Surgical Emergency | Kanavel Signs | Urgent Drainage
- Kanavel four cardinal signs for flexor tenosynovitis diagnosis
- Anatomical boundaries of thenar, midpalmar, and hypothenar spaces
- Indications for emergent surgical drainage vs observation with IV antibiotics
- Horseshoe abscess connects radial and ulnar bursae through Parona space
- MRSA prevalence requires empiric vancomycin until cultures available
- “Describe incisions for each deep space to demonstrate anatomical knowledge
- “Know boundaries: midpalmar septum separates thenar from midpalmar space
- “Explain why tendons necrose quickly: tenosynovium is only blood supply
- “Recognize necrotizing fasciitis - pain out of proportion, crepitus, systemic toxicity
Sign 1: Finger held in semi-flexion.
Sign 2: Sausage digit (entire length).
Sign 3: Tenderness along entire flexor sheath course.
Sign 4: The most specific sign. Severe pain on passive extension.
Introduction
Deep space infections of the hand represent surgical emergencies requiring urgent diagnosis and aggressive treatment. Unlike superficial infections, deep space abscesses develop within anatomically defined fascial compartments where pus accumulates under pressure, compromising vascular supply and destroying tissues. The unique anatomy of the hand creates multiple potential spaces where infection can track, requiring thorough understanding for effective surgical drainage.
The clinical challenge lies in early recognition before irreversible damage occurs. Delay in diagnosis or inadequate surgical drainage results in tendon necrosis, joint destruction, compartment syndrome, and potential digital amputation. Modern antibiotic resistance patterns, particularly MRSA prevalence, complicate empiric therapy decisions.
- Incidence: 2-3 per 10,000 population annually
- Peak age: 30-50 years
- Male predominance (3:1)
- Risk factors: diabetes (40%), immunosuppression
- MRSA prevalence: 30-50% community-acquired
- Delayed presentation common (average 4-5 days)
- Staphylococcus aureus: 60-70% (MRSA 30-50%)
- Streptococcus species: 15-20%
- Polymicrobial: 15-20% (diabetics, contaminated wounds)
- Eikenella corrodens: Human bites
- Pasteurella multocida: Cat/dog bites
- Mycobacteria: Chronic tenosynovitis
- Inoculation via penetrating trauma (70%)
- Direct spread from adjacent infection
- Hematogenous seeding (rare)
- Fascial compartments trap purulent fluid
- Pressure compromises blood supply
- Progressive tissue necrosis develops
Anatomical Spaces of the Hand
Understanding the fascial boundaries defining each space is essential for surgical planning and complete drainage.
Thenar Space
The thenar space lies on the radial side of the hand bounded by critical anatomical structures.
- Radial: Thenar muscles and adductor pollicis
- Ulnar: Midpalmar septum (from third metacarpal to palmar fascia)
- Dorsal: Adductor pollicis fascia
- Palmar: Flexor tendon sheaths to index and long fingers
- Proximal: Carpal tunnel
- Distal: First web space
- Index and long finger lumbrical muscles
- Flexor tendon sheaths (index, long)
- Digital neurovascular bundles
- First web space fullness and swelling
- Thumb held in abduction
- Thenar eminence prominence
- Pain with thumb adduction
Midpalmar Space
The midpalmar space occupies the central and ulnar palm, containing important neurovascular structures.
- Radial: Midpalmar septum (from third metacarpal)
- Ulnar: Hypothenar muscles
- Dorsal: Metacarpals and interosseous fascia
- Palmar: Flexor tendons and palmar fascia
- Proximal: Carpal tunnel
- Distal: Distal palmar crease
- Lumbricals to ring and small fingers
- Flexor tendon sheaths (ring, small)
- Superficial palmar arch
- Digital nerves
- Loss of palmar concavity (palm balloons out)
- Ring and small fingers held flexed
- Dorsal hand swelling (dorsal subcutaneous tissue looser)
- Pain with finger extension
Hypothenar Space
Smaller space overlying hypothenar muscles, less commonly infected.
- Radial: Midpalmar space (no distinct septum)
- Ulnar: Ulnar border of hand
- Dorsal: Fifth metacarpal
- Palmar: Hypothenar muscle fascia
- Proximal: Carpal tunnel
- Distal: Distal palmar crease
- Hypothenar eminence swelling
- Small finger held flexed
- Limited ulnar hand tenderness
- Often confused with midpalmar infection
Parona Space (Quadrilateral Space)
Critical space in distal forearm connecting flexor tendon sheaths, enabling horseshoe abscess formation.
- Radial: Flexor pollicis longus (FPL) tendon
- Ulnar: Flexor digitorum profundus (FDP) tendons
- Dorsal: Pronator quadratus and distal radius
- Palmar: Flexor digitorum superficialis (FDS) tendons
- Communication point between radial and ulnar bursae
- Horseshoe abscess: infection of both bursae plus Parona space
- Requires drainage in distal forearm AND digits
- High morbidity if missed
The Radial and Ulnar Bursae and Proximal Spread
The topic repeatedly relies on the radial and ulnar bursae - to explain the horseshoe abscess, why small-finger tenosynovitis threatens the palm, and how Parona's space connects the two. These are the synovial flexor bursae, and understanding their extent explains which digital infections spread proximally and which stay confined.
- Large synovial sheath enveloping the flexor digitorum superficialis and profundus tendons as they pass through the carpal tunnel.
- In most people it is directly continuous with the flexor sheath of the small finger, so small-finger pyogenic flexor tenosynovitis can decompress proximally into the palm and, through the carpal tunnel, into the distal forearm.
