Craniocervical and Subaxial Instability
- ADI (Atlantodental Interval): Normal is less than 3mm adults, less than 5mm children.
- PADI (Posterior ADI): Less than 14mm indicates cord compromise risk.
- Powers Ratio: Ratio greater than 1 indicates anterior OC-C1 dislocation.
- White-Panjabi Criteria: Score of 5 or greater indicates subaxial instability.
- RA patients: Must screen for AAI before anesthesia/intubation.
- “ADI greater than 3mm in adults is abnormal
- “PADI less than 14mm predicts poor neurological outcome
- “Powers ratio: BC/OA (greater than 1 = anterior dislocation)
- “Always screen RA and Down syndrome patients
- “Harms technique: C1 lateral mass + C2 pedicle screws
Adult: less than 3mm is Normal. Child: less than 5mm is Normal. Reflects transverse ligament integrity.
less than 14mm: Critical threshold for cord compromise. PADI is more prognostic than ADI.
Powers Ratio greater than 1: Anterior dislocation. BDI greater than 12mm: Abnormal Basion-Dens Interval.
Translation: greater than 3.5mm. Angulation: greater than 11 degrees. (White-Panjabi Criteria)
Overview/Epidemiology
Cervical instability is defined as abnormal motion of the cervical spine that results in neurological compromise, incapacitating pain, or structural deformity under physiological loads.
- Trauma: Most common cause overall - MVA, falls, sports
- Rheumatoid arthritis: 25-80% develop AAI over disease course
- Down syndrome: 15-20% have AAI on screening radiographs
- Congenital: Os odontoideum, basilar invagination, occipitalization of C1
- Tumors/Infections: Destabilize through bone destruction
- OC-C1 dislocation has 70% pre-hospital mortality
- Untreated AAI can progress to myelopathy and quadriplegia
- Early recognition and stabilization prevents neurological decline
Anatomy
Upper Cervical Anatomy (OC-C1-C2):
Bony Structures:
- Occiput: Occipital condyles articulate with C1 lateral masses
- Atlas (C1): Ring-shaped, no vertebral body, lateral mass articulations
- Axis (C2): Odontoid process (dens) is the pivot for rotation
- C1-C2 articulation: Allows 50% of cervical rotation
Ligamentous Stabilizers:
- Transverse ligament: Primary restraint to anterior C1 translation
- Alar ligaments: Limit rotation and lateral bending
- Apical ligament: Connects dens tip to basion
- Tectorial membrane: Extension of PLL, covers dens posteriorly
- Cruciate ligament: Transverse + vertical bands
Subaxial Anatomy (C3-C7):
Stabilizing Structures:
- Anterior: ALL, disc, vertebral body
- Middle: PLL, posterior disc, posterior body
- Posterior: Facet capsules, ligamentum flavum, interspinous ligaments
Denis Three-Column Model applies but White-Panjabi criteria more specific for cervical.
Pathophysiology
Traumatic Instability
Mechanism:
- High-energy trauma causes ligamentous disruption or fracture
- Flexion-distraction injuries disrupt posterior ligaments
- Extension injuries disrupt anterior structures
- Rotation and lateral bending cause facet injuries
Patterns:
- OC-C1 dislocation: Usually fatal; survivors have tectorial membrane disruption
- Odontoid fractures: Type II most common, highest nonunion rate
- Hangman's fracture: Bilateral C2 pars fracture
- Facet dislocations: Unilateral (25% subluxation) or bilateral (50% subluxation)
Neurological Compromise Mechanism:
The spinal cord at C1-C2 level is approximately 10mm in diameter. The canal normally provides approximately 20mm of space.
