Blood Supply of the Forearm
Superficial Radial Nerve.
- In the middle third of the forearm, the Radial Artery is closely associated with the Superficial Radial Nerve (running laterally).
- Risk: Injury during harvest or dissection.
- Rule: The nerve leaves the artery in the distal third to pass dorsally.
Ulnar Nerve Relationship.
- The Ulnar Artery joins the Ulnar Nerve in the middle third.
- Relation: The Artery is usually LATERAL (radial) to the Nerve.
- Mnemonic: "Nerve is Medial" (but strictly speaking, at the wrist, ulnar nerve is medial to artery).
- Main Muscle Cover
- Brachioradialis
- Nerve Relation
- Radial Nerve (Superficial)
- Hand Contribution
- Deep Palmar Arch
- Main Muscle Cover
- Flexor Carpi Ulnaris
- Nerve Relation
- Ulnar Nerve
- Hand Contribution
- Superficial Palmar Arch
- Main Muscle Cover
- FDP/FPL
- Nerve Relation
- AIN
- Hand Contribution
- Wrist Capsule
- Main Muscle Cover
- Supinator
- Nerve Relation
- PIN
- Hand Contribution
- Dorsal Carpal Arch
T-T-T-TContents of Carpal Tunnel (Not Arteries)
Hook:Arteries are generally NOT in the carpal tunnel.
M-U-L-LRelation at Wrist
Hook:At the wrist: the ulnar nerve sits medial to the ulnar artery; the superficial radial nerve has already left the radial artery to run dorsally.
SIRBranches of Radial Artery
Hook:SIR Radial.
Overview
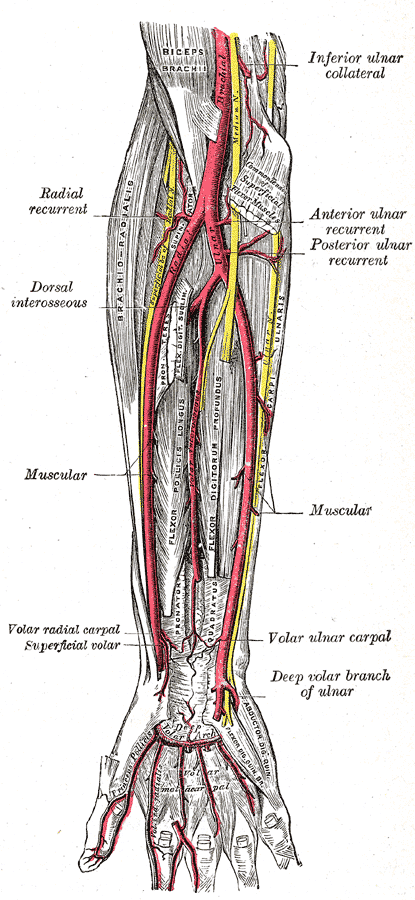
The forearm vascular supply is derived from the bifurcation of the Brachial Artery in the Cubital Fossa (opposite the neck of the radius). It divides into the Radial and Ulnar arteries, which travel down the lateral and medial borders of the forearm, respectively, to form the vascular arches of the hand.
Neurovascular
Radial Artery
- Origin: Smaller terminal branch of Brachial Artery.
- Course:
- Runs distally on the lateral side of the forearm.
- Covered by the belly of Brachioradialis (proximal 2/3).
- Becomes superficial in the distal 1/3 (site of palpation/ABG).
- Winds around the lateral aspect of the wrist (Anatomical Snuffbox).
- Branches:
- Radial Recurrent: Ascends to anastomose with Radial Collateral.
- Muscular: To lateral extensors/flexors.
- Superficial Palmar Branch: Completes superficial arch.
This artery is the direct continuation of the direction of the brachial artery, though smaller in caliber.
Anatomical Illustration

Anastomoses
Elbow Anastomosis
Ensures collateral circulation around the joint.
- Radial Recurrent joins Radial Collateral.
- Ulnar Recurrent (Ant/Post) joins Ulnar Collateral (Inf/Sup).
- Interosseous Recurrent joins Middle Collateral.
Clinical Note: This rich network allows ligation of the brachial artery distal to the Profunda in emergency, though not recommended appropriately.
