Median Nerve Entrapment | Most Common Compression Neuropathy | 9 Tendons + 1 Nerve
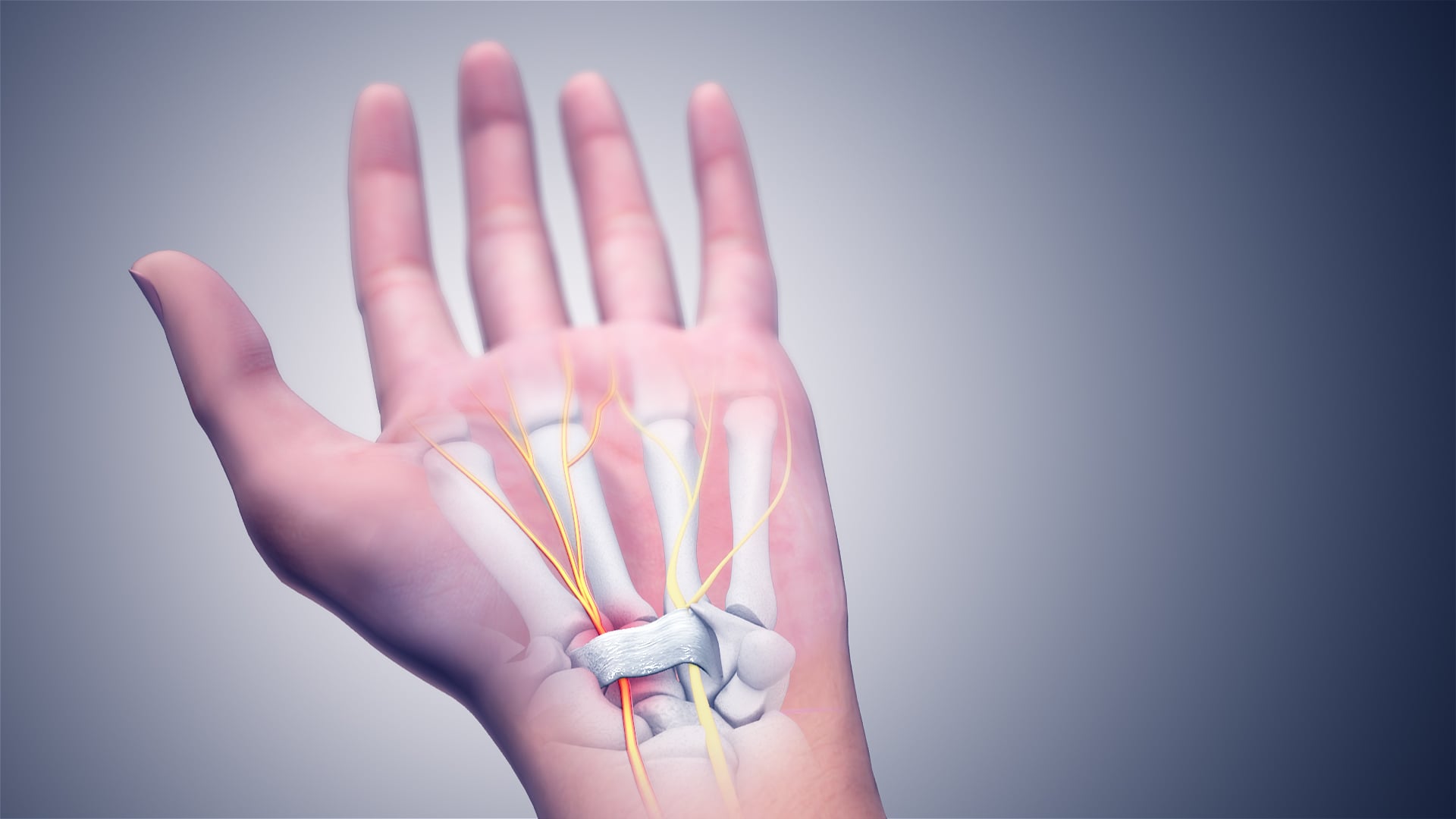
- Carpal tunnel contents: 9 flexor tendons (4 FDS + 4 FDP + FPL) + median nerve (most superficial)
- Thenar atrophy = SEVERE: APB wasting indicates axonal loss, requires urgent surgery, incomplete recovery
- Palmar cutaneous branch spared: Branches proximal to tunnel, preserves palmar sensation
- Phalen's test: Wrist flexion 60 seconds reproduces symptoms (68% sensitive, 73% specific)
- NCS criteria: Motor latency greater than 4.5ms, sensory latency greater than 3.5ms across wrist
- “Nocturnal paresthesia with flick sign = virtually diagnostic
- “Durkan's compression test (87% sensitive) better than Phalen's or Tinel's
- “Open vs endoscopic CTR = similar outcomes, faster recovery with endoscopic
- “Pillar pain (10-20%) = most common post-op complication, resolves by 3 months
APB wasting indicates SEVERE CTS with axonal damage. This is an urgent surgical indication. Do NOT delay with conservative measures. Counsel patient that motor recovery may be incomplete despite surgery. Sensory symptoms improve but thenar strength may not fully return.
Floor = carpal bones (scaphoid, trapezium radially; pisiform, hamate ulnarly). Roof = transverse carpal ligament (flexor retinaculum). Contents = 10 structures: 4 FDS + 4 FDP + FPL + median nerve (most superficial and radial). Median nerve is at highest risk.
Palmar sensation preserved in true CTS because the palmar cutaneous branch arises 5cm proximal to wrist crease and passes superficial to transverse carpal ligament. Use this to distinguish from C6 radiculopathy or more proximal median nerve lesions.
NCS confirms diagnosis and grades severity. Prolonged distal motor latency (greater than 4.5ms) and sensory latency (greater than 3.5ms). EMG shows denervation in thenar muscles if severe. May be normal in early mild disease. Compare to contralateral and ulnar nerve.
9 TENDONS + 1 NERVE = 10Carpal Tunnel Contents
Hook:9 tendons + 1 nerve = 10 structures. Median nerve is number 10 and most superficial!
LOAFMedian Nerve Motor Supply (LOAF)
Hook:LOAF muscles = what you can't do when median nerve fails - can't hold a loaf of bread!
