Second Most Common Entrapment Neuropathy | Ulnar Nerve | Elbow
- Ulnar Nerve Territory: Small finger and ulnar half of ring finger (palmar and dorsal)
- Froment's Sign: Thumb IP flexion when pinching - indicates adductor pollicis weakness
- Wartenberg's Sign: Small finger abduction at rest - indicates weak 3rd palmar interosseous
- Claw Hand: Ring and small finger hyperextension at MCP with IP flexion (ulnar paradox)
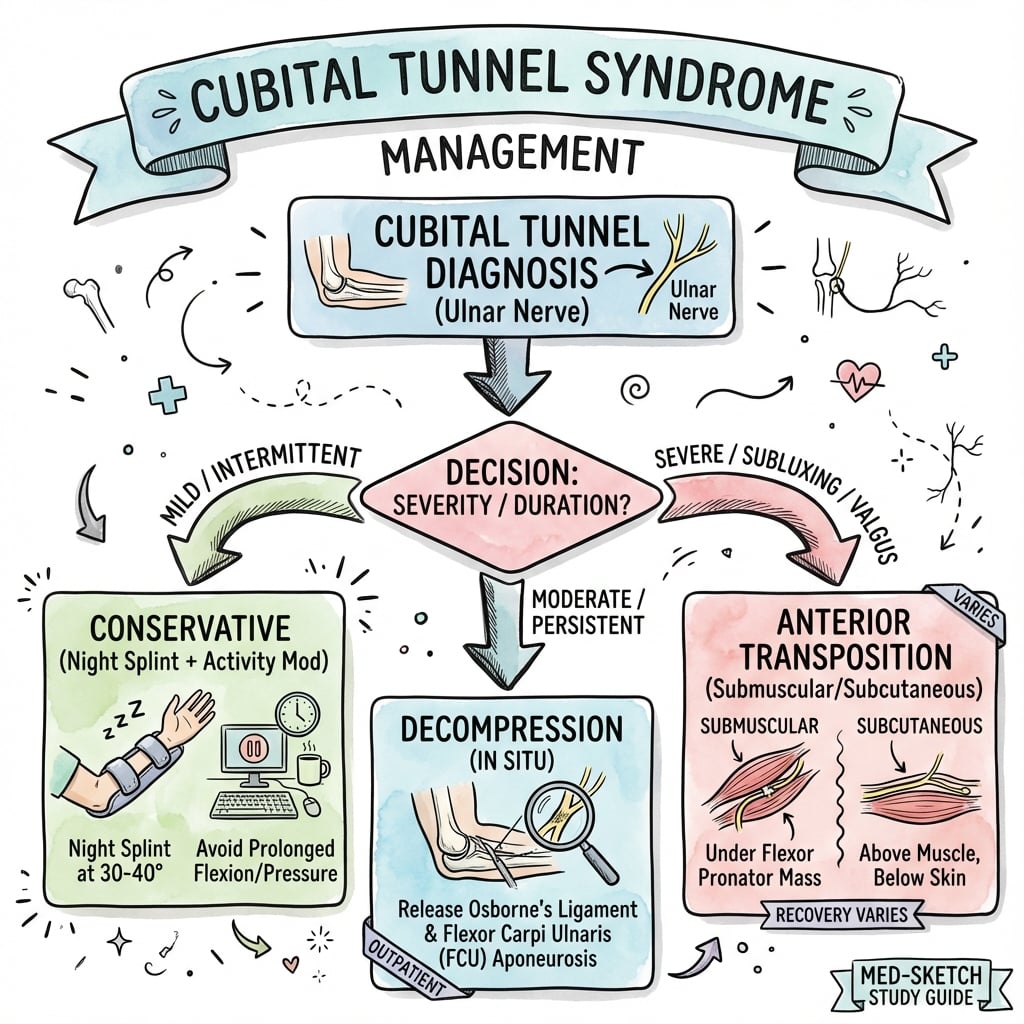
- Surgery Options: In-situ decompression vs anterior transposition - similar outcomes
- “Froment's positive = motor involvement = Grade II+
- “Intrinsic atrophy = urgent surgery, incomplete recovery
- “Elbow flexion test reproduces symptoms
- “Ulnar claw is WORSE with LOW lesion (ulnar paradox)
Thumb IP flexion when pinching paper. Indicates adductor pollicis weakness (ulnar nerve). Uses FPL (median) to compensate.
