Sacral Agenesis and Caudal Dysgenesis
- Maternal diabetes is the strongest known risk factor for CRS.
- Renshaw classification (types I-IV) grades the amount of sacrum lost and predicts function.
- Spinopelvic instability and lumbosacral kyphosis are the major spinal problems.
- Neurological deficit is usually fixed and motor-predominant; watch for the rare progressive case.
- Neurogenic bladder/bowel drives long-term morbidity (renal damage).
- “Maternal diabetes association
- “Renshaw types I-IV
- “Buddha / cross-legged sitting posture
- “Spinopelvic fusion for unstable high types
CRS is the malformation most classically linked to maternal diabetes. In any neonate with absent/short sacrum, lower-limb wasting or a fixed "frog-leg" posture, ask about and document maternal glycaemic control. Conversely, infants of diabetic mothers warrant a careful spinal and lower-limb examination.
Most deficits are static, but a minority deteriorate. New or worsening weakness, sensory level or sphincter change suggests a treatable lesion (tethered cord, syrinx, anterior meningocele) - image the whole neuraxis with MRI rather than assuming the deficit is fixed.
- Problem
- High sacral loss - trunk not supported on pelvis
- Action
- Bracing then spinopelvic fusion (Renshaw III-IV)
- Problem
- Incontinence, reflux, renal damage
- Action
- Early urology, CIC, bowel programme
- Problem
- Hip/knee flexion, popliteal webbing, clubfoot
- Action
- Physiotherapy, selective soft-tissue surgery
- Problem
- Progressive deficit if present
- Action
- MRI neuraxis, neurosurgical referral
DIVACauses / Risk Factors - DIVA
Hook:A DIVA's diabetic mother - links the headline associations of CRS.
SPINEOrthopaedic Problems - SPINE
Hook:Think SPINE up then down - spine, posture, hip, nerves, feet.
IVRenshaw Types - Severity Climbs I to IV
Hook:Higher Roman numeral = more bone lost = less stable, less likely to walk.
Overview/Epidemiology
Caudal regression syndrome (CRS) - also called sacral agenesis or caudal dysgenesis - is a spectrum of congenital malformations caused by premature termination of development of the caudal (tail) end of the spine and cord.
- Spectrum: From isolated coccygeal absence, through partial and complete sacral agenesis, to the most severe extreme of sirenomelia (fused lower limbs).
- Prevalence: Rare, around 1 in 25,000 live births; markedly higher in pregnancies complicated by diabetes.
- Sex: Roughly equal overall, with a female excess in the Currarino subgroup.
- Cognition: Usually normal intelligence - the disability is musculoskeletal, neurological (below the lesion) and sphincteric.
According to PubMed, an orthopaedic narrative review by Jasiewicz and Kacki divides CRS into three broad groups (sirenomelia, complete sacral absence, and partial sacral absence) and identifies spinal deformity, spinopelvic instability and lower-limb deformity as the dominant orthopaedic problems (DOI).
Pathophysiology and Genetics
Embryology
- The caudal cell mass and secondary neurulation form the lower sacrum, coccyx and conus. An early insult (around weeks 3-7) disturbs caudal mesoderm and notochord, producing the bony and neural deficit together.
- Because the bone and the corresponding cord segments form together, the level of motor loss tends to mirror the level of bony absence.
Mechanisms (no single proven cause)
- Maternal diabetes / diabetic embryopathy: the strongest association; hyperglycaemia is teratogenic to the caudal mesoderm.
- Vascular hypoperfusion: a proposed "caudal steal" reducing blood flow to the developing caudal region (most invoked for sirenomelia).
- Genetic: the MNX1 (HLXB9) homeobox gene underlies Currarino syndrome (sacral agenesis + presacral mass + anorectal malformation) and familial sacral agenesis.
According to PubMed, Gajagowni et al. classify CRS as a recognised form of diabetic embryopathy, emphasising the link between maternal hyperglycaemia and caudal malformation (DOI). Dworschak et al. confirm MNX1 as the major causative gene in Currarino syndrome, mutated in roughly half of patients tested and most familial cases (DOI).
Classification Systems
Renshaw Classification of Sacral Agenesis
The most widely used orthopaedic system, based on the amount of sacrum present and the iliac-vertebral relationship.
- Type I: Partial unilateral sacral agenesis (hemisacrum) - normal or oblique lumbosacral junction.
- Type II: Partial bilateral (symmetric) sacral agenesis - a stable articulation between the lowest vertebra and the ilia (S1 usually present).
- Type III: Total sacral agenesis with variable lumbar loss - iliac wings articulate with the sides of the lowest present vertebra.
