AIN Palsy | FPL/FDP Index/PQ Weakness | No OK Sign | Median Nerve Branch
- AIN is pure motor branch of median nerve, no sensory fibres
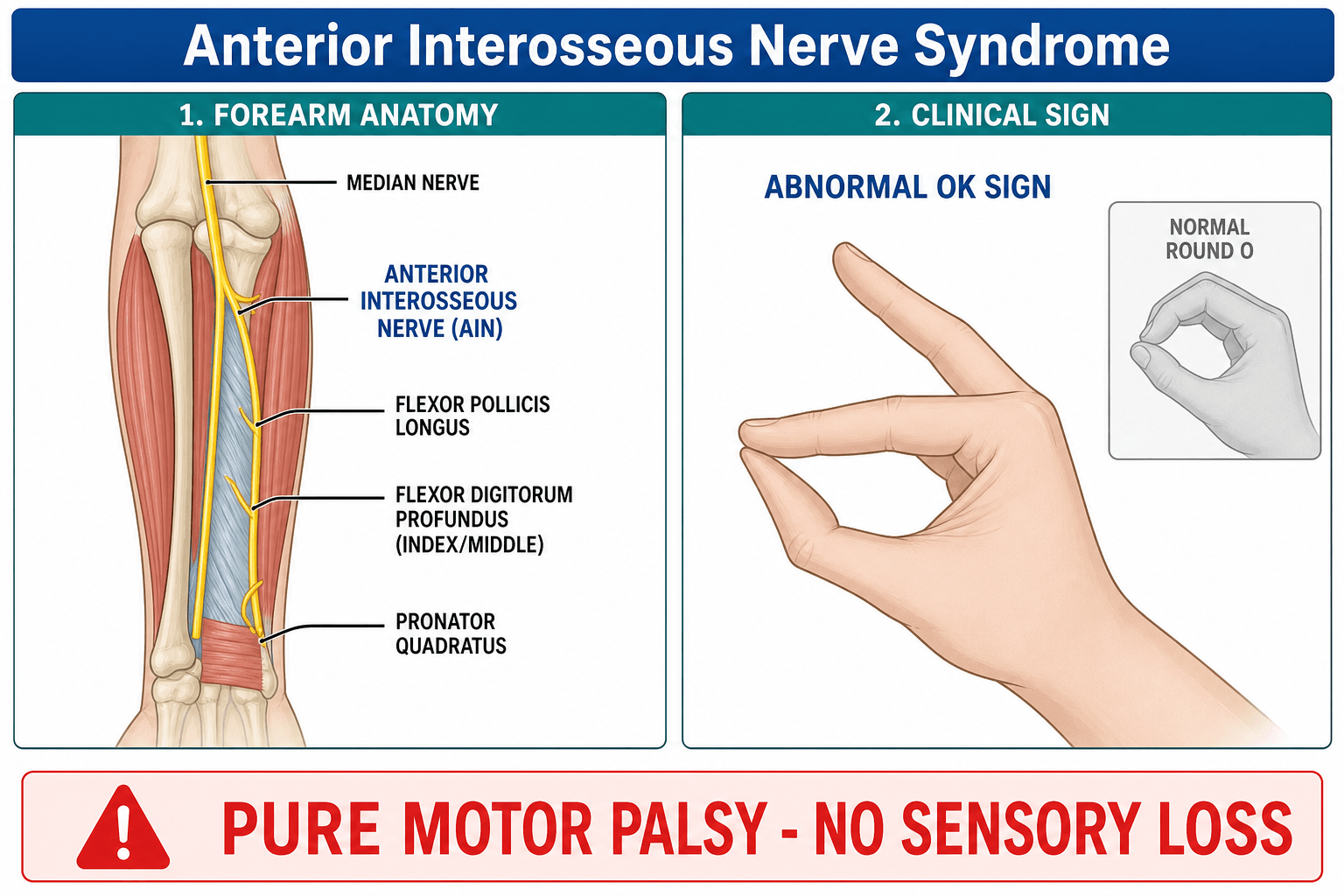
- Classic sign: inability to make OK sign due to weak FPL and FDP index
- Pronator quadratus weakness tested by resisted pronation with elbow flexed
- Most cases are neuritis (observation first), surgery for compression or no recovery
- Differentiate from Parsonage-Turner by absence of pain and other nerve involvement
- “AIN palsy = weak pinch, normal sensation in median distribution
- “OK sign tests both FPL (IP thumb) and FDP index (DIP index)
- “Parsonage-Turner often has preceding severe shoulder pain
- “Surgical decompression considered after 3-6 months without recovery
FPL: Test thumb IP flexion against resistance. Weakness = positive. FDP index: Test index DIP flexion. Compare to middle finger. PQ: Resisted pronation with elbow flexed to 90 degrees (isolates PQ from PT).
