Rare Benign Epiphyseal Cartilage Tumor | Skeletally Immature | Chicken-Wire Calcification
- Epiphyseal location in skeletally immature patient is pathognomonic
- Chicken-wire calcification pattern on histology is diagnostic hallmark
- ABC formation occurs in 30-40% of cases creating mixed cystic-solid appearance
- Painful symptoms with activity-related pain and joint effusion common
- Curettage with adjuvants (phenol, cryotherapy) is standard treatment with 10-20% recurrence
- “Think chondroblastoma for any epiphyseal lesion in adolescent with pain
- “Chicken-wire calcification refers to calcified lacunar rim around chondroblasts
- “Giant cells present but not as numerous as giant cell tumor
- “Rare benign metastasis to lungs can occur (not malignant transformation)
Epiphyseal location in open physis patient is the key diagnostic feature. After physeal closure, may extend into metaphysis. Most common sites: proximal humerus, distal femur, proximal tibia, proximal femur.
Chicken-wire calcification pattern from calcified lacunar rims around chondroblasts. Mononuclear chondroblasts with oval nuclei plus osteoclast-type giant cells. S100 positive on immunohistochemistry.
Secondary ABC develops in 30-40% creating expansile cystic appearance. This can obscure underlying chondroblastoma diagnosis. Look for solid component with chicken-wire pattern.
Extended curettage with adjuvants is gold standard. Phenol, cryotherapy, or PMMA cementation reduce recurrence from 30% to 10-20%. Wide excision for recurrent or expendable bones (fibular head).
- Age
- 10-25y (open physis)
- Location
- Epiphysis
- Key Feature
- Chicken-wire calcification
- Giant Cells
- Present (moderate)
- Age
- 20-40y (closed physis)
- Location
- Epiphysis-metaphysis
- Key Feature
- Soap-bubble, eccentric
- Giant Cells
- Numerous (predominant)
- Age
- Over 30y
- Location
- Epiphysis
- Key Feature
- Clear cytoplasm, low-grade
- Giant Cells
- Absent
- Age
- Any age
- Location
- Epiphysis
- Key Feature
- Fever, elevated inflammatory markers
- Giant Cells
- Absent
Overview and Epidemiology
Chondroblastoma is a rare benign cartilage tumor accounting for less than 1% of all bone tumors. It is unique in arising from the epiphysis of long bones in skeletally immature patients (peak age 10-25 years). The characteristic histological feature is chicken-wire calcification - a lacy pattern of calcified lacunar rims surrounding chondroblasts. Despite being benign, chondroblastoma causes significant pain and can recur in 10-20% after curettage. Rare cases exhibit benign pulmonary metastasis (not malignant transformation) that may spontaneously regress.
- Age: Peak 10-25 years (range 5-30)
- Sex: Male predominance 2:1
- Incidence: Under 1% of all bone tumors
- Skeletal maturity: 90% occur before physeal closure
- Proximal humerus: 20-25% (most common)
- Distal femur: 20% (second most common)
- Proximal tibia: 15-20%
- Proximal femur: 10-15%
- Other sites: Calcaneus, talus, patella rare
Why Epiphyseal Location Matters
Epiphyseal lesion + OPEN physis = Think chondroblastoma (or infection)
Epiphyseal lesion + CLOSED physis = Think giant cell tumor (or clear cell chondrosarcoma)
The status of the growth plate is critical for narrowing differential diagnosis. Chondroblastoma arises when physis is open and may extend into metaphysis after physeal closure. Giant cell tumor typically presents after physeal closure (age 20-40).
Pathophysiology and Pathology
Histogenesis
Chondroblastoma arises from germinative cartilage cells in the epiphysis - primitive chondroblasts that normally form secondary centers of ossification. The exact trigger for neoplastic transformation is unknown. Recent molecular studies have identified recurrent H3F3B K36M mutations in 95% of chondroblastomas, suggesting this is a driver mutation.
- H3F3B K36M mutation: Found in 95% of cases
- Histone H3.3 variant: Affects epigenetic regulation
- Diagnostic utility: Can help distinguish from mimics
- Not hereditary: Somatic mutation, not germline
- Growth pattern: Slow progressive enlargement
- Joint involvement: May penetrate articular cartilage (5-10%)
- ABC formation: Secondary ABC develops in 30-40%
- Benign metastasis: Rare pulmonary implants (under 1%)
Gross Pathology
Curettage specimen reveals friable red-gray tissue with gritty consistency due to calcifications. The tumor is well-circumscribed within the epiphysis, sometimes with cystic hemorrhagic areas if secondary ABC is present.
Histology - The Diagnostic Triad
Microscopic Features
Mononuclear round to polygonal cells with distinct cell borders, pink cytoplasm, and oval nuclei with longitudinal nuclear grooves. Nuclei may have coffee-bean appearance. These are the neoplastic cells.
Osteoclast-type multinucleated giant cells scattered throughout. Less numerous than in giant cell tumor. Giant cells are reactive, not neoplastic.