- Type IV: Total sacral and partial lumbar agenesis - the iliac wings are fused or approximated behind the caudal vertebra (most unstable).
Rule of thumb: Types I-II are typically stable (the spine sits on the pelvis); types III-IV are unstable and at risk of progressive kyphosis.
Sirenomelia: The Severe Extreme of the Spectrum
Sirenomelia is named repeatedly as the most severe end of the caudal spectrum, but never developed. It is worth knowing both as the conceptual extreme and because the relationship between sirenomelia and caudal regression syndrome is itself an exam point.
What it is. Sirenomelia (the "mermaid" malformation) is fusion of the lower limbs into a single midline lower extremity, with severe sacral/caudal agenesis. It sits at the extreme end of caudal dysgenesis but is distinguished from "ordinary" CRS by a near-constant cluster of lethal visceral anomalies:
- Sirenomelia
- Fused into a single midline limb (apus/unipus/dipus variants)
- Caudal regression (non-siren)
- Two separate limbs, variably wasted and contractured
- Sirenomelia
- Single large 'vitelline' artery steals flow from the aorta ('vascular steal') - the leading pathogenic theory
- Caudal regression (non-siren)
- Caudal mesoderm insult; vascular steal less central
- Sirenomelia
- Near-constant bilateral renal agenesis/dysgenesis → oligohydramnios, Potter sequence, pulmonary hypoplasia; imperforate anus, absent bladder
- Caudal regression (non-siren)
- Renal/anorectal anomalies common but not uniformly lethal
- Sirenomelia
- Usually fatal (the renal agenesis/pulmonary hypoplasia, not the limb fusion, kills) - survival is rare
- Caudal regression (non-siren)
- Compatible with life; normal cognition; long-term function depends on level
The exam point is the cause of death: a baby with sirenomelia dies not because the legs are fused but because of bilateral renal agenesis → oligohydramnios → Potter sequence and pulmonary hypoplasia. Whether sirenomelia is the same disease as CRS or a distinct "vascular steal" entity is debated, but for orthopaedic exams it is best framed as the lethal extreme of the same caudal spectrum, defined by limb fusion and incompatible visceral malformations.
If asked why sirenomelia is (almost always) fatal while the rest of the CRS spectrum is survivable, do not say "the fused legs". The answer is bilateral renal agenesis → oligohydramnios → Potter sequence with pulmonary hypoplasia. The single midline 'vitelline' artery stealing aortic flow is the favoured pathogenic mechanism.
Clinical Assessment
History
- Antenatal: maternal diabetes/glycaemic control, abnormal anomaly scan (absent distal vertebrae), oligohydramnios.
- Function: sitting balance, ability to stand/walk, ambulatory aids.
- Sphincters: urinary and faecal continence, recurrent urinary tract infection, constipation.
- Progression: any new weakness, sensory change or deterioration (red flag).
Examination
- Posture: characteristic cross-legged "Buddha" / frog-leg sitting posture; flattened buttocks with a short natal cleft.
- Spine: lumbosacral kyphosis, the palpable "step-off" of the deficient sacrum, scoliosis.
- Lower limbs: muscle wasting (calf/thigh), fixed hip and knee flexion contractures, popliteal webbing/pterygia, foot deformity.
- Neurology: a motor-predominant flaccid paraparesis with a clear motor level; sensation is often relatively preserved (a classic dissociation).
- Other systems: perineum/anus (imperforate or stenotic anus), abdomen (palpable bladder), associated VACTERL features.
