Pure Motor Branch of Median Nerve | No Sensory Loss | OK Sign Weakness
- Pure Motor Palsy: NO sensory loss distinguishes AIS from median nerve compression
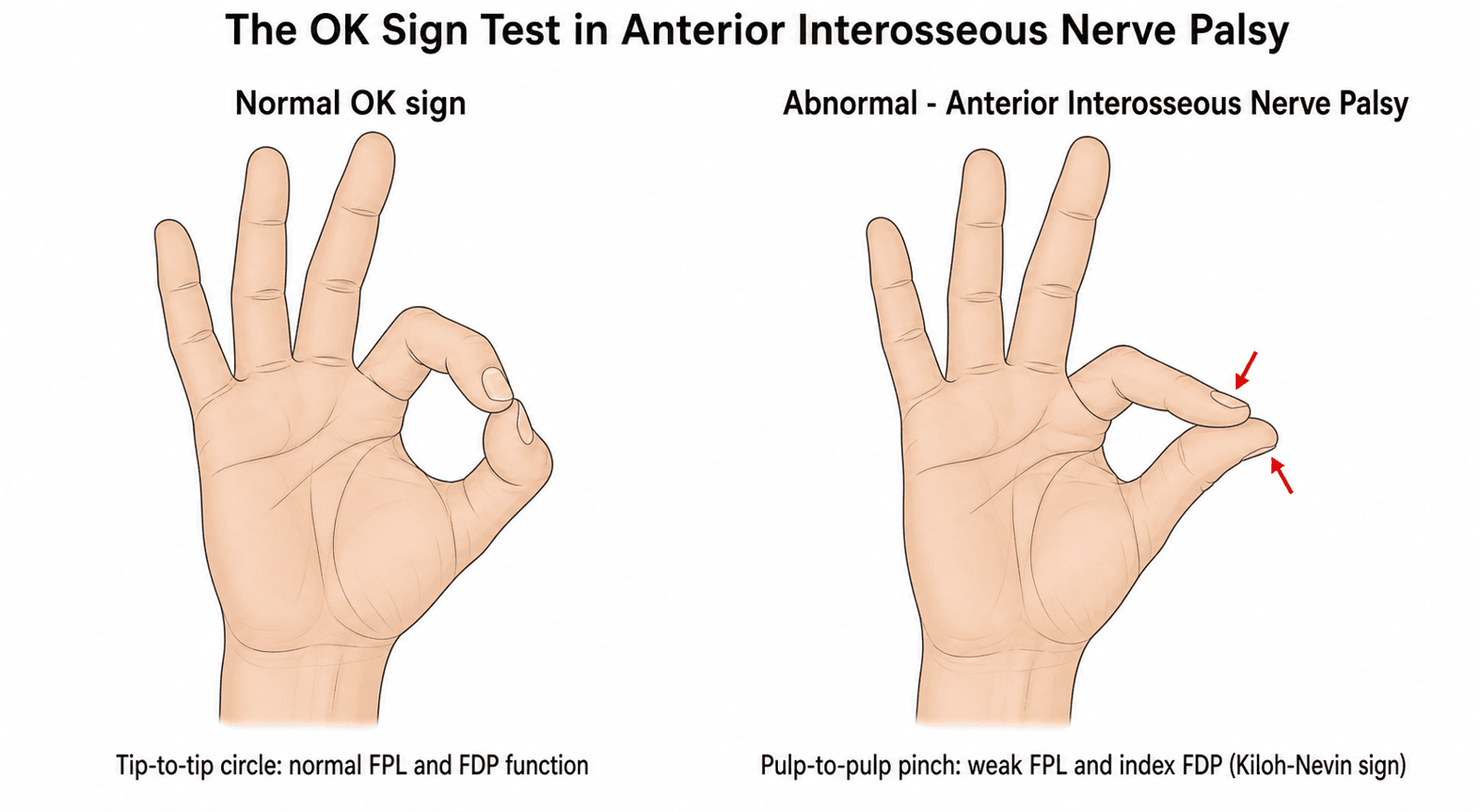
- OK Sign Test: Cannot make circle with thumb IP and index DIP - both remain extended
- Muscles Affected: FPL, FDP to index (and middle), pronator quadratus only
- Natural History: 60-70% recover spontaneously within 6 months - observe first
- Compression Site: Usually between two heads of pronator teres or fibrous bands
- “No sensory loss = AIN syndrome not median nerve
- “OK sign weakness = FPL + FDP index involvement
- “Pronator quadratus weakness hard to detect clinically
- “Observe 3-6 months before surgery - high spontaneous recovery
Zero sensory loss. If there is ANY sensory involvement, it is NOT isolated AIN syndrome - consider median nerve or pronator syndrome.
