Zone III Extensor Tendon Injury
- Caused by rupture of the Central Slip insertion (Zone III).
- Lateral bands subluxate volarly (below axis of rotation) to become PIPJ flexors.
- The Triangular Ligament must stretch/fail to allow band subluxation.
- Elson's Test is the most sensitive clinical sign for acute central slip injury.
- Treatment requires splinting the PIPJ in extension while allowing the DIPJ to flex (this pulls lateral bands dorsal).
- Chronic deformities (Type II/III) are very difficult to treat surgically.
- “If the patient can extend the DIPJ while the PIPJ is held at 90 degrees, the Central Slip is intact.
- “The deformity is progressive; acute injuries may not show deformity immediately.
- “The 'Buttonhole' refers to the head of the proximal phalanx popping through the lateral bands.
Acute Presentation Initially, only the central slip is ruptured. The lateral bands have NOT yet subluxed. The finger looks straight or only slightly swollen. The classic deformity takes 10-14 days to develop as the triangular ligament stretches. Missing this leads to a fixed deformity.
Elson's Test You MUST perform Elson's test on any "jammed" finger with dorsal PIPJ tenderness. Assume rupture until proven otherwise. Treat with "Safety Splinting" if unsure.
- Pathology
- Central Slip Rupture
- PIPJ
- Flexed
- DIPJ
- Hyperextended
- Pathology
- Volar Plate Laxity
- PIPJ
- Hyperextended
- DIPJ
- Flexed
- Pathology
- Volar Plate Injury
- PIPJ
- Flexed
- DIPJ
- Normal/Stiff
- Pathology
- Terminal Tendon
- PIPJ
- Normal
- DIPJ
- Flexed
SLIDEPathomechanics
Hook:The bands SLIDE down.
FLOPElson's Test Interpretation
Hook:A ruptured central slip makes the DIPJ FLOP.
Overview
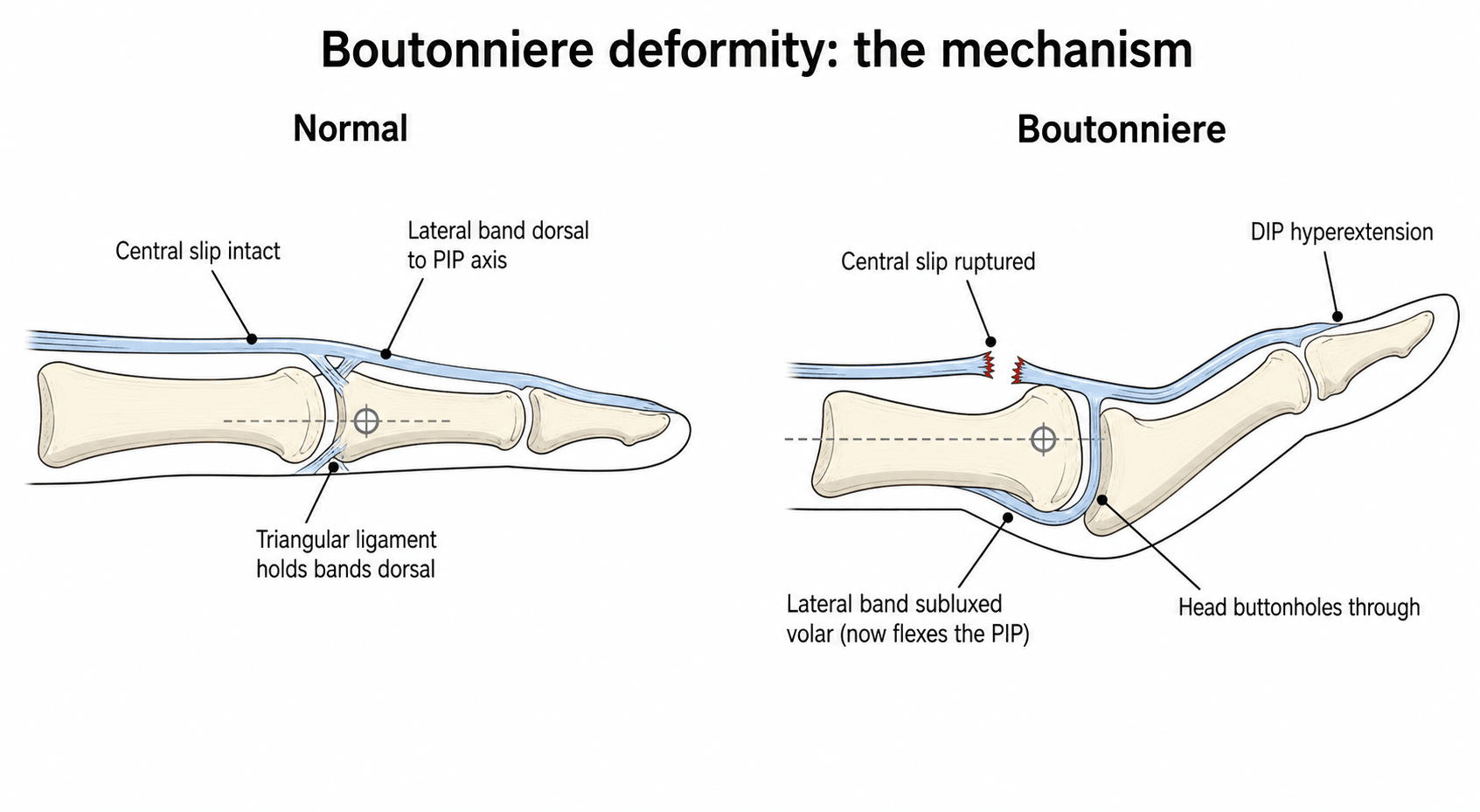