Investigations
Imaging
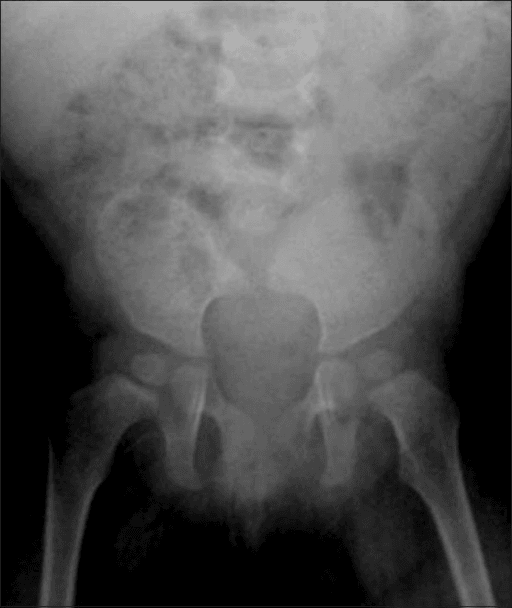
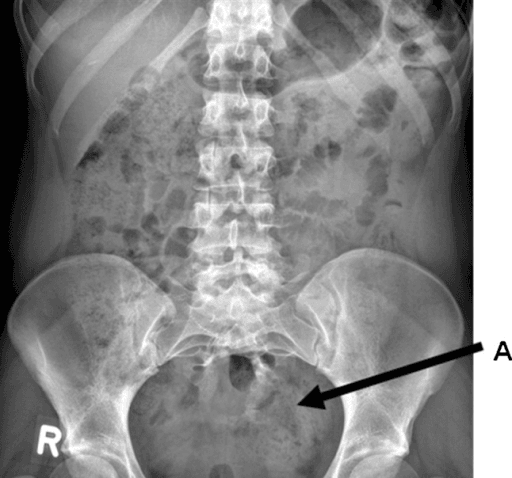
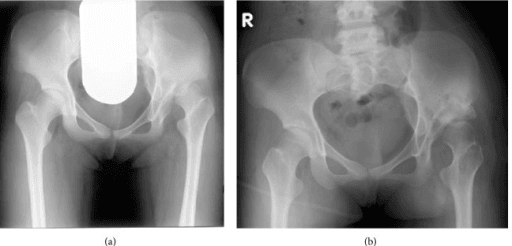
- Plain radiographs (AP/lateral whole spine + pelvis): define the last intact vertebra, the amount of sacrum present and the iliac articulation - the basis for Renshaw typing.
- MRI of the whole neuraxis: the key study - shows the conus level, tethered cord, syrinx, lipoma and any anterior sacral meningocele. Mandatory before surgery and for any progressive deficit.
- CT / 3D reconstruction: helpful for planning spinopelvic fixation in complex bony anatomy.
- Renal tract ultrasound +/- MCUG / urodynamics: assess the neurogenic bladder and upper tracts.
Other
- Genetic testing (MNX1) where Currarino syndrome or familial sacral agenesis is suspected.
- Maternal investigation for diabetes if not already known.
Differential Diagnosis
- Key Differentiator
- Absent sacrum/coccyx, motor-predominant deficit, maternal diabetes link
- Key Differentiator
- Open neural tube defect, sac on the back, hydrocephalus/Chiari II
- Key Differentiator
- Sickle sacrum + presacral mass + anorectal malformation (MNX1)
- Key Differentiator
- Vertebral, anal, cardiac, TE, renal, limb anomalies without the specific sacral-loss pattern
- Key Differentiator
- Fused lower limbs - the severe extreme of the caudal spectrum
- Key Differentiator
- Progressive deficit with a normal sacrum
Key distinguishing points
- CRS vs spina bifida: CRS is a deficiency of bone/cord (closed), not an open neural tube defect, and sensation is comparatively spared.
- CRS vs Currarino: Currarino has the specific triad and a stable scimitar sacrum rather than diffuse instability.
- Sirenomelia sits at the most severe end of the same caudal spectrum.
Management Algorithm
Overall Approach
- The bony defect is irreversible - the goal is to maximise function, stability and continence, not to restore normal anatomy.
- Multidisciplinary: orthopaedics, neurosurgery, urology, colorectal/paediatric surgery, rehabilitation.
- Sequence: stabilise life-threatening associations first (cardiac, renal, anorectal), then address spine stability, then limb function.
Anterior Sacral Meningocele
The anterior sacral meningocele is flagged in the complications table, the Currarino discussion and an unanswered viva follow-up ("What are the risks of an anterior sacral meningocele?"), so it deserves to be developed. It is the most dangerous of the Currarino presacral masses.
What it is. An anterior sacral meningocele is a herniation of the dural sac through the defect in the deficient anterior sacrum into the presacral (retroperitoneal) space - a CSF-filled diverticulum sitting in front of the sacrum, classically through the "scimitar/sickle" sacral defect of Currarino syndrome. It communicates with the thecal sac through a narrow neck.
Because an anterior sacral meningocele communicates directly with the CSF, trans-rectal or trans-vaginal aspiration or biopsy can seed organisms into the subarachnoid space and cause fatal meningitis. Any presacral mass in a patient with sacral agenesis must be imaged (MRI) to define a CSF communication BEFORE anyone considers a needle - the diagnosis is made by imaging, not by aspiration.