Cannot pinch with thumb tip and index tip. Both IP joints remain extended forming a pinch pulp-to-pulp instead of tip-to-tip.
60-70% recover spontaneously. Observation for 3-6 months is first-line treatment. Do not rush to surgery.
FPL tendon rupture, FDP rupture, pronator syndrome. Check for sensory loss and palpate tendons to differentiate.
- Likely Diagnosis
- Acute AIS (traumatic)
- Treatment
- Observation 3-6 months, EMG at 6 weeks
- Key Pearl
- 70% recover spontaneously
- Likely Diagnosis
- Idiopathic AIS
- Treatment
- Observation 3-6 months, consider imaging
- Key Pearl
- Most common presentation
- Likely Diagnosis
- Pronator syndrome
- Treatment
- Different treatment - may need earlier surgery
- Key Pearl
- Sensory loss rules out pure AIN
FPL FDP PQAIN Motor Innervation
Hook:FPL FDP PQ - The three muscles that make the OK sign work! All motor, zero sensory!
SENSORYAIS vs Pronator Syndrome Differentiation
Hook:SENSORY tells you what's missing in AIS - no sensory loss!
Overview and Epidemiology
AIS is the classic pure motor median nerve palsy. Understanding that it has ZERO sensory loss and high spontaneous recovery rate is critical for exam scenarios and preventing unnecessary surgery.
Anterior Interosseous Syndrome is isolated compression or injury of the anterior interosseous nerve, a pure motor branch of the median nerve.
- Age: Any age, peak 30-50 years
- Sex: No clear gender predilection
- Bilateral: Rare (suggests systemic cause)
- Occupational: Can occur with repetitive pronation
Much less common than carpal tunnel syndrome.
- Diagnosis often delayed: Mistaken for tendon rupture
- High spontaneous recovery: 60-70% within 6 months
- Pure motor palsy: No sensory loss key to diagnosis
- Surgical outcomes: Good if selected appropriately
Observation is first-line treatment in most cases.
Pathophysiology and Mechanisms
The anterior interosseous nerve branches from the median nerve 4-6cm distal to the lateral epicondyle, just AFTER the nerve passes between the two heads of pronator teres. It is a PURE MOTOR branch with zero cutaneous sensory distribution.
- Origin: Median nerve, 4-6cm distal to lateral epicondyle
- Course: Descends on anterior surface of interosseous membrane
- Termination: Pronator quadratus and wrist joint capsule (sensory only to joint)
- Flexor pollicis longus (FPL): Thumb IP flexion
- Flexor digitorum profundus to index (and middle): Index and middle DIP flexion
- Pronator quadratus (PQ): Forearm pronation (weak clinically)
- Between two heads of pronator teres
- Fibrous bands from deep head of pronator teres
- Accessory muscles (Gantzer's muscle)
- Lacertus fibrosus (bicipital aponeurosis)
- Thrombosed vessels or aberrant radial arteries
FIBROMACauses of AIS
Hook:FIBROMA - Think of anatomical causes from fractures to masses to anomalies!