Lacy network of calcified lacunar rims surrounding chondroblasts creating a chicken-wire pattern. This represents dystrophic calcification of pericellular matrix. Diagnostic hallmark on low power.
Cartilaginous matrix may be present focally. Chondroblasts embedded in hyaline or myxochondroid matrix. Calcification common.
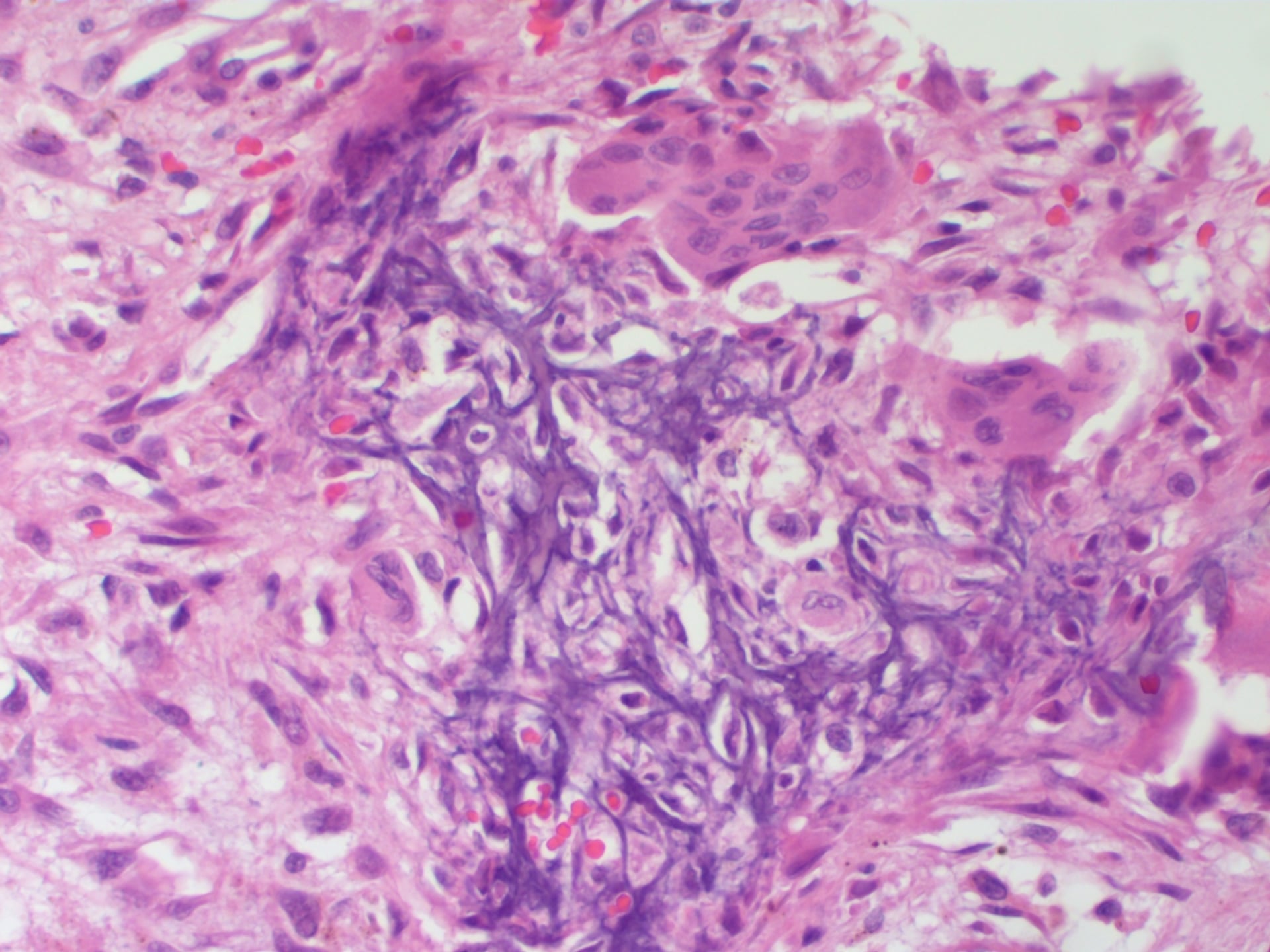
The chicken-wire calcification pattern is created by calcification of the pericellular (lacunar) matrix around individual chondroblasts. On hematoxylin and eosin staining, this appears as a fine lacy network of purple-blue material outlining cells. At low magnification, it resembles chicken wire fencing. This pattern is PATHOGNOMONIC for chondroblastoma and distinguishes it from all other bone tumors including giant cell tumor.
