Malignant Cartilage Tumor | Second Most Common Primary Bone Malignancy | Variable Biological Behavior
- Resistant to chemotherapy and radiotherapy - surgery is the only curative treatment
- Histological grade is the most important prognostic factor determining survival
- Distinguishing low-grade chondrosarcoma from enchondroma is challenging clinically and histologically
- Pelvis and proximal femur are most common sites - central (medullary) subtype predominates
- Pain in a previously asymptomatic cartilage lesion suggests malignant transformation
- “Chondrosarcoma is radio-resistant and chemo-resistant - wide surgical resection is mandatory
- “Pathological fracture is rare but indicates aggressive biology
- “Dedifferentiated chondrosarcoma has biphasic pattern: low-grade cartilage plus high-grade sarcoma
- “Pelvic chondrosarcomas have worse prognosis due to late presentation and difficulty achieving wide margins
Surgical resection is the ONLY curative treatment. Chondrosarcoma is notoriously resistant to both chemotherapy and radiotherapy. Wide margins are essential.
Histological grade determines survival. Grade I has 90% 10-year survival, Grade III only 29%. Grading is challenging - requires adequate tissue and expert pathology.
Distinction is notoriously difficult. Pain, size greater than 5cm, endosteal scalloping greater than two-thirds cortical thickness, and uptake on bone scan suggest malignancy.
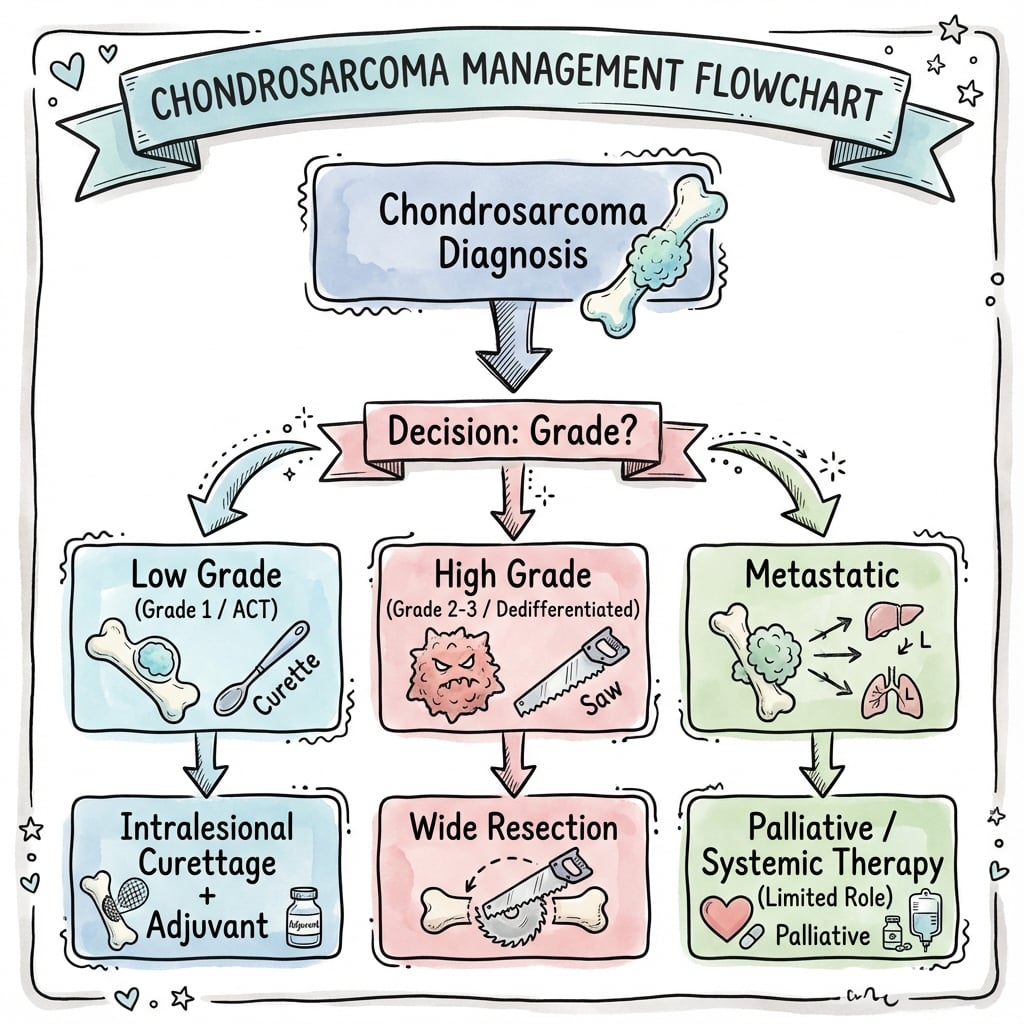
Worst prognosis subtype. Biphasic tumor with low-grade cartilage component plus high-grade non-cartilaginous sarcoma. Treated as high-grade sarcoma with neoadjuvant chemotherapy.
Overview and Epidemiology
Chondrosarcoma is a malignant tumor characterized by the production of cartilaginous matrix by neoplastic cells. It is the second most common primary malignant bone tumor after osteosarcoma, accounting for approximately 20% of all primary bone malignancies. The annual incidence is approximately 1 per million population.
Chondrosarcoma represents a unique challenge in orthopaedic oncology because it is resistant to both chemotherapy and radiotherapy, making surgical resection the only curative option. The difficulty in distinguishing low-grade chondrosarcoma from benign enchondroma creates diagnostic and treatment dilemmas. Histological grading is the most important prognostic factor.
- Peak age: 50-70 years (conventional type)
- Gender: Male predominance (2:1 ratio)
- Clear cell and mesenchymal: Younger patients (20-40 years)
- Rare in children: Under 1% of cases
- Pelvis: 30-40% (most common site)
- Proximal femur: 20-30%
- Ribs and scapula: 10-15%
- Proximal humerus: 10%
- Rare: Hands and feet (unlike enchondroma)
Pathophysiology and Mechanisms
Cartilage Tumor Biology
Chondrosarcoma arises from malignant transformation of chondrocytes. Understanding cartilage biology explains the treatment resistance of these tumors.