Classification Systems
Clinical Severity Classification
- Clinical Findings
- Weakness only, no atrophy
- EMG Findings
- Denervation in affected muscles
- Treatment
- Observation 3-6 months
- Clinical Findings
- Progressive weakness, no recovery at 3 months
- EMG Findings
- Ongoing denervation
- Treatment
- Continue observation to 6 months
- Clinical Findings
- Muscle atrophy or no recovery at 6 months
- EMG Findings
- No reinnervation potentials
- Treatment
- Surgical exploration
Severity guides timing of intervention.
Clinical Assessment
- Onset: Acute (post-trauma) or gradual (idiopathic)
- Pain: May have initial forearm pain (Parsonage-Turner)
- Weakness: Difficulty pinching, writing, turning keys
- No numbness: Critical negative finding
- Red flags: Sensory loss (not pure AIN), progressive atrophy
Ask specifically about numbness to rule out pronator syndrome.
- OK sign test: Cannot make tip-to-tip circle
- Pinch pattern: Pulp-to-pulp instead of tip-to-tip
- FPL testing: Isolate thumb IP flexion
- FDP index testing: Isolate index DIP flexion
- Sensory exam: MUST be completely normal
- Tinel's: May be positive over AIN course
Always test sensation to confirm pure motor palsy.
- Technique
- Ask patient to make circle with thumb and index
- Positive Finding
- Extended IP joints, pulp-to-pulp pinch
- Indicates
- FPL and FDP index weakness
- Technique
- Stabilize thumb MCP, ask to flex IP
- Positive Finding
- Weak or absent IP flexion
- Indicates
- FPL denervation
- Technique
- Stabilize PIP, ask to flex DIP
- Positive Finding
- Weak or absent DIP flexion
- Indicates
- FDP denervation
- Technique
- Resist pronation with elbow flexed 90°
- Positive Finding
- Subtle weakness (hard to detect)
- Indicates
- PQ denervation
Key differentials: FPL tendon rupture, FDP rupture, pronator syndrome (has sensory loss), high median nerve palsy, neuralgic amyotrophy. Palpate tendons and check sensation carefully.
Partial AIN Palsy: Not Always the Full OK-Sign
The classic teaching is the complete OK-sign pattern (weak FPL and index FDP), but the evidence shows AIN palsy is frequently incomplete — a point the fascicular-constriction model explains and examiners probe.
- The fascicles are topographically distinct. The motor fascicles destined for FPL, index FDP and pronator quadratus travel as separate, identifiable fascicular groups within the median nerve well proximal to the branch point, so a focal (neuralgic-amyotrophy) constriction can pick off one fascicle in isolation.
- The common partial patterns:
- Isolated FPL palsy — the commonest partial form (weak thumb IP flexion alone; the "isolated FPL" group in the classic series).
- Isolated index FDP palsy (weak index DIP flexion alone).
- FPL plus index FDP without clinically detectable PQ weakness (PQ is hard to test anyway).
- Why it matters. A patient with only weak thumb-tip flexion can still have AIN palsy — do not exclude the diagnosis because the full OK sign is preserved; conversely, isolated FPL weakness must still be distinguished from an FPL tendon rupture (check the tenodesis effect and palpate the tendon).
- Prognostic note. Single-fascicle (partial) involvement and any manual-muscle-test improvement by six months predict good recovery, whereas a complete, non-improving palsy is the group considered for neurolysis.
Q: A patient cannot flex the thumb IP joint but has normal index DIP flexion and normal sensation — can this still be AIN palsy? A: Yes — isolated FPL palsy is the commonest partial AIN palsy, because the FPL, index-FDP and PQ fascicles are topographically separate in the median nerve and a focal (neuralgic-amyotrophy) constriction can hit one alone. Distinguish it from an FPL tendon rupture (tenodesis test, palpable gap). A preserved full OK sign does not exclude AIN palsy.
Investigations
Investigation Protocol
Clinical diagnosis based on pure motor palsy affecting FPL, FDP index, and PQ with ZERO sensory loss. OK sign weakness is diagnostic.