Immunohistochemistry
- Staining
- Positive (strong)
- Interpretation
- Confirms chondroid differentiation
- Staining
- Positive
- Interpretation
- Specific for chondroblastoma
- Staining
- Positive (mutation-specific antibody)
- Interpretation
- Highly specific, aids diagnosis
- Staining
- Negative
- Interpretation
- Excludes epithelial tumors
Secondary Aneurysmal Bone Cyst
30-40% of chondroblastomas develop secondary ABC component, creating blood-filled cystic spaces within the tumor. This can:
- Obscure the underlying chondroblastoma on imaging (appears purely cystic)
- Lead to rapid expansion and pathological fracture
- Make biopsy diagnosis challenging if solid component not sampled
When biopsying an epiphyseal lesion with ABC features, ensure multiple samples from solid areas are obtained. Sampling only the cystic/ABC component will miss the underlying chondroblastoma diagnosis. Review imaging to target solid nodules for biopsy needle placement.
Classification
- Category: Benign cartilage tumor
- Behavior: Locally aggressive (intermediate)
- ICD-O Code: 9230/0
- Epiphyseal location (distinguishing feature)
- Contains mononuclear chondroblasts
- "Chicken-wire" calcification pattern
- H3K36M mutation (diagnostic marker)
- Intracapsular, well-demarcated
- Minimal symptoms, incidental finding
- Observation may be appropriate
- Most common presentation
- Symptomatic, progressive growth
- Contained by natural barriers
- Curettage with adjuvant therapy
- Breaks through cortex or physis
- Extracompartmental extension
- May require en bloc resection
Chondroblastoma is the only benign cartilage tumor that arises in the epiphysis. This epiphyseal location with open physes in a young patient is virtually pathognomonic. Other cartilage tumors (enchondroma, osteochondroma) arise in metaphysis or diaphysis.
Clinical Presentation
- Pain: Dull aching pain, worse with activity (90%)
- Duration: Chronic pain over months to years
- Joint effusion: Reactive synovitis in adjacent joint (40%)
- Stiffness: Limited range of motion from pain and effusion
- Limp: If lower extremity involvement
- Tenderness: Localized to epiphyseal region
- Effusion: Joint swelling from reactive synovitis
- ROM: Restricted by pain, not mechanical block
- Muscle atrophy: Quadriceps wasting if chronic knee pain
- Warmth: May be warm but not erythematous
Typical Clinical Scenarios
Common Presentations by Location
Adolescent athlete with shoulder pain worse with overhead activity. Limited abduction and forward flexion. May mimic rotator cuff tendinitis or impingement.
Adolescent with anterior knee pain and effusion. Pain with running or jumping. May be misdiagnosed as patellofemoral pain syndrome or Osgood-Schlatter disease.
Adolescent with knee pain localized to proximal tibia. Effusion common. May mimic meniscal tear or tibial spine injury.
Child or adolescent with hip pain and limp. Pain with internal rotation. May be confused with slipped capital femoral epiphysis (SCFE) or Perthes disease.
Think chondroblastoma when:
- Adolescent (10-25 years) with chronic epiphyseal pain
- Pain worse with activity, not relieved with rest
- Joint effusion out of proportion to trauma history
- X-ray shows epiphyseal lytic lesion with sclerotic rim
- MRI shows bone marrow edema extending beyond lesion
Do NOT dismiss as growing pains or overuse injury - persistent epiphyseal pain in adolescent warrants imaging.
Rare Presentations
In 5-10% of cases, tumor penetrates articular cartilage into joint space. Presents with mechanical symptoms, locking, catching. May mimic loose body or meniscal tear. Arthroscopy reveals cartilage defect with tumor tissue.
Rare phenomenon (under 1%) where tumor cells implant in lungs without malignant transformation. Usually asymptomatic, discovered on chest imaging. May spontaneously regress. Not true malignancy - termed benign metastasizing chondroblastoma.
The classic teaching is "long-bone epiphysis," but a viva will test whether you know chondroblastoma also arises in epiphyseal-equivalent and atypical locations - and these behave or present differently.
- Apophyses (epiphyseal equivalents): the greater trochanter, tibial tubercle, iliac crest and patella - same biology as an epiphyseal lesion, because apophyses are secondary ossification centres. Keep chondroblastoma in the differential for a lytic apophyseal lesion in a young patient.
- Tarsal bones (talus and calcaneus): present late with vague hindfoot/ankle pain (often misdiagnosed as a sprain or a simple cyst), are technically difficult to access, and carry a higher recurrence rate than long-bone lesions.
- Craniofacial skeleton - classically the temporal bone/skull base: a recognised atypical site occurring in older patients than long-bone disease, presenting with hearing loss, temporomandibular symptoms or a skull-base mass.
- Flat and irregular bones (rib, pelvis, scapula) are rare but reported.
Exam point: chondroblastoma is not confined to the long-bone epiphysis - it also occurs in apophyses (greater trochanter, tibial tubercle, patella - epiphyseal equivalents), the tarsal bones (talus/calcaneus, which present late and recur more), and the craniofacial skeleton (temporal bone/skull base, in older patients) - so an epiphyseal-equivalent lytic lesion anywhere in a young patient should raise the diagnosis.
Investigations and Imaging
Imaging Atlas

Plain Radiography
X-rays are the first-line investigation and often suggest the diagnosis based on epiphyseal location and appearance.
