Axial Neck Pain | Diagnosis by Blockade | Radiofrequency Ablation Treatment
- Facet joints (Z-joints) are the most common source of chronic neck pain after whiplash.
- Pain is typically AXIAL and NON-RADICULAR (Referral zones exist but do not follow dermatomes).
- Degenerative changes on X-ray/CT do NOT correlate well with pain (False positives common).
- Diagnosis CANNOT be made by history/exam alone - requires Diagnostic Blocks (MBB).
- Treatment of choice for confirmed cases is Radiofrequency Neurotomy (RFA).
- “C2/3 Facet refers pain to the Occiput (Cervicogenic Headache).
- “C5/6 Facet refers pain to the shoulder/scapula.
- “Pain is worse with Extension and Rotation (Loading the facet).
- “Single uncontrolled block has a high false-positive rate (around 27%) - hence double blocking is the Gold Standard.
Treat the patient, not the scan. Severe OA on X-ray does NOT mean the joint is painful. Normal joints CAN be painful (post-whiplash).
Rule out radiculopathy. If arm pain exceeds neck pain or a neuro deficit is present, the Nerve Root is the suspect, not the Facet.
False-positive rate of a single block is about 27% (placebo, systemic spread). Sedation invalidates results. A Pain Diary is essential.
Overview & Epidemiology
Definition: Pain arising from the cervical zygapophysial (facet) joints, typically axial and non-radicular. Diagnosis is made by response to controlled medial branch blocks, not by imaging.
Epidemiology
- Most common identifiable source of chronic neck pain after whiplash (around 60% of cases; Lord 1996).
- C2/3 and C5/6 are the most frequently involved levels.
- Female predominance; onset often delayed 24-48 hours after a motor-vehicle deceleration injury.
- Neck pain overall is a leading global cause of years lived with disability.
Why it matters: Degenerative facet change on imaging is near-universal with age and correlates poorly with pain, so a structured block-based pathway is essential before committing to ablation.
Pathophysiology and Mechanisms
Facet Joint Structure
- Synovial joint.
- Oriented at 45 degrees in the coronal plane.
- Resists anterior translation and rotation.
Innervation (Crucial for RFA)
- Each joint is innervated by the Medial Branch of the dorsal ramus.
- Dual Innervation: Each joint receives branches from the level above and the same level.
- Example: C4/5 joint is supplied by C4 and C5 medial branches.
- Exception: C2/3 joint is supplied by the Third Occipital Nerve (TON) and C2 medial branch.
Pain Referral Patterns (Bogduk Maps)
- C2/3: Occiput, Mastoid (Headache).
- C3/4: Upper neck.
- C5/6: Lower neck, Trapezius ridge, Acromion.
- C6/7: Scapula border.
Classification Systems
IASP / Bogduk Diagnostic Criteria
Classification relies on response to diagnostic blocks, not imaging.
- Possible Facet Pain: History and Exam suggestive. Imaging shows OA.
- Probable Facet Pain: Greater than 80% relief from a SINGLE Medial Branch Block (MBB).
- Definite Facet Pain: Greater than 80% relief from TWO comparative blocks (e.g. Lignocaine then Bupivacaine) on different occasions.
Whiplash-Associated Disorders (Quebec Classification)
Facet pain is repeatedly framed here as the commonest source of chronic pain after whiplash, and the WAD mnemonic appears above — but the grading examiners expect, the Quebec Task Force classification of Whiplash-Associated Disorders (Spitzer et al, 1995), is worth stating explicitly because it drives triage and prognosis.
- Neck complaint
- None
- Findings
- No neck complaint and no physical signs
- Neck complaint
- Pain, stiffness or tenderness only
- Findings
- No physical (musculoskeletal or neurological) signs
- Neck complaint
- Neck complaint
- Findings
- Musculoskeletal signs: reduced range of motion and point tenderness
- Neck complaint
- Neck complaint
- Findings
- Neurological signs: reduced or absent reflexes, weakness, sensory deficit
- Neck complaint
- Neck complaint
- Findings
- Fracture or dislocation
- Symptoms such as headache, dizziness, tinnitus, dysphagia, temporomandibular pain and memory disturbance may accompany any grade and are not themselves graded.
- The vast majority of presentations are Grade I to II; Grade IV (fracture/dislocation) mandates immobilisation and the cervical-fracture pathway, not a pain-block pathway.
