Microbiology and Surgical Management
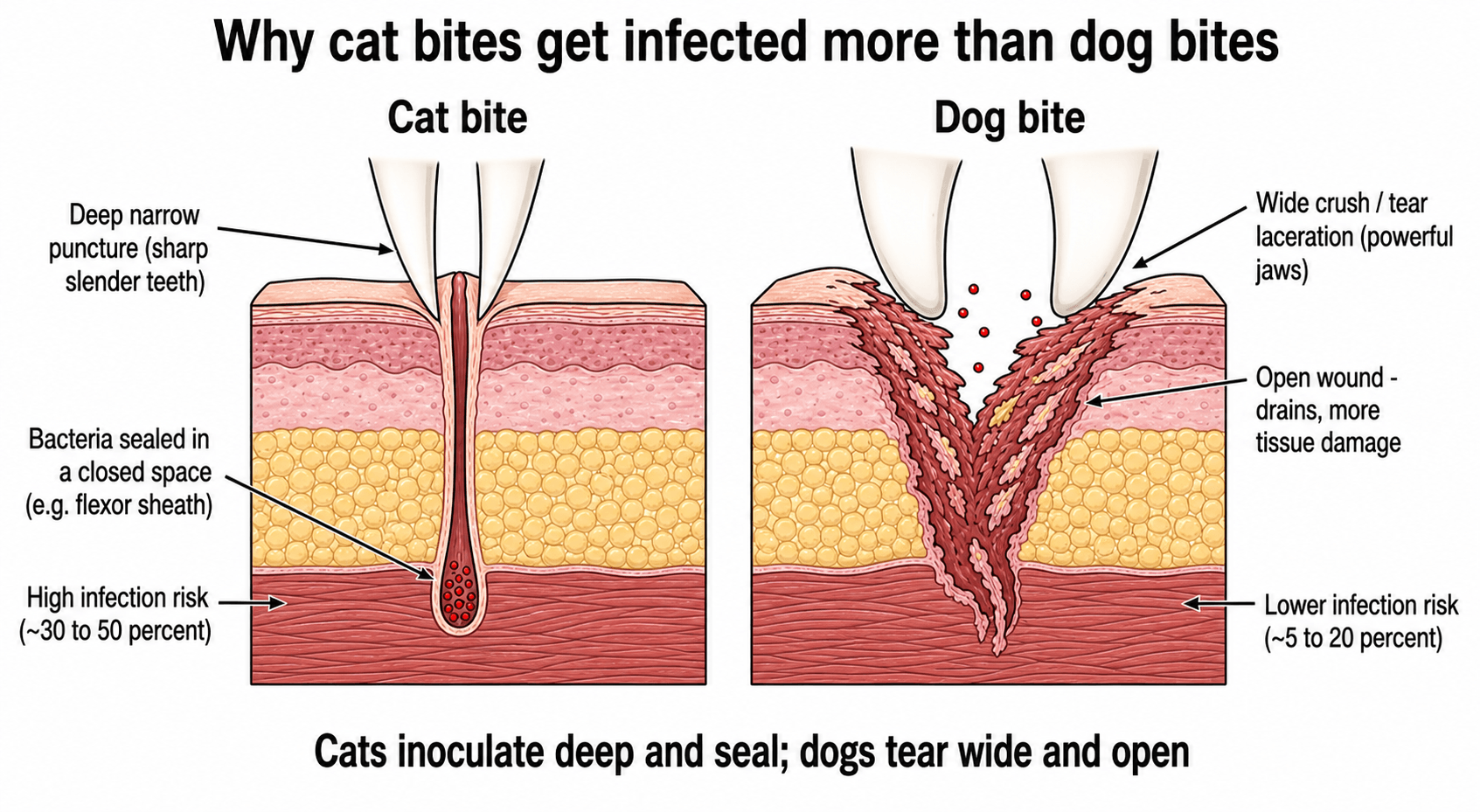
- Cats bite deep (Puncture) → Pasteurella multocida → Rapid infection (less than 24h).
- Dogs bite wide (Crush/Tear) → Polymicrobial → Slower infection (greater than 24h).