The hand is supplied by two palmar arches (much larger than the carpal arches), and the dominant contributor differs between them:
- Superficial palmar arch — the more distal arch (at the level of the outstretched thumb / Kaplan's cardinal line). It is mainly the continuation of the ULNAR artery, completed laterally by the superficial palmar branch of the radial artery (complete in roughly 70 per cent of hands). It gives the common palmar digital arteries, which split into the proper palmar digital arteries — the dominant supply to the fingers.
- Deep palmar arch — the more proximal arch (about a finger-breadth proximal to the superficial one). It is mainly the continuation of the RADIAL artery (after it crosses the snuffbox and dives between the heads of the first dorsal interosseous), completed by the deep branch of the ulnar artery. It gives the palmar metacarpal arteries and, importantly, the princeps pollicis (thumb) and radialis indicis (radial side of the index) — so the radial artery is the dominant supply to the thumb and radial index.
- Dorsally, the dorsal carpal arch gives the dorsal metacarpal arteries; the first dorsal metacarpal artery is the basis of the kite flap and the dorsal scaphoid/snuffbox supply.
Persistent median artery (the variant the vivas flag): the embryonic median artery — the original axial artery of the forearm — usually regresses, but it persists in a minority, running with the median nerve (often through the carpal tunnel) and sometimes contributing to the superficial arch. It is a recognised cause of carpal tunnel syndrome (and acute CTS if it thromboses), a structure to avoid injuring at carpal tunnel release, and a confounder of Allen-test interpretation; its prevalence appears to be rising across generations.
Pathology: Ischemia
Compartment Syndrome.
- Edema within the deep volar compartment occludes the microcirculation (AIA).
- Muscles infarct and fibrose.
- Result: Flexion contracture of wrist and fingers (Claw).
- Sign: Pain on passive extension (Stretch test).
Vasospasm.
- Digital arteries spasm.
- While primarily digital, severe proximal disease in Ulnar/Radial arteries (Buerger's, Hypothenar Hammer) can mimic or exacerbate.
Differential Diagnosis of the Ischaemic / Painful Hand
- Key Feature
- Pain on passive stretch, tense compartment
- Vessel / Level
- Microcirculation (AIN territory first)
- Distinguishing Test
- Clinical; compartment pressure if obtunded
- Key Feature
- Pulseless, expanding haematoma
- Vessel / Level
- Radial or ulnar artery
- Distinguishing Test
- CT angiography / on-table exploration
- Key Feature
- Repetitive palm trauma, ulnar-sided digital ischaemia
- Vessel / Level
- Distal ulnar artery (Guyon's canal)
- Distinguishing Test
- Duplex / angiography of ulnar artery
- Key Feature
- Bilateral, cold-triggered, fully reversible
- Vessel / Level
- Digital arteries (no fixed lesion)
- Distinguishing Test
- Normal large-vessel imaging
- Key Feature
- Young smoker, distal segmental occlusions
- Vessel / Level
- Distal radial/ulnar and digital arteries
- Distinguishing Test
- Angiography (corkscrew collaterals)
- Key Feature
- Recent arterial line, cool finger
- Vessel / Level
- Radial artery at wrist
- Distinguishing Test
- Doppler / duplex of radial artery
"Release all compartments" needs the anatomy, the technique, and the end-stage grading:
- The compartments: the volar (flexor) compartment — a superficial group (pronator teres, FCR, palmaris longus, FCU, FDS) and a deep group (FDP, FPL, pronator quadratus); the dorsal (extensor) compartment; and the mobile wad (brachioradialis, ECRL, ECRB). The deep volar muscles (FDP/FPL) and the anterior interosseous territory are hit first and hardest.
- Fasciotomy technique: a volar curvilinear incision (extended Henry/McConnell type — beginning medial to the biceps tendon, crossing the elbow crease obliquely to avoid a contracture, running down the forearm and curving to the thenar crease) that releases both the superficial AND deep volar compartments and is carried across the carpal tunnel (decompressing the median nerve and Guyon's canal). Then re-assess — if the dorsal compartment and mobile wad are still tense, add a separate straight dorsal incision. Leave the wounds open; delayed primary closure or skin graft.