- The classification matters for selection: facet-mediated pain and the medial-branch-block pathway are relevant to persistent Grade I-II pain, whereas Grade III (true neurological signs) should redirect you to radiculopathy/myelopathy work-up rather than facet blocks.
A Grade III WAD (genuine neurological deficit) is not a facet-block candidate — neurological signs point to the nerve root or cord. Facet arthropathy is an axial, non-radicular, Grade I-II problem. Conflating the two is a classic trap.
Clinical Assessment
History
- "Deep, aching, dull" pain.
- Worsened by looking up (hanging washing) or turning head (reverse parking).
- Morning stiffness common.
- History of MVA (Whiplash).
Examination
- Inspection: Normal alignment or mild torticollis.
- ROM: Restricted Extension and Rotation.
- Palpation: Paraspinal Tenderness over the facet line (2cm from midline). Deep pressure reproducing "the pain".
- Neurology: Must be NORMAL.
- Provocative Test: Extension + Rotation to the affected side ("Closing the door" on the facet).
Imaging and Investigations
Workup Protocol
- AP/Lat/Oblique.
- Look for: Joint space narrowing, sclerosis, osteophytes.
- "Shingle Sign": Visualizes facet alignment on lateral view.
- More sensitive for OA.
- Rule out fracture or lysis.
- Note: OA presence does NOT confirm pain source.
- Medial Branch Block (MBB).
- Injection of local anesthetic (Lignocaine/Bupivacaine) onto the nerve supply.
- Diagnostic Criteria: Greater than 80% pain relief for the duration of the anesthetic.

Non-Operative Management
Physical Therapy
- Multimodal: Isometric strengthening, ROM, Scapular stabilization.
- Ergonomics: Workstation setup (monitor height).
- Psychology: CBT for chronic pain.
Medications
- NSAIDs.
- Neuropathic agents (Gabapentin/Pregabalin) - questionable efficacy for pure facet pain.
Management Algorithm
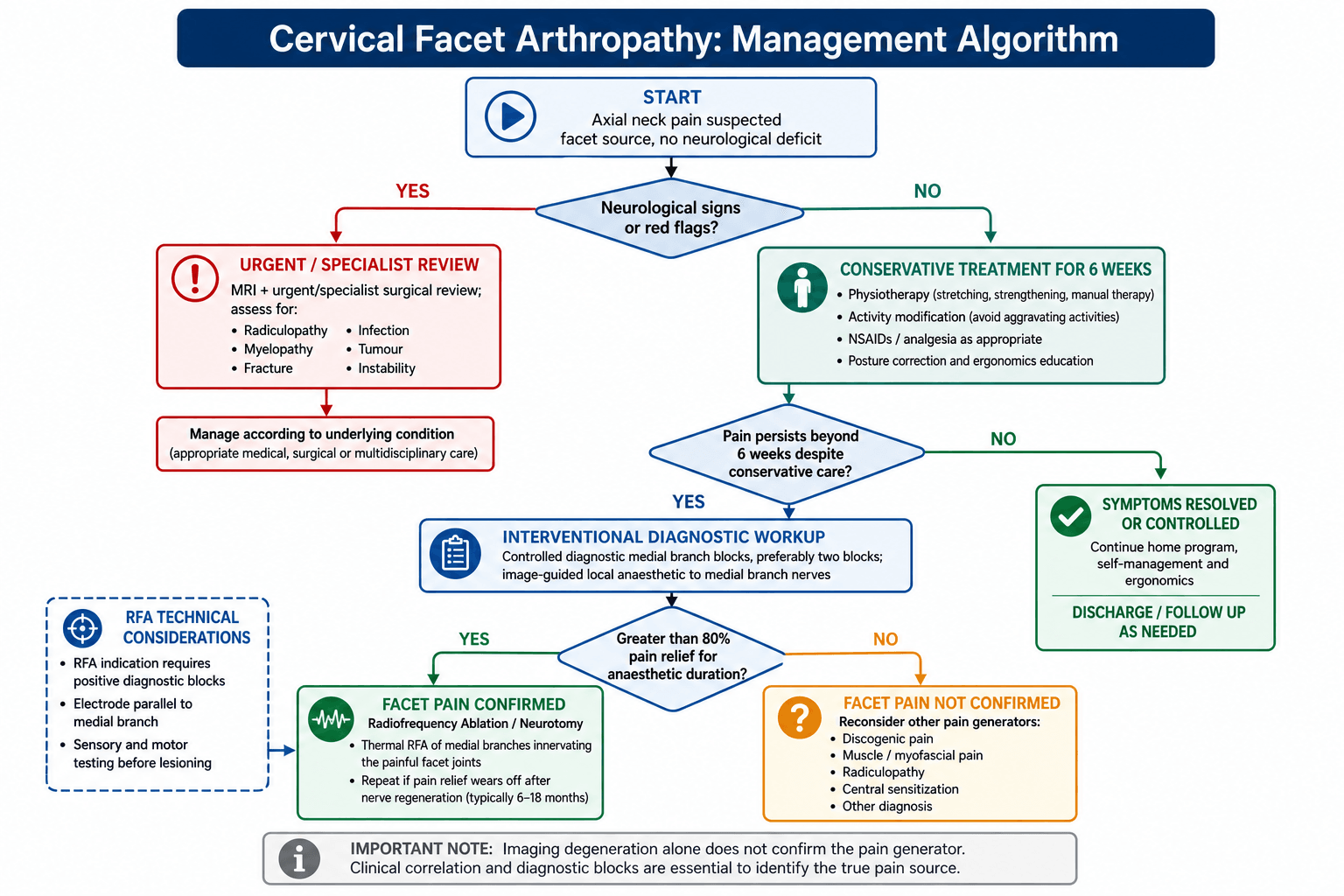
- 1
Axial Neck Pain (No Neuro)
- 2
Pain Persists > 6w?
- 3
Block Response (> 80% Relief)
Surgical Technique
Radiofrequency Neurotomy (RFA)
- Indication: Positive response to TWO diagnostic blocks.
- Goal: Thermal coagulation of the medial branch nerve to interrupt pain signals.
- Mechanism: Heat (80-90°C) creates a lesion.
Technique:
- Placement: Electrode placed Parallel to the nerve (along the waist of the articular pillar).