Abnormal OK sign: Patient cannot flex thumb IP and index DIP simultaneously to form circle. Pinch appears flat or key pinch instead of tip-to-tip.
No sensory loss: AIN carries no cutaneous sensory fibres. Any sensory deficit in median distribution suggests more proximal median neuropathy or separate pathology.
Parsonage-Turner: Preceding severe pain, often multiple nerves, self-limiting. AIN compression: Insidious or post-traumatic, isolated to AIN distribution.
- Diagnosis
- AIN palsy confirmed on motor testing
- Treatment
- Observe 3-6 months, serial exam
- Key Pearl
- Most neuritis cases recover spontaneously
- Diagnosis
- AIN + other nerves involved
- Treatment
- Neurophysiology, observe longer
- Key Pearl
- Parsonage-Turner likely, surgery rarely needed
- Diagnosis
- No recovery after 6 months
- Treatment
- Surgical exploration and decompression
- Key Pearl
- Address ligament of Struthers or PT fascia
FPPAIN Motor Innervation
Hook:FPP = the three muscles that fail in AIN palsy!
OKAYOK Sign Testing
Hook:OKAY sign fails when AIN is the culprit!
PAINAIN vs Parsonage-Turner
Hook:PAIN helps separate neuritis from entrapment!
Overview and Epidemiology
Anterior interosseous nerve syndrome produces a pure motor deficit affecting key pinch function. Because there is no sensory loss, the diagnosis is frequently missed or delayed. Accurate recognition prevents unnecessary median nerve explorations at the wrist and directs appropriate observation versus surgical timing.
- Origin: Branch of median nerve 5-8 cm distal to lateral epicondyle
- Course: Passes between heads of pronator teres, under flexor digitorum superficialis arch
- Termination: Innervates FPL, radial half FDP, PQ
- No sensory component: Pure motor, explains absence of numbness
- Pinch weakness: Critical for fine motor and occupational tasks
- No sensory loss: Distinguishes from carpal tunnel or pronator syndrome
- Self-limiting: Majority resolve with observation alone