Avascular tissue - primary reason for chemotherapy and radiotherapy resistance:
- No blood vessels penetrate cartilage matrix
- Poor drug delivery to tumor cells
- Hypoxic environment reduces radiotherapy efficacy
- Drug resistance proteins highly expressed
- Low mitotic rate: Especially Grade I lesions
- Abundant matrix production: Proteoglycans, collagen type II
- Low metabolic activity: Contributes to imaging patterns
- Lobulated architecture: Tumor nodules separated by fibrous septa
The avascular nature of cartilage matrix creates a physical barrier to chemotherapy drug delivery. Even high-grade dedifferentiated chondrosarcomas receive chemotherapy for the NON-cartilaginous high-grade component, not the cartilage component itself.
Common Anatomic Sites and Biological Behavior
- Frequency
- 30-40%
- Typical Grade
- Grade II-III
- Challenges
- Late presentation, difficult margins, higher recurrence
- Frequency
- 20-30%
- Typical Grade
- Grade I-II
- Challenges
- Reconstruction challenges, risk to neurovascular bundle
- Frequency
- 10-15%
- Typical Grade
- Grade I-II
- Challenges
- Chest wall resection, respiratory compromise
- Frequency
- 10%
- Typical Grade
- Grade I-II
- Challenges
- Brachial plexus proximity, rotator cuff sacrifice
The second route to chondrosarcoma is malignant transformation of an osteochondroma into a secondary peripheral chondrosarcoma (distinct from the central tumours arising from enchondroma). The risk is low for a solitary osteochondroma (under about 1%) but substantially higher in Multiple Hereditary Exostoses (MHE / hereditary multiple osteochondromas, EXT1/EXT2), particularly for central lesions (pelvis, scapula, proximal femur). The single most useful warning sign is the cartilage cap thickness on MRI: a benign cap is thin (a few millimetres in a mature skeleton), whereas a cap thicker than about 1.5-2 cm in a skeletally mature patient strongly suggests transformation — alongside new pain, continued growth after skeletal maturity, and a soft-tissue mass. Biologically these peripheral tumours differ from central chondrosarcoma in that they are IDH-wild-type (the IDH mutation defines central, not peripheral, cartilage tumours). The exam point: in any osteochondroma — especially in MHE — growth or pain after skeletal maturity plus a thick cartilage cap means biopsy/excision, not reassurance.
Classification Systems
Histological Grading System
Histological grading is the most important prognostic factor for chondrosarcoma, directly correlating with survival, metastatic potential, and local recurrence risk.

- Cellularity
- Mildly increased
- Nuclear Features
- Minimal atypia, small nuclei
- Mitoses
- Absent to rare
- 10-Year Survival
- 90%
- Cellularity
- Moderately increased
- Nuclear Features
- Moderate atypia, enlarged nuclei
- Mitoses
- Occasional
- 10-Year Survival
- 81%
- Cellularity
- Markedly increased
- Nuclear Features
- Severe atypia, pleomorphic
- Mitoses
- Frequent
- 10-Year Survival
- 29%
Adequate tissue sampling is critical. Needle biopsy may sample only low-grade areas in a heterogeneous tumor. Up to 10% of tumors show grade progression in different areas. Central core needle biopsy should target the most aggressive-appearing area on imaging (highest T2 signal, cortical destruction, soft tissue mass).
Chondrosarcoma Subtypes
Central (Conventional) Chondrosarcoma
Most common subtype (85%) arising from medullary cavity.
- Arises de novo (75%) or from enchondroma (25%)
- Peak age: 50-70 years
- Pelvis and proximal long bones
- Lobulated hyaline cartilage matrix
- Central medullary lesion
- Rings and arcs calcification pattern
- Endosteal scalloping (greater than two-thirds suggests malignancy)
- Soft tissue mass in higher grades
Primary vs Secondary:
- Primary: Arises de novo in previously normal bone (75%)
- Secondary: Malignant transformation of enchondroma (25%) or osteochondroma (rare)
Secondary chondrosarcomas should be suspected when a long-standing asymptomatic cartilage lesion becomes painful or enlarges.
Central chondrosarcoma can arise from an enchondroma, and that risk is dramatically increased in the enchondromatosis syndromes. Ollier disease is multiple enchondromatosis — numerous enchondromas, typically asymmetric and limb-predominant, often causing deformity and limb-length discrepancy. Maffucci syndrome is enchondromatosis plus soft-tissue spindle-cell haemangiomas (look for the bluish subcutaneous nodules and phleboliths). Both are non-hereditary, sporadic conditions caused by somatic mosaic IDH1/IDH2 mutations (the same mutation that defines central cartilage tumours). The crucial point is malignant transformation: the lifetime risk of chondrosarcoma is high in Ollier (around 25-30%, higher with axial/pelvic disease) and even higher in Maffucci, which additionally carries a markedly raised risk of other (visceral, CNS, ovarian) malignancies. These patients therefore need lifelong surveillance, and any enchondroma that becomes painful, enlarges or develops aggressive imaging features must be assumed malignant until proven otherwise.