Small finger abducted at rest. Weak 3rd palmar interosseous cannot adduct small finger. "Catching on pocket" complaint.
Claw WORSE in low lesion. High lesion: FDP paralyzed so less IP flexion. Low lesion: FDP works so more clawing.
May be incomplete if atrophy. Intrinsic muscle recovery depends on duration. Sensory recovers better than motor.
- McGowan Grade
- Grade I
- Treatment
- Conservative: splint, activity modification
- Key Pearl
- Trial for 3 months before surgery
- McGowan Grade
- Grade II
- Treatment
- Consider surgery if fails conservative
- Key Pearl
- Motor involvement = surgical indication
- McGowan Grade
- Grade III
- Treatment
- Urgent surgical decompression
- Key Pearl
- Motor recovery may be incomplete
FOAMCubital Tunnel Compression Sites
Hook:FOAM - Four sites of potential compression from distal to proximal!
Overview and Epidemiology
Cubital tunnel syndrome is the second most common peripheral nerve compression after CTS. Understanding ulnar nerve anatomy, McGowan grading, and surgical options is essential for the exam.
Cubital Tunnel Syndrome is compression of the ulnar nerve at the elbow as it passes between the medial epicondyle and olecranon.
- Male predominance: 2:1 ratio
- Peak age: 30-50 years
- Bilateral: 30% of cases
- Occupational risk: Repetitive elbow flexion, leaning on elbows
Understanding risk factors helps identify at-risk patients.
- Idiopathic: Most common
- Repetitive flexion: Occupational, sleeping with bent elbow
- Direct pressure: Leaning on elbows
- Cubitus valgus: Tardy ulnar palsy post-fracture
- Osteophytes: Elbow arthritis
Screen for underlying causes in all patients.
Pathophysiology and Mechanisms
The cubital tunnel is a fibro-osseous tunnel at the elbow. FLOOR is the MCL and elbow capsule. ROOF is Osborne's ligament (arcuate ligament connecting the two heads of FCU). The ulnar nerve becomes superficial and vulnerable here.
- Proximal: Arcade of Struthers (5-10cm above epicondyle)
- At Tunnel: Between medial epicondyle and olecranon
- Distal: Between two heads of FCU (Osborne's ligament)
- Elbow flexion: Nerve stretches 4-8mm, tunnel narrows 55%
- Nerve excursion: 10mm with full flexion
- Pressure: Increases 6x from extension to flexion
Tardy Ulnar Nerve Palsy (Cubitus Valgus)
"Cubitus valgus / tardy ulnar palsy" is named three times in this topic - as a cause, as an indication for transposition, and in the management algorithm - so it deserves to be developed, because it is the one cubital tunnel presentation where simple in-situ decompression is not the default answer.
What "tardy" means. Tardy ulnar nerve palsy is a delayed ulnar neuropathy that appears months, years, or even decades after an elbow injury in childhood - classically a lateral condyle fracture nonunion/malunion (the commonest cause) or a physeal injury, both of which arrest lateral-column growth and produce a progressive cubitus valgus deformity. As the carrying angle increases, the ulnar nerve is chronically stretched and angulated as it courses behind the medial epicondyle; repeated traction over years, often compounded by friction and subluxation, eventually produces the neuropathy long after the original fracture has been forgotten.
- Idiopathic cubital tunnel
- Compression in the retrocondylar groove / under Osborne's
- Tardy ulnar palsy
- Chronic traction over a valgus elbow
- Idiopathic cubital tunnel
- Often occupational, leaning, repetitive flexion
- Tardy ulnar palsy
- Childhood elbow fracture (lateral condyle), often remote
- Idiopathic cubital tunnel
- Tinel's/flexion test positive, normal carrying angle
- Tardy ulnar palsy
- Increased carrying angle (cubitus valgus), often visible deformity
- Idiopathic cubital tunnel
- Often normal radiographs
- Tardy ulnar palsy
- Lateral condyle nonunion, valgus deformity, sometimes osteophytes
- Idiopathic cubital tunnel
- In-situ decompression first-line
- Tardy ulnar palsy
- Anterior transposition to de-tension the stretched nerve; correct deformity if appropriate
Why transposition, not in-situ release. The problem in tardy palsy is length and tension, not just a tight roof. Decompressing the tunnel in situ leaves the nerve on the stretch behind a valgus elbow, so anterior transposition (moving the nerve in front of the axis of elbow flexion) is preferred because it shortens the nerve's path and relieves the traction. A correctable bony deformity (e.g. a supracondylar/varus-producing osteotomy for the valgus, or addressing a lateral condyle nonunion) is considered alongside the nerve procedure, particularly in younger patients - though deformity correction alone does not reliably reverse an established neuropathy.