Why it matters / its risks:
- Mechanism
- Direct CSF communication with the rectum (via fistula or after ill-advised aspiration) seeds the subarachnoid space
- Mechanism
- Straining transmits pressure into the CSF-filled sac (a classic symptom)
- Mechanism
- A large presacral CSF sac is a space-occupying pelvic mass
- Mechanism
- The Currarino presacral mass may be mixed (meningocele plus teratoma); the solid element can undergo malignant transformation
Management is neurosurgical: definitive repair is closure of the dural neck (commonly via a posterior trans-sacral or, in selected cases, anterior/laparoscopic approach) to obliterate the communication and decompress the sac, with excision of any associated solid teratomatous component. The classic teaching point that "a presacral mass needs excision" specifically includes securely closing the CSF communication of a meningocele, not simply debulking it.
When a child with a scimitar (Currarino) sacrum has a presacral mass, the single highest-yield safety point is: MRI first, never a trans-rectal/trans-vaginal biopsy or aspiration - an anterior sacral meningocele communicates with the CSF, so needling it risks fatal meningitis. Definitive treatment is surgical closure of the dural neck (plus excision of any teratomatous element).
Surgical Techniques
Spinopelvic Fusion / Stabilisation
Indications: Renshaw III-IV with an unstable, kyphotic lumbosacral junction; an unsupported trunk preventing sitting.
Technique: Posterior multilevel pedicular screw fixation extended to pelvic fixation (iliac/S2-alar-iliac type anchorage). The deficient sacrum is bypassed by anchoring the construct to the ilia, and a structural bone graft/allograft block is used to reconstruct the lumbopelvic junction and sagittal alignment.
Goal: solid fusion of the lumbopelvic segment to give a stable base for sitting and standing.
Complications
Spinal and Neurological
- Pattern
- High (III-IV) types
- Management
- Bracing, spinopelvic fusion
- Pattern
- Causes deterioration
- Management
- MRI surveillance, neurosurgical release
- Pattern
- Currarino subset
- Management
- Neurosurgical repair
- Pattern
- Minority of cases
- Management
- Image neuraxis, treat the lesion
Orthopaedic
- Pattern
- Common
- Management
- Selective reconstruction; supple hip for sitting
- Pattern
- Limits positioning
- Management
- Casting, soft-tissue release
- Pattern
- Common
- Management
- Ponseti, releases, orthoses
- Pattern
- Insensate skin, sitting
- Management
- Pressure care, seating review
Systemic
- Reflux nephropathy / renal failure from an untreated neurogenic bladder - the leading long-term threat to life.
- Recurrent urinary and respiratory infection, faecal incontinence.
- Presacral mass complications (meningitis, malignant change) in Currarino syndrome.
Postoperative Care and Rehabilitation
After Spinopelvic Fusion
- Early: meticulous pressure care over insensate skin; vigilant wound surveillance (high infection risk).
- Mobilisation: graded sitting/standing once the construct allows; custom seating to protect skin and support the trunk.
- Monitoring: serial imaging for fusion and implant integrity; watch for pseudarthrosis and revision needs.
Lifelong Multidisciplinary Follow-Up
- Urology: ongoing bladder management and renal tract surveillance.
- Rehabilitation: bracing, wheelchair/seating, transfers and independence training.
- Neurosurgery: monitor for tethered-cord/syrinx-related deterioration.
- Psychosocial: support for the child and family; intelligence is typically normal so cognitive expectations are unchanged.
Outcomes/Prognosis
What Determines Function
- Bony level / Renshaw type is the key predictor: lower types (I-II) and a lower neurological level favour community ambulation; high types (III-IV) more often become wheelchair/seating dependent.
- Last intact motor level governs walking potential much as in spina bifida.
- Renal preservation is the main determinant of long-term survival.
According to PubMed, Vissarionov et al. reported spinopelvic fusion in 12 children with CRS: a 100% fusion rate with restored sagittal alignment that allowed mobilisation and standing in type III patients (5 complications requiring further care), demonstrating that reconstruction can convert an unstable trunk into a stable, functional base (DOI).
Quality of Life
- Most children have normal cognition and can achieve schooling, employment and independence with appropriate support.
- Continence and skin integrity, rather than walking alone, dominate day-to-day quality of life.
Guidelines, Registries & Global Practice
Global Epidemiology
- CRS is rare (around 1 in 25,000 live births) but its incidence rises many-fold in diabetic pregnancies, making it a sentinel marker of diabetic embryopathy worldwide.
- The spectrum runs from isolated coccygeal absence to sirenomelia; partial sacral agenesis is commoner than complete.
- The Currarino subset shows a slight female predominance and autosomal dominant inheritance via MNX1.