- Volkmann's ischaemic contracture — the end-stage of a missed forearm compartment syndrome (Tsuge grading):
- Mild — part of FDP/FPL (a few digits), little or no nerve deficit → splinting, tendon lengthening/slide.
- Moderate — all the long finger flexors with median (± ulnar) nerve involvement → flexor-origin muscle slide, tendon transfers, neurolysis.
- Severe — flexors and extensors with marked neurological loss → excise infarcted muscle and reconstruct with a free functioning muscle transfer (e.g. gracilis) plus nerve reconstruction.
Classification Systems
While specific classification systems for arterial anatomy are rare, the Adachi Classification for Radial Artery variations is referenced.
Adachi Types (Radial Artery Origin)
- Type I: Normal (Bifurcation in Cubital Fossa).
- Type II: High Origin from Axillary Artery.
- Type III: High Origin from Brachial Artery.
Remember: High takeoff vessels often run superficial to the fascia ("Brachioradial Artery").
Clinical Assessment
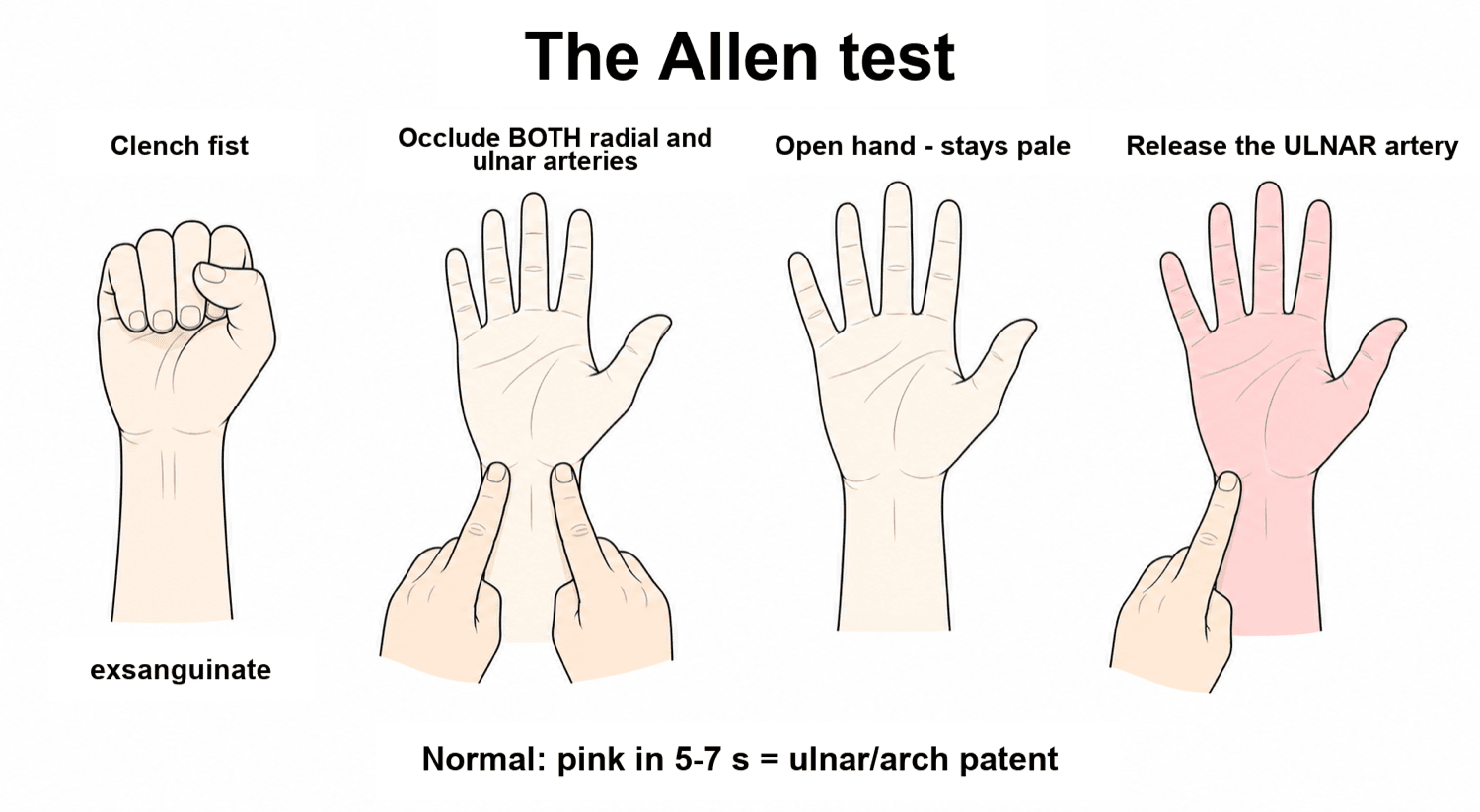
Allen's Test
- Purpose: Assess patency of the Ulnar artery and the Palmar Arch connectivity before harvesting the Radial Artery (ABG or CABG/Flap).
