2:
- Short leg cast, non-weight bearing
- Elevation to reduce swelling
- Ankle ROM exercises (if stable)
Weeks 2-4:
- Transition to walking boot
- Progressive weight bearing (if stable)
- Plantarflexion strengthening
Weeks 4-8:
- Full weight bearing
- Progressive activity
- Return to sport (3-4 months)
Outcomes and Prognosis
Overall Outcomes
ORIF (tension band wiring):
- Success rate: 80-90% (union, pain relief)
- Functional outcomes: 75-85% return to pre-injury level
- Plantarflexion: 80-90% restore normal strength
ORIF (screw fixation):
- Success rate: 75-85% (union, pain relief)
- Functional outcomes: 70-80% return to pre-injury level
- Plantarflexion: 75-85% restore normal strength
Conservative (non-displaced, rare):
- Success rate: 85-90% (union, pain relief)
- Functional outcomes: 80-85% return to pre-injury level
- Plantarflexion: 85-90% restore normal strength
Long-Term Prognosis
Plantarflexion recovery:
- With proper treatment: 80-90% restore normal strength
- Without treatment: 20-30% develop permanent weakness
- Risk factors: Displacement, delayed treatment, inadequate fixation
Guidelines, Registries & Global Practice
Global Epidemiology
- Rare injury: roughly 1.3-2.7% of all calcaneal fractures across published series
- Bimodal pattern: low-energy insufficiency avulsions in elderly osteoporotic women (Lee type I) and higher-energy or direct-blow patterns in younger men
- Strong association with osteoporosis and diabetes/Charcot neuroarthropathy; diabetic prevalence around 19% in surgical series
Society Guidance and Practice Points (Side by Side)
- Emphasis
- Soft-tissue and gastroc-soleus
- Take-home
- Early recognition; protect heel skin; address gastroc tightness
- Emphasis
- Tension-band biomechanics
- Take-home
- Convert Achilles tensile load to interfragmentary compression; stable fixation allows functional rehab
- Emphasis
- Limb-threatening soft tissue
- Take-home
- Treat threatened skin as urgent; early senior decision-making and combined ortho-plastic input
- Emphasis
- Displacement and imaging
- Take-home
- Classify morphology but manage by displacement; use CT for bone and MRI for soft tissue
Registry and Resource-Setting Notes
- No arthroplasty registry applies; evidence is from institutional series, so practice variation is wide and surgeon-dependent.
- High-resource settings: ready access to CT/MRI, multiple implant options (tension band, cannulated screws, suture anchors) and combined ortho-plastic cover for threatened skin.
- Limited-resource settings: reliance on radiographs alone, K-wire and cerclage-based tension band constructs (low cost, effective), and a lower threshold for fragment excision and Achilles reattachment when implants or soft-tissue cover are unavailable. Urgent reduction to save skin remains universal and equipment-independent.
A common foot and ankle viva. Lead with the skin emergency (urgent reduction of the tented heel), then the Achilles avulsion mechanism and loss of push-off. Quote the Lee classification (4 types) and the key point that displacement, not morphology, predicts outcome (Carnero-Martin: displacement greater than or equal to 2cm raises complications to around 91%). Flag the diabetic/osteoporotic insufficiency pattern and how poor bone changes fixation. Be ready to describe tension band wiring in detail and to protect the sural nerve.
Controversies and Areas of Uncertainty
The evidence base for these fractures is limited to small retrospective series and case reports, so several questions remain genuinely unsettled:
- Which classification to use - Morphological schemes (Lee, Beavis) describe the fracture but Carnero-Martin showed they do not predict outcome. A displacement-based prognostic classification is proposed but not yet validated in larger cohorts.
- Fixation construct - Tension band wiring, large cannulated lag screws, plate fixation and suture anchors are all described; no comparative trial establishes superiority. Choice is driven by fragment size, bone quality and surgeon preference rather than high-level evidence.
- Fragment excision versus fixation - In small fragments or very poor (neuropathic/osteoporotic) bone, some advocate excision with Achilles reattachment plus gastrocnemius recession rather than struggling to fix unfixable bone.
- Urgency threshold - There is consensus that threatened skin demands urgent reduction, but the exact displacement or skin-tenting threshold that mandates emergency surgery is not precisely defined.
- Role of gastrocnemius lengthening - Whether to routinely address gastroc-soleus tightness at index surgery to reduce re-displacement is advocated by some (Banerjee) but not standardised.
- Hardware removal - Tension band wires are frequently prominent in this subcutaneous location; rates and timing of elective removal vary widely.