If a viva stem gives an ulnar neuropathy plus an increased carrying angle or a history of a childhood lateral condyle fracture, name tardy ulnar nerve palsy explicitly and say you would favour anterior transposition over in-situ decompression - because the lesion is traction over a valgus elbow, not focal compression. This is the classic exception to the "decompression-first" rule that the rest of this topic establishes.
FWCUlnar Nerve Motor Signs
Hook:FWC = Froment's, Wartenberg's, Claw - the three motor signs of ulnar palsy, in order of severity!
HALF PADUlnar Nerve Hand Muscles
Hook:HALF of the hand is paralyzed by ulnar nerve injury - remember HALF PAD!
Classification Systems
McGowan Classification (Modified)
- Symptoms
- Intermittent paresthesias
- Examination
- Normal strength and sensation
- Treatment
- Conservative
- Symptoms
- Intermittent paresthesias
- Examination
- Weakness without atrophy
- Treatment
- Surgery if fails conservative
- Symptoms
- Persistent paresthesias
- Examination
- Weakness without atrophy
- Treatment
- Surgery recommended
- Symptoms
- Persistent symptoms
- Examination
- Intrinsic atrophy
- Treatment
- Urgent surgery
McGowan grading guides treatment decisions.
Clinical Assessment
- Numbness: Small and ulnar ring finger
- Timing: Worse at night, with elbow flexion
- Dropping objects: Weakness of grip
- Phone sign: Numbness holding phone to ear
- Red flags: Rapid progression, severe weakness
Ask about occupation and sleeping position.
- Tinel's: Over cubital tunnel
- Elbow flexion test: 60 seconds sustained flexion
- Froment's sign: IP flexion when pinching
- Wartenberg's sign: Small finger abduction
- Two-point discrimination: Greater than 6mm abnormal
Always compare to contralateral side.
- Technique
- Pinch paper between thumb and index
- Positive Finding
- IP flexion of thumb
- Indicates
- Adductor pollicis weakness
- Technique
- Observe hand at rest
- Positive Finding
- Small finger abducted
- Indicates
- 3rd palmar interosseous weakness
- Technique
- Sustained elbow flexion 60 seconds
- Positive Finding
- Paresthesias reproduced
- Indicates
- Ulnar nerve compression
- Technique
- Resist shoulder external rotation while scratching nerve
- Positive Finding
- Momentary weakness
- Indicates
- Nerve irritability
Consider: C8/T1 radiculopathy, thoracic outlet syndrome, Guyon's canal compression (ulnar tunnel), pancoast tumor. Check for double crush syndrome.

Investigations
Investigation Protocol
Clinical diagnosis in typical presentations with positive Tinel's, elbow flexion test, and motor signs.
Gold standard. Slowing of motor conduction velocity across elbow (less than 50 m/s). Compare to segment above and below.
For severity grading. Denervation potentials in intrinsics (FDI, ADM). Fibrillations indicate axonal loss.
X-ray: Cubitus valgus, osteophytes, prior fracture. MRI: Subluxation, mass lesion, nerve changes.
Management Algorithm
Conservative Management
Conservative Treatment Steps
Avoid prolonged elbow flexion. Ergonomic workplace assessment. Avoid leaning on elbows.
Keep elbow extended at night. Towel wrap or commercial splint. Prevents nocturnal flexion.
Protect nerve from direct pressure. Wear during day if occupational exposure.
Conservative treatment is appropriate for McGowan Grade I with intermittent symptoms only.
Surgical Technique
In-Situ Decompression
Surgical Steps
Supine, arm on table. Elbow flexed 20-30 degrees. Tourniquet optional.