Steel's Rule of Thirds at C1:
- 1/3 dens
- 1/3 cord
- 1/3 space (buffer)
When PADI (space available for cord) drops below 14mm, cord compression becomes likely. Myelopathy results from:
- Direct mechanical compression
- Vascular compromise (anterior spinal artery)
- Dynamic cord impingement with flexion/extension
Classification
Upper Cervical Instability (OC-C1-C2)
- Type I: Anterior dislocation (most common in survivors)
- Type II: Longitudinal distraction
- Type III: Posterior dislocation
- Anterior subluxation: ADI greater than 3mm (most common)
- Posterior subluxation: Rare, associated with dens fracture
- Rotatory subluxation: Fielding-Hawkins Types I-IV
- Lateral translation: Associated with Jefferson fracture
- Type I: Rotatory fixation without anterior shift
- Type II: Rotatory fixation with 3-5mm anterior shift
- Type III: Rotatory fixation with greater than 5mm shift
- Type IV: Rotatory fixation with posterior shift
Clinical Presentation
History:
- Mechanism of injury (trauma)
- Neck pain, especially with motion
- Myelopathic symptoms: weakness, numbness, gait disturbance
- Electric shock sensation with flexion (Lhermitte's sign)
- History of RA, Down syndrome, or connective tissue disorder
Neurological Assessment
- Hyperreflexia
- Hoffmann sign positive
- Ankle clonus
- Babinski sign positive
- Spastic gait
- Inverted radial reflex
- Test all myotomes C5-T1
- Assess grip strength
- Intrinsic hand muscle wasting
- Dermatomal assessment
- Proprioception (posterior columns)
- Cape-like sensory loss (central cord)
- Spastic, wide-based
- Difficulty with tandem walking
Investigations
Plain Radiographs
Standard Views:
- AP, lateral, open mouth odontoid
- Flexion-extension laterals (supervised, if neurologically intact)
Key Measurements:
- Normal
- Less than 3mm
- Abnormal
- Greater than 3mm
- Normal
- Less than 5mm
- Abnormal
- Greater than 5mm
- Normal
- Greater than 14mm
- Abnormal
- Less than 14mm
- Normal
- Less than 1
- Abnormal
- Greater than 1
- Normal
- Less than 12mm
- Abnormal
- Greater than 12mm
- Normal
- Less than 12mm
- Abnormal
- Greater than 12mm
Powers Ratio (BC/OA):
- BC = basion to posterior C1 arch
- OA = opisthion to anterior C1 arch
- Greater than 1 = anterior OC-C1 dislocation
- Less than 0.7 = posterior dislocation
Flexion-extension views are essential but should only be done with supervision if patient is neurologically intact.
The Cervical Spine Stretch Test
The White-Panjabi checklist assigns 2 points for a positive stretch test, yet the test itself is rarely explained. It is a provocative traction test for occult ligamentous instability in a subaxial injury that looks equivocal on static films.
- Performed supine, patient awake and cooperative, with a lateral radiograph and full neurological check at every step.
- Axial traction is applied through skull tongs (Gardner-Wells) or a head halter and increased in small increments (roughly 5 kg / 10 lb at a time) up to a ceiling of one-third of body weight or about 65 lb (roughly 30 kg), whichever is less.
- A control lateral film is taken before loading; a second lateral is taken at each weight increment.
- Interspace separation of greater than 1.7 mm at any level between the pre-stretch and stretched films, or
- Change in interspace angulation of greater than 7.5 degrees at any level.
- Stop immediately for any neurological change, pain, or excessive separation — the test can convert an occult injury into a cord injury if pushed.
- It is contraindicated in the obtunded or uncooperative patient and where gross instability or a fracture is already obvious.
- In current practice the stretch test is largely historical: dynamic flexion-extension views (when safe) and, above all, MRI of the discoligamentous complex have superseded it, but it remains an examinable component of the White-Panjabi score and a useful conceptual anchor for what "positive stretch test = 2 points" actually means.
Examiners cite it because it forces you to say the two White-Panjabi thresholds out loud — greater than 1.7 mm separation or greater than 7.5 degrees angulation — and to state its hard rules: awake patient, radiograph plus neurology at every increment, ceiling of one-third body weight or 65 lb, and abort on any neurological change. Volunteering that MRI has largely replaced it shows current, safe judgement.
Differential Diagnosis
The key task is to separate true mechanical instability from mimics that cause neck pain or myelopathic signs without abnormal segmental motion.