- Surgical timing: Balance spontaneous recovery against denervation atrophy
Pathophysiology

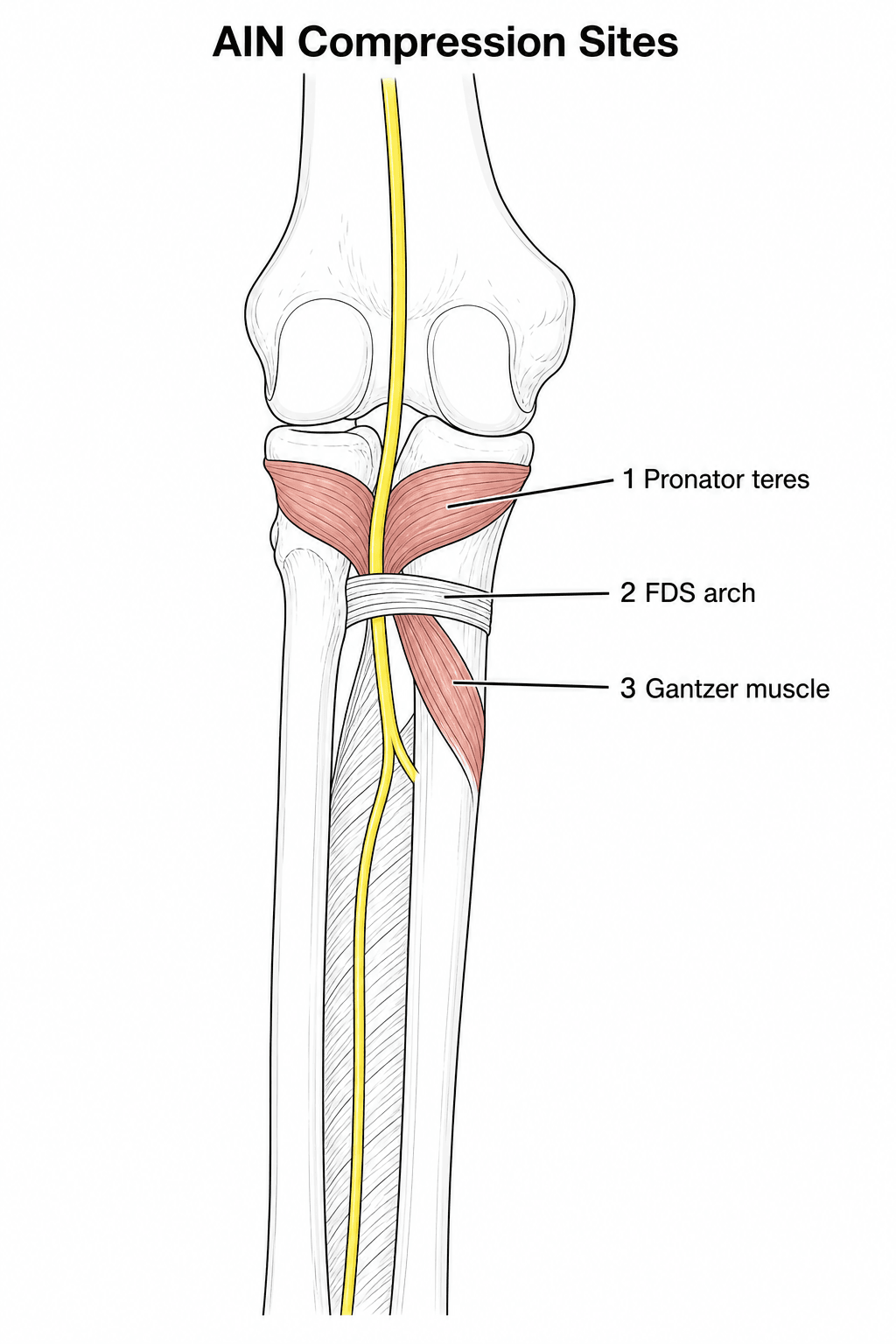
The anterior interosseous nerve can be compressed at multiple points along its course. The most common sites include the fibrous arch of the pronator teres (most frequent), the proximal edge of the flexor digitorum superficialis, an accessory head of the flexor pollicis longus (Gantzer muscle), and rarely the ligament of Struthers or a thrombosed radial artery. Unlike carpal tunnel syndrome, the compression is usually focal and the nerve distal to the lesion remains normal.
Neuritis (most common): Post-viral or idiopathic, self-limiting axonal degeneration Compression: Anatomic fibrous bands or muscle variants Trauma: Supracondylar fracture, forearm fracture, iatrogenic Inflammatory: Part of brachial plexitis (Parsonage-Turner)
FPL flexes the thumb IP joint while FDP index flexes the DIP joint. Both are required for a true tip-to-tip OK circle. When either or both are weak, the patient substitutes with a key pinch (thumb pad against radial side of index), producing the classic flat OK sign. This is pathognomonic when sensation remains intact.
Classification and Types
Classification by Cause
- Mechanism
- Post-viral or inflammatory
- Key Features
- Often painless or mild ache, isolated AIN
- Recovery Potential
- Excellent, 80-90 percent spontaneous
- Mechanism
- Brachial plexitis variant
- Key Features
- Severe preceding shoulder pain, multiple nerves
- Recovery Potential
- Good but slower, 6-18 months
- Mechanism
- Fibrous bands, Gantzer muscle
- Key Features
- Insidious or post-traumatic, no pain
- Recovery Potential
- Variable, may need decompression
- Mechanism
- Fracture, laceration, iatrogenic
- Key Features
- Clear history, often complete lesion
- Recovery Potential
- Depends on nerve continuity
Identifying the underlying mechanism guides the duration of observation versus timing of exploration.