MEDIAN TRAPCTS Risk Factors
Hook:Median nerves get caught in a MEDIAN TRAP!
PDTProvocative Tests - PDT
Hook:PDT = Phalen's, Durkan's, Tinel's - test them all but Durkan's is best!
Overview and Epidemiology
Carpal tunnel syndrome (CTS) is the most common peripheral nerve compression neuropathy, resulting from compression of the median nerve beneath the transverse carpal ligament at the wrist. The condition affects 3-6% of the general population and accounts for approximately 90% of all entrapment neuropathies.
Epidemiology
- Female predominance: 3:1 ratio (hormonal factors, smaller carpal tunnel)
- Peak incidence: 40-60 years of age
- Bilateral involvement: 50-60% of cases
- Dominant hand: Typically more symptomatic
- Occupational: Repetitive wrist flexion, vibration exposure
- Idiopathic: Greater than 50% of cases (no identifiable cause)
- Diabetes mellitus: 10% prevalence in diabetics vs 3% general population
- Pregnancy: 2-7% incidence, usually resolves post-partum
- Hypothyroidism: Myxedema deposition in tunnel
- Rheumatoid arthritis: Synovial proliferation
- Obesity: BMI greater than 30 increases risk 2-fold
- Previous wrist fracture: Distal radius fractures (especially malunion)
CTS is the most frequently tested nerve compression in orthopaedic exams. You must know: (1) the 10 structures in the tunnel, (2) why palmar sensation is spared, (3) provocative test sensitivity/specificity, (4) NCS criteria, (5) surgical anatomy including recurrent motor branch variations.

Anatomy
Carpal Tunnel Anatomy
The carpal tunnel is a fibro-osseous canal at the wrist formed by the concave arch of the carpal bones (floor) and the transverse carpal ligament (roof).
- Floor: Carpal bones arranged in two rows
- Proximal row: Scaphoid (radial), lunate, triquetrum, pisiform (ulnar)
- Distal row: Trapezium (radial), trapezoid, capitate, hamate (ulnar)
- Roof: Transverse carpal ligament (flexor retinaculum)
- Attachments: Scaphoid tubercle and trapezium (radial) to pisiform and hook of hamate (ulnar)
- Length: Approximately 2.5-3cm
- Thickness: 2-3mm (thickens with age and loading)
- Median nerve - most superficial and radial 2-5. Four FDS tendons - superficial layer 6-9. Four FDP tendons - deep to FDS
- FPL tendon - radial to FDP tendons
The median nerve lies most superficial in the tunnel, directly beneath the transverse carpal ligament. This makes it vulnerable to compression from any increase in tunnel pressure or decrease in tunnel volume. The nerve is also the most radial structure, lying between FPL (radial) and FDS to index finger.
Median Nerve Anatomy
- Enters forearm between two heads of pronator teres
- Lies deep to FDS in forearm
- Gives off anterior interosseous nerve (pure motor) in proximal forearm
- Gives off palmar cutaneous branch 5-6cm proximal to wrist crease
- Enters carpal tunnel deep to transverse carpal ligament
- Exits tunnel and gives off recurrent motor branch to thenar muscles
- Divides into digital branches for sensation
- Arises 5cm proximal to wrist crease
- Passes superficial to transverse carpal ligament
- Supplies sensation to thenar and central palm
- Spared in true CTS - key diagnostic feature
- Anatomical variations (important for surgery):
- Extraligamentous (50%): Exits distal to ligament (safest)
- Subligamentous (30%): Travels under ligament then exits
- Transligamentous (20%): Pierces through ligament (at risk during release)
- Supplies thenar muscles (LOAF): Lumbricals 1-2, Opponens pollicis, Abductor pollicis brevis, Flexor pollicis brevis (superficial head)
Pathophysiology
Pressure-Ischemia Cascade
Pressure-Ischemia Sequence:
-
Increased Intracarpal Pressure
- Normal pressure: 2-10 mmHg
- CTS pressure: 30-110 mmHg (threshold for symptoms = 30 mmHg)
- Wrist flexion/extension increases pressure further
-
Venous Congestion
- Increased pressure → venous obstruction
- Edema within epineurium
- Further increases pressure (vicious cycle)
-
Ischemia and Demyelination
- Chronic ischemia → focal demyelination
- Reversible at this stage with decompression
- Manifests as sensory symptoms and prolonged latencies on NCS
-
Axonal Damage
- Severe chronic compression → axonal loss
- Irreversible - leads to thenar atrophy
- Wallerian degeneration occurs
- Recovery limited even after decompression
Nocturnal symptoms occur because: (1) During sleep, wrists naturally fall into flexion which increases tunnel pressure, (2) Dependent position of hands causes venous congestion, (3) Recumbent position redistributes fluid increasing edema. This is why night splinting in neutral position is effective.
Classification Systems
Clinical Severity Classification
- Symptoms
- Intermittent paresthesia, nocturnal symptoms
- Examination
- Normal sensation, normal motor, positive provocative tests
- Management
- Splinting 6-8 weeks, activity modification
- Symptoms
- Persistent paresthesia, occasional weakness
- Examination
- Sensory deficit in median distribution, positive Phalen's/Durkan's
- Management
- Injection trial OR proceed to surgery
- Symptoms
- Constant numbness, weakness, thenar wasting
- Examination
- Thenar atrophy, APB weakness, impaired 2PD
- Management
- Urgent carpal tunnel release
Clinical severity guides urgency of treatment. Mild cases warrant conservative trial. Severe cases require urgent surgery.
