Salvage Osteotomy | Incongruent Hip Dysplasia | Medialisation | Capsular Fibrocartilage Metaplasia | PAO Alternative | Sciatic Notch to AIIS
- The Chiari osteotomy is a SALVAGE procedure — it does not reorient the acetabulum (unlike PAO), but rather displaces it medially to increase superolateral coverage by the proximal iliac shelf
- The key selection criterion is joint INCONGRUENCE — if the femoral head and acetabulum have matching geometry, PAO is preferred because it preserves native articular cartilage as the bearing surface
- The interposed joint capsule undergoes fibrocartilaginous metaplasia, forming a new weight-bearing surface between the iliac roof and the femoral head — this is the fundamental biological mechanism
- Sciatic nerve injury is the most feared complication — the osteotomy exits through the greater sciatic notch and the nerve lies directly posterior to the ilium at this level
- Chiari osteotomy shortens the limb slightly and displaces the hip centre medially, which reduces the joint reaction force (advantage) but may cause abductor lever-arm dysfunction (disadvantage)
- “Always begin a viva answer by distinguishing congruent from incongruent dysplasia — PAO for congruent, Chiari for incongruent
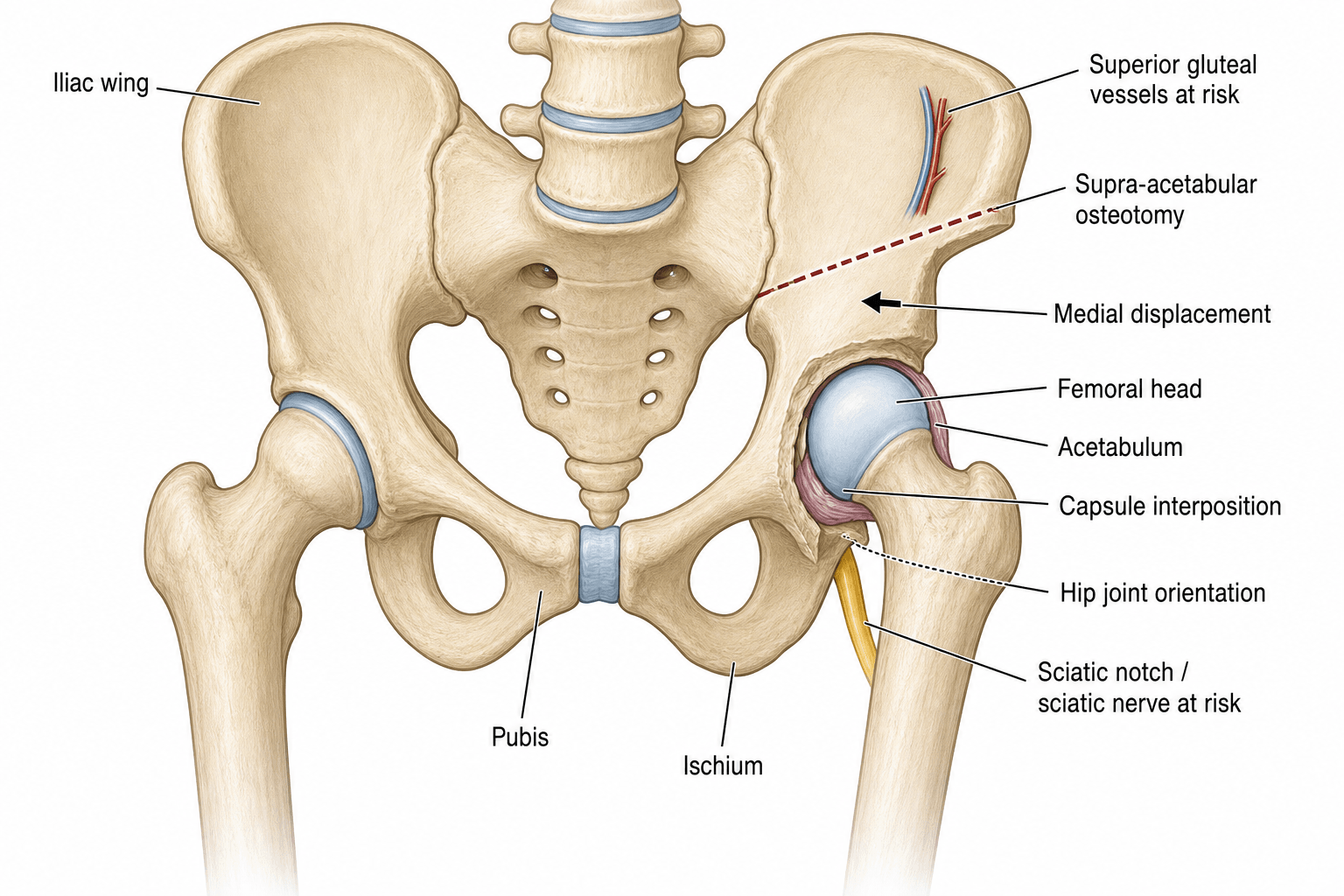
- “The osteotomy cut runs in a curved line from the greater sciatic notch posteriorly to a point just above the anterior inferior iliac spine (AIIS) anteriorly
- “Medial displacement of 10-15 mm (roughly 50% of the iliac thickness) is the typical target — over-displacement risks medial impingement and obturator nerve injury
- “The Chiari is NOT a reorientation osteotomy — it is a medial displacement that creates a new expanded roof; examiners will test whether you understand this distinction
Chiari Pelvic Osteotomy