- Why Parallel?: Electricity flows sideways. Placing the needle perpendicular ("Gun barrel") creates a smaller lesion and might miss the nerve.
- Testing:
- Sensory: 50Hz (Patient feels buzzing in neck).
- Motor: 2Hz (Look for multifidus twitch). Absence of arm twitch is critical (Rule out root stimulation).
- Lesioning: 90 seconds @ 80°C. Multiple lesions per nerve.
Outcomes:
- 60-80% of patients get relief.
- Duration: 9-12 months (nerve regenerates).
- Can be repeated.
Pulsed vs Conventional (Thermal) Radiofrequency
The viva section above offers "pulsed or thermal RFA of the TON," but only conventional thermal RF is described elsewhere. These are two distinct modalities and the distinction is examinable.
- Conventional / continuous thermal RF
- Continuous
- Pulsed RF (PRF)
- Brief pulses with silent phases that let heat wash out
- Conventional / continuous thermal RF
- About 80 to 90 degrees C
- Pulsed RF (PRF)
- Kept at or below 42 degrees C (below the neurodestructive threshold)
- Conventional / continuous thermal RF
- Thermal coagulation / ablation (neurodestructive)
- Pulsed RF (PRF)
- Neuromodulatory, non- or minimally destructive
- Conventional / continuous thermal RF
- Best supported (Lord NEJM RCT and outcome studies)
- Pulsed RF (PRF)
- Weaker and less durable evidence; not equivalent
- Conventional thermal RF destroys the medial branch by heat coagulation; it is the modality validated by the Lord NEJM trial and the basis of the durable relief quoted above.
- Pulsed RF exposes the nerve to a rapidly fluctuating electric field while keeping the tissue cool, so it does not coagulate the nerve. It is proposed where a destructive lesion is undesirable, but its evidence for facet-mediated neck pain is weaker than thermal RF.
- Third occipital nerve (TON): TON neurotomy is technically harder (larger, more variable nerve over the C2/3 joint) and thermal lesioning predictably causes temporary cutaneous numbness and transient unsteadiness/ataxia in the treated territory; this side-effect profile is part of why pulsed RF is sometimes considered there, though thermal neurotomy remains the better-evidenced option.
Conventional thermal RF (80 to 90 degrees C, neurodestructive) is the evidence-based treatment for confirmed cervical facet pain. Pulsed RF (kept at or below 42 degrees C, non-destructive, neuromodulatory) is a lower-evidence alternative — do not present it as equivalent to thermal neurotomy.