Acute CTS is a separate entity from the chronic compressive disease graded above, and it is a surgical emergency that examiners love to test - never manage it down the splint-then-electrodiagnostics-then-elective-surgery pathway. It is a closed-compartment phenomenon: a sudden rise in intracarpal pressure damages the median nerve over hours.
distal radius fracture (especially high-energy injuries, and iatrogenically from an over-flexed, ulnar-deviated "Cotton-Loder" reduction position), perilunate or lunate dislocation, carpal/crush trauma, bleeding into the tunnel (anticoagulation, haemophilia, vascular injury), high-pressure injection injury, local infection, burns, and a tight constricting cast or dressing.
rapidly progressive, severe and unrelenting median-territory pain and paraesthesia, pain that is out of proportion and worsened by passive finger extension - in contrast to the intermittent, nocturnal, slowly progressive symptoms of chronic CTS. Worsening or non-resolving median symptoms after a distal radius fracture reduction are acute CTS until proven otherwise.
do NOT wait for nerve conduction studies. Split or remove constricting casts and dressings, take the wrist out of excessive flexion, elevate, and proceed to urgent open carpal tunnel decompression (combined with fracture stabilisation when relevant). Delay risks permanent median nerve injury. (Note this differs from the transient median paraesthesia that settles immediately on reducing a fracture, which can be observed.)
Clinical Assessment
History
- Nocturnal paresthesia: Waking at night with numbness (75% of patients)
- Flick sign: Shaking or flicking hand to relieve symptoms (pathognomonic)
- Distribution: Thumb, index, middle, and radial half of ring finger
- Palmar sensation preserved: Key distinguishing feature
- Progression: Sensory → motor (weakness, clumsiness, dropping objects)
- Sustained wrist flexion (driving, reading, phone use)
- Repetitive gripping or pinching
- Vibration exposure
- Cold weather
- Pain radiating to forearm or shoulder (25%)
- Difficulty with fine motor tasks (buttoning, writing)
- Weakness of pinch grip
The flick sign (patient shakes or flicks hand to relieve symptoms) has 93% sensitivity and 96% specificity for CTS. Ask: "What do you do when symptoms wake you at night?" If they demonstrate shaking/flicking, this is virtually diagnostic.
Examination
- Thenar muscle bulk: Compare both hands with palms up
- APB wasting: Depression at thenar eminence
- Skin changes: Trophic changes in severe cases
- Light touch: Median nerve distribution (radial 3.5 digits palmar)
- Two-point discrimination: Greater than 6mm abnormal (normal 2-5mm)
- Semmes-Weinstein monofilaments: Objective sensory testing
- Compare to ulnar territory: Little finger as control
- Abductor pollicis brevis: KEY MUSCLE
- Patient places hand palm-up on table
- Ask to point thumb to ceiling against resistance
- Palpate APB during contraction
- Grade strength (0-5 scale)
- Opponens pollicis: Touch thumb tip to little finger tip
- Pinch strength: May be weak in advanced disease
- Technique
- Maximum wrist flexion 60 seconds
- Positive Finding
- Paresthesia in median distribution
- Sensitivity
- 68%
- Specificity
- 73%
- Technique
- Maximum wrist extension 60 seconds
- Positive Finding
- Paresthesia in median distribution
- Sensitivity
- 48%
- Specificity
- 76%
- Technique
- Tap over carpal tunnel at wrist crease
- Positive Finding
- Electric sensation in median distribution
- Sensitivity
- 50%
- Specificity
- 77%
- Technique
- Direct compression over tunnel 30 seconds
- Positive Finding
- Paresthesia in median distribution
- Sensitivity
- 87%
- Specificity
- 90%
- Technique
- BP cuff inflated above systolic for 60s
- Positive Finding
- Reproduction of symptoms
- Sensitivity
- 70%
- Specificity
- 80%
Differential Diagnosis:
- Distinguishing features
- Nocturnal paraesthesia, flick sign, median digits
- Palmar sensation
- Spared (palmar cutaneous branch proximal)
- Key test
- Durkan's compression; NCS
- Distinguishing features
- Neck pain, dermatomal arm pain, reflex changes (biceps/triceps)
- Palmar sensation
- Often affected (proximal to branch)
- Key test
- Spurling's test; cervical MRI
- Distinguishing features
- Proximal forearm pain, NO night symptoms, FDS/FPL/AIN may be weak
- Palmar sensation
- Affected (lesion proximal to branch)
- Key test
- Resisted pronation/FDS provocation
- Distinguishing features
- Provoked by arm elevation, often ulnar (C8-T1) distribution
- Palmar sensation
- Variable
- Key test
- Roos/EAST test; Adson's
- Distinguishing features
- Little and ulnar-ring finger, hypothenar/interossei wasting
- Palmar sensation
- Median palm spared (ulnar territory affected)
- Key test
- Elbow flexion test; Froment's; NCS
- Distinguishing features
- Symmetrical stocking-glove, systemic (diabetes, alcohol)
- Palmar sensation
- Affected diffusely, not median-specific
- Key test
- Bloods, generalised NCS
- Distinguishing features
- Radial-sided wrist PAIN (not numbness), 1st extensor compartment
- Palmar sensation
- Normal
- Key test
- Finkelstein / Eichhoff test
- Distinguishing features
- Mechanical thumb-base pain, crepitus, grind
- Palmar sensation
- Normal
- Key test
- Grind test; radiographs
- Bilateral severe symptoms with rapid onset → consider cervical myelopathy
- Numbness in palmar region → not true CTS, consider proximal lesion
- Weakness without sensory symptoms → consider motor neuron disease or C8 radiculopathy
- Atypical distribution → consider alternative diagnosis
A classic examinable concept absent from the simple "CTS versus cervical radiculopathy" differential: the two can coexist and compound each other. The double-crush hypothesis (Upton and McComas, 1973) proposes that a single axon compressed at one point becomes more vulnerable to a second, often subclinical, compression elsewhere along its course - impaired axoplasmic flow from the proximal lesion lowers the threshold for symptoms at the distal site, so two mild lesions together produce disproportionate symptoms.
- A proximal lesion - most commonly C6/C7 cervical radiculopathy, but also thoracic outlet or a proximal median (pronator) compression - frequently coexists with median compression at the wrist; either lesion alone may be mild or subclinical.
- It is a recognised explanation for persistent symptoms after a technically complete carpal tunnel release - the unaddressed proximal lesion remains. When release fails to relieve symptoms, or when symptoms are atypical, extend beyond the median territory, or include neck/proximal arm features, actively look for a proximal source (cervical spine examination and imaging, proximal nerve conduction studies).
- A "reverse" double crush (a distal lesion sensitising a proximal segment) is also described.
always consider a second compression site - especially the cervical spine - when CTS presentation is atypical or surgery does not deliver the expected relief.