Boutonniere deformity is a flexion deformity of the PIPJ coupled with hyperextension of the DIPJ, resulting from dysfunction of the central slip of the extensor mechanism.
The term "Boutonniere" (French for Buttonhole) describes the condyles of the proximal phalanx protruding dorsally through the defect between the lateral bands.
Pathophysiology and Mechanisms
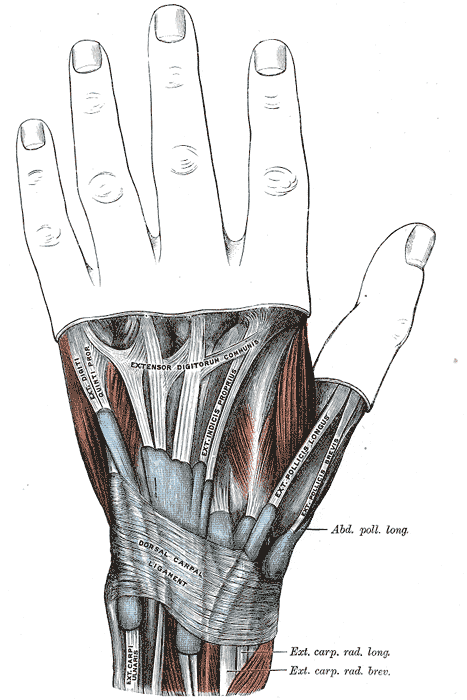
Normal Extensor Anatomy (Zone III)
- Central Slip: Inserts into the dorsal base of the Middle Phalanx. Extends the PIPJ.
- Lateral Bands: Run laterally. Join distally to form Terminal Tendon.
- Triangular Ligament: Connects the two lateral bands dorsally over the Middle Phalanx. Prevents them falling volar.
- Transverse Retinacular Ligament: Connects lateral bands to the volar plate. Pulls them volar.
- Oblique Retinacular Ligament (ORL, ligament of Landsmeer): Arises from the volar flexor sheath/proximal phalanx, passes VOLAR to the PIP axis but DORSAL to the DIP axis, and joins the terminal tendon. It links PIP and DIP motion (the "tenodesis" coupling) — PIP extension passively assists DIP extension.
The interplay between the Triangular and Transverse ligaments is critical for stability. The ORL is the structure that, when it contracts in a chronic deformity, drives the fixed DIP hyperextension.
"Zone III" is shorthand from the Verdan extensor zone classification — examiners expect you to place the injury in the system. The odd-numbered zones lie over joints and the even-numbered zones over the bones between them:
- Zone I — DIP joint (terminal tendon; injury = mallet finger).
- Zone II — middle phalanx.
- Zone III — PIP joint (central slip; injury = boutonniere).
- Zone IV — proximal phalanx.
- Zone V — MCP joint (sagittal band; injury = extensor subluxation / "fight bite").
- Zone VI — metacarpal, Zone VII — wrist/extensor retinaculum, Zone VIII — distal forearm.