EMG/NCS at 6 weeks post-onset. Denervation potentials in FPL, FDP (radial), and PQ. Normal sensory studies. Helps confirm diagnosis and establish baseline.
MRI forearm if mass lesion suspected, trauma history, or no recovery at 3 months. May show space-occupying lesion, hematoma, or nerve changes.
Repeat EMG to assess for reinnervation potentials. If no recovery, consider surgical exploration.
Electrodiagnostic Findings:
- Motor NCS: May be normal (nerve supplies only 3 muscles deep in forearm)
- Sensory NCS: NORMAL (critical finding)
- EMG: Denervation potentials (fibrillations, positive sharp waves) in FPL, FDP index/middle, and PQ
- Follow-up EMG: Reinnervation potentials indicate recovery
Management Algorithm

Conservative Management (First-Line)
Observation Protocol
Observation and activity modification. Avoid heavy gripping and pinching. Baseline EMG at 6 weeks to confirm diagnosis. Hand therapy for ROM.
Continue observation. Clinical reassessment monthly. Most spontaneous recoveries begin in this period. Maintain ROM exercises.
Repeat EMG at 3-4 months. If no clinical or electrical recovery, consider imaging and surgical exploration. If improving, continue observation.
Surgery if no recovery by 6 months. Some advocate waiting up to 12 months if showing gradual improvement. Balance against muscle atrophy risk.
Observation for 3-6 months is standard as most cases recover spontaneously.
Surgical Technique
Anterior Interosseous Nerve Exploration
Surgical Steps
Supine, arm on table, tourniquet. Volar approach, curvilinear incision from 2cm distal to elbow flexion crease extending 10-12cm distally along ulnar border of mobile wad.
Identify and protect lateral antebrachial cutaneous nerve. Divide lacertus fibrosus. Retract brachioradialis laterally.
Identify median nerve between FDS and FCR. Trace distally to identify pronator teres. Release nerve from between two heads of pronator teres.
Identify AIN branching from median nerve 4-6cm distal to epicondyle. Follow nerve distally along interosseous membrane. Release all fibrous bands, anomalous muscles (Gantzer's), or compressing structures.
Release nerve throughout course. Excise any mass lesions. Ensure nerve glides freely. Inspect FPL, FDP, and PQ muscle bellies for atrophy.
Layered closure. No drain typically needed. Bulky dressing and forearm splint in neutral position.
Complete decompression from origin to pronator quadratus is essential.
Complications
- Incidence
- 20-40%
- Management
- Counsel pre-operatively, therapy
- Incidence
- 5-10%
- Management
- Careful dissection, neurolysis if symptomatic
- Incidence
- Rare (under 2%)
- Management
- Prevent with gentle handling
- Incidence
- Rare (under 5%)
- Management
- Ensure complete release
- Incidence
- Rare
- Management
- Early therapy, multidisciplinary care
Incomplete recovery is the most common outcome issue. Counsel patients that surgery aims to prevent further deterioration and allow recovery, but full strength may not return, especially if atrophy is present.
Tendon Transfers for Established AIN Palsy
The outcomes and global-practice sections name tendon transfer as the salvage when the nerve does not recover — here are the specific transfers, because only two functions need restoring.
- What actually needs restoring. The deficit is loss of thumb IP flexion (FPL) and index DIP flexion (index FDP); pronator quadratus loss is well compensated by pronator teres and needs no transfer, and there is no sensory deficit to address.
- For thumb IP flexion (FPL): brachioradialis (BR) to FPL is the workhorse transfer (adequate excursion, expendable donor); an FDS (e.g. ring) to FPL transfer is an alternative.
- For index DIP flexion: a side-to-side tenodesis of the index FDP to the adjacent intact (middle/long) FDP restores index distal flexion by borrowing the working profundus mass — simple and reliable.
- When to do it. Reserved for established palsy with no clinical or electrical recovery after adequate observation and/or neurolysis, particularly with muscle atrophy where reinnervation is unlikely; it is the principal salvage where microsurgical neurolysis is unavailable. General tendon-transfer principles (donor expendability, synergism, one-tendon-one-function, supple joints) are developed in the tendon-transfers topic.