Investigations
Nerve Conduction Studies (NCS)
Gold standard for diagnosis confirmation and severity grading.
- Atypical presentation
- Bilateral severe symptoms
- Confirm diagnosis before surgery
- Medico-legal cases
- Young patients (under 40)
- Assess severity and prognosis
- Sensory NCS: Orthodromic (digit to wrist) or antidromic (wrist to digit)
- Stimulate at wrist, record from index or middle finger
- Measure distal sensory latency and amplitude
- Normal latency less than 3.5ms
- Motor NCS: Stimulate median nerve at wrist, record from APB
- Measure distal motor latency
- Normal latency less than 4.5ms
- Compare to ulnar nerve (ADM)
- Prolonged median sensory latency greater than 3.5ms
- Prolonged median motor latency greater than 4.5ms
- Median-ulnar sensory latency difference greater than 0.5ms
- Median-ulnar motor latency difference greater than 1.0ms
Ultrasound
- Cross-sectional area (CSA): Greater than 10-12mm² at tunnel inlet
- Flattening ratio: Anterior-posterior to medial-lateral diameter
- Bowing of retinaculum: Displacement greater than 2mm
- Dynamic assessment: Nerve movement with finger flexion
- Identify masses: Ganglion, persistent median artery
- Non-invasive, no electrical stimulation
- Real-time visualization
- Identifies structural causes
- Can guide injection
- Operator-dependent
- Does not assess function
- Cannot quantify severity like NCS
MRI
- Suspected mass lesion
- Atypical presentation
- Failed surgery
- Research purposes
- T2 hyperintensity of nerve
- Nerve enlargement
- Muscle edema (if acute denervation)
- Thenar atrophy (chronic)
Laboratory Studies
Screen for associated conditions:
- TSH (hypothyroidism)
- HbA1c (diabetes)
- Rheumatoid factor/anti-CCP (rheumatoid arthritis)
- Serum protein electrophoresis (amyloid if suspected)
Management Algorithm
Treatment Pathway
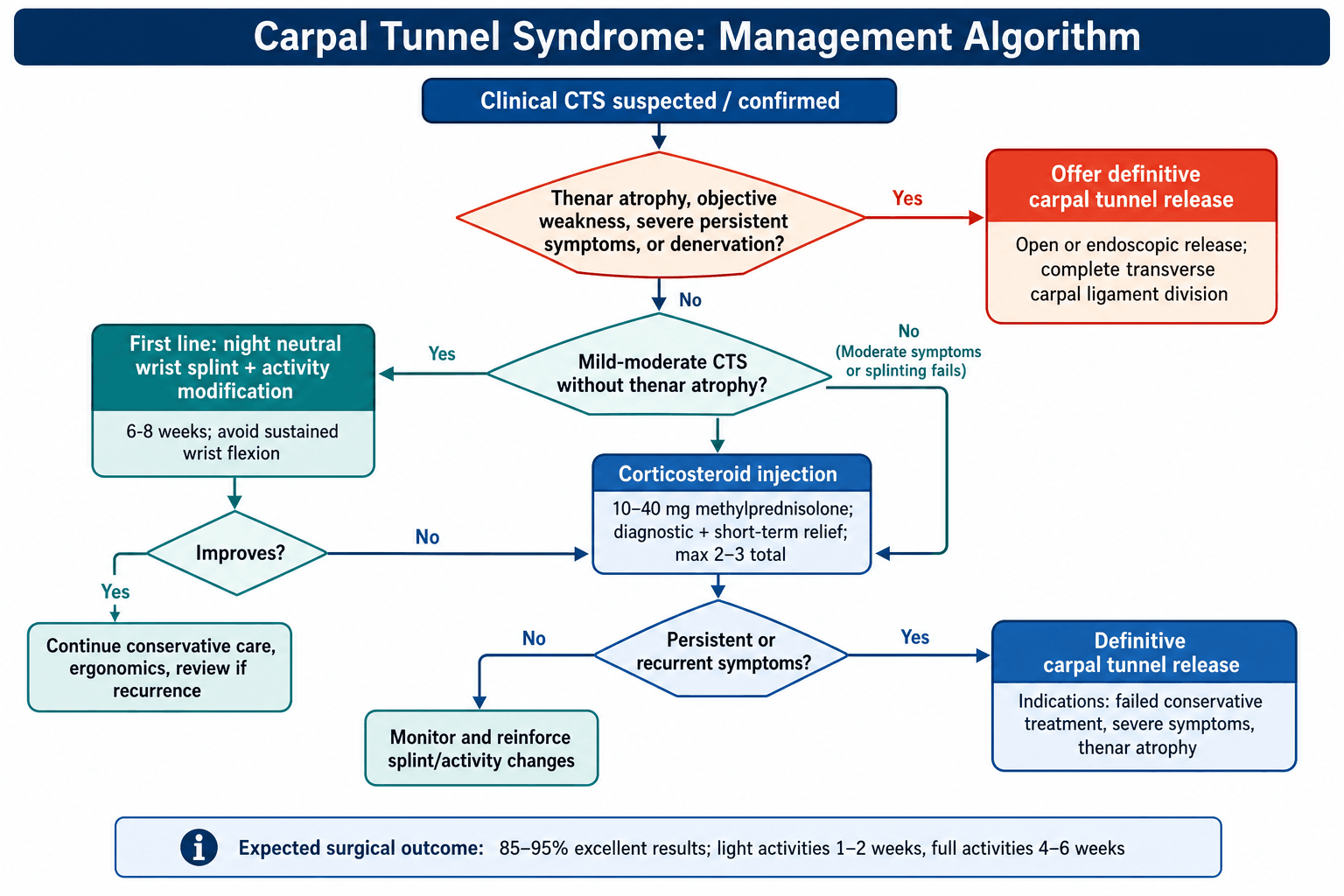
Mild to moderate CTS without thenar atrophy:
- Night splinting in neutral wrist position for 6-8 weeks
- Activity modification (avoid sustained flexion)
- NSAIDs for symptom control (limited evidence)
- Consider corticosteroid injection if splinting fails
Success rate: 30-50% with splinting, 60-80% short-term with injection
If splinting fails or moderate symptoms:
- Single injection 10-40mg methylprednisolone into tunnel
- Ulnar to palmaris longus, proximal to wrist crease
- Avoid intraneural injection (test with small volume first)
- Relief within days, lasts weeks to months
- Can repeat once, maximum 2-3 injections total
Success rate: 70-80% short-term relief, 20-30% long-term
Indications: Severe symptoms, thenar atrophy, failed conservative treatment
- Open or endoscopic carpal tunnel release
- Day surgery under local or regional anesthesia
- Divide transverse carpal ligament completely
- Return to light activities 1-2 weeks, full activities 4-6 weeks
Success rate: 85-95% excellent outcomes
Night Splinting
Technique:
- Wrist in neutral (0-5 degrees extension) NOT flexion or hyperextension
- Worn during sleep for minimum 6-8 weeks
- Full-time splinting not superior to night-only
- More effective in mild disease, pregnancy, recent onset
- Success rate 30-50% at 6 months
Activity Modification
Recommendations:
- Avoid sustained wrist flexion (computer use, driving)
- Take frequent breaks from repetitive tasks
- Ergonomic adjustments (keyboard height, mouse position)
- Modify sports grip (cycling, tennis)
Conservative management with splinting and activity modification is appropriate first-line treatment for mild to moderate CTS without thenar atrophy.