- Steps:
- Patient clenches fist (exsanguinate).
- Occlude both Radial and Ulnar arteries.
- Patient opens hand (should be pale).
- Release Ulnar Artery.
- Result:
- Positive (Normal): Hand flushes within 5-7 seconds.
- Negative (Abnormal): Hand remains pale (Ulnar supply insufficient).
A negative Allen's test is a contraindication to Radial Artery harvest.
Clinical Significance
Vascular Injury Management
- Action
- Ligate (if hand perfused)
- Rationale
- Redundancy is sufficient
- Action
- Repair Dominant (Ulnar) or Both
- Rationale
- Create Shunt first
- Action
- Explore + Papaverine
- Rationale
- Relieve kinking/spasm
Investigations
Hand-Held Doppler
- Indication: Assessing flow in trauma or pre-harvest.
- Triphasic: Normal flow.
- Monophasic: Indicates proximal stenosis or collateral flow.
- Allen's Confirmation: Audible signal change during compression.
Use a standard 8MHz vascular probe.
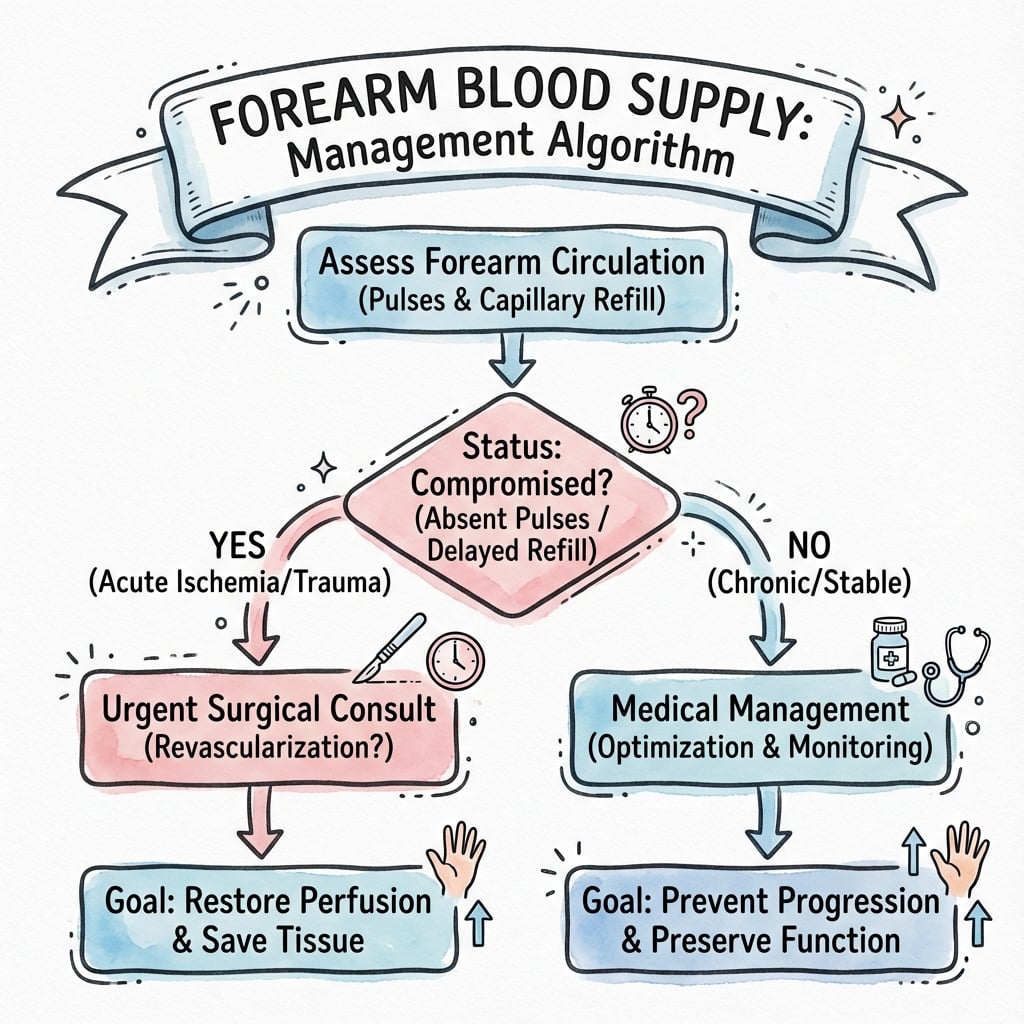
Management Algorithm
Surgical Considerations
Radial Forearm Free Flap (RFFF)
- Type: Fasciocutaneous flap (Type B).