- 1
- Abnormal segmental motion under physiological load
- 2
- Dynamic flexion-extension imaging, ADI/PADI, White-Panjabi
- 1
- Static canal stenosis, no abnormal motion
- 2
- MRI cord signal, static canal diameter
- 1
- Radiculopathy or myelopathy without translation
- 2
- MRI disc, neutral alignment
- 1
- Physiological C2-C3 / C3-C4 step-off that reduces on extension
- 2
- Swischuk spinolaminar line
- 1
- Fixed ossicle, may mimic acute fracture
- 2
- CT (corticated margins) vs fracture
- 1
- Rigid fused spine, highly unstable transverse fracture
- 2
- CT/MRI whole spine, low threshold
- 1
- Congenital fusion shifting motion to open segments
- 2
- Dynamic radiographs of mobile levels
Management
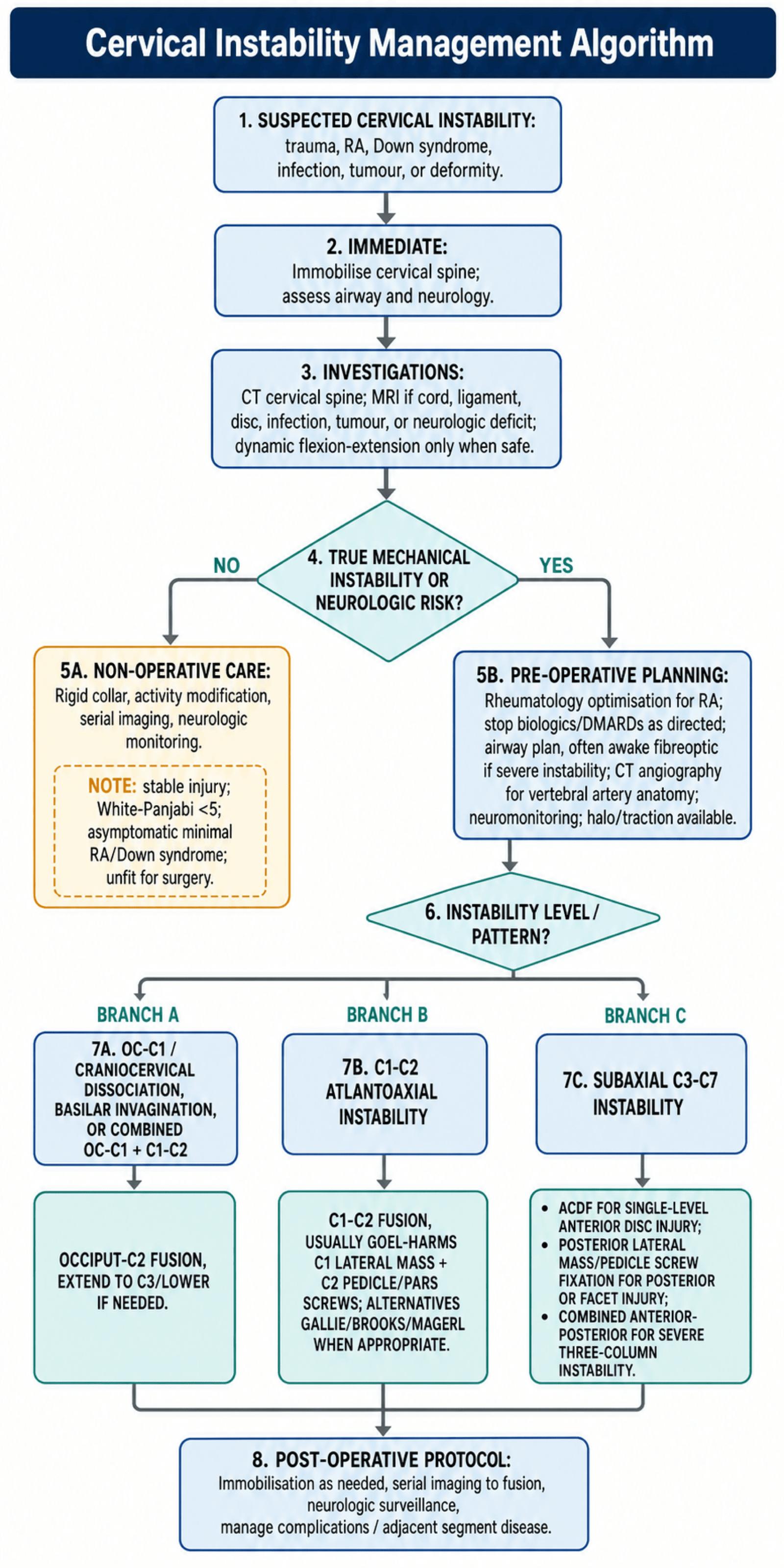
Pre-operative Planning:
- RA patients need pre-op rheumatology optimization
- Stop biologics/DMARDs as directed
- Airway plan with anesthesia (awake fiberoptic if severe instability)
- Prepare for prone vs lateral positioning
- Have halo available if needed for intra-op traction
Non-operative Management
- Stable injuries (White-Panjabi less than 5)
- Asymptomatic RA with minimal ADI increase
- Asymptomatic Down syndrome with AAI on screening
- Patient unfit for surgery
- Rigid cervical collar (Miami J, Aspen)
- Activity modification
- Serial imaging to monitor progression
- Neurological monitoring
- 6-12 weeks for stable injuries
- Indefinite monitoring for RA/Down syndrome
- True instability rarely heals without surgery
- High failure rate for type II odontoid in elderly
Airway & Anaesthetic Management of the Unstable Cervical Spine
The one-pager warns that RA patients must be screened for atlantoaxial instability before anaesthesia, and the vivas and SafetyAlert repeatedly invoke awake fibreoptic intubation — but the airway plan itself is worth developing, because laryngoscopy is often the moment of greatest iatrogenic cord risk.