Surgical Technique
Open Carpal Tunnel Release
- Failed conservative treatment (6+ months)
- Moderate to severe NCS changes
- Thenar muscle atrophy or weakness
- Persistent disabling symptoms
- Patient preference for definitive treatment
- Acute carpal tunnel (trauma, hemorrhage)
- Supine position, arm on hand table
- Upper arm tourniquet (250 mmHg)
- Prep and drape hand and forearm
- Local anesthetic (1% lidocaine with epinephrine) OR regional block
- Mark incision with wrist flexed then extended to avoid transverse crease
- Longitudinal incision in line with radial border of ring finger
- From distal wrist crease to mid-palm
- Length 3-4cm (extended release) or 2-3cm (mini-open)
- Stay ulnar to thenar crease
- Avoid crossing wrist crease transversely (hypertrophic scar)
-
Skin and Subcutaneous Dissection
- Incise skin with knife
- Identify and protect palmar cutaneous branch (travels superficially)
- Divide palmar fascia in line with incision
- Identify transverse carpal ligament (white, fibrous band)
-
Identify Landmarks
- Palmaris longus: Surface landmark (ulnar to this)
- Flexor carpi radialis: Radial boundary (avoid)
- Ulnar neurovascular bundle: Ulnar boundary (stay radial to this)
-
Divide Transverse Carpal Ligament
- Insert mosquito forceps UNDER ligament to protect nerve
- Elevate ligament away from nerve
- Divide ligament with knife or scissors under direct vision
- Release distally to superficial palmar arch (feel "give")
- Release proximally into antebrachial fascia (2cm proximal to crease)
- Ensure COMPLETE division (run probe underneath)
-
Inspect Tunnel Contents
- Visualize median nerve (should be flattened, may be hourglass)
- Check for anatomical variations: Bifid nerve, persistent median artery
- Look for masses: Ganglion, lipoma
- Assess synovium: Proliferative synovitis may need debulking
- DO NOT perform internal neurolysis (increases scar, worse outcomes)
-
Hemostasis and Closure
- Release tourniquet
- Achieve meticulous hemostasis (prevents hematoma)
- DO NOT repair transverse carpal ligament (would recreate compression)
- Close skin only with interrupted 4-0 nylon sutures
- Apply bulky dressing in functional position
- Allow immediate finger ROM
- Divide ligament completely (incomplete release = most common cause of failure)
- Extend release into forearm fascia proximally
- Extend release to superficial arch distally
- Protect recurrent motor branch (exits ulnar side of nerve distally)
- If thenar muscles not visible, assume extraligamentous recurrent branch
- Palmar cutaneous branch: Superficial, easily injured with skin incision
- Recurrent motor branch: Variable course (transligamentous in 20%)
- Superficial palmar arch: Distal limit of release
- Ulnar nerve and artery: Ulnar boundary of incision
Meticulous attention to anatomical landmarks and direct visualization of the transverse carpal ligament ensures safe and complete release with excellent long-term outcomes.
Complications
- Incidence
- 10-20%
- Presentation
- Pain at thenar/hypothenar eminence for 3-6 months
- Management
- Reassurance, hand therapy, resolves spontaneously
- Incidence
- 2-5%
- Presentation
- Persistent symptoms unchanged from pre-op
- Management
- Repeat NCS, revision surgery if confirmed
- Incidence
- 5-10%
- Presentation
- Tender incision scar for months
- Management
- Desensitization, silicone gel, massage
- Incidence
- 0.1-0.5%
- Presentation
- Immediate post-op numbness or weakness
- Management
- Urgent exploration if transection suspected
- Incidence
- 0.3-1%
- Presentation
- Thenar weakness post-operatively
- Management
- Exploration and repair if identified early
- Incidence
- Under 1%
- Presentation
- Hematoma, brisk bleeding
- Management
- Immediate control, vascular repair
- Incidence
- 1-5%
- Presentation
- Severe pain, stiffness, autonomic changes
- Management
- Multidisciplinary pain management, PT/OT
- Incidence
- Under 1%
- Presentation
- Wound erythema, drainage, fever
- Management
- Antibiotics, wound care, possible I&D
- Incidence
- Rare
- Presentation
- Weakness of grip, visible tendon prominence
- Management
- Rare, usually asymptomatic
Pillar Pain
Most common complication (10-20% of patients):
- Mechanism: Separation of thenar and hypothenar origins from transverse ligament
- Presentation: Aching pain at bases of thumb and hypothenar eminences
- Worse with grip and pinch
- Typically resolves by 3 months, some up to 6-12 months
- Management: Reassurance, grip strengthening, thenar massage
- Prevention: Partial ligament release NOT recommended (risk incomplete decompression)
Incomplete Release
Second most common cause of persistent symptoms:
- Failure to divide ligament completely distally or proximally
- Inadequate proximal release of antebrachial fascia
- Failure to identify anomalous anatomy
- Diagnosis: Repeat NCS, ultrasound showing residual compression
- Management: Revision open CTR with extended release
Nerve Injuries
- Rare (0.1-0.3%) but devastating
- Present immediately post-op with dense numbness and weakness
- Management: Urgent exploration and primary repair
- May need nerve graft if gap
- More common (0.3-1%), especially with transligamentous variant
- Present with thenar weakness
- Management: If identified within 72 hours, explore and repair
- Late recognition: conservative management, tendon transfers if needed