Clinical Assessment
- Onset: Acute after viral illness versus insidious compression
- Pain: Severe shoulder pain suggests Parsonage-Turner, mild forearm ache suggests compression
- Function: Difficulty with pinch, buttoning, writing, using scissors
- Trauma: Previous supracondylar or forearm fracture
- Systemic: Recent vaccination, infection, or inflammatory condition
- OK sign: Ask patient to make circle with thumb and index, apply resistance
- FPL strength: Thumb IP flexion, grade 0-5, compare contralateral
- FDP index: DIP flexion of index only, middle finger should be normal
- PQ test: Resisted pronation elbow flexed 90 degrees, weakness indicates AIN
- Sensation: Light touch and two-point discrimination normal in median distribution
- Other nerves: Screen radial, ulnar, and remaining median (PT, FCR, FDS) to exclude plexitis
Technique: Patient sits with forearm supinated. Ask them to touch the tip of the thumb to the tip of the index finger forming a perfect O. Apply gentle resistance to the thumb IP and index DIP while observing the posture. Positive finding: Inability to maintain tip-to-tip contact, resulting in a flat or key pinch posture. The thumb IP and index DIP remain extended or hyperextended. Interpretation: Confirms combined FPL and FDP index weakness. Isolated FPL weakness may still allow partial circle with index compensation.
AIN Syndrome versus Pronator Syndrome
The two median-nerve entrapments of the proximal forearm are constantly confused and are a favourite exam pairing. The discriminator is sensory involvement and the muscles affected.
- AIN syndrome
- AIN (pure motor terminal branch)
- Pronator syndrome
- Main median nerve trunk in the forearm
- AIN syndrome
- NORMAL (no cutaneous fibres)
- Pronator syndrome
- Altered — palmar cutaneous branch (thenar/palm) and median digital territory
- AIN syndrome
- FPL, FDP index, pronator quadratus (OK-sign failure)
- Pronator syndrome
- May involve all median muscles incl. FCR, FDS, thenar; AIN muscles variably
- AIN syndrome
- Minimal or none
- Pronator syndrome
- Aching volar forearm pain, worse with activity
- AIN syndrome
- OK sign, resisted pronation (PQ)
- Pronator syndrome
- Pain/paraesthesiae on resisted pronation (PT), resisted long-finger FDS, or resisted elbow flexion-supination (lacertus)
- AIN syndrome
- Absent
- Pronator syndrome
- Usually absent (helps separate from carpal tunnel, which is nocturnal)
The key points: pronator syndrome has sensory symptoms and forearm pain because the whole median trunk is involved — including the palmar cutaneous branch, which arises proximal to the carpal tunnel — whereas AIN syndrome is purely motor with normal sensation. Pronator syndrome is also distinguished from carpal tunnel syndrome by the lack of night symptoms and by palmar (thenar-eminence) sensory involvement: the palmar cutaneous branch is spared in carpal tunnel because it runs superficial to the flexor retinaculum.
AIN syndrome = pure motor, normal sensation. Pronator syndrome = motor PLUS sensory (forearm ache and median-territory/palmar sensory change, but typically NO night pain — unlike carpal tunnel). If a "weak pinch" patient has any median sensory change, the lesion is the main median trunk (pronator syndrome or more proximal), not the AIN.
Investigations
Investigation Sequence
Diagnosis is clinical. Motor testing of FPL, FDP index and PQ plus intact median sensation is sufficient in most cases. No imaging required initially.
Indication: Confirm axonal loss, exclude more proximal median lesion, map other nerve involvement (Parsonage-Turner). Findings: Reduced amplitude of compound muscle action potentials from FPL/PQ, normal sensory studies, fibrillation potentials in affected muscles after 3 weeks. Timing: Perform at 3-4 weeks post-onset for maximal sensitivity.
Indication: Visualise fibrous bands, Gantzer muscle, nerve swelling, or space-occupying lesion. Findings: Nerve enlargement proximal to compression site, loss of fascicular pattern. Limitation: Normal study does not exclude neuritis or subtle compression.
Views: AP and lateral elbow, forearm. Look for: Supracondylar fracture callus, forearm fracture malunion, anomalous bone.
Do not order MRI of the forearm as the first test. The diagnosis is made at the bedside with the OK sign and PQ testing. Imaging and electrophysiology are reserved for atypical features, failure to recover, or when surgery is being considered. Early EMG (less than 3 weeks) may be falsely negative.