Complications
- Risk
- Common (5%)
- Note
- Burning pain (Sunburn feeling). Self-limiting (2-4 weeks).
- Risk
- Rare
- Note
- Drift of needle anteriorly hitting the Nerve Root. Avoid by Motor Testing.
- Risk
- Very Rare
- Note
- Epidural abscess.
- Risk
- 20-30%
- Note
- Technical failure or Incorrect diagnosis (False pos block).
Postoperative Care
- Post-RFA:
- Ice packs for sore neck.
- Resume normal activity immediately.
- Physio to capitalize on the "Pain-free window".
Outcomes and Prognosis
- Natural History: Recurrent/Relapsing course.
- RFA Efficacy: The Lord 1996 NEJM RCT showed median relief of 263 days (vs 8 days for sham).
- Whiplash: Poorer prognosis if litigation ongoing, high baseline pain, or Catastrophizing.
Guidelines, Registries & Global Practice
Global Epidemiology
- Neck pain is among the leading global causes of years lived with disability (Global Burden of Disease).
- After whiplash, cervical facet joints are the most common identifiable pain source (around 60% of chronic cases; C2/3 and C5/6 most frequent).
- Female predominance; recovery is strongly modulated by psychosocial factors and the local compensation environment.
- Diagnostic Blocks
- Not recommended as routine for non-specific neck pain
- RFA Position
- RFA not recommended outside research for axial neck pain
- Diagnostic Blocks
- Two controlled (comparative or placebo) blocks required
- RFA Position
- RFA endorsed in rigorously selected, block-positive patients
- Diagnostic Blocks
- Controlled blocks to confirm before ablation
- RFA Position
- RFA an option after positive controlled blocks
- Diagnostic Blocks
- Comparative blocks favoured; placebo control debated
- RFA Position
- RFA accepted for confirmed facet pain
Practice Variation (high- vs limited-resource)
- High-resource settings: fluoroscopy- or CT-guided diagnostic blocks and RFA are routine in pain/spine services.
- Limited-resource settings: image-guided blocks and RFA equipment may be unavailable; care relies on physiotherapy, analgesia and activity modification, with surgical fusion reserved for instability or deformity.
- The major payer/policy divergence is whether controlled blocks are mandated before RFA (SIS/ASRA, NASS) or whether the whole pathway is restricted (NICE).
Controversies & Areas of Uncertainty
- Placebo vs comparative blocks: Comparative blocks (two anaesthetics) still carry residual false positives; only placebo-controlled triple blocks fully exclude placebo, but these are impractical in routine care.
- NICE vs interventionalist societies: NICE restricts diagnostic blocks and RFA for non-specific neck pain, citing weak trial evidence, whereas SIS/ASRA/NASS support RFA when strict block-based selection is applied. The conflict largely reflects how patients are selected.
- Imaging-pain mismatch: Degenerative facet changes on CT/MRI correlate poorly with the pain source, so imaging cannot confirm or exclude the diagnosis.
- Durability and repetition: Relief is finite because the medial branch regenerates; the optimal re-treatment interval and long-term effect on adjacent-segment health remain undefined.
- Whiplash chronicity: Cross-jurisdiction differences in chronicity highlight the contribution of psychosocial and compensation factors rather than a purely structural cause.
Mnemonics
FACETFacet Features
Hook:Key clinical features.
SAME + ABOVEInnervation Rule
Hook:Each joint has dual innervation. (e.g. C5/6 joint is supplied by C5 and C6 medial branches).
WADWhiplash Rule
Hook:Epidemiology of facet trauma.
MCQ Practice Points
Q: What is the false positive rate of a single uncontrolled medial branch block? A: About 27% (Barnsley 1993, 95% CI 15-38%). This is why dual blocks are required for definitive diagnosis.
Q: The C5/6 facet joint is innervated by which nerves? A: C5 and C6 medial branches. (Same level and level above).
Q: For maximum efficacy, how should the RFA electrode be placed relative to the nerve? A: Parallel. This maximizes the length of nerve captured in the thermal lesion.
Q: Which movement typically aggravates facet joint pain? A: Extension and Rotation. This mechanially loads the joint.
Q: What is the most common side effect of RFA? A: Post-neurotomy Neuritis (Sunburn sensation). Occurs in 5% of patients.