Complex Regional Pain Syndrome (CRPS)
Severe complication (1-5%):
- Disproportionate pain, stiffness, swelling
- Autonomic changes (temperature, color, sweating)
- Early recognition critical
- Management: Multidisciplinary (pain specialist, PT/OT, psychology)
- Gabapentin, vitamin C prophylaxis (some evidence)
- Sympathetic blocks if severe
Postoperative Care and Recovery
Postoperative Protocol
Protection phase:
- Bulky dressing with wrist in neutral
- Elevate hand above heart (prevent edema)
- Immediate finger ROM - flex and extend fingers hourly
- Keep dressing dry
- Ice for pain control
- Oral analgesia (paracetamol, NSAIDs)
Wound check and suture removal:
- Remove dressing at 1 week
- Remove sutures at 10-14 days
- Begin scar massage with moisturizer
- Light activities of daily living permitted
- Avoid heavy lifting (greater than 2kg)
- Grip strengthening exercises - squeeze soft ball
Return to function:
- Progressive grip strengthening
- Desensitization if scar tender
- Full finger ROM expected
- Return to desk work 1-2 weeks
- Return to manual labor 4-6 weeks (open) or 2-4 weeks (endoscopic)
- Driving when can control vehicle safely (typically 1-2 weeks)
Expected outcomes:
- Sensory recovery: Complete by 3-6 months
- Motor recovery: Depends on pre-op severity, may take 6-12 months
- Grip strength: Returns to baseline by 3-6 months
- Pillar pain: Should resolve by 3-6 months
- Scar maturation: 6-12 months
Hand Therapy
- Severe pre-operative stiffness
- Pillar pain persisting beyond 6 weeks
- CRPS symptoms
- Slow recovery of function
- Grip weakness
- Scar sensitivity
- Edema control (elevation, retrograde massage)
- Scar desensitization and massage
- Grip strengthening (progressive resistance)
- Pinch strengthening
- Tendon gliding exercises
- Return to work conditioning
Expected Recovery Timeline
- Timeline
- Immediate to weeks
- Notes
- Nocturnal symptoms resolve immediately
- Timeline
- Weeks to months
- Notes
- Depends on severity, mild = weeks
- Timeline
- Months
- Notes
- Incomplete if severe atrophy
- Timeline
- 3-6 months
- Notes
- Open slower than endoscopic initially
- Timeline
- 1-2 weeks
- Notes
- Variable by patient
- Timeline
- 4-6 weeks open, 2-4 weeks endo
- Notes
- Depends on demands
- Timeline
- 3-6 months
- Notes
- 85-95% satisfied
Outcomes and Prognosis
Success Rates
Overall surgical outcomes:
- Excellent/Good: 85-95% patient satisfaction
- Symptom relief: 90-95% for nocturnal paresthesia
- Sensory recovery: 80-90% complete if mild-moderate pre-op
- Motor recovery: Variable - depends on severity and duration
Prognostic Factors:
- Favorable Prognosis
- Less than 1 year
- Poor Prognosis
- Greater than 2 years
- Favorable Prognosis
- Mild to moderate (no atrophy)
- Poor Prognosis
- Severe with thenar wasting
- Favorable Prognosis
- Under 50 years
- Poor Prognosis
- Over 65 years
- Favorable Prognosis
- Sensory changes only
- Poor Prognosis
- Absent responses, denervation
- Favorable Prognosis
- No diabetes
- Poor Prognosis
- Diabetes present
- Favorable Prognosis
- Normal BMI
- Poor Prognosis
- BMI greater than 35
- Favorable Prognosis
- No WC claim
- Poor Prognosis
- Active WC claim
- Favorable Prognosis
- Unilateral
- Poor Prognosis
- Bilateral severe
Functional Outcomes
- Most widely used validated outcome measure
- Symptom Severity Scale (11 questions)
- Functional Status Scale (8 questions)
- Improvement of 1.0+ points clinically significant
- Symptom score improves from 3.2 to 1.5 (out of 5)
- Functional score improves from 2.8 to 1.4
- Maximal improvement at 3-6 months
- 85-90% would have surgery again
- 10-15% disappointed (persistent symptoms or complications)
- Higher satisfaction with appropriate patient selection
Recurrence
True recurrence (scar tissue causing recompression):
- Incidence: 5-10% over 10 years
- Risk factors: Diabetes, rheumatoid arthritis, dialysis
- Presentation: Gradual return of symptoms after initial relief
- Diagnosis: Repeat NCS, ultrasound showing recurrent compression
- Management: Revision CTR with neurolysis ± coverage (fat flap, vein wrap)
Persistent symptoms (inadequate release):
- More common than true recurrence
- Never had symptom-free interval post-op
- Due to incomplete ligament division
- Management: Revision CTR if confirmed on imaging
Guidelines, Registries & Global Practice
Carpal tunnel syndrome is the most common compression neuropathy worldwide and is managed in essentially every health system, but diagnostic pathways and thresholds for surgery differ by region and resource setting.
Global Epidemiology
According to PubMed, the best population-based estimate comes from Atroshi et al (JAMA 1999, DOI), a Swedish general-population survey of 2466 responders: clinically certain CTS prevalence was 3.8%, electrophysiologically confirmed median neuropathy 4.9%, and combined clinical-plus-electrophysiological CTS 2.7%. Hand paraesthesia symptoms were far more common (14.4%), so symptoms alone over-estimate disease.
- Prevalence: roughly 3-5% of the general adult population, with a consistent female predominance (about 3:1 in most series).
- Occupational burden: markedly higher in jobs with forceful, repetitive or vibratory hand use (e.g. food/meat processing, assembly, construction) - work-related attributable fractions are concentrated in a small number of high-risk jobs (Roquelaure et al, BMC Public Health 2018, DOI).