- Primary closure is CONTROVERSIAL but accepted for face (excellent blood supply) and large lacerations (loosely).
- Puncture wounds should NEVER be closed primarily.
- Augmentin (Amoxicillin/Clavulanate) is the antibiotic of choice.
- “Capnocytophaga canimorsus causes overwhelming sepsis in asplenic/immunocompromised patients.
- “Bats can carry rabies-related lyssaviruses worldwide. Treat any bat exposure as a potential rabies exposure.
- “Eikenella corrodens is HUMAN bite, not animal.
A cat-bite puncture over the volar finger that is red and painful on passive extension is flexor tenosynovitis until proven otherwise - it needs urgent washout, not oral antibiotics and discharge. Never close a puncture or a hand bite primarily, and never rely on cephalexin monotherapy (poor Pasteurella cover).
Overview & Epidemiology
Animal bites are common, potentially limb-threatening injuries that combine mechanical tissue damage with bacterial inoculation. They account for up to 1% of emergency presentations worldwide, with dogs responsible for the large majority and cats for a smaller but disproportionately infective share. School-age children are bitten most often, frequently by a familiar animal.
- Dogs (around 80-90%): Powerful jaws produce crush, tear and avulsion injuries; deep structural damage and paediatric facial fractures are possible, but infection rates are comparatively low.
- Cats (around 5-15%): Fine sharp teeth inoculate bacteria deep into closed spaces; despite small entry wounds, infection rates reach 30-50%.
- High-risk hosts: Asplenic, cirrhotic, diabetic and immunocompromised patients face disproportionately severe infections regardless of wound size.
Pathophysiology & Microbiology
Bite infections are driven by the oral flora of the biting animal inoculated directly into tissue. Infected wounds are typically polymicrobial, with a median of around 5 organisms per culture (Talan, NEJM 1999).
- Pasteurella species are the hallmark: P. canis predominates in dogs and P. multocida in cats. Pasteurella produces a characteristically rapid (often under 24 hours) cellulitis with intense pain and serosanguinous discharge.
- Aerobic co-pathogens: streptococci, staphylococci, Moraxella, Neisseria.
- Anaerobes: Fusobacterium, Bacteroides, Porphyromonas, Prevotella - common in deep wounds.
- Capnocytophaga canimorsus: a fastidious Gram-negative rod from dog/cat saliva that causes fulminant sepsis (DIC, shock, purpura) in asplenic and immunocompromised hosts, with around 30% mortality.
- Mechanical factor: cat punctures seal bacteria within closed tissue planes (flexor sheath, joint), converting a tiny wound into a deep-space infection.
Beyond Pasteurella, Capnocytophaga and Eikenella, examiners like the organism-to-animal matches for less common but classic exposures:
- Cat-scratch disease - Bartonella henselae: after a cat scratch or bite; regional tender lymphadenopathy days to weeks later, usually self-limiting (azithromycin if treatment is needed).
- Rat-bite fever - Streptobacillus moniliformis (or Spirillum minus in Asia): fever, rash and migratory arthralgia after a rat bite; treated with penicillin.
- Monkey / macaque bite - Herpes B virus (Cercopithecine herpesvirus 1): rare but can cause fatal encephalomyelitis; needs urgent wound care and antiviral prophylaxis (valaciclovir or aciclovir).
- Seal finger ("spekfinger") - Mycoplasma species: a painful, indolent finger infection after a seal bite that responds to tetracyclines, not to standard beta-lactams.
The teaching point: take an exposure history (which animal, and where in the world) - it changes both the organism you must cover and the prophylaxis you give.
Classification of Bite Injuries
- Puncture: Deep, narrow inoculation (typical of cats). Highest infection risk; never closed primarily.
- Laceration: Tearing wound (typical of dogs). Lower infection rate but greater tissue loss.
- Crush / devitalisation: Large-dog jaw force; non-viable tissue and even compartment syndrome risk.
- Avulsion: Soft-tissue loss that may require reconstruction or flap coverage.
Clinical Presentation & Assessment
- History: Animal type and provocation, time since injury, tetanus and rabies risk (region, vaccination), and host factors (asplenia, immunosuppression, diabetes, cirrhosis).