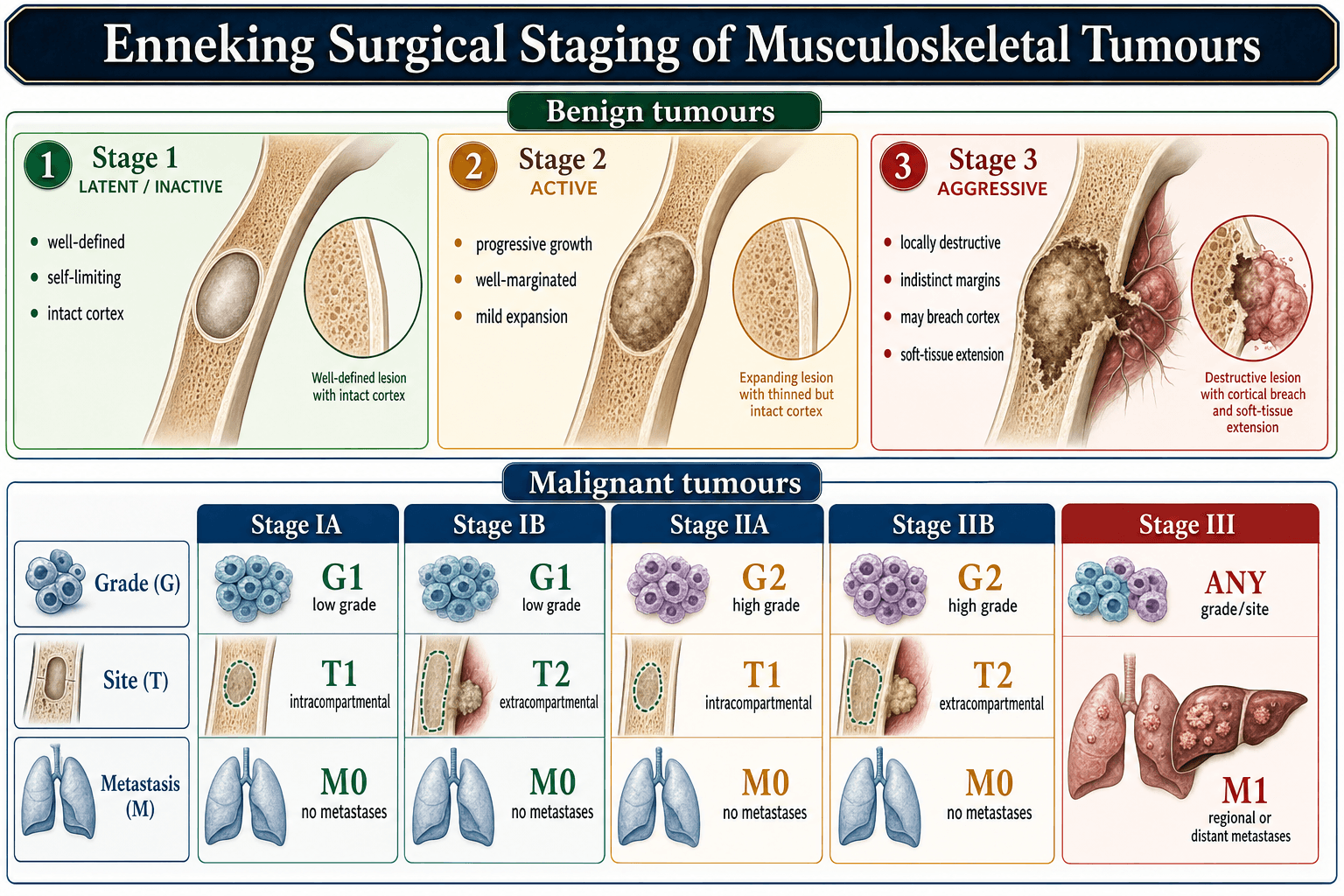
Staging
Enneking Surgical Staging System
Chondrosarcoma is staged using the Enneking staging system for musculoskeletal sarcomas.
- Grade
- Low (G1)
- Site
- Intracompartmental (T1)
- Metastases
- None (M0)
- 5-Year Survival
- Greater than 90%
- Grade
- Low (G1)
- Site
- Extracompartmental (T2)
- Metastases
- None (M0)
- 5-Year Survival
- 80-90%
- Grade
- High (G2-G3)
- Site
- Intracompartmental (T1)
- Metastases
- None (M0)
- 5-Year Survival
- 50-70%
- Grade
- High (G2-G3)
- Site
- Extracompartmental (T2)
- Metastases
- None (M0)
- 5-Year Survival
- 30-50%
- Grade
- Any
- Site
- Any
- Metastases
- Present (M1)
- 5-Year Survival
- Under 20%
Compartmental status:
- Intracompartmental (T1): Confined within bone cortex or within a single anatomic compartment
- Extracompartmental (T2): Extends beyond cortex into soft tissues or crosses major fascial planes
Clinical Presentation
- Pain: Dull, aching (70-80% of patients)
- Mass: Palpable swelling (50%)
- Pathological fracture: Rare (5-10%) but indicates aggressive biology
- Incidental finding: Asymptomatic lesion on imaging
- Slow progression: Months to years typical
- Pain in enchondroma: Suspect malignant transformation
- Rapid onset symptoms: Higher-grade lesions
- Pelvic lesions: Late presentation due to deep location
Distinguish enchondroma from chondrosarcoma:
- New pain in a previously asymptomatic cartilage lesion
- Progressive pain despite conservative treatment
- Lesion size greater than 5cm
- Axial skeleton or proximal long bone location (enchondromas favor hands)
- Cortical destruction or soft tissue mass
- Age over 40 years with new cartilage lesion
Physical Examination
- Palpable mass: Firm, deep, fixed to bone
- Tenderness: Over lesion site
- Range of motion: May be restricted if juxta-articular
- Pathological fracture: Deformity, crepitus (rare)
- General condition: Usually well (not systemically unwell)
- Lymph nodes: Not typically involved