- Systemic associations: diabetes, obesity, hypothyroidism, pregnancy, rheumatoid arthritis and amyloid raise risk across all populations.
Major Guidelines, Side by Side
- Diagnosis
- Clinical diagnosis; electrodiagnostics recommended to confirm and grade, especially pre-operatively
- First-line
- Immobilisation (splint), steroid injection, oral steroid for mild-moderate
- Surgery / key stance
- Surgical release recommended over no surgery; routine internal neurolysis, flexor tenosynovectomy and epineurotomy NOT recommended (moderate-strong evidence)
- Diagnosis
- Largely clinical; nerve conduction studies if diagnosis uncertain or before surgery
- First-line
- Splinting and/or corticosteroid injection for mild-moderate symptoms
- Surgery / key stance
- Refer for decompression if severe, persistent, or with motor signs; open and endoscopic both accepted
- Diagnosis
- Clinical + electrodiagnostic confirmation; ultrasound as adjunct (nerve CSA)
- First-line
- Splint and injection; steroid injection has best short-term evidence
- Surgery / key stance
- Decompression for refractory or severe disease; technique by surgeon preference
- Diagnosis
- Predominantly clinical (NCS often unavailable)
- First-line
- Splinting and injection where available
- Surgery / key stance
- Open release under local anaesthetic / WALANT favoured (low cost, no NCS dependency)
Across guidelines the common threads are: (1) CTS is fundamentally a clinical diagnosis; (2) electrodiagnostic testing confirms the diagnosis, grades severity and predicts outcome but is not mandatory in classic cases; (3) splinting and a single corticosteroid injection are reasonable first-line measures for mild-moderate disease; and (4) surgical decompression is the definitive treatment, indicated urgently when there is thenar wasting or motor loss. The main genuine divergence is how readily electrodiagnostics are required before surgery (more emphasised in North America and for medico-legal/occupational cases) versus a more clinically driven pathway elsewhere.
Registry and Large-cohort Evidence
CTS is not an implant procedure, so it is not captured by the arthroplasty joint registries (NJR, AJRR, AOANJRR, SHAR). The closest "registry-scale" evidence comes from large national audit and administrative cohorts. According to PubMed, Bland (Muscle Nerve 2001, DOI) analysed 1268 decompressions and reported a 69% self-reported success rate, with pre-operative nerve-conduction grade the strongest outcome predictor - very severe (axonal) and entirely normal studies both did worse than mid-grade abnormality.
Global Practice Variation
- Anaesthesia: wide-awake local anaesthetic no-tourniquet (WALANT) and field-block open release are increasingly standard worldwide and are particularly valuable where theatre and anaesthetic resources are limited.
- Technique: endoscopic release is more common in well-resourced centres for faster return to work, but Cochrane evidence (Scholten 2007) shows no long-term advantage over open release.
- Imaging: high-resolution ultrasound (median nerve cross-sectional area) is used as a first-line confirmatory test in some European and Asian centres, reducing reliance on nerve conduction studies.
Medico-Legal and Consent Considerations (universal)
Informed consent should cover the natural history, conservative options and their success rates, and surgical risks: median or recurrent motor branch injury (0.1-0.5%), pillar pain (10-20%), incomplete relief (especially when thenar atrophy is already present), complex regional pain syndrome (rare), and the recovery/return-to-work timeline. Documentation of severity grading, thenar assessment, electrodiagnostic results and the duration of conservative treatment is good practice in any jurisdiction. The recurring litigation themes are nerve transection, incomplete release with persistent symptoms, and delayed diagnosis leading to irreversible thenar wasting.
MCQ Practice Points
Q: How many structures pass through the carpal tunnel?
A: 10 structures - Nine flexor tendons (4 FDS, 4 FDP, 1 FPL) plus the median nerve. The median nerve is the most superficial and radial structure. Note that the ulnar nerve and artery pass through Guyon's canal, NOT the carpal tunnel.
Q: Why is palmar sensation preserved in carpal tunnel syndrome?
A: The palmar cutaneous branch of the median nerve branches 5-6cm proximal to the wrist crease and passes superficial to the transverse carpal ligament. Therefore it is not compressed in the tunnel. This is a key feature that distinguishes CTS from more proximal median nerve lesions or C6 radiculopathy.
Q: Which muscles are supplied by the recurrent motor branch of the median nerve?
A: LOAF - Lumbricals 1 and 2, Opponens pollicis, Abductor pollicis brevis, Flexor pollicis brevis (superficial head only). The deep head of FPB is supplied by the ulnar nerve. Adductor pollicis is also ulnar nerve.
Q: Which clinical test has the highest sensitivity for diagnosing CTS?
A: Durkan's compression test (87% sensitivity, 90% specificity) - direct compression over the carpal tunnel for 30 seconds. This is more sensitive than Phalen's test (68% sensitivity) or Tinel's sign (50% sensitivity). However, Phalen's is more commonly asked about in exams.
Q: What are the nerve conduction criteria for diagnosing CTS?
A: Prolonged distal motor latency greater than 4.5ms (wrist to APB) and/or prolonged sensory latency greater than 3.5ms (wrist to digit). May also see reduced amplitudes if severe. Always compare to ulnar nerve as internal control. Median-ulnar sensory latency difference greater than 0.5ms is significant.
Q: What is the most common anatomical variant of the recurrent motor branch?
A: Extraligamentous (50%) - the motor branch exits the median nerve distal to the transverse carpal ligament. This is the safest variant during surgery. Subligamentous (30%) travels under the ligament before exiting. Transligamentous (20%) pierces through the ligament and is at risk during endoscopic release.
Q: What is the most common complication after carpal tunnel release?
A: Pillar pain (10-20% incidence) - aching pain at the thenar and hypothenar eminences due to separation of muscle origins from the divided ligament. Typically resolves spontaneously by 3-6 months. Managed with reassurance and hand therapy.
Q: How should you manage carpal tunnel syndrome in pregnancy?