Side-by-Side Guidance
- Emphasis
- Pre-conception and first-trimester glycaemic optimisation is the principal modifiable factor; anomaly scanning detects absent distal vertebrae
- Emphasis
- Renshaw/Pang typing guides bracing vs spinopelvic fusion; image the neuraxis before deformity surgery
- Emphasis
- Early CIC, anticholinergics and upper-tract surveillance to prevent reflux nephropathy
- Emphasis
- MNX1 testing and family screening in Currarino syndrome / familial sacral agenesis
Practice Variation
- High-resource settings: multidisciplinary clinics (orthopaedics, neurosurgery, urology, colorectal, rehabilitation), MRI neuraxis screening and spinopelvic reconstruction available.
- Limited-resource settings: diagnosis is clinical/radiographic; care prioritises continence, renal protection and seating, with referral for the rare progressive neurological case.
- Because the lesion is fixed, prevention through maternal diabetes control offers the greatest public-health impact globally.
Controversies and Areas of Uncertainty
Static versus progressive deficit Historically all deficits were assumed fixed, leading to a purely orthopaedic, "wait-and-watch" stance. Pang and Hoffman showed a treatable progressive subgroup; the modern debate is how aggressively to image and intervene for subtle deterioration versus accepting a stable baseline.
Hip reduction in non-ambulators Whether to reduce a dislocated hip in a child who will not walk is contested. Many favour a supple, pain-free hip for sitting over forced reduction, which can stiffen the hip and worsen seating.
Timing and extent of spinopelvic fusion The threshold for fusing an unstable high-type spine - and how early to do it in a growing child - is not standardised; surgeons balance sitting stability against growth, infection risk over insensate skin, and revision burden.
MCQ Practice Points
Q: What is the strongest known maternal risk factor for caudal regression syndrome? A: Maternal diabetes mellitus (diabetic embryopathy).
Q: Which classification grades sacral agenesis by the amount of sacrum present and the iliac-vertebral relationship? A: The Renshaw classification (types I-IV), modified by Pang.
Q: Which Renshaw types are typically unstable and at risk of progressive kyphosis? A: Types III and IV (total sacral agenesis) - candidates for spinopelvic fusion.
Q: What is the characteristic neurological dissociation in CRS? A: Motor-predominant flaccid paraparesis with relatively preserved sensation.
Q: Name the Currarino triad and its gene. A: Sacral agenesis + presacral mass + anorectal malformation, caused by MNX1 (HLXB9).
Q: What is the leading long-term threat to life in CRS? A: Renal failure from an untreated neurogenic bladder (reflux nephropathy).
Self-Assessment Quiz
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A neonate born to a poorly controlled diabetic mother has wasted lower limbs, a fixed frog-leg posture and a short natal cleft. What is your approach?”
“A 4-year-old with total sacral agenesis (Renshaw IV) cannot sit unsupported - the trunk collapses on the pelvis with a progressive lumbosacral kyphosis. What can you offer?”
“A child investigated for chronic constipation and anorectal stenosis is found to have a sickle-shaped (scimitar) sacrum on radiograph. What unifying diagnosis and what must you exclude?”
DEFINITION
- Sacral agenesis / caudal dysgenesis
- Failed caudal embryo development
- Spectrum to sirenomelia
- Normal intelligence
AETIOLOGY
- Maternal diabetes (strongest)
- Vascular hypoperfusion
- MNX1 (Currarino)
- VACTERL overlap
CLASSIFICATION
- Renshaw I-IV
- I-II usually stable
- III-IV unstable
- Pang modification
NEUROLOGY
- Motor-predominant deficit
- Sensation often preserved
- Watch for progression
- Tethered cord / syrinx
ORTHOPAEDIC
- Spinopelvic instability
- Lumbosacral kyphosis
- Hip/knee contractures
- Clubfoot, popliteal web
MANAGEMENT
- Multidisciplinary, supportive
- Spinopelvic fusion (III-IV)
- Neurogenic bladder/bowel care
- Excise presacral mass (Currarino)
Evidence Base
- Reviews caudal regression / sacral agenesis as a recognised diabetic embryopathy
- Maternal hyperglycaemia is teratogenic to the developing caudal mesoderm
- Multisystem (renal, anorectal, neurological) associations parallel lesion severity
- MNX1 is the major causative gene in Currarino syndrome
- MNX1 mutation found in ~57% of CS patients tested (most familial, fewer sporadic)
- Slight female predominance (female:male ~1.39:1)
- Autosomal dominant family with hereditary sacral agenesis (10 affected members)
- Four had presacral teratoma/anterior meningocele; three suffered serious complications (meningitis, recurrence, sepsis)
- Several presented initially with anorectal anomalies