MCQ Practice Points
Q: What is the relationship between calcaneal tuberosity fractures and Achilles tendon function? A: Calcaneal tuberosity is insertion site for Achilles tendon - Avulsion causes loss of plantarflexion power and inability to push off. ORIF required if displaced to restore function and prevent equinus contracture.
Q: When is ORIF required for calcaneal tuberosity fractures? A: Displacement greater than 2mm or loss of active plantarflexion - Prevents equinus contracture and loss of push-off strength. Tension band wiring preferred - converts tensile force to compression, allows early motion.
Q: Why is tension band wiring preferred for calcaneal tuberosity fractures? A: Converts tensile force from Achilles to compression at fracture site - Biomechanically superior to screw fixation alone. Allows early motion and weight bearing. High union rate (80-90% good results).
Q: What structure is at risk in the posterior approach for calcaneal tuberosity fractures? A: Sural nerve - Runs 1-2cm posterior to lateral malleolus. Injury causes lateral foot numbness and painful neuroma. Protect nerve during exposure (5-10% injury rate).
Q: What is the main complication of untreated calcaneal tuberosity fractures? A: Equinus contracture - Proximal migration of fragment causes contracture in 10-15% if untreated. Early ORIF prevents contracture. Adequate fixation essential to maintain reduction.
Calcaneal Insufficiency Avulsion (CIA) and the Brodsky 3B Pattern
The topic repeatedly flags an "insufficiency" or "Charcot" avulsion and labels it "Brodsky 3B" (in the One-Pager, the InfoCard grid, the Greenhagen evidence card and viva scenario 3) without defining the entity. The calcaneal insufficiency avulsion (CIA) fracture is a distinct sub-group that every candidate should be able to separate from an ordinary traumatic avulsion.
What CIA means
- Definition - a posterior tuberosity avulsion occurring through pathologically weak bone with little or no trauma. Greenhagen (already cited) notes that CIA fractures make up part of the 1.3-2.7% of calcaneal fractures attributed to reduced bone mineral density, and that in a person with diabetes the avulsion most likely represents a Charcot neuroarthropathy event rather than a simple mechanical failure.
- Where "Brodsky 3B" fits - the Brodsky anatomic classification locates Charcot neuroarthropathy by region: midfoot (type 1, the commonest), hindfoot (type 2) and ankle (type 3A) are developed in the dedicated Charcot topic. Type 3B denotes the posterior calcaneus - a pathologic avulsion of the tuberosity (os calcis). Labelling a tuberosity avulsion "Brodsky 3B" therefore signals a neuropathic, insufficiency mechanism, not a high-energy injury.
Why it changes management
- Neuropathic/osteoporotic bone gives poor screw purchase, so conventional lag-screw ORIF frequently fails or loses reduction.
- Greenhagen's described answer was fragment excision, gastrocnemius recession, and double-row suture-anchor Achilles reattachment (rearfoot AOFAS improved from 27 to 88 at one year) rather than struggling to fix unfixable bone.
- Suspect CIA when the avulsion is spontaneous or follows trivial force, when the patient is diabetic or neuropathic, and always screen for previously undiagnosed diabetes and peripheral neuropathy and assess bone quality before planning fixation.
A spontaneous or low-trauma calcaneal tuberosity avulsion is a red flag for a Charcot insufficiency (Brodsky 3B) event - check the sensory examination and blood glucose, anticipate poor bone, and be ready to abandon screws for suture anchors and tendon reattachment. The full Brodsky Charcot classification and its reconstructive principles belong to the Charcot neuroarthropathy topic; here the point is simply that "Brodsky 3B" flags a neuropathic os-calcis avulsion.
ACHILLESCalcaneal Tuberosity Features
Hook:ACHILLES: Achilles avulsion, Calcaneal tuberosity, Heel pain, Insertion site, Loss of plantarflexion, Lateral nerve risk, Equinus contracture, Surgery required!
Emergency Closed Reduction of the Tented Heel
The topic's single loudest message is that the skin, not the bone, is the emergency, yet the actual skin-saving maneuver is never described. When the proximally migrated fragment tents or blanches the posterior heel skin, provisional reduction should be attempted urgently - ideally within hours - before pressure necrosis develops.
The maneuver
- Relax the deforming force first - flex the knee and hold the ankle in plantarflexion (equinus) to slacken the gastrocnemius-soleus-Achilles complex that is pulling the fragment proximally.
- Reduce and decompress - with the muscle relaxed, apply direct manual pressure over the displaced fragment to push it back down onto the tuberosity bed, relieving the skin.
- Hold and reassess - immobilise in a well-padded plantarflexion (equinus) splint or backslab, then confirm that skin colour, blanching and capillary refill improve.