- Chest examination: Metastases rare at presentation
- Neurovascular status: Assess for compression
Investigations and Imaging
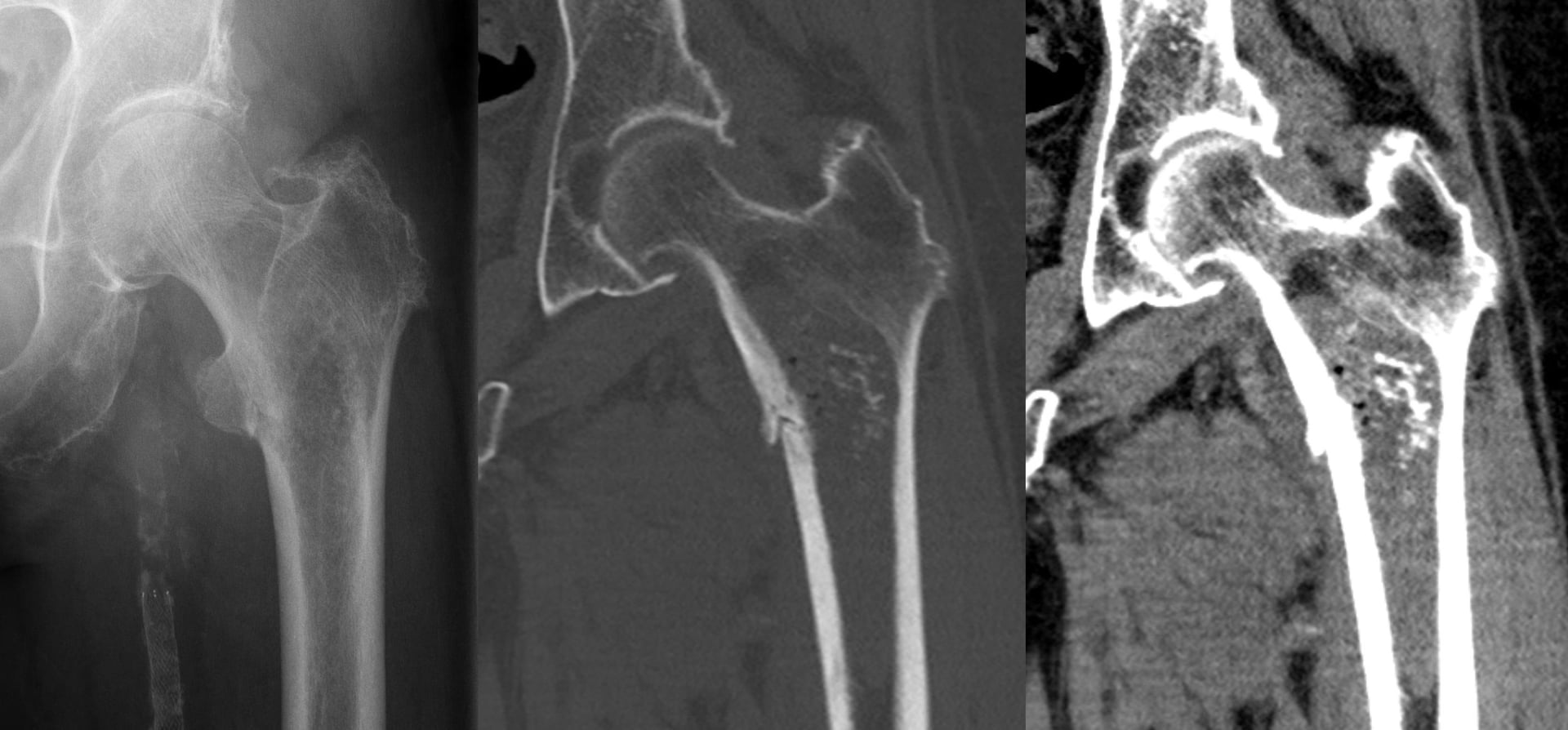
Diagnostic Imaging Protocol
Essential initial investigation. Two orthogonal views of entire bone.
- Matrix: Rings and arcs calcification (popcorn pattern)
- Endosteal scalloping: Greater than two-thirds cortical thickness suggests malignancy
- Cortical destruction: Higher grades
- Soft tissue mass: Mineralized in higher grades
- Pathological fracture: Rare but indicates aggressive biology
Metaphyseal or diaphyseal (central type), epiphyseal (clear cell).
Gold standard for local staging. MRI of entire bone with joint above and below.
- T1: Low signal (cartilage)
- T2/STIR: High signal (lobulated appearance)
- T1 post-contrast: Septal and nodular enhancement
- Extent of medullary involvement
- Cortical destruction and soft tissue extension
- Neurovascular encasement
- Joint invasion (contraindicates limb salvage)
- Skip lesions (rare in chondrosarcoma)
High-resolution for lung metastases (site of 90% of metastases).
- PET-CT: Useful for detecting metastases and assessing grade (higher SUV in high-grade)
- Bone scan: May show uptake (more common in malignant lesions vs enchondroma)
- Skeletal survey: Alternative in pediatric patients
Core needle biopsy preferred (performed by or in consultation with treating surgeon).
Critical biopsy principles:
- Longitudinal approach in line with definitive incision
- Avoid neurovascular structures
- Sample most aggressive area (use imaging to guide - high T2 signal, cortical destruction)
- Adequate tissue: Multiple cores from different areas if heterogeneous
- Frozen section: Not reliable for grading chondrosarcoma
The biopsy tract must be excised en bloc with definitive resection. Poorly planned biopsy can compromise limb salvage surgery. All biopsies should be performed at or in consultation with the sarcoma treatment center.