- Inspection: Wound type and depth, devitalised tissue, contamination, proximity to joints/tendons.
- Neurovascular and tendon exam: Document distal sensation, perfusion and active tendon function before and after exploration.
- Signs of established infection: Spreading erythema, lymphangitis, abscess, fever; in the digit look for the four Kanavel signs of flexor tenosynovitis (fusiform swelling, semi-flexed posture, tenderness along the sheath, pain on passive extension).


Investigations & Imaging
- Plain radiographs: Assess for fracture, air in a joint (penetration), and radiopaque foreign bodies such as tooth fragments. A normal film does not exclude joint penetration, cartilage injury or a radiolucent foreign body.
- Bloods: FBC and inflammatory markers (CRP) when infection is suspected or systemic features are present.
- Microbiology: Send deep tissue or pus for aerobic and anaerobic culture; warn the laboratory of the bite history so fastidious organisms (Pasteurella, Capnocytophaga) are sought and cultures held longer.
- Advanced imaging: Ultrasound or CT may help locate occult or radiolucent foreign bodies in persistently infected wounds.
Imaging Atlas
Dog vs Cat vs Human Bite: Differentiating Features
- Dog Bite
- Crush and tear (powerful jaws)
- Cat Bite
- Deep puncture (sharp slender teeth)
- Human Bite
- Laceration / occlusal or clenched-fist
- Dog Bite
- Lower (around 5-20%)
- Cat Bite
- Higher (around 30-50%)
- Human Bite
- High, especially over MCP joint
- Dog Bite
- P. canis (Pasteurella in ~50%)
- Cat Bite
- P. multocida (Pasteurella in ~75%)
- Human Bite
- Less Pasteurella; Eikenella corrodens
- Dog Bite
- Capnocytophaga canimorsus (asplenic sepsis)
- Cat Bite
- Pasteurella multocida (rapid cellulitis)
- Human Bite
- Eikenella corrodens, oral anaerobes
- Dog Bite
- Crush, devitalised tissue, fractures in children
- Cat Bite
- Tenosynovitis and septic arthritis from sealed punctures
- Human Bite
- Fight-bite joint penetration, viral transmission (HBV/HCV/HIV)
- Dog Bite
- Selected lacerations/face can be closed early
- Cat Bite
- Never close punctures
- Human Bite
- Never close hand bites; leave open
A wound over the dorsal MCP joint described as a "dog bite" must always raise suspicion of a fight-bite (clenched-fist human bite), which the patient may conceal. Both demand exploration for joint penetration, but the human bite carries Eikenella corrodens and bloodborne-virus risk.
Management Algorithm
- Wash and irrigate: Immediate copious low-pressure normal saline irrigation - the single most effective step to reduce both bacterial and rabies risk.
- Debride: Excise devitalised and contaminated tissue; remove foreign bodies (tooth fragments).
- Assess and document: Neurovascular and tendon status, joint penetration, photograph wounds.
- Prophylaxis: Tetanus per status; rabies post-exposure prophylaxis per regional risk and WHO category.
- Antibiotics: Amoxicillin-clavulanate for high-risk wounds and hosts (see Antibiotic Guidelines).
Surgical Technique: Drainage of Hand-Space Infection
- Indication: Pyogenic flexor tenosynovitis (Kanavel signs) - a surgical emergency.
- Approach: Brunner or mid-lateral incision; open the sheath distally near A5 and proximally near A1.
- Irrigation: Pass a fine catheter through the sheath and irrigate with copious saline until effluent is clear; consider leaving an irrigation catheter.
- Aftercare: Elevation, IV antibiotics, early hand-therapy review to balance infection control against stiffness.
Complications
- Septic Arthritis: From direct inoculation. Destroys cartilage rapidly (chondrolysis). requiring serial washouts.
- Osteomyelitis: If bone is bitten.
- Tenosynovitis: Pyogenic flexor tenosynovitis requires urgent drainage.
- Rabies: Almost universally fatal once symptomatic. Globally over 99% of human rabies is dog-transmitted; bat lyssaviruses (for example Australian and European Bat Lyssavirus) require the same post-exposure protocol.