Radiographic Features
Epiphyseal lesion in patient with open or recently closed physis. This location is diagnostic in the right age group. After physeal closure, tumor may extend into metaphysis.
Eccentric lytic lesion with well-defined geographic borders. Thin sclerotic rim common (50-70%). May have stippled calcifications within lesion (chicken-wire pattern not visible on X-ray).
Typically 2-5cm diameter. Smaller lesions may be entirely within epiphysis. Larger lesions expand epiphysis and may cross into metaphysis.
Usually absent unless secondary ABC causes expansion or pathological fracture. Solid periosteal reaction suggests aggressive behavior (rare malignant transformation).
Sclerotic rim is present in 50-70% of chondroblastomas and represents reactive bone formation. This distinguishes chondroblastoma from infection (no rim) and is less prominent than in chondroblastoma (thinner rim). If rim is very thick and irregular, consider clear cell chondrosarcoma in older patient.
MRI - Gold Standard for Extent Assessment
MRI is mandatory for surgical planning to assess:
- Extent of marrow involvement
- Cartilage penetration into joint
- Secondary ABC component
- Relationship to physis and neurovascular structures
- T1: Low to intermediate signal (solid component)
- T2: High signal (cartilage) + very high signal (ABC cysts)
- STIR: Extensive bone marrow edema (extends beyond tumor)
- Enhancement: Solid portions enhance; cystic ABC areas have fluid-fluid levels
- Epiphyseal centered: Confirms location
- Bone marrow edema: May extend throughout epiphysis and metaphysis (exaggerates true tumor size)
- Joint effusion: Reactive synovitis common
- ABC component: Fluid-fluid levels if secondary ABC present
Extensive bone marrow edema on MRI STIR sequences extends far beyond the actual tumor margins. This reactive edema is inflammatory response and not tumor infiltration. True tumor size is better assessed on T1-weighted images where only the solid lesion shows low signal. Do NOT mistake edema for tumor when planning surgery - curettage only the lytic cavity, not entire edema zone.
CT Scan
CT is useful for:
- Detecting calcifications within tumor (chicken-wire pattern as subtle stippled density)
- Assessing cortical breakthrough if ABC component causes expansion
- Preoperative planning for cortical window placement
Biopsy
Biopsy is required for definitive diagnosis before surgery. Open biopsy preferred over needle biopsy due to:
- Need for adequate tissue (avoid sampling only ABC component)
- Small epiphyseal lesions difficult to target with needle
- Risk of pathological fracture through biopsy tract
- Indication
- Large accessible lesion
- Advantage
- Minimally invasive, outpatient
- Risk
- Sampling error if ABC component targeted
- Indication
- Small epiphyseal lesion
- Advantage
- Adequate tissue, direct visualization
- Risk
- Requires OR, pathological fracture risk
- Indication
- Expendable bone (fibular head)
- Advantage
- Diagnostic and therapeutic in one procedure
- Risk
- Not feasible for most locations
Differential Diagnosis
- Age
- 10-25y
- Physis Status
- Open
- Histology
- Chicken-wire calcification
- Giant Cells
- Moderate
- Age
- 20-40y
- Physis Status
- Closed
- Histology
- Sheets of giant cells
- Giant Cells
- Numerous
- Age
- Over 30y
- Physis Status
- Closed
- Histology
- Clear cytoplasm, low-grade
- Giant Cells
- Absent
- Age
- Any
- Physis Status
- Open or closed
- Histology
- Inflammatory cells, organisms
- Giant Cells
- Absent
- Age
- Under 20y
- Physis Status
- Usually metaphysis
- Histology
- Langerhans cells, eosinophils
- Giant Cells
- Absent
Both are epiphyseal lesions with giant cells, but key differences:
- Age 10-25y (open physis)
- Chicken-wire calcification
- S100 positive
- Giant cells moderate in number
- 10-20% recurrence
- Age 20-40y (closed physis)
- No calcification pattern
- S100 negative
- Giant cells numerous (sheets)
- 20-50% recurrence, locally aggressive
"While both are epiphyseal lesions with giant cells, chondroblastoma occurs in younger patients before physeal closure and has characteristic chicken-wire calcification. Giant cell tumor presents after physeal closure with sheets of giant cells and no specific calcification pattern. S100 immunostain is positive in chondroblastoma, negative in GCT."
Management Algorithm

Extended Curettage with Adjuvants
Gold standard treatment for chondroblastoma. Goal is to remove tumor while preserving joint and growth plate.