Examiners want to see that you choose the right operation for the right hip. If the femoral head and acetabulum are congruent (matching shapes, good articular cartilage), the answer is periacetabular osteotomy (PAO) — which reorients the socket while preserving native cartilage. The Chiari is reserved for incongruent joints where the socket and head do not match, where there is significant subluxation with lateral uncovering, or where prior surgery has scarred the joint. Reaching for Chiari when PAO is appropriate loses marks.
- Best option
- Periacetabular osteotomy (PAO / Ganz)
- Reasoning
- Reorients the acetabulum to improve coverage; preserves native articular cartilage; best long-term joint preservation when geometry is favourable
- Best option
- Chiari medial displacement osteotomy
- Reasoning
- Salvage: medial displacement creates an expanded roof; capsular metaplasia provides a new bearing surface; indicated when PAO cannot achieve congruence
- Best option
- Total hip replacement (THR)
- Reasoning
- Definitive treatment for end-stage dysplastic OA; modern implants and techniques handle dysplastic anatomy well; subtrochanteric shortening osteotomy may be needed for high dislocation
- Best option
- Chiari osteotomy (possibly combined with femoral varus derotation osteotomy)
- Reasoning
- Salvage in the skeletally immature; medial displacement improves coverage while growth potential remains; femoral osteotomy addresses coxa valga
Overview and Indications
The Chiari pelvic osteotomy, described by Karl Chiari in Vienna in 1953, is a medial displacement osteotomy of the ilium performed just above the acetabulum. The distal fragment — bearing the acetabulum and femoral head — is shifted medially beneath the intact proximal iliac shelf, which acts as a new, expanded acetabular roof. The interposed hip capsule undergoes fibrocartilaginous metaplasia, creating a new weight-bearing neosurface.
unlike the Ganz periacetabular osteotomy (PAO), which reorients the acetabulum to restore coverage while preserving native hyaline cartilage congruence, the Chiari displaces the acetabulum medially. It is therefore a salvage procedure — used when the femoral head and acetabulum are incongruent and cannot be made to match by reorientation alone.