- The thumb has its own zones (TI to TV).
So boutonniere is the Zone III lesion, sitting between mallet finger (Zone I) and the sagittal-band injuries (Zone V) — a common spot-the-zone viva.
Classification Systems
Burton Classification
- Stage I: Supple. Passive correction of PIPJ is possible.
- Stage II: Fixed deformity. Contracture of lateral bands.
- Stage III: Fixed deformity + Arthritis.
Stage I is treatable with splinting. Stage II requires surgical release or serial casting.
Clinical Assessment
Examination
- Deformity: Look for PIP flexion and DIP hyperextension.
- Open: Check for dorsal laceration.
- Tenderness: Dorsal base of Middle Phalanx.
- Boyes Test (ORL tightness): Hold the PIP in full extension and passively flex the DIP. Limited DIP flexion with the PIP extended that improves when the PIP is flexed = a tight oblique retinacular ligament. This identifies the chronic secondary contracture that must be released for the DIP to regain motion. (Contrast: Elson's test diagnoses the central slip rupture itself.)
- Passive correctability: Can the PIP be passively brought to full extension? Yes = supple (Burton I, splint); No = fixed (Burton II, regain extension first).
Early changes can be subtle. Compare with the other hand.
The lateral bands that subluxate in boutonniere are not separate structures — they are largely the continuation of the intrinsic muscles (the interossei and lumbricals), which insert into the extensor hood and lateral bands. The intrinsics therefore flex the MCP and extend the IP joints through this mechanism.
- Relevance: because the lateral bands carry intrinsic force, a chronically subluxated band and a tight intrinsic system contribute to the deformity and to limited PIP motion.
- Intrinsic tightness (Bunnell) test: passively flex the PIP first with the MCP held in extension (intrinsics on stretch), then with the MCP flexed (intrinsics relaxed). Less PIP flexion with the MCP extended = intrinsic tightness; equal flexion in both positions points instead to a capsular/extrinsic (PIP joint) cause.
- This separates an intrinsic contracture from a true PIP joint contracture — a different problem from the central-slip lesion itself, and one that determines whether release targets the intrinsics or the joint.
Investigations
Radiology
- Views: AP and Lateral.
- Findings:
- Avulsion: May see bony fleck from dorsal base of P2.
- Joint: Assess for OA (Stage III).
- Subluxation: Volar subluxation of middle phalanx may be visible.
- Soft Tissue: Swelling dorsal to PIPJ.
Bony avulsion is treated similarly to tendinous rupture (Splinting), unless huge displaced fragment.