Imaging Features: Enchondroma vs Chondrosarcoma
- Enchondroma (Benign)
- Hands and feet (60%), asymptomatic
- Chondrosarcoma (Malignant)
- Pelvis, proximal femur, ribs (axial skeleton)
- Enchondroma (Benign)
- Usually under 3-4cm
- Chondrosarcoma (Malignant)
- Often greater than 5cm
- Enchondroma (Benign)
- Absent (unless pathological fracture)
- Chondrosarcoma (Malignant)
- Present in 70-80% (dull, aching)
- Enchondroma (Benign)
- Less than one-third cortical thickness
- Chondrosarcoma (Malignant)
- Greater than two-thirds cortical thickness
- Enchondroma (Benign)
- Intact or mildly thinned
- Chondrosarcoma (Malignant)
- Destroyed or breached (higher grades)
- Enchondroma (Benign)
- Absent
- Chondrosarcoma (Malignant)
- Present in Grade II-III
- Enchondroma (Benign)
- No uptake or minimal
- Chondrosarcoma (Malignant)
- Uptake present (more intense in higher grades)
- Enchondroma (Benign)
- Lobulated high signal, thin septa
- Chondrosarcoma (Malignant)
- Thick irregular septa, nodular soft tissue component
Differential Diagnosis
- Key Distinguishing Features
- Hands/feet, asymptomatic, small (under 3-4cm), scalloping under one-third cortex, no soft tissue mass
- Discriminator
- Painless, peripheral, IDH-mutant but no aggressive features
- Key Distinguishing Features
- Epiphyseal, skeletally immature patient, painful, fine matrix, H3K36M mutation
- Discriminator
- Younger age and epiphyseal location overlap with clear cell subtype
- Key Distinguishing Features
- Surface lesion, marrow/cortex continuity; cap over 1.5-2cm or growth after skeletal maturity suggests secondary peripheral chondrosarcoma
- Discriminator
- Cartilage cap thickness on MRI is the key alarm sign
- Key Distinguishing Features
- Younger patient, aggressive periosteal reaction, malignant osteoid, more lytic/permeative
- Discriminator
- Tumour osteoid production and IDH wild-type
- Key Distinguishing Features
- Serpentine sclerotic rim, no endosteal scalloping, no soft tissue mass, often asymptomatic
- Discriminator
- Lacks deep scalloping and aggressive features
- Key Distinguishing Features
- Sacrum/clivus, midline, lytic with soft tissue mass, brachyury positive
- Discriminator
- Midline axial location and immunoprofile
Management
Surgery is the ONLY curative treatment for chondrosarcoma. Unlike osteosarcoma and Ewing sarcoma, conventional chondrosarcoma is resistant to both chemotherapy and radiotherapy. Wide surgical resection with negative margins is essential.
Treatment Algorithm by Grade and Location
Grade I Chondrosarcoma Management
Goals: Wide local excision with negative margins while preserving function.
Treatment Steps
- MRI of entire bone
- CT chest for staging
- Consider PET-CT if diagnosis uncertain
- Intralesional curettage is CONTRAINDICATED (high recurrence)
- Wide resection with 1-2cm margin
- Limb salvage usually achievable
- Reconstruction: Allograft, endoprosthesis, or arthrodesis
- No chemotherapy (ineffective)
- No radiotherapy unless unresectable with positive margins
- Close surveillance for recurrence
- Years 1-2: Every 3-4 months (chest X-ray, local imaging)
- Years 3-5: Every 6 months
- Beyond 5 years: Annually (late recurrences possible)
Even Grade I (low-grade) chondrosarcoma requires wide resection, not curettage. Intralesional treatment has recurrence rates of 50-90%. Some surgeons advocate observation alone for small (under 3cm) asymptomatic Grade I lesions in expendable bones, but this is controversial.
Surgical Technique Principles
Surgical Technique
Preoperative Planning
- MRI entire bone: Determine extent, soft tissue involvement
- CT for bony anatomy: Assess cortical destruction, plan osteotomy levels
- Angiography: Consider for pelvic lesions (preoperative embolization)
- 3D reconstruction: Essential for complex pelvic resections
- Margin planning: 1-2cm for Grade I, 2-3cm for higher grades
- Biopsy tract excision: Plan en bloc excision of tract
- Reconstruction strategy: Endoprosthesis, allograft, or arthrodesis
- Blood products: Type and cross 4-6 units (more for pelvic resections)
Intraoperative frozen section is UNRELIABLE for assessing margins in chondrosarcoma. Cartilage matrix is difficult to section, and distinguishing normal from Grade I chondrosarcoma is challenging even on permanent sections. Plan adequate margins based on preoperative imaging.
Complications
Surgical Complications
- Incidence
- 10% (negative margins) to 40-60% (positive margins)
- Risk Factors
- Positive margins, high grade, inadequate resection
- Management
- Re-resection if feasible, amputation for failed limb salvage
- Incidence
- 5-15% (higher for pelvic resections)
- Risk Factors
- Massive reconstruction, pelvic surgery, diabetes
- Management
- Antibiotics, debridement, implant retention if possible
- Incidence
- 5-10%
- Risk Factors
- Pelvic location, tumor encasement
- Management
- Intraoperative recognition and repair, accept deficit if planned sacrifice
- Incidence
- 5-10% for endoprosthesis
- Risk Factors
- Abductor sacrifice, large head size, patient factors
- Management
- Closed reduction, constrained liner, revision if recurrent
- Incidence
- 15-20% at 10 years
- Risk Factors
- High-impact activities, slow incorporation, osteoporosis
- Management
- Protected weight-bearing initially, ORIF if fracture occurs
- Incidence
- 10% (Grade I) to 70% (Grade III)
- Risk Factors
- High grade, positive margins, local recurrence
- Management
- Surveillance CT chest, metastasectomy if resectable oligometastatic disease
Local recurrence is the most common cause of treatment failure. Most recurrences (70%) occur within first 3 years, but late recurrences beyond 5 years are possible. Inadequate surgical margins are the primary cause. Positive margin re-resection should be strongly considered.