- Increased superolateral coverage — the proximal iliac fragment extends over the femoral head, deepening the acetabulum
- Medialisation of the hip centre — shifting the joint medially reduces the body-weight moment arm and decreases joint reaction force
- Capsular fibrocartilage metaplasia — the hip capsule, compressed between the new iliac roof and the femoral head, differentiates into a fibrocartilaginous weight-bearing surface over 12-18 months
- Hip dysplasia with incongruent joint (femoral head and acetabulum do not have matching geometry) — the primary indication
- Lateral subluxation of the femoral head with significant uncovering (lateral centre-edge angle less than 20 degrees)
- Age under 40-50 years (some authors extend to 55 in selected patients) with preserved or partially preserved cartilage
- Failed prior hip surgery (e.g., prior innominate osteotomy, shelf procedure) with residual subluxation
- Neuromuscular hip dysplasia (cerebral palsy, myelomeningocele) — where joint incongruence and subluxation are typical
- Adolescent dysplasia after triradiate cartilage closure, when PAO is not feasible due to incongruence
- As a salvage after failed PAO or when acetabular reorientation is anatomically impossible
- Legg-Calve-Perthes disease sequelae with aspherical femoral head and incongruent acetabulum
- Developmental dysplasia of the hip (DDH) late presentation with established incongruence
- Combined with femoral varus derotation osteotomy for coxa valga and excessive anteversion
On an AP pelvis radiograph with the hip in neutral, abduction, and adduction (three-view Shenton assessment), assess whether the femoral head fits into the acetabulum. If abduction makes the joint congruent (head nests into the socket), the patient is a PAO candidate. If the joint remains incongruent in all positions (aspherical head, flattened socket, or mismatched geometry), the Chiari osteotomy is the appropriate salvage. Examiners will test this distinction repeatedly.
A strong viva answer places the Chiari within the family of pelvic osteotomies, classified by what they do to the acetabulum:
- Reorientation (redirectional) - free the acetabulum and rotate it to cover the head with native hyaline cartilage; require a congruent joint and (mostly) an open or recently closed triradiate. Examples: Salter (single innominate, hinges on the pubic symphysis), Steel/Tonnis triple, and the Ganz periacetabular osteotomy (PAO) in the mature pelvis.
- Reshaping (acetabuloplasty / incomplete) - an incomplete iliac cut hinges through the triradiate cartilage to bend the roof down over the head; paediatric, needs an open triradiate. Examples: Pemberton (hinges on the triradiate cartilage) and Dega (hinges on the intact medial/posterior cortex).
- Salvage - used when the joint is incongruent and native cartilage cannot be brought to bear; create coverage with a non-hyaline (fibrocartilaginous) surface. Examples: Chiari (medial displacement) and the shelf (extra-articular bone block).
The Chiari is therefore a salvage osteotomy - the examiner wants you to reach for a reorientation procedure (PAO) for the congruent joint and reserve the Chiari/shelf for the incongruent hip.
Neuromuscular dysplasia (cerebral palsy, myelomeningocele) is a recognised Chiari indication because the spastic hip subluxates with an incongruent, often aspherical head. Decision-making is driven by hip surveillance and the Reimers migration percentage (MP) on a standardised supine AP pelvis - the proportion of the femoral head lying lateral to Perkin's line (the lateral acetabular edge):
- MP up to about 30% is within the normal/surveillance range.
- MP about 30-33% or rising indicates subluxation and triggers intervention.
- MP over about 50-60% indicates severe subluxation heading toward dislocation.
In the spastic hip, early subluxation is treated with soft-tissue releases (adductor/psoas) plus a femoral VDRO; once there is fixed acetabular dysplasia, an acetabular procedure is added - a reshaping (Dega / San Diego) acetabuloplasty if the triradiate is open and the head reasonably congruent, or a Chiari (often with VDRO) for the older child with an incongruent, painful subluxated hip. Knowing the MP thresholds and where the Chiari fits in the CP hip is examinable.
Relevant Anatomy and Biomechanical Principles
- The ilium above the acetabulum is a broad, flat sheet of cancellous bone with thin cortices — ideal for osteotomy and rapid healing. The bone is thickest just above the acetabular roof (the supra-acetabular region) and thins towards the iliac crest.
- The greater sciatic notch is the posterior boundary of the ilium; the sciatic nerve, piriformis, and superior/inferior gluteal vessels pass through it. The notch is the posterior exit point of the Chiari osteotomy.
- The anterior inferior iliac spine (AIIS) — giving rise to the direct head of rectus femoris — is the anterior exit point. The osteotomy passes just above the AIIS, staying extra-articular.