Q: What tendon transfers salvage an established, non-recovering AIN palsy? A: Restore the two lost functions: brachioradialis-to-FPL for thumb IP flexion, and a side-to-side tenodesis of the index FDP to the intact middle-finger FDP for index DIP flexion. Pronator quadratus needs no transfer (pronator teres compensates) and there is no sensory loss. Reserve for atrophied, non-recovering palsy.
Postoperative Care
Postoperative Protocol
Forearm splint in neutral position. Wound care. Finger and elbow ROM out of splint. Suture removal at 10-14 days.
Discontinue splint. Begin gentle active ROM all joints. Scar massage. No strengthening yet.
Progressive strengthening. Pinch and grip strengthening exercises. Functional activities.
Monitor for nerve recovery. Repeat EMG at 6 months post-op to assess reinnervation. Recovery may take up to 12-18 months.
Return to work: Light duty at 2-4 weeks. Full duty at 8-12 weeks depending on demands and recovery.
Outcomes and Prognosis
- Spontaneous recovery: 60-70% within 6 months
- Time to recovery: Most within 3-6 months, can take up to 12 months
- Complete recovery: Common in idiopathic and post-traumatic cases
- Neuralgic amyotrophy: Recovery in 80-90% but may take 18-24 months
- Overall improvement: 70-80% good to excellent results
- Complete recovery: 50-60% (lower than spontaneous)
- Partial recovery: 20-30%
- No improvement: 10-20%
- Better Outcome
- Traumatic, mass lesion
- Worse Outcome
- Idiopathic, neuralgic amyotrophy
- Better Outcome
- Short (under 6 months)
- Worse Outcome
- Long (over 12 months)
- Better Outcome
- Absent
- Worse Outcome
- Present pre-operatively
- Better Outcome
- Younger
- Worse Outcome
- Elderly
Early surgical decompression for compressive masses has excellent outcomes. Prolonged observation (over 12 months) may lead to irreversible muscle atrophy.
Guidelines, Registries & Global Practice
Global Epidemiology:
- Rare condition — far less common than carpal tunnel syndrome; precise incidence unknown
- Accounts for under 1% of upper-limb compressive/inflammatory neuropathies in most hand-surgery series
- Most spontaneous cases now classed within neuralgic amyotrophy (annual incidence of NA estimated around 1 per 1,000)
- Peak age 30-50 years; no consistent sex predilection; bilateral disease is rare
Side-by-Side Society Approach (no condition-specific registry exists for AIS):
- Diagnostic emphasis
- Clinical pure-motor pattern plus EMG
- Surgical timing
- Observe first; explore if no recovery
- Imaging
- MRI/MR neurography if available
- Diagnostic emphasis
- Clinical diagnosis, confirm with NCS/EMG
- Surgical timing
- Trial of observation, then neurolysis
- Imaging
- HRUS / MR neurography increasingly used
- Diagnostic emphasis
- Recognise neuralgic amyotrophy spectrum
- Surgical timing
- Earlier interfascicular neurolysis advocated by some centres
- Imaging
- HRUS-led localisation of constriction
- Diagnostic emphasis
- Relevant mainly when AIS follows fracture
- Surgical timing
- Treat compressive cause; explore if structural
- Imaging
- Imaging directed at fracture/callus
There is broad consensus that electrodiagnostic confirmation precedes surgery and that structural compression (mass, fracture, callus) warrants earlier exploration, while spontaneous palsy is observed first.