Curved incision between medial epicondyle and olecranon. 6-8cm. Protect medial antebrachial cutaneous nerve.
Identify and protect nerve. Release Osborne's ligament (FCU aponeurosis). Release distally between FCU heads.
Release arcade of Struthers if tight. Release medial intermuscular septum.
Layered closure. Check nerve excursion. No drain required.
In-situ decompression is technically simpler with lower complication rate.

Medial Epicondylectomy: The Third Operation
The evidence base above repeatedly names a third procedure - medial epicondylectomy - yet it is never described in the technique section. It is worth knowing because it occupies the middle ground between in-situ decompression and transposition and is a recurring viva option.
The principle. Rather than moving the nerve, the surgeon removes the bony prominence the nerve is tethered against. After decompressing the tunnel, the medial epicondyle is osteotomised (partial or complete), so the ulnar nerve is free to glide anteriorly on its own during elbow flexion without the formal mobilisation, dissection and potential devascularisation of a transposition. It therefore preserves the nerve's intrinsic blood supply better than transposition while still removing the retrocondylar tether.
- Detail
- Resect the epicondyle so the nerve self-translates anteriorly; no formal transposition
- Detail
- Less nerve mobilisation/devascularisation than transposition; addresses subluxation by removing the point it catches on
- Detail
- Medial elbow pain/tenderness over the resection, and VALGUS INSTABILITY if the MCL origin (inferior epicondyle) is over-resected - hence 'partial' epicondylectomy is favoured
- Detail
- Flexor-pronator origin disruption/weakness, heterotopic bone, persistent symptoms
What the evidence shows. Outcomes are broadly equivalent to the other operations but stage-dependent. A randomised trial within the Cochrane review found no difference between medial epicondylectomy and anterior transposition in clinical or neurophysiological outcome (Cochrane, PMID 27845501). The staged meta-analysis (Mowlavi, PMID 10946931) is more nuanced: in minimal/mild disease total symptom relief was actually achieved most often after medial epicondylectomy, but in severe disease it produced the poorest operative result. The practical message is that it is a reasonable alternative in milder disease and for the subluxating nerve, but it is not a rescue for the atrophic hand, and the MCL must be respected to avoid trading neuropathy for instability.
The anterior bundle of the medial collateral (ulnar collateral) ligament - the primary restraint to valgus - originates from the inferior aspect of the medial epicondyle. A complete epicondylectomy risks detaching it and producing valgus instability, so a partial (minimal) epicondylectomy is the modern preference: enough bone to let the nerve translate, not so much that you destabilise the elbow.
Complications
- Incidence
- 5-10%
- Management
- Careful dissection, neurolysis if symptomatic
- Incidence
- 5-15%
- Management
- Revision with transposition
- Incidence
- Rare
- Management
- Avoid MCL injury, repair if damaged
- Incidence
- 2-5%
- Management
- Standard wound care
- Incidence
- 10-20%
- Management
- Counsel pre-operatively especially if atrophy
MABC nerve injury causing painful neuroma is the most common complication. Careful handling and protection during dissection is essential.
Postoperative Care
Postoperative Protocol
Soft dressing, sling optional. Elevate arm. Finger ROM immediately. Wound check at 1 week.
Remove sutures. Begin gentle elbow ROM. Avoid resisted flexion.
Progressive strengthening. Full ROM by 4 weeks. Grip strengthening from week 6.
Assess nerve recovery. Sensory improvement first. Motor recovery may take 6-12 months.
Return to work: Desk work 1-2 weeks. Manual work 6-8 weeks.
Outcomes and Prognosis
Success Rates:
- In-situ decompression: 80-90% good/excellent
- Anterior transposition: 80-90% good/excellent
- Comparison: No significant difference in outcomes
Prognostic Factors:
- Better Outcome
- I-II
- Worse Outcome
- III with atrophy
- Better Outcome
- Short (under 6 months)
- Worse Outcome
- Long (over 1 year)
- Better Outcome
- Younger
- Worse Outcome
- Elderly
- Better Outcome
- Absent
- Worse Outcome
- Present
Motor recovery is often incomplete if intrinsic atrophy is present pre-operatively.