At a Glance
- Facet Joint (Z-Joint)
- Neck (Axial)
- Discogenic Pain
- Neck (Axial)
- Radiculopathy
- Arm (Radicular)
- Facet Joint (Z-Joint)
- Extension / Rotation
- Discogenic Pain
- Flexion / Loading
- Radiculopathy
- Extension / Spurling's
- Facet Joint (Z-Joint)
- Somatic (Head/Scapula)
- Discogenic Pain
- Somatic (Interscapular)
- Radiculopathy
- Dermatomal (Hand)
- Facet Joint (Z-Joint)
- None
- Discogenic Pain
- None
- Radiculopathy
- Motor/Sensory Loss
Exam Day Cheat Sheet
Key Concepts
- Axial Pain (No Radiculopathy)
- Extension Loading pattern
- MBB is gold standard diagnosis
- Double block required
Anatomy
- Dual Innervation (Same + Above)
- C2/3 = Headache (TON)
- C5/6 = Shoulder
- Facet angles 45 deg
Treatment
- Conservative first
- RFA (Parallel placement)
- Success = 9-12 months relief
- No Fusion
- Sensory + Motor Testing
Stats
- 60% of chronic post-whiplash neck pain
- 27% False-Positive Rate (Single Block)
- 54-55% in comparative-block series
- Female predominance
Image Manifest
- [1-preoperative-image-a-plain-radiograph-lateral-imag.png]: Lateral X-ray showing facet sclerosis
- [5-plain-radiographs-of-a-57-year-old-man-a-lateral-i.png]: Lateral spondylosis
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“45F, MVA 6 months ago. Chronic neck pain, worse looking up. MRI shows some degeneration C5/6. Physio failed. What is your approach?”
“A patient complains of unilateral occipital headaches radiating from the neck. Worse with neck rotation. Which joint is culpable?”
“You are performing cervical medial branch radiofrequency neurotomy. How do you position the electrode, why, and how do you confirm safe placement before lesioning?”
Evidence Base
Prevalence of Cervical Facet Pain after Whiplash
- Placebo-controlled local anaesthetic blocks in 68 chronic post-whiplash neck-pain patients.
- Overall prevalence of cervical zygapophysial joint pain (C2/3 or below) was 60% (95% CI 46-73%).
- C2/3 joint pain prevalence was 50% in patients with dominant headache.
- Diagnosis survived placebo challenge, confirming it is a genuine clinical entity.
Prevalence by Comparative Blocks
- Double-blind comparative blocks (lignocaine vs bupivacaine) in 50 chronic post-whiplash patients.
- Painful zygapophysial joints identified in 54% (95% CI 40-68%).
- Established the comparative-block paradigm prior to the later placebo-controlled study.
- Cervical facet pain was the most common source in this population.
Landmark RCT: Radiofrequency Neurotomy
- 24 patients with block-confirmed facet pain randomised to active RFA (80 degrees C, multiple lesions) vs sham.
- Median time to return of 50% pain was 263 days (active) vs 8 days (sham), p=0.04.
- At 27 weeks 7/12 active patients were pain-free vs 1/12 sham.
- Numbness in the treated nerve territory occurred but was not troubling to patients.
Effectiveness in Practice
- 104 patients selected by controlled diagnostic blocks, treated by ISIS-trained operators.
- Successful outcome (complete or at least 80% relief, restored ADLs) in 61-74% across two practices.
- Median duration of relief allowing for repeat treatment was 20-26 months.
- Demonstrates real-world reproducibility when rigorous technique and selection are used.
Third Occipital Nerve Headache
- C2/3 (third occipital nerve) headache prevalence was 27% across all whiplash patients.
- In patients with dominant headache the prevalence rose to 53%.
- No history or examination feature reliably predicted the diagnosis before nerve blocks.
- Tenderness over the C2/3 joint was significantly associated with a positive diagnosis.
Radiofrequency Lesion Geometry
- Photographic temperature mapping shows RF lesions extend radially around the electrode tip, not beyond it.
- Lesion grows along the active tip, so electrodes laid parallel to the nerve capture a longer segment.
- A perpendicular tip risks the nerve slipping past the narrow lesion edge.
- Larger tips, higher tip temperature and longer lesion times enlarge the lesion.
False-Positive Rate of Single Blocks
- Single uncontrolled blocks compared against a double-blind comparative-block reference standard.
- False-positive rate of single blocks was 27% (16 of 60 joints; 95% CI 15-38%).
- Causes: placebo response, systemic absorption and spread to adjacent structures.
- Uncontrolled blocks have substantially reduced specificity.