- The hip joint capsule attaches to the acetabular rim (labrum) and the intertrochanteric line anteriorly. In the Chiari, the capsule is deliberately preserved intact between the osteotomised surfaces — it is the substrate for fibrocartilaginous metaplasia.
- The triradiate cartilage (in children) fuses at approximately 12-16 years; the Chiari is performed after fusion to avoid growth disturbance.
- Sciatic nerve — exits the pelvis through the greater sciatic notch, typically deep to the piriformis. It lies immediately posterior to the ilium at the level of the osteotomy exit. This is the most critical structure at risk.
- Superior gluteal nerve and artery — exit the greater sciatic notch above the piriformis and supply the gluteus medius, gluteus minimus, and tensor fasciae latae. They may be stretched or injured during medial displacement of the distal fragment.
- Femoral nerve — runs on the anterior surface of the iliacus, medial to the AIIS. At risk from anterior retraction during exposure.
- Obturator nerve and artery — pass through the obturator foramen on the inner table of the ilium. Excessive medial displacement of the distal fragment can compress the nerve against the inner pelvic wall.
- Internal iliac vessels — lie on the inner table of the ilium posteriorly; protected by the iliacus muscle but at theoretical risk from penetration of the inner cortex.
- Medialisation of the hip centre reduces the body-weight moment arm (the horizontal distance from the body's centre of gravity to the hip centre). By the Pauwels principle, this decreases the resultant joint reaction force.
- However, medialisation also shortens the abductor lever arm (the distance from the hip centre to the greater trochanter), which may weaken abductor efficiency and contribute to a Trendelenburg gait.
- The fibrocartilaginous neosurface that develops from capsular metaplasia is biomechanically inferior to hyaline cartilage — it has lower wear resistance and less capacity for load distribution. This is why the Chiari is a time-buying salvage, not a definitive cure.
- The proximal iliac shelf provides approximately 15-20 degrees of additional lateral coverage, depending on the degree of displacement.
Internervous Plane and Surgical Interval
The Chiari osteotomy uses an anterior approach to the hip and ilium — there is no true internervous plane at the iliac wing. The exposure is through a muscle-splitting and subperiosteal dissection.
Standard approach (modified Smith-Petersen / ilioinguinal variation):
- Skin incision: a longitudinal or slightly curved incision along the iliac crest, extending from the posterior third of the crest to the AIIS region, or a bikini-type incision for cosmesis.
- Superficial dissection: the interval between the tensor fasciae latae (superior gluteal nerve) and the sartorius (femoral nerve) is developed distally. The lateral femoral cutaneous nerve is at risk in this interval and must be identified and protected.
- Deep dissection — outer table: the gluteus medius and minimus are elevated subperiosteally from the outer table of the ilium, exposing the supra-acetabular region down to the hip capsule. The capsule is identified but NOT opened.
- Deep dissection — inner table: the iliacus is elevated subperiosteally from the inner table of the ilium. This exposes the quadrilateral surface and the margin of the greater sciatic notch from the medial side.
- Exposure of the greater sciatic notch: both inner and outer table dissections converge on the greater sciatic notch. A Blount retractor or Hohmann spike is passed through the notch (subperiosteally, hugging bone) to protect the sciatic nerve and superior gluteal vessels. This step is critical — the retractor must be placed on bone, not in the soft tissues.
The osteotomy exits posteriorly through the greater sciatic notch, where the sciatic nerve, superior gluteal nerve, and superior gluteal vessels lie in immediate proximity. A blunt retractor passed subperiosteally through the notch — hugging the bone of the posterior column — is essential. Placing the retractor into the soft tissues of the notch risks direct nerve injury. Examiners will ask specifically how you protect the sciatic nerve during this step.
Patient Positioning and Setup
- Position: supine on a radiolucent table with a small sandbag under the ipsilateral buttock to internally rotate the femur and improve access to the posterior ilium. The leg is draped free to allow hip flexion, abduction, and rotation during the procedure.
- Anaesthesia: general or spinal anaesthesia. A lumbar plexus block (or iliac crest block) may supplement analgesia but should not obscure assessment of sciatic or femoral nerve function post-operatively.