When closed reduction is enough, and when to open
- Closed reduction is a temporising measure to protect the soft-tissue envelope; it rarely gives a stable definitive result because the strong Achilles pull re-displaces the fragment, so definitive fixation still follows once soft tissues allow.
- If plantarflexing the ankle and manual pressure fail to relieve skin tenting or blanching, this converts to an emergency open reduction to decompress the skin directly - do not wait for an elective list when the heel skin is white.
Knee flexion plus ankle plantarflexion unloads the Achilles; then push the fragment down and splint in equinus - do it within hours of recognising a tented, blanched heel. If the skin does not decompress, go straight to emergency open reduction. Provisional reduction saves the skin; it does not replace definitive fixation.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 55-year-old woman presents with posterior heel pain and inability to push off after fall. Clinical examination shows loss of active plantarflexion and palpable gap at calcaneal tuberosity. X-rays show displaced calcaneal tuberosity fracture with 5mm proximal migration.”
“A 50-year-old patient has a displaced calcaneal tuberosity fracture requiring ORIF. The examiner asks you to describe the tension band wiring technique in detail.”
“A 68-year-old woman with type 2 diabetes and peripheral neuropathy presents 36 hours after a trip. There is a displaced calcaneal tuberosity (beak) fracture on the lateral radiograph, the fragment is migrating proximally, and the skin over the posterior heel is white and blanched. How do you manage her?”
Key Concepts
- Calcaneal tuberosity = Achilles tendon insertion site
- Achilles avulsion = loss of plantarflexion power
- ORIF required if displaced (greater than 2mm)
- Tension band wiring preferred (converts tensile to compression)
Classification (Lee 2012)
- Type I: Simple extra-articular avulsion (sleeve) - elderly women, all fibres
- Type II: Beak fracture - often direct blow, all fibres, skin risk
- Type III: Infrabursal mid-third - superficial fibres (MRI)
- Type IV: Beak + superior triangular fragment - deep fibres (MRI)
- Key point: displacement (not type) predicts outcome (Carnero-Martin)
Treatment
- Non-displaced (rare): Conservative (cast, NWB 6-8 weeks)
- Displaced (most): ORIF with tension band wiring (80-90% good results)
- Large fragment: Screw fixation alternative (75-85% good results)
- Loss of plantarflexion: Absolute indication for ORIF
Surgical Technique
- Posterior approach: Midline or posterolateral, protect sural nerve
- Tension band: K-wires (2.0-2.5mm) + figure-8 wire (1.2-1.25mm)
- Wire anterior to K-wire axis (on tension side)
- Converts tensile force to compression
- Verify reduction fluoroscopically
Complications
- Sural nerve injury: 5-10% (prevent by protecting nerve)
- Equinus contracture: 10-15% if untreated (prevent with early ORIF)
- Loss of plantarflexion: 10-15% (prevent with anatomic reduction)
- Nonunion: 5-10% (prevent with rigid fixation)
- Hardware prominence: 20-30% (remove if symptomatic)
Evidence Base
Lee Classification of Calcaneal Tuberosity Avulsion
- Tuberosity fractures = 2.6% of calcaneal fractures
- Type I commonest, in elderly women
- Achilles fibre involvement varies by type
- MRI required to confirm types III and IV
Displacement Predicts Outcome (Prognostic Classification)
- Displacement magnitude drives complications and skin compromise
- Displacement of 2cm or more: complications rise from 30% to 91%
- Beavis classification NOT prognostic
- 62% complication, 38% secondary surgery rate
JAAOS Review: Skin and Gastroc-Soleus Are Key
- Most common in elderly and diabetic patients
- Displacement threatens posterior heel skin
- Stable fixation of the displaced fragment required
- Address gastroc-soleus tightness to improve outcome
Surgical Series: Screw vs Plate Fixation Outcomes
- 90% excellent/good, mean AOFAS 91.1
- Large fragments into subtalar joint: plate fixation
- Skin necrosis can require flap coverage
- Emergency ORIF when soft tissues compromised
Diabetic Insufficiency Avulsion: Suture-Anchor Technique
- Diabetic avulsions are often a Charcot event
- Poor bone defeats conventional screw fixation
- Fragment excision + double-row anchor reattachment
- AOFAS improved from 27 to 88 at one year
Contemporary Review: Anatomy, Classification and Fixation
- Skin/tendon risk tracks with Lee and Carnero-Martin types
- CT for bony detail; MRI for soft tissue
- Fixation must resist strong Achilles pull
- Multiple modern fixation constructs available