A: Conservative management - night splinting in neutral position is first-line. Symptoms usually resolve post-partum (2-4 weeks after delivery). Corticosteroid injection is safe if splinting fails. Avoid surgery during pregnancy unless severe progressive motor loss. Most cases resolve without intervention.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 52-year-old woman presents with 8 months of waking at night with numbness in her right hand. She shakes her hand for relief. Her symptoms are worse after driving. Examination shows normal thenar bulk, positive Phalen's test. How would you manage this patient?”
“A 65-year-old diabetic man presents with constant numbness and difficulty buttoning his shirt. On examination, there is obvious thenar muscle wasting and weakness of thumb abduction. What is your management?”
“A 45-year-old woman returns 6 months after open carpal tunnel release with persistent symptoms identical to pre-operative. Her nerve conduction studies showed severe CTS pre-operatively. What is your approach?”
Key Anatomy
- Tunnel contents: 9 tendons (4 FDS + 4 FDP + FPL) + median nerve = 10 total
- Floor = carpal bones; Roof = transverse carpal ligament (2.5-3cm long)
- Median nerve most superficial and radial (at risk)
- Palmar cutaneous branch: 5cm proximal, travels superficial (SPARED)
- Recurrent motor branch: Extraligamentous 50%, subligamentous 30%, transligamentous 20%
- LOAF muscles: Lumbricals 1-2, Opponens, APB, FPB superficial head
Clinical Diagnosis
- Classic triad: Nocturnal paresthesia + flick sign + median distribution
- Distribution: Thumb, index, middle, radial half ring (palmar ONLY)
- Thenar atrophy = SEVERE (APB wasting, urgent surgery needed)
- Provocative tests: Durkan's 87% sens (best), Phalen's 68% sens, Tinel's 50% sens
- Differential: C6 radiculopathy (palmar sensation affected), pronator syndrome, TOS
Investigations
- NCS gold standard: Motor latency greater than 4.5ms, sensory greater than 3.5ms
- EMG: Denervation in APB if severe (fibrillations, positive sharp waves)
- Ultrasound: Nerve CSA greater than 10mm² at inlet, can identify masses
- MRI not routine (only if mass or atypical)
- Screen: TSH (hypothyroid), HbA1c (diabetes), RF (RA)
Management Algorithm
- Mild-moderate WITHOUT atrophy: Splint neutral position 6-8 weeks first
- Injection: 70-80% short-term relief, 20-30% long-term, limit 2-3 max
- Severe OR thenar atrophy: Urgent CTR (do NOT delay)
- Surgery success: 85-95% excellent outcomes
- Open vs endoscopic: Similar long-term, endoscopic faster recovery
Surgical Technique (Open CTR)
- Incision: Longitudinal in line with ring finger, ulnar to thenar crease, 3-4cm
- Protect palmar cutaneous branch (superficial), recurrent motor branch (variable)
- Divide TCL completely: Distal to superficial arch, proximal into forearm 2cm
- Do NOT repair ligament (recreates compression)
- Do NOT perform neurolysis (increases scar, worse outcomes)
Complications
- Pillar pain: 10-20%, thenar/hypothenar ache, resolves 3-6 months
- Incomplete release: 2-5%, most common cause persistent symptoms
- Median nerve injury: 0.1-0.5%, urgent exploration if suspected
- Recurrent motor branch injury: 0.3-1%, thenar weakness
- CRPS: 1-5%, severe pain/stiffness, multidisciplinary management
Exam Favorites
- Why palmar sensation spared? Palmar cutaneous branch proximal to tunnel
- Most sensitive test? Durkan's compression (87% sens, 90% spec)
- Thenar atrophy management? Urgent surgery, counsel incomplete motor recovery
- Most common complication? Pillar pain 10-20%, resolves 3-6 months
- NCS criteria? Motor greater than 4.5ms, sensory greater than 3.5ms
- Pregnancy CTS? Splinting first-line, usually resolves post-partum
Evidence Base
According to PubMed, the citations below have been verified against the primary record (title, journal, year and reported findings).
- Open carpal tunnel release vs night wrist splinting for idiopathic CTS
- General-improvement success at 3 months: 80% surgery vs 54% splinting (difference 26%, 95% CI 12-40%)
- Success at 18 months: 90% surgery vs 75% splinting (difference 15%, 95% CI 3-27%)
- By 18 months, 41% of the splint group had crossed over to surgery
- 33 RCTs of surgical techniques for CTS reviewed
- No alternative technique gave significantly better symptom relief than standard open release
- Endoscopic release allowed earlier return to work/activities (weighted mean difference about 6 days, 95% CI 3-9)
- Choice between open and endoscopic is guided by surgeon and patient preference
- 12 randomised/quasi-randomised studies, 671 participants
- Local steroid injection improved symptoms at 1 month vs placebo (RR 2.58, 95% CI 1.72-3.87)
- Significant symptom relief beyond 1 month vs placebo was not demonstrated
- Two injections gave no significant added benefit over a single injection
- Methylprednisolone 80 mg vs 40 mg vs saline placebo, all 111 patients followed to 5 years
- No significant difference in symptom severity score between steroid and placebo at 5 years
- Subsequent surgery rate: 84% (80 mg), 92% (40 mg) and 97% (placebo)
- Steroid significantly delayed and modestly reduced eventual surgery (log-rank P=.002 for 80 mg vs placebo)
- Population-based study of 2466 responders in southern Sweden
- Clinically certain CTS prevalence 3.8% (95% CI 3.1-4.6%)
- Electrophysiologically confirmed median neuropathy 4.9% (95% CI 4.1-5.8%)
- Clinically AND electrophysiologically confirmed CTS 2.7% (95% CI 2.1-3.4%)
- 600 clinically symptomatic hands graded purely on median nerve electrodiagnostics
- Six classes: negative, minimal, mild, moderate, severe, extreme
- Distribution: extreme 3%, severe 14%, moderate 36%, mild 24%, minimal 21%, negative 3%
- Advanced (severe/extreme) classes concentrated in older patients; milder classes in younger women
- 1268 carpal tunnel decompressions assessed by postal questionnaire
- Overall self-reported surgical success rate 69%
- Greater age, lower symptom scores, longer duration and male sex predicted poorer outcome
- Middle-grade NCS abnormality had better outcomes than either very severe or normal studies