Management Algorithm
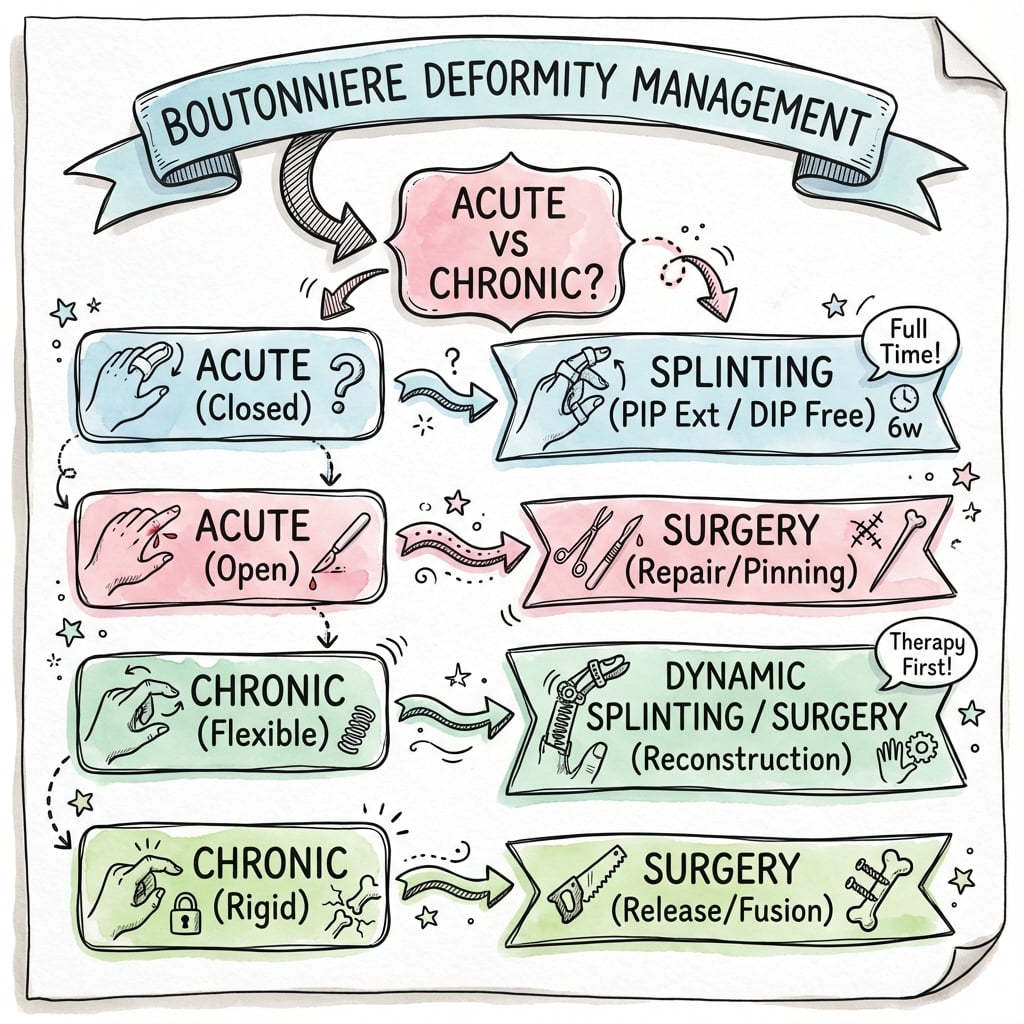
Conservative Management (Stage I)
- Goal: Restore central slip continuity + Move lateral bands dorsal.
- Splint: PIPJ in FULL extension (block extension).
- DIPJ: LEFT FREE. Must be flexed actively.
- Mechanism: Active DIP flexion while PIP is extended pulls the lateral bands distally and dorsally (via Triangular ligament), reducing them.
- Duration: 6 weeks continuous.
- Follow-up: Weekly review to ensure compliance and splint fit.
This is known as the "Safety Splint" position.
FREEManagement Goals
Hook:FREE the DIPJ to fix the PIPJ.
Surgical Considerations
Acute Repair
- Approach: Dorsal zig-zag incision centered over PIPJ.
- Repair: 4-0 non-absorbable mattress suture into central slip.
- Fixation: K-wire across PIPJ in extension for 3-4 weeks.
- Triangular Ligament: Must be repaired to prevent lateral band subluxation.
- Closure: Skin closure over buried sutures.
Do not overtighten the central slip, or you will cause a DIPJ extension lag. The goal is merely to appose the tendon ends, not to create tension.
Complications
- Stiffness: Loss of PIP flexion is common after prolonged splinting.
- DIPJ Lag: If lateral bands are tight.
- Recurrence: If triangular ligament is incompetent.
- Skin Necrosis: From tight splints.
- Hypersensitivity: Often managed with desensitization.
- DIPJ Hyperextension: If the central slip is overtightened during repair.
- Quadriga Effect: If the FDP is tethered.
- Infection: Post-operative, or from the initial injury (human bite?).
Rehabilitation
- Splint: PIPJ straight (full extension). DIPJ left free.
- Exercises: Active DIPJ flexion 20 reps every hour while awake.
- Mechanism: Active DIP flexion pulls lateral bands distally and dorsally via the oblique retinacular ligament, encouraging dorsal relocation.
- Hygiene: Remove splint 1-2 times daily for skin care while holding PIP extended.
- Edema Control: Coban wrap, elevation.
- Wean: Start gentle active PIP flexion (20-30°) initially.
- Progression: Increase arc 10° per week based on extensor lag.
- Monitor: If extensor lag greater than 10° recurs, back to full-time splint.
- Night Splint: Continue at night for additional 4 weeks.
- Exercises: Active assisted and passive ROM.
- Full Activity: Gradual return by 12 weeks.
- Grip Strengthening: Theraputty, grip exercises.
- Night Splint: May continue for 3-6 months in some patients.
- Functional Goals: Return to sport/work-specific activities.
Splint Types
- Cylinder Splint: Simple, inexpensive, good for initial immobilization.
- Capener Splint: Dynamic splint with spring mechanism for chronic deformity.