Guidelines, Registries & Global Practice
Global Epidemiology
- Second most common upper-limb entrapment neuropathy after carpal tunnel syndrome (Cochrane, PMID 27845501).
- Population incidence approximately 30 per 100,000 person-years (US claims database, PMID 28362959); rises with age, slightly higher in men.
- Around 40% of diagnosed patients eventually undergo surgery; surgical conversion increases with age.
Side-by-Side Guidance
- Diagnosis
- Clinical plus NCS/EMG to grade severity; ultrasound increasingly used
- First-line
- Activity modification, night extension splinting
- Surgical default
- In-situ decompression; transposition for subluxation/revision
- Diagnosis
- Clinical diagnosis; NCS to confirm and grade
- First-line
- Conservative 3-6 months for mild disease
- Surgical default
- Simple decompression first-line (NICE-aligned)
- Diagnosis
- NCS plus high-resolution ultrasound (nerve CSA)
- First-line
- Conservative for McGowan I
- Surgical default
- Decompression; submuscular transposition in selected severe/revision cases
- Diagnosis
- Address structural causes (osteophytes, cubitus valgus)
- First-line
- Treat underlying deformity
- Surgical default
- Decompression plus deformity correction where relevant
Across societies the convergent position—supported by Level I trials (PMID 15730578) and meta-analyses (PMID 18056489, 27845501)—is that simple in-situ decompression is the default operation, with transposition reserved for documented subluxation, revision, or specific deformity (e.g. cubitus valgus tardy ulnar palsy).
Registry & Outcome Notes
- No dedicated international cubital tunnel registry exists; evidence rests on RCTs and administrative databases (e.g. PMID 28362959).
- Reported good/excellent outcomes are 80-90% across techniques, with revision rates of roughly 4-5% (PMID 29481399).
High- vs Limited-Resource Practice
- High-resource: routine NCS/EMG, ultrasound nerve cross-sectional area, day-case surgery, endoscopic options.
- Limited-resource: clinical diagnosis and the elbow flexion/Tinel tests guide management; open in-situ decompression under local or regional anaesthesia is effective, low-cost, and avoids the need for advanced neurophysiology.
Documentation & Consent (universal)
- Record motor examination (Froment's, Wartenberg's) and any intrinsic wasting at each visit.
- Consent must include risk of incomplete motor recovery when atrophy is present, MABC nerve injury, wound complications, and recurrence.
- Capture occupational exposure where work-related causation is plausible.
Controversies and Areas of Uncertainty
Older dogma reserved transposition for severe (McGowan III) cases, but RCT evidence (Gervasio, PMID 15617592) and the Cochrane review (PMID 27845501) show equivalence even with severe impairment. The optimal operation for the atrophic hand remains debated.
Subluxation is the classic indication for transposition, yet Bartels Part 1 (PMID 15730578) found outcomes unaffected by subluxation after simple decompression. Whether subluxation alone justifies transposition is unsettled.
Endoscopic in-situ release gives equivalent clinical outcomes (Buchanan, PMID 29481399) with less scar pain but more haematoma. Cost, learning curve, and limited long-term data keep its role contested.
High-resolution ultrasound (enlarged nerve cross-sectional area) is increasingly used, but diagnostic thresholds are not standardised and NCS/EMG remains the reference standard. The place of imaging in equivocal cases is evolving.
Other open questions: when (if ever) to operate in purely sensory McGowan I disease that fails conservative care; the value of supplementary nerve-gliding exercises (no added benefit over advice in the one RCT analysed by Cochrane); and the lack of a unified outcome metric across trials, which complicates pooling.
MCQ Practice Points
Q: Which fingers are affected in ulnar nerve compression? A: Small finger and ulnar half of ring finger - both palmar AND dorsal surfaces (unlike CTS which is palmar only).
Q: Which muscle is tested by Froment's sign? A: Adductor pollicis - the only muscle that adducts the thumb (except for first interosseous to lesser extent). Innervated by ulnar nerve.
Q: Why is clawing worse in a LOW ulnar nerve lesion? A: FDP function preserved. In high lesion, FDP to ring/small is paralyzed so IP flexion is weak. In low lesion, FDP works normally, causing pronounced IP flexion with MCP hyperextension.