Hourglass Fascicular Constriction and Neuralgic Amyotrophy
A major shift in understanding is that many spontaneous "AIN palsies" are not extrinsic compressions at all, but intrinsic fascicular lesions within the neuralgic amyotrophy (Parsonage-Turner) spectrum.
- High-resolution ultrasound and MRI increasingly demonstrate one or more hourglass-like constrictions — sometimes frank fascicular torsion — of the AIN fascicles, often located proximal to the elbow within the median nerve itself, rather than a discrete band at a classic compression site.
- The Maldonado-type re-analysis (see Evidence Base) found that presumed "isolated AIN" lesions frequently show more diffuse, proximal median-nerve fascicular involvement on careful EDX/MRI review, with no radiological sign of compression — supporting an inflammatory rather than entrapment mechanism in many cases.
Why it matters surgically:
- If exploration for a presumed entrapment finds a normal nerve at the classic compression sites, the lesion may be an intrinsic constriction more proximally, and a simple decompression will not help.
- For a demonstrated hourglass constriction that fails to recover, the described options are interfascicular neurolysis, or resection of the constricted segment with nerve grafting or fascicular transfer — fundamentally different from a release.
- This is the AIN analogue of the same phenomenon seen in PIN palsy, and it explains why the results of simply decompressing spontaneous cases are unpredictable.
A spontaneous AIN palsy with a normal nerve at the usual entrapment sites may be an hourglass fascicular constriction or torsion within the median nerve more proximally (neuralgic amyotrophy spectrum), best shown on high-resolution US/MRI. It is treated by neurolysis or resection-and-graft of the constriction, not by a routine decompression — so image the whole nerve, not just the forearm.
Management Algorithm
Initial Management - Observation (First Line for Most Cases)
Goal: Allow spontaneous axonal regeneration while monitoring for recovery.
Observation Protocol
Confirm isolated AIN motor deficit, document baseline strength grades, counsel on natural history. Reassure patient that 70-90 percent of neuritis cases recover without surgery.
Repeat OK sign, FPL, FDP index and PQ grading. Photograph pinch posture for comparison. Any improvement = continue observation.
Baseline EMG if not already performed. Repeat at 3-4 months to assess reinnervation. Nascent motor units indicate ongoing recovery.
No clinical or EMG recovery after 4-6 months = consider surgical exploration. Partial recovery continuing = extend observation to 9-12 months.
Most spontaneous recoveries occur between 3 and 9 months. Waiting beyond 12 months risks irreversible muscle atrophy and poorer surgical outcomes. The decision for exploration is individualised based on patient age, occupation, EMG evidence of ongoing denervation versus reinnervation, and patient preference.
Complications
- Incidence
- 10-20 percent if no recovery by 12 months
- Risk Factors
- Delayed diagnosis, age greater than 50, complete lesion
- Management
- Tendon transfer (FDS to FPL) if no recovery
- Incidence
- 30-40 percent of operated cases
- Risk Factors
- Greater than 12 months delay, severe axonal loss
- Management
- Realistic pre-op counselling essential
- Incidence
- Common if sensory symptoms attributed incorrectly
- Risk Factors
- Failure to test OK sign and PQ
- Management
- Re-explore median nerve at elbow level
- Incidence
- 5-10 percent of transfers
- Risk Factors
- Adhesions, over-tensioning, donor weakness
- Management
- Revision surgery or therapy
The most common error is performing carpal tunnel decompression in a patient with isolated AIN palsy. These patients have normal sensation and normal thenar bulk. Always perform the OK sign test and PQ testing before listing any patient for carpal tunnel surgery. A normal sensory study in the presence of motor deficit should raise suspicion of AIN pathology.
Outcomes and Prognosis
- Observation Success
- 80-90 percent full or near-full recovery
- Surgical Success
- Rarely required
- Long-term Function
- Excellent pinch strength
- Observation Success
- 70-85 percent useful recovery by 18 months
- Surgical Success
- Not indicated
- Long-term Function
- Mild residual weakness common
- Observation Success
- Variable without surgery
- Surgical Success
- 70-80 percent improvement
- Long-term Function
- Good if less than 9 months delay
- Observation Success
- Poor spontaneous recovery
- Surgical Success
- 40-60 percent improvement
- Long-term Function
- Often residual lag, consider transfer
Best prognosis: Young patient, partial lesion, early improvement within 3 months, idiopathic neuritis. Poor prognosis: Age greater than 50, complete lesion at presentation, greater than 12 months delay to surgery, Parsonage-Turner with widespread involvement. Key threshold: 6 months without any clinical or EMG recovery is the usual point at which surgical exploration is discussed.