Surgical Technique
- Review MRI to identify true tumor margins (not edema)
- Plan cortical window away from articular surface
- Protect adjacent physis if still open
- Identify neurovascular structures at risk
- Create cortical window (1-2cm) using drill and osteotome
- Position window to access all tumor while preserving subchondral bone
- Save bone window for later replacement if possible
- Thorough curettage with sharp curettes of all sizes
- Remove all gross tumor tissue and membrane
- Extend to subchondral bone but do NOT penetrate articular cartilage
- Inspect cavity walls under direct visualization
- High-speed burr: Remove additional 1-2mm of cavity wall
- Phenol: Apply 5% phenol-soaked gauze for 2 minutes, then copious saline lavage
- OR Cryotherapy: Liquid nitrogen freeze-thaw cycles (2-3 cycles)
- OR Argon beam: Thermal ablation of cavity surface
- Bone grafting: Morselized allograft or autograft
- OR PMMA cementation: Methylmethacrylate (generates heat, kills cells)
- Fill cavity completely to restore structural integrity
- Replace cortical window or use cement as bone substitute
Extended curettage with adjuvants reduces recurrence from 30% (simple curettage) to 10-20%. Mechanisms:
- High-speed burr: Mechanically removes microscopic tumor on cavity wall
- Phenol: Chemical cauterization kills surface cells (penetrates 1-2mm)
- Cryotherapy: Freeze-thaw cycles rupture cell membranes
- PMMA: Exothermic polymerization generates heat (60-80°C) killing cells
Exam answer: "I would perform extended curettage with adjuvant treatment to reduce recurrence. After thorough curettage with curettes, I would use high-speed burr to remove an additional 1-2mm of cavity wall, then apply phenol for 2 minutes followed by copious saline lavage. This reduces recurrence from 30% to approximately 10-20%."
In patients with open growth plate, avoid damage to physis during curettage:
- Stay within epiphysis, do NOT cross physis into metaphysis
- Use imaging guidance or fluoroscopy to confirm margins
- If tumor extends across physis (rare), accept some residual tumor to preserve growth
- Growth arrest from physeal damage causes limb length discrepancy
In proximal femur chondroblastoma, risk of avascular necrosis if disrupting blood supply. Consider wide excision with femoral head replacement in older adolescent near skeletal maturity.
This completes the curettage technique discussion.
The MCQ section mentions radiofrequency ablation in passing, but it is worth knowing as a developing alternative to open curettage - increasingly used for the small, surgically difficult chondroblastoma.
- What and where: CT-guided percutaneous radiofrequency ablation (RFA) (or cryoablation) of a small lesion (typically under about 2 cm) in a deep or technically awkward site - classically the talus or the femoral head/neck - where open curettage is morbid.
- Advantages: day-case, no bone graft, bone-preserving, faster recovery.
- Critical caveats:
- It provides no tissue diagnosis - a confirmatory biopsy must be obtained first (ideally at the same sitting); never ablate an undiagnosed epiphyseal lesion.
- Thermal injury risk to adjacent articular cartilage (chondrolysis), an open physis (growth arrest), and neurovascular structures/skin within about 1 cm - so it is avoided for subarticular lesions hugging the joint surface or lesions close to nerves unless thermoprotection (hydrodissection, gas/saline insulation) is used.
- Not suitable for larger lesions or those with a significant secondary ABC component; incomplete ablation/recurrence may require repeat ablation or conversion to curettage.
Exam point: percutaneous RFA/cryoablation is a minimally invasive option for the small chondroblastoma in a difficult site (talus, femoral head) - but it requires a diagnostic biopsy first and is limited by thermal risk to cartilage, physis and nerves, so it does not replace extended curettage for most accessible lesions.
Surgical Technique
- Cortical window: Create adequate access (larger than lesion diameter)
- Intralesional curettage: Remove all visible tumor with curettes
- High-speed burr: Extend margins 1-2 mm into normal bone
- Adjuvant therapy: Apply local adjuvant
- Bone void filling: Bone graft or cement
- Phenol (89% pure solution, 3 min)
- Cryotherapy (liquid nitrogen)
- High-speed burr (mechanical)
- Argon beam coagulation
- Mechanical support
- Allows early weight-bearing
- Exothermic reaction adds adjuvant effect
- Easier surveillance for recurrence
- Autograft or allograft
- Biological reconstruction
- Preferred in young patients
- May obscure recurrence on imaging
Extended curettage with adjuvant therapy reduces recurrence from 30% (simple curettage) to 10-15%. The combination of mechanical extension (high-speed burr) plus local adjuvant (phenol or cryotherapy) plus bone cement provides the best local control while preserving joint function and physeal integrity.
Complications
Treatment-Related Complications
- Incidence
- 10-20% (with adjuvants), 30% (without)
- Risk Factors
- Incomplete curettage, no adjuvant, ABC component
- Management
- Repeat curettage or wide excision for multiple recurrences
- Incidence
- 2-5%
- Risk Factors
- Large subchondral defect, early weight-bearing
- Management
- Non-weight-bearing, internal fixation if displaced
- Incidence
- 5-10%
- Risk Factors
- Subchondral curettage too aggressive
- Management
- Cartilage repair, accept degenerative arthritis risk
- Incidence
- Under 5%
- Risk Factors
- Physeal injury during curettage in young patient
- Management
- Limb length monitoring, epiphysiodesis or lengthening if needed
- Incidence
- 10-15%
- Risk Factors
- Prolonged immobilization, adhesions
- Management
- Aggressive physiotherapy, manipulation under anesthesia
- Incidence
- 2-3%
- Risk Factors
- Standard surgical site infection risk
- Management
- Antibiotics, debridement if deep infection
Recurrence after curettage occurs in 10-20% despite adjuvants. Typical timeline: 1-3 years post-op. Management:
- Confirm recurrence with MRI and biopsy (distinguish from bone graft resorption)
- First recurrence: Repeat extended curettage with adjuvants - success rate 70-80%
- Second recurrence: Consider wide excision if feasible (expendable bone)
- Multiple recurrences: En bloc resection or accept disease and manage symptoms
Key point: Multiple recurrences do NOT indicate malignant transformation. Chondroblastoma is benign but can be locally persistent. Avoid radiation therapy due to malignant transformation risk.