- Supply: Septocutaneous perforators from Radial Artery.
- Anatomy:
- Passes in the septum between Brachioradialis and FCR.
- Venous drainage is via the Venae Comitantes or Cephalic Vein.
- Harvest: Raises the artery with the flap. Requires confirming Ulnar competency (Allen's Test).
This is the "Workhorse" flap for Head and Neck reconstruction.
Complications
- Arterial Line Complications: Thrombosis (5-10%), Pseudoaneurysm, AV fistula.
- Harvest Ischemia: Hand ischemia if collateral flow inadequate.
- Compartment Syndrome: Need for fasciotomy involving release of all compartments (Volar superficial/deep, Dorsal, Mobile Wad).
Rehabilitation
- Post-Flap: Monitor flap colour/turgor (Doppler signals).
- Compartment Release: Delayed closure vs skin graft. Therapy to prevent contracture.
Prognosis
- Single Artery Ligation: Excellent prognosis if Allen's test was normal. Minimal subjective cold intolerance.
- RFFF Donor Site: 20-30% reported cold intolerance. Aesthetic dissatisfaction is common.
- Vascular Repair: 80-90% patency rates for clean lacerations.
Guidelines, Registries & Global Practice
Global epidemiology of relevant anatomy
- A complete superficial palmar arch is present in only about 70-80% of hands across CT-angiographic and cadaveric series, so ulnar-dependent perfusion of the hand cannot be assumed before radial sacrifice.
- The brachioradial (high-origin, superficial radial) artery is the commonest major arterial variant of the upper limb, reported in roughly 10-15% of limbs in cadaveric and embryological series.
Side-by-side society guidance
- Domain
- Radial conduit for CABG
- Recommendation
- Radial artery preferred over saphenous vein as a second arterial graft in suitable patients with high-grade stenoses
- Domain
- Vascular trauma & flaps
- Recommendation
- Document dual-vessel patency and collateral flow before harvesting or ligating a forearm artery
- Domain
- Both-bone forearm & compartment syndrome
- Recommendation
- Low threshold for fasciotomy; clinical diagnosis takes priority over pressure thresholds
- Domain
- Hypothenar hammer / entrapment
- Recommendation
- Image distal vessels (duplex or CTA) before attributing digital ischaemia to vasospasm
Registry & trial signal
- The radial artery's standing as a CABG conduit rests on the RADIAL pooled randomised data (lower graft occlusion and adverse cardiac events versus vein), which is the main reason forearm collateral assessment matters in cardiac as well as hand practice.
High- vs limited-resource practice variation
- Well-resourced settings: Duplex ultrasound, CT angiography and continuous-wave Doppler routinely supplement the Allen's test before harvest or in vascular trauma.
- Limited-resource settings: The clinical Allen's test and hand-held Doppler remain the mainstay; awareness of its false-positive (~50%) and false-negative rates is essential to avoid both unnecessary conduit exclusion and iatrogenic hand ischaemia.
Controversies & Areas of Uncertainty
The clinical Allen's test has poor sensitivity and specificity (false-positive rates around 50%) for predicting hand ischaemia after radial harvest. Many vascular labs now mandate Doppler or digit-pressure confirmation, yet a normal bedside Allen's test remains the most widely taught pre-harvest screen worldwide.