Q: What does the evidence show regarding in-situ decompression vs anterior transposition? A: Similar outcomes. Cochrane review (Caliandro 2016) shows no significant difference. Simple decompression has lower complication rate. Reserve transposition for subluxation or revision.
Q: What is the Arcade of Struthers and why is it important? A: Musculofascial band 5-10cm proximal to medial epicondyle. Potential compression site that must be released during decompression to prevent recurrence.
Q: What is Osborne's ligament? A: The arcuate ligament connecting the two heads of FCU. Forms the roof of the cubital tunnel. Release is essential during decompression.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old office worker presents with 6 months of numbness in the small finger. He leans on his elbows at his desk. Tinel's is positive over the elbow. Froment's is negative.”
“A 45-year-old man has 12 months of small finger numbness and now notices weakness holding a key. On examination, Froment's sign is positive and there is early wasting of the first dorsal interosseous.”
“A patient returns 6 months after in-situ decompression with persistent symptoms and now has subluxation of the ulnar nerve with elbow flexion. What is your approach?”
Key Anatomy
- Ulnar nerve between medial epicondyle and olecranon
- Osborne's ligament = FCU aponeurosis (roof)
- Arcade of Struthers 5-10cm proximal
- MABC nerve at risk superficially
Clinical Signs
- Froment's = thumb IP flexion when pinching
- Wartenberg's = small finger abducted
- Claw hand = MCP hyperextension + IP flexion
- Ulnar paradox = worse claw in LOW lesion
Classification
- McGowan I = sensory only = conservative
- McGowan II = weakness = consider surgery
- McGowan III = atrophy = urgent surgery
- Modified IIA/IIB distinguishes intermittent vs persistent
Surgery Options
- In-situ decompression = first line
- Anterior transposition = subluxation/revision
- Submuscular = high demand/revision
- All have 80-90% success
Complications
- MABC neuroma = most common
- Recurrence 5-15%
- Incomplete motor recovery if atrophy
- Elbow instability if MCL injured
Evidence Base
- 9 RCTs, 587 participants; UNE is 2nd commonest entrapment neuropathy
- Simple decompression vs transposition: no difference in clinical improvement (RR 0.93, 95% CI 0.80-1.08, moderate-quality evidence)
- Transposition associated with more wound infections (RR 0.32, 95% CI 0.12-0.85)
- Equally effective even when nerve impairment is severe
- 4 RCTs pooled (2 submuscular, 2 subcutaneous transposition)
- No difference in clinical scores (3 trials, 261 patients; SMD -0.04, 95% CI -0.36 to 0.28)
- No difference in postoperative motor conduction velocity (2 trials, 100 patients)
- Narrow confidence intervals exclude clinically meaningful difference
- 152 patients randomized: 75 simple decompression vs 77 anterior subcutaneous transposition
- Good/excellent: 49/75 (decompression) vs 54/77 (transposition) — not significant
- Complication rate lower with decompression (9.6% vs 31.1%; RR 0.32, 95% CI 0.14-0.69)
- Outcome unaffected by nerve subluxation or symptom severity
- 70 patients with SEVERE (Dellon grade 3) cubital tunnel syndrome
- Simple decompression vs deep submuscular transposition with flexor-pronator Z-lengthening
- Good/excellent: 80% (decompression) vs 82.9% (transposition) — no significant difference
- No severe complications or recurrences in either group
- 5 studies, 655 patients (226 endoscopic, 429 open in-situ release)
- Equivalent good/excellent Bishop scores (OR 1.27, 95% CI 0.59-2.75) and VAS reduction
- Endoscopic: less scar tenderness/elbow pain (OR 0.19) but more haematoma (OR 5.70)
- Reoperation rates similar (4.9% endoscopic vs 4.1% open)
- Meta-analysis of 30 studies with staged pre- and post-operative outcomes
- Mild disease: all modalities similar; nonoperative care had highest recurrence
- Moderate disease: submuscular transposition most efficacious
- Severe disease: no modality consistently effective; medial epicondylectomy poorest
- Largest population study: US claims database, 53,401 new cases (2006-2012)
- Adjusted incidence 30.0 per 100,000 person-years
- 41.3% of diagnosed patients underwent surgery; rate rises with age
- Slightly higher incidence in men overall; incidence increases with age in both sexes