Postoperative Care
Usually 1-2 days
- Multimodal analgesia
- Transition to oral medications day 1
- Avoid NSAIDs initially (theoretical bone healing concern)
- Sutures/staples removed 10-14 days
- Keep wound dry until healed
- Watch for hematoma, drainage
- Touch weight-bearing for 4-6 weeks (lower extremity)
- Progressive weight-bearing based on bone healing
- Full weight-bearing by 8-12 weeks typically
- Upper extremity: sling 2-4 weeks, then ROM exercises
- Avoid impact activities for 3-6 months
- Return to sports when imaging confirms healing
Recurrence typically occurs within 2 years. Follow-up schedule: radiographs every 3 months for year 1, every 6 months for year 2, then annually for 5 years. CT or MRI if plain films suspicious. Most recurrences present with return of pain before imaging changes.
Outcomes and Prognosis
Long-Term Prognosis
Excellent overall prognosis for chondroblastoma. With appropriate treatment:
- 80-90% cured with single curettage and adjuvants
- Recurrences manageable with repeat curettage or excision
- Functional outcomes excellent in most cases
- Risk of degenerative arthritis low (under 10%) if articular surface preserved
- Malignant transformation extremely rare (under 1%)
For patients and families:
- Chondroblastoma is benign - not cancer
- Surgery is curative in 80-90% with single procedure
- Even if recurrence occurs, repeat surgery is effective
- Long-term function and return to sports expected
- Lifetime risk of arthritis is low if joint surface protected
- No need for lifelong surveillance after 5 years disease-free
Guidelines, Registries & Global Practice
Global Epidemiology
Chondroblastoma is consistently reported as a rare benign bone tumour, accounting for under 1% of all primary bone tumours across published series. Demographics are stable across continents: a male predominance (roughly 2:1) and a young age at presentation. In the largest published multicentre extremity series (199 patients), the mean age was 18 years, with the proximal tibia (27.6%) and proximal femur (26.1%) the most common sites, and the physis open in 25.7%, closing in 22.2% and closed in 52.1% at presentation. In a paediatric-only multicentre cohort restricted to open physes (87 patients), the mean age was 12.5 years with the proximal tibia and proximal femoral epiphysis predominating.
- Consensus Position
- WHO 2020 lists chondroblastoma as a benign cartilage tumour (ICD-O 9230/0) defined by H3F3B K36M mutation
- Evidence Base / Source
- WHO Classification of Tumours: Soft Tissue and Bone, 5th ed (2020); Behjati 2013
- Consensus Position
- Mandatory biopsy of epiphyseal lesions; H3K36M IHC / H3F3B testing to confirm and exclude mimics
- Evidence Base / Source
- Behjati 2013 (PMID 24162739); Kervarrec 2017 (PMID 28059095)
- Consensus Position
- Intralesional (extended) curettage with grafting/cement is first-line worldwide; en bloc resection reserved for expendable/recurrent disease
- Evidence Base / Source
- Xu 2015 (PMID 26041854); Suneja 2005 (PMID 15972914)
- Consensus Position
- Avoided as primary therapy due to malignant transformation concern; not endorsed in benign-tumour guidance
- Evidence Base / Source
- Historical case-series consensus; sarcoma network guidance
Guideline & Network Positions
- Relevant Position
- Benign cartilage tumour, locally aggressive potential; molecularly defined entity
- Practice Implication
- Standardises diagnosis; H3K36M as defining marker
- Relevant Position
- Bone sarcoma guidelines mandate referral of bone tumours to specialist sarcoma centres before biopsy
- Practice Implication
- Biopsy and surgery in a multidisciplinary bone tumour unit
- Relevant Position
- Suspected primary bone tumours referred to a recognised bone tumour treatment centre
- Practice Implication
- Centralised care; planned biopsy through the operating unit
- Relevant Position
- Bone cancer pathway: image, then refer indeterminate aggressive lesions to a sarcoma centre for biopsy
- Practice Implication
- Avoids inappropriately placed biopsy tracts
Chondroblastoma is too rare for a dedicated implant registry; the evidence base is built from multicentre tumour-unit cohorts rather than arthroplasty-style registries. The recurring registry-grade message is that biopsy and definitive surgery should occur within a specialist musculoskeletal tumour unit, because an inappropriately placed biopsy tract can compromise later limb-salvage surgery. Reported local recurrence ranges widely by case-mix - approximately 5% in a mixed-maturity extremity cohort (Xu 2015) up to 32% in strictly open-physis paediatric lesions (Sailhan 2009) - reflecting that open-physis, strictly epiphyseal and proximal humeral/femoral lesions are the highest-risk groups.