- Post-Traumatic Stress Disorder (PTSD): Common after dog attacks.
Rehabilitation
Acute Phase (Days 1-7)
- Splinting: Position of safety (Intrinsic plus) for hand bites to prevent contracture
- MCP joints flexed 70-90°
- IP joints extended
- Wrist in neutral to slight extension
- Edema Control: Elevation above heart level is critical
- Compressive dressing (non-circumferential)
- Active finger pumping exercises when permitted
- Wound Care: Daily dressing changes to monitor for spreading infection
Subacute Phase (Weeks 1-4)
- Mobilization: Early controlled mobilization once infection cleared
- Active range of motion within splint
- Passive range if tendon repair performed (modified Duran protocol)
- Scar Management: Silicone sheets, massage once epithelialized
- Strengthening: Gradual isometric then isotonic exercises
Late Phase (Weeks 4-12)
- Return to Function: Occupation-specific rehabilitation
- Desensitization: For painful scars or hypersensitivity
- Contracture Prevention: Night splinting if MCP or PIP stiffness developing
In animal bites with tendon injury, the balance between infection control (immobilization) and adhesion prevention (early motion) is critical. Generally, err on the side of infection control first - a stiff finger is better than an amputated one.
Prognosis
- Infection Rate: With proper debridement and antibiotics, infection rate is low (less than 5% for dogs).
- Function: Depends on structural injury. Nerve repairs in dirty wounds have poorer outcomes.
- Cosmesis: Scar revision may be needed later.
Antibiotic Guidelines
Augmentin (Amoxicillin + Clavulanate). It covers Pasteurella, Staph, Strep, and Anaerobes. Allergy (Penicillin): Doxycycline (or TMP/SMX) + Metronidazole (for anaerobes). Alternate: Moxifloxacin (monotherapy, covers all). Avoid: Cephalexin (Keflex) alone - it does NOT cover Pasteurella effectively.
- Prophylaxis: Indicated for all cat bites, deep dog bites, hand bites, and immunocompromised hosts. Duration: 3-5 days.
- Treatment: Indicated for established infection. Duration: 7-14 days. IV if systemic signs.
Guidelines, Registries & Global Practice
Global Epidemiology
- Burden: Mammalian bites account for up to 1% of all emergency department visits worldwide (per the Cochrane review of mammalian-bite prophylaxis).
- Species mix: Dogs cause roughly 80-90% of bites globally; cats 5-15%; humans and other species the remainder. School-age children make up nearly half of those bitten.
- Infection risk: Dog-bite lacerations have lower infection rates (commonly cited 5-20%) than cat-bite punctures (30-50%), reflecting deep inoculation in a closed space rather than wide tearing.
- Rabies: WHO estimates roughly 59,000 human rabies deaths per year, over 95% in Asia and Africa and over 99% transmitted by dogs - in stark contrast to rabies-free regions where the chief concern is wound infection.
Side-by-Side Guideline Comparison
- IDSA (US, 2014)
- Amoxicillin-clavulanate
- NICE / BOA (UK)
- Co-amoxiclav
- AO / WHO (global)
- Amoxicillin-clavulanate
- IDSA (US, 2014)
- Doxycycline or fluoroquinolone plus anaerobic cover
- NICE / BOA (UK)
- Doxycycline plus metronidazole
- AO / WHO (global)
- Macrolide/doxycycline plus metronidazole
- IDSA (US, 2014)
- High-risk wounds and hosts (hand, face, deep puncture, immunocompromised)
- NICE / BOA (UK)
- Cat bites, human bites, hand/face/foot, puncture, immunocompromised
- AO / WHO (global)
- Risk-stratified by wound and host
- IDSA (US, 2014)
- Avoid except selected facial wounds
- NICE / BOA (UK)
- Avoid in hand/puncture; cosmetic closure of face acceptable
- AO / WHO (global)
- Avoid in high-risk wounds; delayed closure preferred
- IDSA (US, 2014)
- Per regional risk assessment
- NICE / BOA (UK)
- Per UK rabies risk algorithm (travel exposure)
- AO / WHO (global)
- WHO category-based PEP (wash, vaccine, +/- immunoglobulin)
Registry and Surveillance Notes
- Animal bites are notifiable in many jurisdictions chiefly for rabies surveillance, not for orthopaedic outcomes; there is no dedicated international bite-injury implant registry.