- Fluoroscopy: essential. The image intensifier is positioned for AP and iliac oblique (Judet) views of the acetabulum. The AP view confirms the osteotomy level and displacement; the iliac oblique view confirms the posterior exit at the sciatic notch.
- Tourniquet: generally NOT used for pelvic osteotomies (the field is too proximal). Meticulous haemostasis with electrocautery and bone wax is essential.
- Cell saver or typed and cross-matched blood: the subperiosteal dissection of the iliac wing and the cancellous bone of the osteotomy can produce meaningful blood loss (typical estimated blood loss 300-800 mL). Blood should be available.
- Pre-operative planning: standing AP pelvis, false-profile (Lequesne), and Dunn/lateral radiographs. Three-view congruence assessment (neutral, abduction, adduction). CT scan with 3D reconstruction is increasingly used to plan the osteotomy level and angle. The lateral centre-edge angle of Wiberg, Tönnis angle, and anterior centre-edge angle are measured.
Surgical Technique
The iliac crest is exposed through a longitudinal or bikini incision. The iliac apophysis is split (in younger patients) or the gluteal muscles are elevated directly from the outer table. Subperiosteal dissection exposes the outer table of the ilium from the iliac crest to the hip capsule. The inner table is similarly exposed by elevating the iliacus.
A blunt retractor (Blount, Hohmann, or a specialised Chiari retractor) is passed subperiosteally through the greater sciatic notch, hugging the bone of the posterior column. A second retractor is placed at the AIIS anteriorly. The hip capsule is identified but left undisturbed.
The osteotomy line is marked on the supra-acetabular ilium — a concave curved line from the greater sciatic notch posteriorly to just above the AIIS anteriorly. The cut is angled approximately 10-15 degrees cephalad from the horizontal (relative to the pelvis) so that medial displacement creates an overlapping shelf.
The cut is made with an oscillating saw and completed with angled osteotomes, proceeding from anterior to posterior. The osteotomy must stay extra-articular — the superior rim of the acetabulum is the inferior boundary. The posterior cortex at the sciatic notch is the last cut, made carefully with a narrow osteotome under protection of the sciatic nerve retractor.
The distal fragment (bearing the acetabulum and femoral head) is displaced medially by approximately 50% of the iliac thickness (10-15 mm). This is achieved by controlled pressure on the greater trochanter with the hip in slight flexion and abduction, or with a lamina spreader. The displacement should be even without rotation.
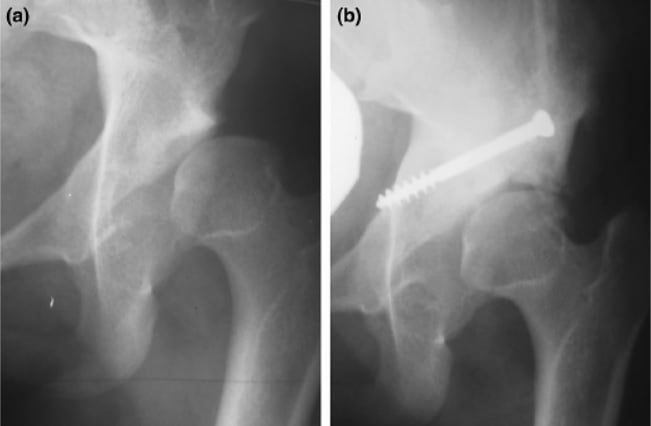
The fragments are fixed with 2-3 cancellous lag screws inserted from the proximal iliac fragment into the displaced distal fragment. The screws are typically placed along the iliac wing. A neutralisation plate may be added for rotational stability.
The gluteal muscles are reattached to the iliac crest with heavy absorbable sutures through drill holes. A drain is placed in the wound. The iliac apophysis is closed in younger patients.
(1) Intra-articular extension — if the saw or osteotome enters the acetabulum, the joint is violated and the fibrocartilaginous neosurface mechanism is compromised. Always stay proximal to the acetabular rim. (2) Sciatic nerve injury — a retractor placed through the sciatic notch into soft tissues rather than hugging bone can cause permanent nerve palsy. (3) Over-displacement — shifting the distal fragment more than roughly 60-70% of iliac width risks medial impingement, obturator nerve injury, and difficulty with future THR. Displacement is NOT better if it is excessive.