- Safety Pin Splint: Low-profile, allows more function.
- Serial Casting: For fixed Stage II deformity to gain passive extension.
Red Flags During Rehabilitation
- Extensor lag greater than 15° on weaning
- Increasing flexion contracture
- Pain at terminal extension (tendon healing issue)
- Skin breakdown under splint
Prognosis
- Acute: Excellent prognosis if splinted early (within 3 weeks of injury).
- Chronic: Poor prognosis. Reconstruction often swaps deformity for stiffness.
- Bony: Good prognosis with union if avulsion fragment adequately reduced.
- Arthritis: Long term consequence of uncorrected subluxation.
- Function: Even with some residual deformity, hand function can remain good if range is preserved.
- Patient Satisfaction: Often higher with a slightly deformed but mobile finger than a straight but stiff one.
- Chronic Pain: Rare, unless secondary arthritis develops.
- Cosmesis: The main complaint for many patients.
Prognostic Factors
- Time to Treatment: Early treatment (less than 3 weeks) = better outcomes.
- Stage at Presentation: Stage I has superior outcomes compared to Stage II/III.
- Compliance: Poor splint compliance leads to recurrence.
- Age: Younger patients heal better but may be less compliant.
- Occupation: Manual workers may require longer rehabilitation.
Guidelines, Registries & Global Practice
Global Epidemiology
- Traumatic: Closed central slip injury is a ball-sport and contact-sport injury worldwide (basketball, volleyball, football/soccer, rugby, Australian football, cricket, handball) from forced PIP flexion against an actively extending finger, plus axial-load "jamming". Peak incidence in active adults aged 20–40.
- Open: Lacerations over the dorsal PIP (knife, glass, machinery, bites) account for the open subgroup and are at high risk of being missed.
- Inflammatory: Rheumatoid arthritis is the leading non-traumatic cause and is typically bilateral and multi-digit; psoriatic arthritis and SLE contribute. With modern biologic disease control the incidence of advanced rheumatoid boutonniere has fallen.
Side-by-Side Guidance (where emphasis differs)
There is no single randomised-trial-based society guideline for boutonniere; the consensus across hand-surgery bodies is convergent.
- Core recommendation
- Acute closed: PIP extension splint, DIP free for active flexion; surgery for open / displaced bony avulsion / failed conservative
- Practical emphasis
- Evidence-based reviews caution that surgery trades PIP extension for flexion
- Core recommendation
- Same splinting principle; emphasises early diagnosis with Elson test and hand-therapy-led splinting
- Practical emphasis
- Hand therapists fabricate and supervise relative-motion / PIP extension orthoses
- Core recommendation
- Clinical diagnosis (Elson), splint non-displaced injuries, restore passive extension before reconstructing fixed deformity
- Practical emphasis
- Staged approach to chronic / fixed deformity
- Core recommendation
- Central-slip-protective splinting; reserve reconstruction for selected chronic cases
- Practical emphasis
- Realistic goal-setting; function over cosmesis
Registry and Outcome Notes
- No implant registry applies — boutonniere management is soft-tissue and splint-based, so arthroplasty/implant registries (NJR, AJRR, AOANJRR) do not capture it. Evidence is drawn from cadaveric biomechanical work and surgical case series rather than registry data.
- Surgical series (e.g. Towfigh & Gruber, 172 patients) report roughly two-thirds excellent/good results after reconstruction, with a consistent minority of satisfactory/poor outcomes — a pattern echoed across the literature.
High- vs Limited-Resource Practice Variation
- High-resource settings: Custom thermoplastic and relative-motion orthoses fabricated by certified hand therapists; ultrasound or MRI available for equivocal cases; structured graded rehabilitation.
- Limited-resource settings: Prefabricated splints, low-cost aluminium-foam (Zimmer-type) or plaster cylinder casts, and serial casting deliver equivalent biomechanics — the central slip does not "know" what the splint is made of. Early, correctly positioned, consistently worn immobilisation matters far more than splint cost.
- Universal barrier: Compliance with 6 weeks of continuous PIP extension splinting (heat, skin maceration, manual-work demands) is the dominant determinant of success in every health system; patient education and review drive outcomes more than any device.
Controversies and Areas of Uncertainty
There are no randomised controlled trials comparing splinting regimens or operative techniques in boutonniere deformity. Recommendations rest on cadaveric biomechanics, case series, and expert consensus — a frequent examiner probe.