Postoperative Care and Rehabilitation
Postoperative Rehabilitation After Endoprosthetic Reconstruction
Rehabilitation Timeline
Goals: Pain control, prevent complications
- DVT prophylaxis (LMWH for 6 weeks)
- Wound drain management (remove when output under 30ml per 24 hours)
- Mobilize day 1-2 with physiotherapy
- Hip precautions if proximal femoral replacement (no flexion over 90 degrees)
Weight-bearing: Immediate weight-bearing as tolerated (endoprosthesis provides immediate stability)
- Gait training with walking aids
- ROM exercises within precautions
- Wound healing (sutures removed 2-3 weeks)
- Monitor for infection, dislocation
Goals: Restore functional independence
- Wean walking aids as strength improves
- Progressive resistance exercises
- Return to ADLs (driving at 6-8 weeks if safe)
- No high-impact activities (running, jumping - lifelong)
Surveillance and monitoring:
- Maintain muscle strength and joint ROM
- Annual prosthesis surveillance (X-ray for loosening, wear)
- Low-impact activities encouraged (swimming, cycling)
- Lifelong activity modifications (avoid high-impact sports)
Surveillance Protocol
Every 3 months:
- Clinical examination
- Chest X-ray (PA and lateral)
- Local imaging (X-ray or MRI)
- 70% of recurrences occur within first 3 years
Every 6 months:
- Clinical examination
- Chest X-ray
- Local imaging
- CT chest if concerning findings
Annually:
- Clinical examination
- Chest X-ray
- Local imaging
- Late recurrences possible - lifelong surveillance
Annual X-rays:
- Endoprosthesis: Loosening, wear, subsidence
- Allograft: Fracture, nonunion, collapse
- Earlier imaging if pain or functional decline
Role of Radiotherapy
Chondrosarcoma is radio-resistant. Radiotherapy is NOT standard treatment.
Consider radiotherapy only for:
- Unresectable tumors (skull base, axial spine)
- Positive margins when re-resection not feasible
- Palliation of metastases
- Proton beam therapy (skull base lesions)
- Carbon ion radiotherapy (emerging)
- Dose: 60-70 Gy conventional, 70-80 CGE proton
Limited efficacy, local control under 50%
Prognosis and Outcomes
Prognostic Factors
- Favorable Prognosis
- Grade I (low-grade)
- Unfavorable Prognosis
- Grade III or dedifferentiated
- Favorable Prognosis
- Appendicular skeleton (extremities)
- Unfavorable Prognosis
- Axial skeleton (pelvis, spine, ribs)
- Favorable Prognosis
- Wide negative margins (greater than 2cm)
- Unfavorable Prognosis
- Intralesional or positive margins
- Favorable Prognosis
- Less than 5cm
- Unfavorable Prognosis
- Greater than 10cm
- Favorable Prognosis
- Under 40 years
- Unfavorable Prognosis
- Over 60 years
- Favorable Prognosis
- None (M0)
- Unfavorable Prognosis
- Present (M1) - lungs, bone
- Favorable Prognosis
- Periosteal or clear cell
- Unfavorable Prognosis
- Dedifferentiated or mesenchymal
Histological grade is the single most important prognostic factor for chondrosarcoma, more important than size or anatomic location. Grade I has 90% 10-year survival vs Grade III 29%. This emphasizes the critical importance of adequate biopsy tissue for accurate grading.
Metastatic Disease and Recurrence
- Lungs: 90% of metastases
- Bone: 10% (especially with higher grades)
- Late metastases: Can occur 5-10 years after resection
- Metastatic rate: 10% (Grade I), 30% (Grade II), 70% (Grade III)
- Adequate margins: 10% recurrence
- Marginal/positive margins: 40-60% recurrence
- Time to recurrence: Average 2-3 years (range: 6 months to 10 years)
- Management: Re-resection if feasible, amputation if limb salvage fails
Survival by Grade
- 5-Year Survival
- 90-95%
- 10-Year Survival
- 90%
- Metastatic Rate
- 5-10%
- 5-Year Survival
- 70-85%
- 10-Year Survival
- 81%
- Metastatic Rate
- 25-30%
- 5-Year Survival
- 35-55%
- 10-Year Survival
- 29%
- Metastatic Rate
- 70-75%
- 5-Year Survival
- 10-25%
- 10-Year Survival
- Under 10%
- Metastatic Rate
- Over 90%
Guidelines, Registries & Global Practice
Global Epidemiology
Chondrosarcoma is the most common primary bone sarcoma in adults and the second most common primary bone malignancy overall (after osteosarcoma), with an annual incidence of roughly 1 per million population worldwide. Population-based registry data (SEER) confirm a steep prognostic gradient by subtype: median survival ranges from around 97 months for juxtacortical lesions down to only about 11 months for dedifferentiated tumours, with metastatic disease at diagnosis the dominant independent predictor of death across all subtypes (Amer et al., J Orthop Res 2020 — PMID 31498474).
- Region
- Europe
- Core Recommendation
- Refer to a bone-sarcoma reference centre before biopsy; en bloc wide resection; no routine chemo/radiotherapy for conventional chondrosarcoma
- Evidence Basis
- Expert consensus, registry and cohort data
- Region
- UK
- Core Recommendation
- Mandatory specialist-centre management and sarcoma MDT; suspected bone tumour referral pathway; surgery is primary treatment
- Evidence Basis
- Guideline + service-configuration evidence
- Region
- USA
- Core Recommendation
- Wide excision for resectable disease; consider particle (proton/carbon-ion) RT for unresectable/axial; chemo only for mesenchymal and dedifferentiated subtypes
- Evidence Basis
- Category 2A consensus
- Region
- Global
- Core Recommendation
- Atypical cartilaginous tumour (ACT) terminology for grade-1 appendicular lesions; reserve 'chondrosarcoma' grade 1 for axial sites
- Evidence Basis
- Molecular + histological consensus
All chondrosarcomas should be managed at a designated bone-sarcoma reference centre and discussed at a sarcoma MDT BEFORE biopsy. This is a near-universal principle across guidelines (ESMO, NICE/BOA, NCCN).