Structures at Risk and Complications
The Chiari osteotomy carries a significant complication profile that reflects the magnitude of the procedure and the proximity of critical neurovascular structures.
- Sciatic nerve injury — the most feared complication. Reported rates vary from approximately 1-5% for transient neuropraxia and less than 1% for permanent palsy. The nerve is at risk at the greater sciatic notch exit point of the osteotomy and from stretching during medial displacement. Protection with a subperiosteal retractor is mandatory.
- Femoral nerve injury — from anterior retraction during exposure of the AIIS region. Usually a neuropraxia that resolves.
- Obturator nerve injury — excessive medial displacement can compress the obturator nerve on the inner table. Presents with medial thigh sensory changes and adductor weakness.
- Superior gluteal nerve injury — the nerve exits the sciatic notch and runs along the outer table of the ilium to supply the gluteus medius and minimus. Elevation of the glutei and displacement of the fragment may stretch or injure it, contributing to abductor weakness and a Trendelenburg gait.
- Loss of abductor power — medial displacement of the hip centre shortens the abductor lever arm (the distance from the hip centre to the greater trochanter decreases). Even with intact nerve supply, mechanical efficiency is reduced. This is an inherent trade-off of the procedure.
- Limb shortening — the osteotomy shortens the limb by approximately 5-10 mm (the amount of medial displacement). If combined with a femoral varus osteotomy, further shortening may occur. A shoe raise may be needed.
- Incomplete or inadequate coverage — under-displacement leaves the femoral head uncovered. The procedure fails if the displacement is insufficient to create a functional shelf. Intra-operative fluoroscopy must confirm adequate coverage before fixation.
- Medial over-displacement — excessive medial shift causes impingement of the femoral head against the inner pelvic wall and may narrow the obturator foramen. It also makes future THR more difficult by altering the anatomy.
- Intra-articular extension — the most devastating technical error; if the osteotomy enters the joint, the articular surface is destroyed. Prevention requires careful identification of the acetabular rim and staying proximal to it.
- Progression of osteoarthritis — the fibrocartilaginous neosurface, while functional, is biomechanically inferior to hyaline cartilage. Long-term progression to osteoarthritis is common, particularly if pre-operative arthritis was already present (Tönnis grade 2). The Chiari buys time, but most patients will eventually require THR.
- Heterotopic ossification — reported in approximately 5-15% of cases; prophylaxis with NSAIDs or single-dose radiation therapy is used in high-risk patients.
- Nonunion or delayed union — rare because the osteotomy is through well-vascularised cancellous metaphyseal bone, but reported in approximately 1-3% of cases. Smoking increases risk.
- Hardware irritation — prominent screws on the iliac crest or wing may cause pain and require removal after union.
- Wound haematoma and infection — the extensive subperiosteal dissection and cancellous bone surfaces create a risk of haematoma formation. Deep infection is reported in approximately 1-2% of cases.
The Chiari medialises the hip centre, which reduces joint reaction force (good) but also shortens the abductor lever arm (bad). The net effect on abductor function depends on the balance between these forces. In practice, many patients have a mild persistent Trendelenburg gait. Examiners will ask you to explain this trade-off — it is the fundamental biomechanical compromise of the procedure.
Guidelines, Registries and Global Practice
There is no single universal guideline specifically for the Chiari osteotomy; it is increasingly regarded as a historical or specialist salvage technique in the era of PAO. However, its role is recognised in several international contexts:
- AAOS (US): the AAOS clinical practice guideline for hip dysplasia in the young adult recognises pelvic osteotomy (including Chiari) as a treatment option when conservative measures fail. PAO is the first-line recommendation for congruent dysplasia; the Chiari is mentioned as an alternative for incongruent joints.
- BOA/BOAST (UK): the British Orthopaedic Association standards for hip preservation surgery recommend that pelvic osteotomies be performed in specialist centres with expertise in hip dysplasia management. PAO is the preferred reorientation procedure; Chiari is reserved for salvage situations.