Practice Variation
- Adjuvant choice varies by centre and region: high-speed burr is near-universal, with phenol, cryotherapy, argon-beam or PMMA cementation selected by surgeon preference and lesion site; no head-to-head trial establishes superiority.
- Void filling differs by maturity: bone graft is favoured in skeletally immature patients to preserve biology, whereas PMMA is often chosen in older patients for immediate stability and easier surveillance of the cement-bone interface.
- Image-guided ablation (radiofrequency / cryoablation) is an emerging option for small, surgically difficult lesions in some interventional-radiology-led centres but is not yet standard of care.
Documentation & Consent (Global Best Practice)
- Record growth-plate status (open vs closed) explicitly on imaging reports — it drives the differential
- Document that the differential includes chondroblastoma, giant cell tumour and infection, and that biopsy precedes any definitive surgery
- Consent for curettage should cover recurrence (approximately 10-20% with adjuvants, higher in open-physis lesions), physeal/growth-disturbance risk (under 5%), articular damage and arthritis risk (5-10%), and phenol-related soft-tissue injury
- Counsel that wide excision is reserved for recurrent disease or expendable bone (e.g. proximal fibula)
MCQ Practice Points
Q: What is the classic location and age distribution for chondroblastoma?
A: Chondroblastoma is an epiphyseal tumor (arises in secondary ossification center) occurring in skeletally immature patients (10-25 years, M greater than F). Most common locations: Proximal humerus, proximal tibia, distal femur, proximal femur. The epiphyseal location in a young patient with open/recently closed physes is pathognomonic. This contrasts with giant cell tumor (metaphyseal/epiphyseal in skeletally mature patients).
Q: What are the characteristic imaging features of chondroblastoma?
A: Radiographs: Well-defined, geographic lytic lesion in the epiphysis; Sclerotic rim (narrow zone of transition); Internal matrix calcification (40-60%, "chicken-wire" pattern); Size usually 3-6 cm. MRI: Low-intermediate signal T1, heterogeneous T2; Marked surrounding bone marrow edema (disproportionate to lesion size - classic feature); May extend across physis. CT best demonstrates matrix calcification.
Q: What is the histological hallmark of chondroblastoma?
A: Chondroblasts: Round/polygonal cells with well-defined cytoplasmic borders, grooved or "coffee bean" nuclei. Chicken-wire calcification: Fine calcification surrounding individual cells (pericellular). Chondroid matrix: Immature cartilaginous matrix between cells. Giant cells: Scattered osteoclast-like multinucleated giant cells present but not as prominent as in GCT. Immunohistochemistry: S-100 positive, SOX9 positive; H3K36M mutation present in 95% of cases.
Q: What is the standard treatment for chondroblastoma?
A: Standard treatment is intralesional curettage with extended techniques (high-speed burr, electrocautery, phenol or hydrogen peroxide) followed by bone grafting or cement. Local recurrence rate: 10-20% (higher in skeletally immature patients with open physes). Cryotherapy should be used cautiously near physis/articular cartilage. Radiofrequency ablation is an option for small lesions. Rare malignant transformation or pulmonary metastases can occur (1-2%).
Q: How do you differentiate chondroblastoma from other epiphyseal lesions?
A: Chondroblastoma: Young patient (open physes), epiphyseal, sclerotic margin, matrix calcification, extensive edema. Giant cell tumor (GCT): Skeletally mature patient, extends from metaphysis into epiphysis, no sclerotic margin, no matrix, less edema. Clear cell chondrosarcoma: Older patient (30-60 years), proximal femur common, may have aggressive features. Langerhans cell histiocytosis: Younger children, may be epiphyseal but often diaphyseal, no matrix. Infection (Brodie abscess): Metaphyseal location more common, periosteal reaction.
At a Glance
Chondroblastoma is a rare benign cartilage tumour (less than 1% of bone tumours) characterised by epiphyseal location in skeletally immature patients (ages 10-25 years). The key differential is that epiphyseal lesion + open physis = chondroblastoma, whereas closed physis suggests giant cell tumour. Most common sites are proximal humerus (20-25%), proximal femur, and around the knee (70% combined). Histological hallmark is "chicken-wire" calcification—calcified lacunar rims around mononuclear chondroblasts, with S100 positivity. Secondary ABC develops in 30-40%, creating mixed cystic-solid appearance. Treatment is extended curettage with adjuvants (phenol, cryotherapy, or PMMA), reducing recurrence from 30% to 10-20%. Rare "benign pulmonary metastases" can occur—these are not malignant transformation and are managed with observation.
EPIPHYSISChondroblastoma Key Features
Hook:Think EPIPHYSIS - this is where chondroblastoma lives! Young patient, pain in epiphysis, chicken-wire on biopsy.