Classic teaching permits ligating one forearm artery if the hand is well perfused, relying on arch redundancy. Increasing data on cold intolerance and the ~30% incidence of incomplete arches has prompted some surgeons to repair both vessels whenever feasible, especially in young or manual-working patients.
The ulnar artery is usually described as the larger terminal branch and dominant arch contributor, but codominance is common and radial-dominant arches exist. Dominance should be confirmed by imaging in the individual patient rather than assumed from textbook averages.
Absolute (greater than 30 mmHg) versus delta-pressure (less than 30 mmHg) thresholds for fasciotomy remain debated. Most authorities, including AO teaching, regard compartment syndrome as a clinical diagnosis, with pressure measurement reserved for the obtunded or equivocal patient.
MCQ Practice Points
Q: The Common Interosseous Artery is a branch of which vessel? A: Ulnar Artery.
Q: Which artery is the primary contributor to the Deep Palmar Arch? A: Radial Artery.
Q: The Ulnar Artery passes deep to which head of Pronator Teres? A: Deep Head. (The Median Nerve passes between the heads).
Q: The Radial Artery lies just lateral to which tendon at the wrist? A: Flexor Carpi Radialis (FCR).
Q: Which vessel does the Radial Recurrent artery anastomose with? A: Radial Collateral Artery (from Profunda Brachii).
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“You have just performed a prolonged forearm fracture fixation under tourniquet. On release, the hand remains white. What is your algorithm?”
“Describe the anomaly of the 'High Bifurcation' of the radial artery.”
“A patient with a both-bone forearm fracture complains of increasing pain despite casting. Steps?”
Anatomy
- Ulnar Artery: Larger, Medial, Deep to Pronator
- Radial Artery: Smaller, Lateral, Deep to Brachioradialis
- Common Interosseous: From Ulnar
- Deep Arch: Radial / Superficial Arch: Ulnar
Key Relations
- Radial Nerve: Lateral to Radial Artery (Middle 1/3)
- Ulnar Nerve: Medial to Ulnar Artery (Distal 2/3)
- Median Nerve: Between heads of Pronator (Artery is deep)
- AIA/PIA: On Interosseous Membrane
- Posterior Interosseous: Pierces Supinator Muscle
Clinical
- Allen's Test: Collateral Flow (Essential pre-op test)
- Compartment Syndrome: AIA Ischemia (First affected)
- RFFF: Fasciocutaneous Flap (Allen's negative required)
- Anastomoses: Carpal arches protect hand perfusion
- Radial Flap: Most common free forearm flap
Evidence Base
Every citation below has been checked against its source record in PubMed. The RADIAL pooled analysis explains why the radial artery (and therefore forearm collateral assessment) matters in cardiac as well as hand surgery; the anatomical and CT-angiography series quantify variant anatomy and the ~30% incomplete-arch rate; and the Allen-test studies show why the bedside test alone is neither sensitive nor specific.
Radial-Artery or Saphenous-Vein Grafts in Coronary-Artery Bypass Surgery (RADIAL pooled analysis)
- Patient-level pooled analysis of 6 randomised trials (1036 patients: 534 radial, 502 vein)
- Radial-artery grafts had lower adverse cardiac events at mean 60 months (HR 0.67, 95% CI 0.49-0.90)
- Radial grafts had a significantly lower risk of graft occlusion (HR 0.44, 95% CI 0.28-0.70)
- No difference in all-cause mortality (HR 0.90, 95% CI 0.59-1.41)
Variations of the arterial pattern in the upper limb revisited: a morphological and statistical study, with a review of the literature
- Morphological study of 192 embalmed cadavers with meta-analysis of prior series
- Brachioradial (high-origin, superficial radial) artery is the commonest major variant
- Variant patterns unified into a 12-category classification of arm and forearm arteries
Outcomes of Radial Forearm Free Flap Closure With Split-Thickness Skin Graft Versus Primary Closure
- 198 radial forearm free flap donor sites; 81 with patient-reported outcomes
- Split-thickness skin graft gave better scar quality but higher tendon-exposure rates than hatchet flap
- Hand outcome (MHOQ) scores were similar between closure techniques