- EFORT/European consensus: European centres, particularly in Austria, Germany, and Japan, have the largest published experience with Chiari osteotomy. The technique is accepted as a valid salvage when PAO is not feasible.
- Developmental dysplasia of the hip has an incidence of approximately 1-3% in neonatal screening programmes worldwide, with geographic and ethnic variation (higher in populations practising swaddling with hip extension and adduction).
- Despite universal neonatal screening in many countries, late-presenting DDH and adolescent/young adult dysplasia remain common, particularly in regions without screening programmes.
- The pool of patients who may benefit from a salvage osteotomy (Chiari) persists globally, particularly in low- and middle-income countries where late presentation is more common.
- National joint registries (NJR — UK, AOANJRR — Australia, SHAR — Swedish) do not specifically track Chiari osteotomy as a separate procedure, but they record conversion to THR after prior pelvic osteotomy. Registry data suggest that prior pelvic osteotomy (of any type) increases the complexity of THR conversion but does not compromise long-term implant survivorship when performed by experienced surgeons.
- The Swedish Hip Arthroplasty Register has published data showing that THR after prior Chiari osteotomy has a slightly higher early complication rate (dislocation, nerve injury) compared with primary THR for primary OA, but revision rates at 10 years are comparable.
- Japanese and Austrian centres have the largest historical experience with Chiari osteotomy, reflecting the influence of Chiari's Vienna school and the high incidence of DDH in Japan.
- In North America and the UK, PAO has largely superseded Chiari for primary dysplasia treatment since the 1990s; the Chiari is now reserved for salvage cases.
- In low- and middle-income settings, the Chiari remains a valuable option because it does not require specialised implants (screws alone suffice) and provides durable results without the need for arthroplasty in young patients who perform manual labour.
- The trend globally is toward PAO for congruent dysplasia and Chiari (or hip replacement) for incongruent joints, with the Chiari occupying a narrowing niche as a salvage procedure in younger patients not yet ready for THR.
- Conversion is more complex than primary THR due to altered acetabular anatomy (medialised socket, expanded roof, fibrocartilaginous neosurface, potential hardware).
- The medialised hip centre may require medial placement of the acetabular component, and bone defects in the supra-acetabular region may need bone grafting or augments.
- Despite technical challenges, long-term THR survivorship after prior Chiari is generally comparable to primary THR when performed by experienced surgeons.
Memory Aids
DISPLACEPatient Selection — DISPLACE
Hook:Chiari is for DISPLACE — Dysplasia Incongruent, Subluxated, Preserved cartilage, Lateral uncovering, Adolescent-to-young adult, salvage when PAO is not suitable
NOTCHSurgical Technique — NOTCH TO SPINE
Hook:The Chiari cut runs NOTCH TO SPINE (sciatic notch to AIIS), angled 10-15 degrees cephalad, displacing the acetabulum medially by half the iliac width
DISPLACEDComplications — DISPLACED HIP
Hook:Chiari complications can be remembered as DISPLACED HIP — the procedure displaces the hip, and the complications reflect this fundamental trade-off
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old woman presents with progressive right groin pain and a limp. She was treated with a Pavlik harness as an infant for DDH. Radiographs show a dysplastic right hip with lateral subluxation, a lateral centre-edge angle of 8 degrees, and an aspherical femoral head that does not congruously reduce into the acetabulum on abduction views. The Tönnis grade is 1. Discuss your management.”
“A 32-year-old woman underwent a left Chiari pelvic osteotomy 18 hours ago for incongruent DDH. On post-operative morning ward rounds, she reports numbness in her left foot and inability to dorsiflex or evert the foot. The operative note states the osteotomy was uneventful with adequate displacement. How would you manage this?”