conventional direct laryngoscopy forces occipito-atlantal extension, which can drive an unstable segment (especially C1-C2 in RA, or a subaxial dislocation) into the cord. The goal is a secured airway with minimal cervical motion and a preserved ability to check neurology.
- Awake fibreoptic intubation — the reference technique for known or severe instability. The neck stays neutral, the patient self-maintains tone, and a neurological check is possible after intubation and after positioning while the patient is still awake.
- Videolaryngoscopy — produces less upper cervical extension than direct laryngoscopy and is a reasonable asleep alternative when awake technique is impractical.
- Direct laryngoscopy with manual in-line stabilisation (MILS) — the front of a hard collar is opened and an assistant holds the head neutral (a hold, not traction, which could distract an unstable segment) while the collar is reapplied afterwards.
- Keep rigid immobilisation until the airway is secured; avoid brisk flexion, extension, rotation, or traction throughout.
- Log-roll for transfers; position prone onto Mayfield tongs or a horseshoe with the head-neck held neutral, re-checking alignment after turning.
- Intra-operative neuromonitoring (SSEP/MEP) and the option of an awake wake-up test guard the cord during reduction and instrumentation.
- Rheumatoid arthritis compounds the risk: cricoarytenoid arthritis (a narrowed, immobile glottis), temporomandibular joint disease (limited mouth opening), a friable mucosa and skin, and the very atlantoaxial subluxation being treated — all push firmly toward an awake fibreoptic plan.
- Down syndrome adds macroglossia, midface hypoplasia, and possible atlanto-occipital as well as atlantoaxial laxity.
Say the principle first: secure the airway with the least cervical movement while keeping the ability to test neurology. Then name the tools — awake fibreoptic intubation for severe/known instability, videolaryngoscopy or direct laryngoscopy with manual in-line stabilisation (a hold, never traction) as alternatives — and finish with the RA red flags: cricoarytenoid and TMJ involvement plus the subluxation itself.
Complications
Perioperative Complications
- Cord injury (rare, less than 1%)
- Root injury (C2 - occipital numbness)
- Worsening myelopathy
- Vertebral artery injury (2-4% with C1-C2 screws)
- May be asymptomatic if contralateral dominant
- Cerebellar stroke if bilateral injury
- Post-op swelling and airway compromise
- Delayed extubation often needed
- Consider ICU monitoring
- Pressure sores (prone positioning)
- Brachial plexus injury
- Peripheral nerve injury
Complication Prevention:
- Pre-operative CT angiography for vertebral artery dominance
- Neuromonitoring (SSEPs, MEPs) intraoperatively
- Meticulous technique with anatomical landmarks
- Appropriate collar immobilization post-op
Guidelines, Registries & Global Practice
Global epidemiology:
- Trauma is the leading cause worldwide, with motor-vehicle and fall mechanisms predominating in high-income settings and a higher proportion of high-energy/road-traffic trauma in low- and middle-income countries.