- Rabies-endemic regions rely on WHO and national surveillance to guide post-exposure prophylaxis supply, whereas rabies-free regions (parts of Oceania, Western Europe, the UK) focus reporting on dangerous-animal legislation.
Rabies and Bat Lyssavirus
- Rabies-free vs endemic regions: In rabies-free countries the dominant risk from a domestic dog or cat bite is bacterial infection, not rabies; in endemic regions every unprovoked bite should trigger a WHO category-based PEP assessment.
- Lyssaviruses in bats: Several regions harbour rabies-related lyssaviruses in bats (for example Australian Bat Lyssavirus, European Bat Lyssavirus). Any bat bite, scratch or mucous-membrane exposure should be managed as a potential rabies exposure regardless of the local terrestrial-rabies status.
- PEP principles (WHO): Immediate copious wound washing, rabies vaccine series, and rabies immunoglobulin infiltrated at the wound for category III exposures or immunocompromised hosts. Symptomatic rabies is almost universally fatal.
The "category-based PEP" the rabies guidance refers to is the WHO three-tier exposure scheme - examiners expect you to define it:
- Category I - touching or feeding an animal, or licks on intact skin: no exposure, no PEP (wash if in doubt).
- Category II - nibbling of uncovered skin, or minor scratches or abrasions without bleeding: wound washing plus rabies vaccine.
- Category III - single or multiple transdermal bites or scratches, licks on broken skin, mucous-membrane contamination with saliva, or any direct bat contact: wound washing plus vaccine plus rabies immunoglobulin (infiltrated into and around the wound).
Immunocompromised hosts and all bat exposures are treated as Category III. Immediate wound washing with soap and water is the first step in every category.
Tetanus Prophylaxis (Global Principle)
- Clean Minor Wound
- No prophylaxis
- Tetanus-Prone Wound
- No prophylaxis
- Clean Minor Wound
- No prophylaxis
- Tetanus-Prone Wound
- Tetanus toxoid booster
- Clean Minor Wound
- Tetanus toxoid booster
- Tetanus-Prone Wound
- Booster plus tetanus immunoglobulin
- Clean Minor Wound
- Booster
- Tetanus-Prone Wound
- Booster plus tetanus immunoglobulin
High- vs Limited-Resource Practice Variation
- High-resource settings: Ready access to co-amoxiclav, theatre time for washout, microbiology with anaerobic culture, and reliable rabies vaccine/immunoglobulin stocks.
- Limited-resource settings: Rabies-endemic with potential vaccine/immunoglobulin shortages; the WHO emphasises immediate, thorough wound washing with soap and water as the single most cost-effective intervention to reduce rabies and bacterial infection where definitive prophylaxis is constrained.
Controversies & Areas of Uncertainty
- Primary closure of dog bites: Historically all bites were left open. Modern RCT evidence (Paschos, Injury 2013) shows that thoroughly irrigated, early-presenting, non-puncture dog-bite lacerations - especially of the face - can be closed primarily with better cosmesis and no excess infection. The hand and puncture wounds remain off-limits to primary closure.
- Routine antibiotic prophylaxis for low-risk dog bites: The Cochrane review found no proven benefit of prophylaxis for general cat or dog bites, only for hand bites and human bites. Practice nonetheless leans toward prophylaxis in many high-risk wounds and hosts because the consequences of hand-space infection are severe; this gap between trial evidence and pragmatic practice is a legitimate viva discussion point.
- Cephalosporin monotherapy: First-generation cephalosporins (cephalexin) have unreliable activity against Pasteurella multocida and are inadequate as sole therapy; this is a recurring exam trap and a real-world prescribing error.
- Irrigation pressure and additives: Extrapolating from the FLOW trial, high-pressure pulsatile lavage offers no benefit over low-pressure saline and soap additives may be harmful; copious low-pressure normal saline is preferred.