One-liner
- Medial displacement osteotomy of the ilium above the acetabulum — a salvage procedure for incongruent hip dysplasia and subluxation
- Described by Karl Chiari (Vienna, 1953); mechanism is medialisation of the acetabulum with capsular fibrocartilaginous metaplasia forming a new weight-bearing surface
Chiari vs PAO (the key distinction)
- PAO: for CONGRUENT dysplasia — reorients the socket, preserves hyaline cartilage
- Chiari: for INCONGRUENT dysplasia — displaces the socket medially, creates fibrocartilage neosurface
- Assess congruence with abduction-adduction radiographs
- If the joint matches on abduction views, PAO is the answer — not Chiari
Indications (DISPLACE)
- Dysplasia with INCONGRUENCE (femoral head and socket do not match)
- Inadequate lateral coverage (LCE angle less than 20 degrees)
- Subluxation of the femoral head
- Preserved or partially preserved cartilage (Tönnis 0-2)
- Limb salvage timing (young patient, under 40-50, not ready for THR)
- Exclusion of PAO suitability (PAO must be ruled out first)
Technique (NOTCH TO SPINE)
- Curved iliac osteotomy: greater sciatic notch posteriorly to just above AIIS anteriorly
- Angle: 10-15 degrees cephalad from horizontal
- Displacement: approximately 50% of iliac width (10-15 mm medial)
- Capsule preserved intact — NOT opened (fibrocartilaginous metaplasia substrate)
- Fixation: 2-3 cancellous lag screws from proximal to distal fragment
Structures at risk
- Sciatic nerve (greatest risk — at greater sciatic notch exit)
- Superior gluteal nerve and vessels (outer table, post-displacement stretch)
- Femoral nerve (anterior retraction near AIIS)
- Obturator nerve (excessive medial displacement compresses on inner table)
- Lateral femoral cutaneous nerve (superficial dissection interval)
Complications (DISPLACED HIP)
- Damage to sciatic nerve (1-5% neuropraxia, less than 1% permanent)
- Inadequate or excessive displacement
- Shortening of the limb (5-10 mm)
- Progression of OA (fibrocartilage inferior to hyaline — eventual THR likely)
- Loss of abductor power (medialised centre shortens lever arm)
- Acetabular retroversion, HO (5-15%), nonunion (1-3%), hardware irritation
Outcomes
- Approximately 70-80% satisfactory results at 10-20 years in selected patients
- Better outcomes in younger patients (under 35) and lower pre-operative arthritis grade
- Approximately 15-20% require conversion to THR at 15-20 years
- THR after Chiari is more complex but implant survivorship is comparable to primary THR
Evidence Base
- Karl Chiari described the medial displacement pelvic osteotomy as a means to create an expanded acetabular roof over a subluxated femoral head. The osteotomy is performed through the ilium just above the acetabulum, with medial displacement of the distal fragment. The interposed hip capsule undergoes metaplasia to form a new weight-bearing surface. The original report described encouraging early clinical results.
- In 73 hips followed for 20 to 34 years after Chiari osteotomy, approximately 73% had good or excellent clinical results at latest follow-up. Survivorship analysis showed approximately 80% of hips survived without requiring THR at 20 years, declining to approximately 60% at 30 years. Pre-operative arthritis grade and patient age at surgery were the strongest predictors of long-term outcome.
- In 56 Chiari osteotomies reviewed at mean 12 years, clinical results were satisfactory in approximately 75% of cases. The authors emphasised that the Chiari is most effective when performed before significant degenerative change has occurred. Patients with pre-operative Tönnis grade 0-1 arthritis had substantially better outcomes than those with grade 2 or higher. Sciatic nerve neuropraxia occurred in 2 cases (both recovered).
- Compared long-term survivorship of Chiari osteotomy and shelf arthroplasty in adults with hip dysplasia. Both procedures showed declining survivorship over time, with Chiari osteotomy demonstrating better outcomes in younger patients with lower pre-operative arthritis grades. Conversion to THR was the endpoint in survivorship analysis. Age at surgery and pre-operative arthritis stage were the strongest predictors of survivorship for both procedures.
- In 90 Chiari osteotomies in adults with 2-15 years' follow-up, clinical and radiographic outcomes were correlated with pre-operative arthritis grade and adequacy of displacement. Patients younger than 35 with Tönnis grade 0-1 had the best outcomes. Adequate medial displacement (at least 50% of iliac width) correlated with improved coverage and clinical scores. Sciatic nerve neuropraxia occurred in approximately 3% and heterotopic ossification in approximately 10%.