- Well-resourced settings: MR neurography / high-resolution ultrasound localise intraneural constrictions; interfascicular microneurolysis available
- Limited-resource settings: diagnosis is clinical (pure motor pattern, normal sensation, OK-sign weakness), often without electrodiagnostics; management defaults to observation, with tendon transfer reserved for established non-recovery
- Tendon transfer (e.g. brachioradialis to FPL, side-to-side FDP) remains a robust salvage globally where microsurgical neurolysis is unavailable
- Record the pure motor nature (zero sensory loss) confirming the diagnosis
- Counsel on the high spontaneous recovery rate and the rationale for an observation period
- Consent for surgery should include incomplete recovery, cutaneous nerve injury, and persistent weakness
- Note that recovery may take 6-12 months or longer
Controversies and Areas of Uncertainty
The biggest controversy in AIS is its very nature. The classical teaching — external mechanical compression in the forearm (pronator teres heads, Gantzer's muscle, fibrous bands) — has been substantially challenged. Contemporary high-resolution imaging and surgical series increasingly show that most spontaneous AIN palsy is a form of neuralgic amyotrophy (Parsonage-Turner syndrome) with intraneural hourglass-like fascicular constrictions located in the median nerve AT or ABOVE the elbow, not external compression distally.
- Classical view: distal forearm entrapment requiring decompression
- Modern view: intraneural fascicular constriction (neuralgic amyotrophy)
- Most series now favour the neuralgic amyotrophy model for spontaneous cases
- True external compression is reserved for trauma, mass, or fracture cases
The distinction changes WHERE you would operate (above elbow vs forearm).
- Conservative camp: observe 6 months (improvement by 6 months predicts full recovery)
- Early-surgery camp: explore at 3 months if discrete constriction on imaging
- No randomised trial exists; evidence is cohort-level
- Decision increasingly guided by HRUS / MR neurography findings
Both camps agree on early surgery for structural compression.
- Mild-moderate constriction: interfascicular neurolysis alone
- Severe constriction (loss of fascicle continuity): resection and neurorrhaphy
- Some report nerve/tendon transfers when reinnervation is unlikely
- Persistent constriction can remain even after clinical recovery, questioning its causal role
- HRUS and MR neurography can localise the proximal intraneural lesion
- Not universally available; many units still diagnose clinically plus EMG
- Imaging may upstage a "forearm" problem to a proximal one
- High- vs limited-resource settings differ markedly in access
MCQ Practice Points
Q: What distinguishes anterior interosseous syndrome from pronator syndrome? A: Zero sensory loss. AIS is a pure motor palsy (AIN has no cutaneous sensory distribution). Pronator syndrome has sensory loss in median nerve distribution because the nerve is compressed proximal to the AIN branching.
Q: What does the OK sign test? A: FPL and FDP to index. Inability to make tip-to-tip pinch (thumb IP and index DIP extended) indicates weakness of FPL and FDP index, pathognomonic for AIN palsy.
Q: What percentage of AIS cases recover spontaneously? A: 60-70% within 6 months. This high spontaneous recovery rate justifies observation as first-line treatment before considering surgical exploration.
Q: What muscles are innervated by the anterior interosseous nerve? A: FPL, FDP to index (and middle), and pronator quadratus. Only these three muscles - no cutaneous sensation.
Q: Where does the AIN branch from the median nerve? A: 4-6cm distal to the lateral epicondyle. This is just distal to the pronator teres, which is why pronator teres compression can affect AIN.
Q: What is Gantzer's muscle? A: Accessory head of FPL. Anatomical variant present in 45-65% of people. Arises from medial epicondyle and can compress the AIN.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old man presents with 2 months of difficulty pinching objects. He cannot make an 'OK' sign properly. His thumb and index finger IPs remain extended when he tries. Sensation in the hand is completely normal. What is your diagnosis and management?”
“A 28-year-old woman sustained a proximal radius fracture treated non-operatively 8 weeks ago. She now presents with difficulty writing and pinching. Examination shows weak OK sign but normal sensation. What is your approach?”
“A patient with idiopathic AIS has been observed for 6 months with no clinical improvement. Repeat EMG shows persistent denervation with no reinnervation potentials. MRI shows no mass lesion. The patient has visible atrophy of the thenar eminence. What is your approach?”