- Poorly planned biopsy contaminates tissue planes and compromises limb salvage
- Reference-centre care is independently associated with better local control and survival
- National sarcoma networks (e.g. UK sarcoma MDTs, European EURACAN/EMSOS centres, US NCI-designated centres) coordinate rare-tumour care
Because chondrosarcoma is rare, most high-quality outcome data come from bone-tumour registries and multi-institutional collaboratives, not RCTs:
- EMSOS (European Musculo-Skeletal Oncology Society) - source of the 337-patient dedifferentiated series
- SEER (USA) - population-level subtype survival benchmarks
- National bone-sarcoma registries contribute to international collaborative trials
Practice Variation
- Variation
- Many centres now use intralesional curettage plus local adjuvant; others retain wide resection
- Rationale
- Low metastatic risk and good local control with curettage in expendable appendicular sites; axial lesions still need wide resection
- Variation
- Available in select European, Japanese and US centres; absent in many regions
- Rationale
- High-dose particle RT improves local control in unresectable skull-base/axial disease but is resource-intensive
- Variation
- Higher rates of amputation and late presentation; limb salvage less available
- Rationale
- Limited access to imaging, endoprostheses, allograft banks and specialist MDTs
Key documentation and consent points:
- Diagnosis delay litigation: Pain in cartilage lesion requires investigation - document imaging and biopsy decisions
- Biopsy tract contamination: Document MDT discussion and biopsy planning by sarcoma surgeon
- Margin status: Intraoperative frozen sections, document decision-making if margins compromised
- Amputation consent: Discuss possibility of amputation before limb salvage surgery if margins cannot be achieved
- Prognosis discussion: Document discussion of grade-specific survival rates
- Surveillance protocol: Provide written follow-up schedule and emphasize importance of compliance
Multidisciplinary Team Composition
Essential members:
- Orthopaedic oncologist (surgeon)
- Medical oncologist
- Radiation oncologist
- Musculoskeletal radiologist
- Musculoskeletal pathologist
- Specialist oncology nurse
- Physiotherapist, occupational therapist
- Psychologist, social worker
MCQ Practice Points
Q: Which statement about chondrosarcoma epidemiology is correct? A: Chondrosarcoma accounts for 20% of primary bone malignancies, making it the second most common after osteosarcoma. Peak age is 50-70 years with male predominance 2:1. Most common sites are pelvis (30-40%) and proximal femur (20-30%).
Q: What is the most important prognostic factor in chondrosarcoma? A: Histological grade is the single most important prognostic factor. Grade I has 90% 10-year survival, Grade II 81%, Grade III 29%. Grade is more important than size or anatomic location in determining prognosis.
Q: Why is chemotherapy not used for conventional chondrosarcoma? A: Conventional chondrosarcoma is resistant to both chemotherapy and radiotherapy due to poor vascularity of cartilage matrix and low cell turnover. Wide surgical resection is the ONLY curative treatment. Exception: Dedifferentiated and mesenchymal subtypes receive chemotherapy.
Q: Which chondrosarcoma subtype has the worst prognosis? A: Dedifferentiated chondrosarcoma has the worst prognosis with only 7-24% 5-year survival. It shows biphasic pattern: low-grade cartilage plus high-grade non-cartilaginous sarcoma. Treated with neoadjuvant chemotherapy unlike conventional chondrosarcoma.
Q: What imaging features help distinguish chondrosarcoma from enchondroma? A: Features suggesting malignancy (PEST mnemonic): Pain, Endosteal scalloping greater than two-thirds cortical thickness, Size greater than 5cm, Tracer uptake on bone scan or PET. Also: axial skeleton location, soft tissue mass, and age over 40 years.
Q: What is the local recurrence rate with positive margins after chondrosarcoma resection? A: Positive margins increase local recurrence from under 10% (negative margins) to 40-60% (positive margins). Margin status is the most important surgical factor for local control. Re-resection should be considered if anatomically feasible.
At a Glance
Chondrosarcoma is the second most common primary bone malignancy (20%), characterized by malignant cartilage formation. It is resistant to chemotherapy and radiotherapy - wide surgical resection is the ONLY curative treatment. Histological grading (I-III) is the most important prognostic factor: Grade I has 90% 10-year survival while Grade III drops to 29%. The pelvis and proximal femur are most common sites. Key diagnostic challenge: distinguishing low-grade chondrosarcoma from benign enchondroma - pain, size greater than 5cm, and endosteal scalloping greater than two-thirds cortical thickness suggest malignancy. Dedifferentiated chondrosarcoma (biphasic: low-grade cartilage plus high-grade sarcoma) has worst prognosis.
- Grade
- Grade I (well-differentiated)
- Surgery
- Wide resection with margins
- Prognosis
- 90% 10-year survival, excellent
- Grade
- Grade II (intermediate)
- Surgery
- Wide resection, consider adjuvant if margin close
- Prognosis
- 81% 10-year survival, good
- Grade
- Grade III (poorly differentiated)
- Surgery
- Wide resection, consider chemotherapy
- Prognosis
- 29% 10-year survival, poor
- Grade
- Dedifferentiated (biphasic)
- Surgery
- Wide resection plus neoadjuvant chemotherapy
- Prognosis
- 7-24% 5-year survival, very poor
PUFFChondrosarcoma Anatomical Distribution
Hook:Chondrosarcoma goes for the PUFF - Pelvis and pUoximal femur are favorite sites, unlike enchondroma which prefers hands!
PESTFeatures Suggesting Malignancy (Enchondroma vs Chondrosarcoma)
Hook:When an enchondroma becomes a PEST (painful, eroding, sizable, and tracer-positive), suspect chondrosarcoma!
CCPM-DChondrosarcoma Subtypes
Hook:CCPM-D covers Central (common), Clear cell (epiphysis), Periosteal (surface), Mesenchymal (young), and Dedifferentiated (deadly)!
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 55-year-old man presents with mild thigh pain for 6 months. X-ray shows a 6cm lobulated lesion in the proximal femoral metaphysis with rings and arcs calcification and endosteal scalloping involving two-thirds of the cortical thickness. What is your assessment and management?”