- Rheumatoid arthritis historically caused cervical instability in 25-80% over the disease course; the incidence of severe craniocervical disease has fallen markedly in regions with early access to modern DMARDs and biologics.
- Down syndrome screening series report atlantoaxial instability in roughly 10-20%, the large majority asymptomatic (Pueschel and Scola: 14.6%).
Side-by-side guidance:
- Position
- Subaxial trauma stratified by morphology, discoligamentous complex, neurology; score over 4 favours surgery
- Position
- Major-trauma cervical clearance pathways; MRI before reduction where ligamentous or disc injury is suspected
- Position
- Emphasis on PADI and dynamic imaging for rheumatoid AAI; surgery before neurological decline
- Position
- Down syndrome: clinical screening emphasised; routine flexion-extension radiographs for sport no longer universally mandated
- Craniocervical and upper-cervical fusion volumes are low, so high-quality evidence is dominated by single-centre series and biomechanical studies rather than large registries.
- Spine registries (e.g. national spine surgery and trauma databases in the UK, US, Scandinavia) increasingly track subaxial fusion outcomes, adjacent-segment disease, and revision rates.
- Where CT angiography, intra-operative neuromonitoring, and navigation are available, screw-based constructs (Goel-Harms, lateral mass, pedicle) are standard.
- In limited-resource settings, wiring techniques, halo immobilisation, and traction-based reduction retain a larger role; awake intubation and meticulous landmark-based technique remain universally applicable.
Controversies & Areas of Uncertainty
- Routine flexion-extension radiographs for Down syndrome sport clearance — historically mandated, now widely questioned because asymptomatic radiographic AAI poorly predicts catastrophic injury; many bodies emphasise clinical screening and symptom-directed imaging instead.
- Powers ratio vs modern measurements — the Powers ratio is insensitive for non-anterior and distraction injuries; CT-based BDI/BAI (Harris lines) and the condyle-C1 interval are more reliable for craniocervical dissociation.
- Type II odontoid fracture in the elderly — operative vs non-operative management remains debated, balancing high non-union rates against the morbidity of surgery and halo immobilisation; fibrous stable non-union may be an acceptable endpoint.
- C2 fixation choice — pedicle vs pars vs translaminar screws are selected by vertebral artery anatomy on pre-operative CT angiography; no single technique is universally superior.
- Closed reduction before MRI in facet dislocations — awake serial traction reduction is advocated by some in alert, cooperative patients, but many centres mandate pre-reduction MRI to exclude a herniated disc that could be driven into the cord.
- Defining instability — White-Panjabi and SLIC are checklists, not validated thresholds for every scenario; clinical judgement integrating dynamic imaging, neurology, and patient factors remains essential.
MCQ Practice Points
Q: What is the normal atlantodental interval (ADI) in adults? A: Less than 3mm. ADI 3-5mm indicates transverse ligament incompetence; greater than 5mm indicates both transverse and alar ligament failure. In children, normal ADI can be up to 5mm due to ligamentous laxity.
Q: What PADI measurement indicates the spinal cord is at risk? A: Posterior Atlantodental Interval (PADI) less than 14mm predicts neurological deficit. PADI represents the space available for the cord (SAC) at C1-2 and is more predictive of myelopathy than ADI.
Q: How is the Powers Ratio calculated and what does a ratio greater than 1 indicate? A: Powers Ratio = BC/OA where B = basion, C = posterior arch C1, O = opisthion, A = anterior arch C1. Ratio greater than 1 indicates anterior occipito-atlantal dislocation. Normal ratio is 0.77 (range 0.55-1.0).
Q: Which patient populations require routine screening for atlantoaxial instability? A: Down syndrome (trisomy 21) and rheumatoid arthritis patients require screening. Down syndrome patients have 15-20% incidence of atlantoaxial instability due to ligamentous laxity. RA patients develop pannus erosion of the transverse ligament.
At a Glance
Cervical instability refers to abnormal motion between vertebrae that may cause neurological compromise, occurring at the craniocervical junction (OC-C1-C2) or subaxially (C3-C7). Key measurements include the ADI (less than 3mm adults, less than 5mm children) reflecting transverse ligament integrity, PADI less than 14mm indicating cord compromise risk, and Powers ratio greater than 1 for anterior OC-C1 dislocation. Rheumatoid arthritis patients have 25-80% prevalence of atlantoaxial instability and require preoperative screening before anesthesia. White-Panjabi criteria (score ≥5) diagnose subaxial instability. Surgical stabilization (e.g., Harms technique C1 lateral mass + C2 pedicle screws) prevents neurological deterioration.