- Foreign-body imaging: Radiolucent tooth fragments and small radiolucent debris are easily missed on plain films; the role of ultrasound or CT for occult foreign bodies in persistently infected bites is evolving.
Memory Aids
CATS bite deep
Hook:A cat's small puncture hides a deep, sealed, high-risk infection.
DOG wounds
Hook:Dogs tear wide and crush; the hidden danger is Capnocytophaga in the asplenic patient.
BITE workup
Hook:Every bite needs Bug-and-host, Irrigation, Tetanus/rabies, and Exploration.
MCQ Practice Points
Q: Which organism is found in 50% of dog bites and 75% of cat bites? A: Pasteurella multocida.
Q: Why is Cephalexin monotherapy inadequate for animal bites? A: It has poor activity against Pasteurella multocida.
Q: Which organism causes fulminant sepsis in asplenic patients after a dog bite? A: Capnocytophaga canimorsus.
Q: A bite to the thenar eminence most risks which nerve? A: Recurrent motor branch of the Median Nerve.
Q: Which anatomical location allows primary closure of animal bites due to excellent blood supply? A: The Face. Primary closure (loose sutures) is accepted for facial bites due to cosmesis and rich vascular supply.
Q: What is the first-line antibiotic for animal bite prophylaxis? A: Amoxicillin-Clavulanate (Augmentin). Covers Pasteurella, Staph, Strep, and anaerobes. Avoid Cephalexin alone.
At a Glance: Quick Decision Table
- Answer
- Dog (around 80-90% of bites)
- Answer
- Cat bites (deep punctures, around 30-50%)
- Answer
- Pasteurella multocida (rapid cellulitis)
- Answer
- Amoxicillin-clavulanate (co-amoxiclav)
- Answer
- Cephalexin (poor Pasteurella cover)
- Answer
- Selected early facial lacerations
- Answer
- Punctures and hand bites
- Answer
- Capnocytophaga in asplenic host
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 45-year-old lady presents with a small puncture wound to the volar index finger from her cat 12 hours ago. It is red, swollen, and painful on passive extension. How do you manage this?”
“A 6-year-old child was bitten on the cheek by the family dog. There is a 3cm laceration, full thickness. Parents are worried about scarring. Can you close it?”
“A 30-year-old man presents 3 days after a dog bite over the dorsum of the middle-finger MCP joint. He has a swollen, erythematous knuckle and pain on movement. The plain radiograph appears normal. What is your concern and how do you proceed?”
“A 58-year-old man who had a splenectomy after trauma sustains a superficial dog scratch and minor bite to the forearm. The wound looks trivial. He asks whether he needs anything. What is your approach?”
Diagnosis
- History: Animal type, Time, Host factors
- Exam: Neurovascular status, Tendon function
- Signs: Kanavel signs (Tenosynovitis)
- X-ray: Foreign body (Tooth), Fracture, Air in joint
Management
- Irrigation: Copious saline
- Debridement: Aggressive
- Antibiotics: Augmentin (Golden Standard)
- Prophylaxis: Tetanus +/- Rabies (Bats)
Surgical Decisions
- Face: Primary Closure
- Hand/Foot: Leave Open / Loose
- Puncture: Never Close
- Established Infection: Washout
Evidence Base
Primary Closure vs Non-Closure of Dog Bites (RCT)
- RCT of 168 patients: 82 sutured vs 86 left open, all with high-pressure irrigation, povidone-iodine, and antibiotics
- Overall infection rate 8.3%, with no significant difference between primary suturing and non-closure
- Primary closure gave significantly better cosmesis (Vancouver Scar Scale 1.74 vs 3.05, p=0.0001)
- Wounds treated within 8 hours had 4.5% infection vs 22.2% when treated later; head/neck wounds fared best
Antibiotic Prophylaxis for Mammalian Bites (Cochrane)
- Systematic review of 8 RCTs of prophylactic antibiotics versus placebo or no intervention
- Significant reduction in infection after hand bites (OR 0.10, 95% CI 0.01-0.86; NNT 4)
- Significant reduction after human bites in one trial
- No demonstrated benefit of routine prophylaxis for general cat or dog bites; wound type (puncture vs laceration) did not change the effect