Guidelines, Registries & Global Practice
- AIN palsy is uncommon but frequently under-diagnosed worldwide because of the pure motor presentation
- Neuritis predominates in all regions, often post-viral
- Compressive cases are reported more in high-resource centres with access to EMG and ultrasound
- Parsonage-Turner incidence appears similar across populations
- High-resource: Early EMG, serial ultrasound, hand therapy monitoring, microsurgical decompression available
- Limited-resource: Clinical diagnosis alone, prolonged observation, limited access to nerve surgery
- Universal principle: Outcome depends on accurate diagnosis (OK sign + PQ test) and patience with observation
- Surgery: Concentrated in specialist hand units globally, results better with shorter delay
- Diagnosis emphasis
- OK sign + PQ testing, normal sensation
- Observation duration
- 3-6 months minimum, up to 12 months for neuritis
- Surgery indications
- No recovery + compressive features on imaging/EMG
- Diagnosis emphasis
- Clinical diagnosis, EMG for confirmation and prognosis
- Observation duration
- At least 6 months, longer if EMG shows reinnervation
- Surgery indications
- Plateau at 6-9 months in clear entrapment
- Diagnosis emphasis
- High index of suspicion, exclude Parsonage-Turner
- Observation duration
- Individualised, 4-12 months typical
- Surgery indications
- Failed observation, patient preference, occupation
- Diagnosis emphasis
- Consider in all median nerve injuries around elbow
- Observation duration
- Not specifically addressed
- Surgery indications
- Exploration in open injuries or fracture-related
There is no dedicated registry for AIN syndrome. Evidence is limited to retrospective case series and anatomic studies. The consistent message across guidelines is that the majority of cases are neuritis and recover spontaneously. Surgery is reserved for clear compressive pathology or failure to progress after adequate observation. Documentation of the OK sign test and serial motor grades is essential worldwide.
Controversies & Areas of Uncertainty
Most authors recommend 6-12 months, but the exact point at which surgery becomes futile is not defined by high-quality data. Some units operate at 4 months while others wait 18 months for neuritis. Patient age, occupation and EMG trajectory guide individual decisions.
Ultrasound can demonstrate nerve swelling and dynamic compression but is operator-dependent. MRI better visualises muscle denervation and occult masses but is more expensive. Neither changes management in straightforward neuritis.
FDS to FPL transfer is reliable for permanent AIN loss but timing is debated. Some surgeons offer it at 12 months while others wait 18-24 months. The decision balances irreversible atrophy against the small chance of very late reinnervation.
When the AIN appears normal at exploration, some surgeons perform proximal median nerve fascicular neurolysis looking for intraneural compression. Evidence for benefit is anecdotal and the procedure risks iatrogenic injury to other fascicles.
MCQ Practice Points
Q: Which muscles are innervated by the anterior interosseous nerve? A: FPL, FDP to index and middle (radial half), and PQ. The AIN is the terminal motor branch of the median nerve. It supplies the deep flexors of the thumb and index (and often middle) finger plus the pronator quadratus. The middle finger FDP may receive dual innervation from the ulnar nerve.
Q: What is the significance of an abnormal OK sign in a patient with normal median sensation? A: It indicates AIN palsy. The OK sign requires simultaneous IP flexion of the thumb (FPL) and DIP flexion of the index (FDP index). Failure produces a flat or key pinch. Normal sensation excludes carpal tunnel syndrome or more proximal median neuropathy.
Q: How do you differentiate AIN syndrome from Parsonage-Turner syndrome? A: Pain history and nerve involvement. Parsonage-Turner features severe shoulder girdle pain preceding weakness and often involves additional nerves (suprascapular, long thoracic). Pure AIN compression is usually painless or has mild forearm ache and remains isolated to AIN muscles.
Q: When is surgical decompression indicated for AIN palsy? A: After 4-6 months of observation with no clinical or EMG recovery in compressive or traumatic cases. Neuritis (including Parsonage-Turner) is observed for at least 12 months. Surgery releases the pronator teres, FDS arch, and any Gantzer muscle or ligament of Struthers.