Key Anatomy
- AIN = pure motor branch of median nerve
- Branches 4-6cm distal to lateral epicondyle
- Innervates only 3 muscles: FPL, FDP (index/middle), PQ
- Zero cutaneous sensory distribution
Clinical Diagnosis
- OK sign weakness = cannot pinch tip-to-tip
- Normal sensation = key to diagnosis
- FPL and FDP index weakness, PQ weak (hard to test)
- EMG: denervation in 3 muscles, normal sensory studies
Differential Diagnosis
- Pronator syndrome = has sensory loss (palmar)
- FPL tendon rupture = palpable tendon gap
- High median nerve palsy = thenar weakness + sensory
- Neuralgic amyotrophy = painful onset, shoulder involvement
Natural History
- 60-70% recover spontaneously within 6 months
- Observation first-line treatment
- EMG at 6 weeks to confirm diagnosis
- Surgery if no recovery by 6 months
Surgical Technique
- Volar approach, expose median nerve proximally
- Trace AIN from origin distally
- Release all fibrous bands and anomalous muscles
- Gantzer's muscle common compression site
Outcomes
- Non-op: 60-70% full recovery
- Post-op: 70-80% good-excellent
- Recovery takes 6-12 months
- Atrophy portends incomplete recovery
Evidence Base
- 100 limbs with spontaneous AIN palsy from 24 institutions, conservative vs interfascicular neurolysis by patient choice
- Good recovery (FPL and index FDP MRC grade 4 or better) in 39 of 49 conservatively treated limbs
- ALL 26 limbs showing 1-grade MMT improvement by 6 months on conservative care achieved good recovery
- Of 59 limbs with no recovery at 6 months, good recovery in 30 of 36 with subsequent neurolysis vs 13 of 23 continuing conservative care
- 21 patients with spontaneous AIN palsy, all managed non-operatively (mean age 39)
- Antecedent limb/shoulder pain in 17 of 21, settled within 6 weeks in every case
- MRC grade 4 or better reached in all 15 with complete FDP-index palsy and 16 of 18 with complete FPL palsy
- Recovery within 12 months in patients under 40; age strongly correlated with outcome
- Reconceptualises AINS as a form of neuralgic amyotrophy (Parsonage-Turner syndrome), NOT external forearm compression
- Fascicular constrictions localise to the anterior interosseous fascicular group AT or ABOVE the medial epicondyle
- Up to 30% of patients left with permanent weakness or palsy — spontaneous recovery is not assured
- Fascicular microneurolysis at or above the elbow is the procedure of choice for non-recovering cases
- 20 patients (22 nerves) with spontaneous hourglass-like fascicular constriction of upper-limb nerves
- Acute pain always the first symptom, followed by rapid severe paralysis; constrictions unrelated to compressive structures
- Histology showed inflammatory infiltration, demyelination and reduced nerve fibres
- Early surgery recommended if no recovery by 3 months; neurolysis for mild-moderate, neurorrhaphy for severe lesions
- 51 cases (49 patients) of AIN and PIN involvement in neuralgic amyotrophy
- Pain was the first symptom in 52.9%, distal to the shoulder in 85.1%; sensory involvement in 27.5%
- Neurolysis significantly improved Hand20 scores (p=0.020) whereas conservative treatment did not (p=0.204)
- Neurolysis can be superior to conservative care in patients with focal constrictions and no spontaneous recovery
- High-resolution ultrasound findings in neuralgic amyotrophy: nerve swelling, incomplete constriction, complete constriction, fascicular entwinement
- These may represent a continuum predicting spontaneous recovery versus need for surgery
- For distal nerves (AIN, PIN), the lesion is almost always in the fascicles within the parent nerve, proximal to the branch point
- History and examination should direct which nerves are scanned
- No high-level guideline mandates surgery before a trial of observation in spontaneous (atraumatic) AIN palsy
- Electrodiagnostic confirmation is recommended before operative intervention
- Definite space-occupying or traumatic compression is an indication for earlier exploration
- Imaging (HRUS / MR neurography) increasingly used to localise the lesion and guide timing