PHACTreatment Adjuvants to Reduce Recurrence
Hook:PHAC the tumor! Use adjuvants to reduce recurrence from 30% down to 10-20%.
CGCHistological Triad of Chondroblastoma
Hook:CGC - Chondroblasts, Giants, Chicken-wire. The classic histological triad!
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“How do you differentiate chondroblastoma from giant cell tumor?”
“Describe your surgical technique for extended curettage of a chondroblastoma in the proximal tibia of a 16-year-old.”
“What is your follow-up protocol after curettage of a chondroblastoma, and how do you detect recurrence?”
Key Facts
- Rare benign epiphyseal cartilage tumor (under 1% of bone tumors)
- Peak age 10-25 years (open physis), male 2:1
- Most common sites: proximal humerus (20-25%), around knee (70% combined)
- Epiphyseal location before physeal closure is pathognomonic
Histology Triad (CGC)
- Chondroblasts - mononuclear cells with oval grooved nuclei
- Giant cells - osteoclast-type, fewer than in GCT
- Chicken-wire calcification - calcified lacunar rims (pathognomonic)
- S100 positive, H3K36M mutation in 95%
Clinical Presentation
- Activity-related pain for months, joint effusion common
- Epiphyseal tenderness, restricted ROM from pain
- X-ray: eccentric lytic with thin sclerotic rim
- MRI: extensive marrow edema (overestimates tumor size)
Differential Diagnosis
- Giant cell tumor: age 20-40y, closed physis, sheets of giant cells
- Clear cell chondrosarcoma: age over 30y, malignant, no chicken-wire
- Infection: fever, elevated CRP/ESR, no calcification pattern
- Chondromyxoid fibroma: metaphyseal, lobulated architecture
Treatment
- Extended curettage with adjuvants (gold standard)
- Adjuvants: phenol, high-speed burr, cryotherapy, or PMMA
- Reduce recurrence from 30% to 10-20%
- Wide excision for recurrent or expendable bones (fibular head)
Complications and Outcomes
- Recurrence 10-20% with adjuvants (1-3 years post-op)
- Secondary ABC in 30-40% (makes curettage more difficult)
- Malignant transformation extremely rare (under 1%)
- Benign pulmonary metastasis (under 1%) - observe, often regresses
Surgical Pearls
- Protect physis in young patients (avoid growth arrest)
- Preserve subchondral bone (prevent articular collapse)
- Biopsy solid component if ABC present (avoid sampling error)
- PMMA for large subchondral defects (structural support plus thermal kill)
Evidence Base and Key Studies
Defining Histone Driver Mutations (Landmark Molecular Study)
- p.Lys36Met (K36M) alterations, predominantly in H3F3B, found in 73 of 77 chondroblastomas (95%)
- Giant cell tumour of bone instead carries H3F3A G34W/G34L mutations (49/53, 92%)
- Mutations restricted to the neoplastic mononuclear stromal cells, not osteoclasts
- Demonstrates exquisite tumour-type specificity of histone H3.3 driver alterations
- Detectable by mutation-specific (H3K36M) immunohistochemistry for routine diagnosis
H3F3 Mutation as a Diagnostic Marker (Validation Study)
- Multicentre series of 281 bone lesions tested by high-resolution melting plus pyrosequencing
- H3F3 mutations identified in 88% of chondroblastomas and 85% of giant cell tumours of bone
- Mutations were sensitive and specific markers separating these from giant-cell-rich mimics
- Rare H3F3 mutations found in dedifferentiated chondrosarcoma mimicking giant cell tumour
- Supports reclassification of diagnostically difficult giant-cell-rich lesions
Surgical Outcomes - Largest Multicentre Series
- Multicentre retrospective analysis of 199 extremity chondroblastomas (145 male, 54 female; mean age 18 years)
- Most common site was proximal tibia (27.6%), then proximal femur (26.1%) and distal femur (19.1%)
- Physis was open in 25.7%, closing in 22.2% and closed in 52.1% at presentation
- Local recurrence 5.0% after curettage and 0% after en bloc resection
- Proximal humeral location was the only significant predictor of recurrence (p=0.001)
Recurrence Risk in Skeletally Immature Patients
- Multicentre review of 87 chondroblastomas, all in patients with open physes (mean age 12.5 years)
- Most common sites were proximal tibia and proximal femoral epiphysis
- Overall local recurrence 32% at minimum 24-month follow-up
- Strictly epiphyseal lesions had significantly higher recurrence than other locations (p=0.004)
- Aneurysmal bone cyst component and surgical method did not independently predict recurrence
Long-Term Function After Intralesional Curettage
- Single-unit retrospective review of 53 histologically proven chondroblastomas treated by intralesional curettage (1974-2000)
- Local recurrence in 7 patients (13.2%) over follow-up of 2 to 27 years
- Three recurrences controlled by repeat curettage; two required endoprosthesis and two below-knee amputation
- One patient had rare malignant metastasising chondroblastoma and died
- Mean Musculoskeletal Tumour Society functional score 94.2% in survivors