“A 65-year-old woman presents with severe hip pain and a large palpable mass. Imaging shows a large pelvic mass with two components: a mineralized chondroid lesion in the ilium plus an adjacent non-mineralized aggressive soft tissue mass. Biopsy shows low-grade cartilage with areas of high-grade pleomorphic sarcoma. What is your diagnosis and management?”
“You have resected a Grade II chondrosarcoma of the distal femur with endoprosthetic reconstruction. Final pathology reports positive margins posteriorly where tumor abuts the popliteal vessels. How do you manage this?”
Key Pathology
- Second most common primary bone malignancy (20%)
- Malignant cartilage-forming tumor - rings and arcs calcification
- Histological grade is most important prognostic factor
- Grade I: 90% 10-year survival, Grade III: 29%
- Conventional type 85%, dedifferentiated worst prognosis (7-24% 5-year survival)
Clinical Presentation
- Pain in cartilage lesion (70-80%) - key symptom
- Pelvis 30-40%, proximal femur 20-30% - central (medullary) subtype
- Peak age 50-70 years, male predominance 2:1
- PEST features suggest malignancy: Pain, Endosteal scalloping, Size greater than 5cm, Tracer uptake
Imaging Protocol
- X-ray: Rings and arcs calcification, endosteal scalloping greater than two-thirds
- MRI entire bone: T2 high signal lobulated, assess extent and soft tissue invasion
- CT chest: Staging for lung metastases (90% of metastases)
- Core needle biopsy: Adequate tissue from most aggressive area (high T2, cortical destruction)
Treatment Principles
- Surgery is ONLY curative treatment - chemo-resistant and radio-resistant
- Wide resection with 1-2cm margins - intralesional curettage contraindicated
- Positive margins: 40-60% recurrence vs negative margins under 10%
- Dedifferentiated type: ONLY subtype receiving chemotherapy (neoadjuvant)
- Radiotherapy: Only for unresectable or positive margins (60-70 Gy)
Prognostic Factors
- Histological grade: Most important factor (Grade I 90%, Grade III 29% 10-year survival)
- Anatomic site: Pelvic worse than appendicular (30-60% vs 70-90% 5-year survival)
- Margin status: Negative margins essential (positive margins increase recurrence 10% to 40-60%)
- Subtypes: Periosteal best, dedifferentiated worst prognosis
Evidence Base and Key Studies
Prognostic Factors in Chondrosarcoma of Bone: A Clinicopathologic Analysis with Emphasis on Histologic Grading
- Landmark study establishing the 3-tier histological grading system for chondrosarcoma
- Grading based on cellularity, nuclear size, nuclear staining (hyperchromasia) and mitotic activity
- Grade correlated strongly with metastasis and survival across the cohort
- Histological grade emerged as the dominant prognostic factor for chondrosarcoma
Chondrosarcoma of Bone: An Assessment of Outcome
- 227 patients (Massachusetts General Hospital), mean follow-up 6 years (range 3-25 years)
- Most common sites: femur (78), pelvis (51), humerus (39); mean age 47 years
- High-grade lesions older and showed more pathological fracture, metastasis, recurrence and death (all p less than 0.001)
- Predictors of metastasis/death: local recurrence, pelvic location, size over 100cm cubed, aneuploidy, grade 3 and dedifferentiation
- Wide margins (outside reactive zone) gave longer survival than marginal or intralesional resection (p less than 0.04)
Dedifferentiated Chondrosarcoma: Prognostic Factors and Outcome from a European Group
- EMSOS multicentre study of 337 dedifferentiated chondrosarcomas from nine European centres
- Overall 5-year survival only 24%; for the 266 non-metastatic patients, 10-year survival was 28%
- 21% had metastases at diagnosis (median survival 5 months)
- Poor prognostic factors: pathological fracture, pelvic location, increasing age and inadequate margins
- Chemotherapy did NOT significantly improve survival in this series
Risk Factors for Survival and Local Control in Chondrosarcoma of Bone
- 153 patients with non-metastatic chondrosarcoma (52 axial, 101 appendicular), minimum 5-year follow-up
- Cumulative survival 70% at 10 years and 63% at 15 years
- Independent risk factors for death: extracompartmental spread, local recurrence and high histological grade
- Independent risk factors for local recurrence: inadequate surgical margins and size greater than 10cm
- Tumour location, type of surgery and symptom duration were NOT independently prognostic
Clear Cell Chondrosarcoma of Bone: Observations in 47 Cases
- 47 clear cell chondrosarcomas from the Mayo Clinic - the defining series for this subtype
- Low-grade tumour with predilection for the ends of long bones, especially the proximal femur
- Male predominance (2.6:1); most patients in the third and fourth decades
- Frequently mimics benign tumours (e.g. chondroblastoma) causing diagnostic difficulty
- Overall mortality 15%; en bloc resection with a margin of normal bone is the treatment of choice
IDH1 and IDH2 Mutations are Frequent Events in Central Chondrosarcoma and Central/Periosteal Chondromas but Not Other Mesenchymal Tumours
- Screened approximately 1200 mesenchymal tumours including 220 cartilaginous tumours
- IDH1/IDH2 mutations found in at least 56% of central and periosteal cartilaginous tumours
- Mutations span the spectrum from enchondroma through conventional central to dedifferentiated chondrosarcoma
- No IDH mutations in peripheral chondrosarcoma or osteochondroma - a key biological distinction
- The mutations generate the oncometabolite 2-hydroxyglutarate and appear early in tumourigenesis
Survival and Prognosis of Chondrosarcoma Subtypes: SEER Database Analysis
- Population-based SEER analysis of the five non-conventional chondrosarcoma subtypes
- Rate of metastasis at presentation rose across subtypes: juxtacortical 2.1%, clear cell 5.7%, myxoid 7.6%, mesenchymal 10.6%, dedifferentiated 19.8%
- Median survival: juxtacortical 97 months, clear cell 79, myxoid 60, mesenchymal 33.5, dedifferentiated only 11 months
- Metastatic disease at diagnosis was the consistent independent predictor of poorer survival across subtypes