ADIADI Values - AC/DC
Hook:AC/DC - Adult 3, Child 5, Danger at 14 (Cord)
PADSWhite-Panjabi Criteria - PADS
Hook:PADS - 5 Points And you have instability (greater than 5 = unstable)
OCOC-C1 Measurements - POB
Hook:POB - Powers, Occipital, Basion: Key craniocervical measurements
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“55-year-old female with 20-year history of rheumatoid arthritis presents with progressive neck pain, electric shock sensation down her spine when flexing her neck, and difficulty with fine motor tasks in her hands. She is on methotrexate and a TNF-inhibitor. How would you assess and manage this patient?”
“Parents of a 12-year-old boy with Down syndrome bring him for clearance to participate in school gymnastics. They have heard about neck problems in Down syndrome. How do you approach this?”
“24-year-old restrained driver involved in high-speed head-on MVA. GCS 15, complaining of severe neck pain. Initial trauma CT shows 'possible craniocervical dissociation'. How do you assess and manage?”
“32-year-old male dove into shallow water and now has severe neck pain and bilateral arm weakness. X-ray shows C6 anterolisthesis on C7. How do you manage this patient?”
KEY MEASUREMENTS
- ADI: less than 3mm (adult), less than 5mm (child) = normal
- PADI: less than 14mm = cord at risk
- Powers Ratio: greater than 1 = anterior OC-C1 dislocation
- BDI/BAI: greater than 12mm = craniocervical dissociation
- Translation greater than 3.5mm = subaxial instability
- Angulation greater than 11 degrees = subaxial instability
WHITE-PANJABI CRITERIA
- Score 5 or greater = clinically unstable
- Anterior elements destroyed = 2 points
- Posterior elements destroyed = 2 points
- Translation greater than 3.5mm = 2 points
- Angulation greater than 11 degrees = 2 points
- Cord damage = 2 points
SURGICAL TECHNIQUES
- Harms: C1 lateral mass + C2 pedicle screws (standard for AAI)
- Magerl: Transarticular C1-C2 screws (higher VA risk)
- Gallie: Wire + graft (supplements screws)
- OC-C2 fusion: For OC-C1 instability
- ACDF: Subaxial anterior approach
- Lateral mass screws: C3-C6 posterior
RA CERVICAL DISEASE
- AAS (atlantoaxial subluxation) = 65%
- SAS (subaxial subluxation) = 20%
- Basilar invagination = 15% (most dangerous)
- PADI less than 14mm = operate before neuro decline
- Stop biologics 2-4 weeks pre-op
- Awake fiberoptic intubation if severe
Evidence Base
- 73 RA patients; PADI correlated with paralysis whereas anterior ADI did not
- All Class III patients had PADI/subaxial canal under 14mm; PADI best predicted recovery
- C1 lateral mass + C2 pars/pedicle polyaxial screws with rods; 37 patients, solid fusion in all
- No neural or vascular injury; allows intra-operative reduction unlike transarticular screws
- 10 cadaveric spines; both screw constructs reduced motion more than Gallie wiring alone
- No significant stability difference between screw-rod and transarticular constructs
- 30 atlantoaxial dislocations fixed via lateral mass plate-and-screw; 100% union
- No morbidity, mortality, or implant failure; rigid direct C1-C2 segmental fixation
- 404 screened; 14.6% had AAI (13.1% asymptomatic, only 1.5% symptomatic needing surgery)
- ADI greatest in flexion; follow-up showed no significant progression
- Defined the Powers ratio (BC/OA); ratio greater than 1 indicates anterior OC-C1 dislocation
- Created for immediate radiographic recognition of an often-fatal injury
- SLIC scores morphology, discoligamentous complex, and neurology (ICC 0.49-0.90)
- Total score greater than 4 favours surgery; under 4 favours non-operative care
- Point-based subaxial checklist; translation over 3.5mm and angulation over 11 degrees each score 2
- Total score of 5 or greater defines clinical instability