Q: What is the expected recovery rate for idiopathic AIN neuritis? A: 80-90 percent achieve useful or full recovery with observation alone. Most recovery occurs between 3 and 12 months. Patients over 50 years and those with complete lesions at presentation have poorer prognosis.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 34-year-old office worker presents with 8 weeks of difficulty pinching and writing. She recalls a flu-like illness 3 months ago. She has no forearm pain or numbness. On examination she cannot make an OK sign, FPL and FDP index are grade 3, PQ is weak, and median sensation is normal. What is your diagnosis and management?”
“A 28-year-old man sustained a supracondylar humerus fracture 7 months ago treated with closed reduction and percutaneous pinning. Pins were removed at 6 weeks. He now has persistent inability to flex his thumb IP and index DIP with a flat OK sign. Sensation is normal. EMG at 5 months showed complete denervation of FPL and FDP index with no reinnervation. How would you manage?”
Key Anatomy
- AIN = pure motor terminal branch of median nerve, 5-8 cm distal to lateral epicondyle
- Innervates FPL, FDP index (radial half), and PQ only
- No cutaneous sensory fibres, therefore normal median sensation
- Compression sites: PT arch, FDS arch, Gantzer muscle, ligament of Struthers
Diagnosis
- OK sign failure = inability to flex thumb IP + index DIP simultaneously
- PQ weakness tested by resisted pronation with elbow flexed 90 degrees
- Normal sensation and thenar bulk distinguishes from carpal tunnel
- Parsonage-Turner suspected if severe preceding shoulder pain or other nerves involved
Management Algorithm
- Observation first for 4-6 months (up to 12 months for neuritis)
- Monthly motor grading + EMG at 3 months and 6 months
- Surgery if no recovery and compressive features or plateau on EMG
- Decompression releases PT, FDS arch, Gantzer, ligament of Struthers
Surgical Pearls
- Henry volar approach, protect lateral cutaneous nerve of forearm
- Release all potential compression points even if nerve looks normal
- Neurolysis or grafting if neuroma-in-continuity found
- Early motion post-op, reinnervation may take 6-12 months
Complications & Salvage
- Permanent weakness if greater than 12 months delay or severe axonal loss
- Tendon transfer (FDS ring to FPL) for failed nerve recovery
- Misdiagnosis as carpal tunnel is common and avoidable
- Incomplete recovery after surgery in 30-40 percent of cases
Evidence Base and Key Trials
The anterior interosseous nerve syndrome
- Classic description of the anterior interosseous nerve syndrome, with particular attention to its anatomical variations
- Emphasised the pure motor deficit (FPL, FDP-index, pronator quadratus) with no sensory loss
- Described compression by fibrous bands of the pronator teres and the flexor digitorum superficialis arch
Gantzer muscle and anterior interosseous nerve compression
- Anatomical study of 25 limbs; Gantzer's muscle (accessory head of FPL) present in 13 (52 percent) and supplied by the anterior interosseous nerve
- Arose from the medial humeral epicondyle in 85 percent (dual epicondyle/coronoid origin in the rest) and inserted onto the ulnar part of FPL
- Gantzer's muscle ALWAYS lay posterior to both the median and anterior interosseous nerves
The incomplete anterior interosseous nerve syndrome
- Series of 33 cases of an INCOMPLETE AIN syndrome - isolated paresis or paralysis of either the flexor pollicis longus OR the index flexor digitorum profundus
- Must be distinguished from flexor tendon rupture, tendon adhesion and stenosing tenosynovitis
- Compression most often by fibrous bands from the deep head of pronator teres and the brachialis fascia
- Recommended observing paresis (most improve spontaneously) and exploring/neurolysing complete paralysis of a muscle-tendon unit only if it fails to improve after 12 weeks
Reinterpretation of Electrodiagnostic Studies and Magnetic Resonance Imaging Scans in Patients with Nontraumatic 'Isolated' Anterior Interosseous Nerve Palsy
- Many presumed isolated AIN palsies show more proximal median nerve or fascicular involvement on reinterpreted EDX/MRI
- True isolated AIN is less common than previously thought; careful imaging review essential
- Changes management by identifying treatable compressive lesions or avoiding unnecessary surgery