- Optimal splint position and type: Static PIP extension splinting is standard, but relative-motion (yoke) splinting and serial casting all have advocates. There is no high-level evidence that any one orthosis is superior, and the construct material (thermoplastic vs aluminium-foam vs cast) is far less important than position and compliance.
- Bony avulsion threshold for surgery: The fragment size or articular involvement that mandates fixation over splinting is not precisely defined; most non-displaced or small avulsions do well with extension splinting, mirroring tendinous injury.
- Surgery for chronic deformity: Reconstruction reliably trades PIP extension for flexion. Whether to operate at all in a functional but cosmetically displeasing finger is genuinely debated — many authorities advise against surgery when the hand is functional.
- Choice of reconstruction: Anatomical central slip reconstruction, lateral band relocation (Littler), terminal/Dolphin tenotomy (Fowler-type), and tendon transfer/graft each have proponents; comparative data are limited and largely retrospective.
- Imaging role: Ultrasound and MRI can demonstrate the central slip, but the diagnosis remains clinical (Elson test). Whether imaging changes management in equivocal closed cases is unproven.
MCQ Practice Points
Q: What is the hallmark finding of a positive Elson's test? A: Rigid extension of the DIPJ when PIPJ is flexed (due to lateral band over-pull).
Q: Which structure limits the dorsal migration of the lateral bands? A: The Transverse Retinacular Ligament.
Q: In splinting for Boutonniere deformity, what is the position of the DIPJ? A: Free / Flexed. (Active flexion recruits lateral bands).
Q: What defines a Stage II deformity? A: Fixed flexion contracture (not passively correctable).
Q: Why do the lateral bands become PIPJ flexors in Boutonniere? A: They subluxate volar to the axis of rotation of the PIPJ, converting their pull from extension to flexion.
Q: How long should a Boutonniere splint be worn continuously? A: 6 weeks continuous, then progressive weaning with night splinting for months.
Q: Which structure, when contracted in a chronic boutonniere, produces the fixed DIP hyperextension, and which test detects it? A: The oblique retinacular ligament (of Landsmeer); a positive Boyes test (DIP flexion limited with the PIP held extended, improving with PIP flexion).
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A basketball player presents with a swollen PIPJ. X-ray is normal. The finger looks straight. What is your exam?”
“A patient presents 3 months post injury with a fixed 45 degree flexion deformity of the PIPJ and hyperextended DIPJ. Management?”
“A patient has a deep laceration over the dorsal PIPJ. Tendon is visible. Mechanism is a glass cut.”
“A 55-year-old female with known rheumatoid arthritis presents with bilateral Boutonniere deformities affecting the index and middle fingers of both hands. Her PIP joints are passively correctable. How do you manage her?”
Classification
- Stage I: Supple (Splint)
- Stage II: Fixed (Cast/Release)
- Stage III: Arthritis (Fuse)
- Pseudo: Volar plate injury
Management
- Splint PIP Extension
- DIP Free (Exercise)
- 6 Weeks Continuous
- Elson's Test is Key
Anatomy
- Central Slip Rupture
- Lateral Bands Volar
- Triangular Lig Failure
- Zone III
Evidence Base
Elson's Test — Original Description (Landmark)
- Closed central slip rupture is easily missed until the late buttonhole deformity appears, by which time Boyes' test (DIP flexion with PIP held extended) is already positive
- New test: with the PIP flexed 90° over a table edge, the patient extends against resistance — absence of PIP extension force PLUS fixed (rigid) DIP extension signals complete central slip rupture
- Allows diagnosis in the acute phase, before deformity develops, when treatment outcomes are best
Biomechanics of the Acute Boutonniere (Cadaveric)
- Central slip detachment alone produced only loss of PIP extension — NOT a boutonniere deformity
- A boutonniere developed only when the central slip, the triangular ligament, AND the transverse/oblique interosseous hood fibres were all divided
- Lateral band subluxation volar to the PIP axis of rotation is required to generate the deformity
Extensor Tendon Injuries at the PIP Joint (Zone III)
- Acute closed central slip injuries are a clinical diagnosis (Elson test) after bony injury is excluded radiographically
- Non-displaced avulsions and lacerations can be splinted; displaced avulsions and complex injuries are surgical
- Fixed deformities must have full passive PIP extension restored (hand therapy or release) BEFORE any tendon reconstruction