- Extends roughly 2 to 3 cm proximal to the proximal wrist crease, into the region of Parona's space.
- The digital sheaths of the index, middle and ring fingers usually terminate at the metacarpal-neck / distal palm level and do NOT communicate directly with the ulnar bursa - which is why isolated index/middle/ring tenosynovitis tends to remain confined to the digit.
- The synovial sheath of the flexor pollicis longus, continuous distally with the thumb flexor sheath and extending proximally through the carpal tunnel into the distal forearm.
- This continuity is why thumb flexor tenosynovitis (like small-finger disease) can track proximally rather than staying in the digit.
- The radial and ulnar bursae communicate in a substantial but variable proportion of individuals (an anatomical variant), typically within or adjacent to Parona's space in the distal forearm.
- Where this communication exists, infection of one bursa can traverse to the other, producing the horseshoe abscess (thumb radial bursa, small-finger ulnar bursa, and the connecting Parona's space all involved) - all three sites must be drained.
Why thumb and small finger are the dangerous digits: their flexor sheaths are continuous with the radial and ulnar bursae respectively, so tenosynovitis of the thumb or small finger can decompress proximally into the palm and distal forearm and - where the bursae communicate - cross to the opposite side as a horseshoe abscess. Infection of the index, middle or ring finger sheaths is far more likely to stay contained within the digit because those sheaths usually end at the distal palm. Always examine the whole hand and distal forearm when the thumb or small finger is the infected digit.
Flexor Tenosynovitis
Infection within the synovial sheath surrounding flexor tendons represents a surgical emergency. The tendon's blood supply derives entirely from vinculae and synovium - infection disrupts this, leading to rapid tendon necrosis.
Kanavel Cardinal Signs
The four cardinal signs described by Kanavel in 1912 remain the diagnostic gold standard.
Detailed Sign Descriptions:
-
Finger Held in Flexed Posture: Patient maintains digit in semiflexion (20-30 degrees) to minimize tendon sheath pressure. Attempts to extend finger produce severe pain.
-
Fusiform Swelling: Uniform swelling along entire digit length creating sausage-like appearance. Distinguishes from localized abscess or paronychia.
-
Tenderness Along Flexor Sheath: Exquisite tenderness over entire tendon course from fingertip to palm. Palpate A1 pulley, flexor sheath, and proximal extent.
-
Pain with Passive Extension: Severe pain elicited by gentle passive finger extension. Stretching infected tendon sheath causes intense pain - pathognomonic finding.
Pathophysiology of Tendon Necrosis
- 0-24 hours: Purulent fluid accumulates in sheath
- 24-48 hours: Pressure exceeds capillary perfusion pressure
- 48-72 hours: Ischemia develops, early tendon changes
- Greater than 72 hours: Irreversible tendon necrosis begins
- Greater than 7 days: Complete tendon destruction, adhesions
- Pressure-induced ischemia (primary)
- Bacterial toxins and proteases
- Inflammatory mediator release
- Adhesion formation
- Synovial destruction
Golden Period for Drainage: Flexor tenosynovitis diagnosed within 48 hours has excellent prognosis with irrigation and drainage. Beyond 72 hours, tendon necrosis risk increases dramatically. Beyond 7 days, salvage procedures (tendon grafting, arthrodesis, amputation) often required. Early aggressive surgical intervention is paramount.
Clinical Assessment and Diagnosis

History
- Mechanism of injury: Penetrating trauma, bite, crush
- Timing: Hours vs days since symptom onset
- Progression: Rapid worsening suggests aggressive infection
- Systemic symptoms: Fever, chills, malaise
- Medical comorbidities: Diabetes, immunosuppression, vascular disease
- Prior antibiotics: May mask presentation
- Tetanus status
- Pain out of proportion to examination (necrotizing infection)
- Rapid progression (hours not days)
- Crepitus (gas-forming organisms)
- Systemic toxicity (sepsis)
- Sensory changes (compartment syndrome)
Physical Examination
- Digit/hand posture
- Swelling pattern and distribution
- Skin changes: erythema, blistering, necrosis
- Wound or entry site
- Lymphangitic streaking
- Fluctuance indicating abscess
- Tenderness localization
- Crepitus (gas)
- Pulse examination
- Lymph node examination
- Active ROM (limited by pain)
- Passive ROM (pain with passive extension in tenosynovitis)
- Neurovascular status (critical documentation)
- Grip strength if able
- Kanavel signs: Systematic assessment all four
- Compartment assessment: Firm, tense compartments
- Allen test: Vascular adequacy
- Two-point discrimination: Baseline nerve function
Laboratory Studies
- Complete blood count (WBC typically elevated)
- C-reactive protein (CRP) and ESR
- Blood glucose (diabetes screening)
- Blood cultures if systemic signs
- Wound culture and Gram stain
- Rule out foreign body (90% sensitivity for metal/glass)
- Assess for osteomyelitis
- Identify gas in soft tissues
- Check for fracture
- Identify fluid collections
- Guide aspiration
- Assess tendon integrity
- Point-of-care availability
- Delineate abscess extent
- Assess deep space involvement
- Evaluate osteomyelitis
- Plan complex surgery
- Foreign body localization
- Gas identification
- Bony involvement
- Alternative to MRI
Imaging Does Not Replace Clinical Diagnosis: Deep space infections and flexor tenosynovitis are clinical diagnoses based on history and physical examination. Imaging is adjunctive to rule out foreign body, assess extent, or plan complex surgery. Never delay surgical drainage to obtain advanced imaging when clinical diagnosis is clear. The examination room is where diagnosis is made.
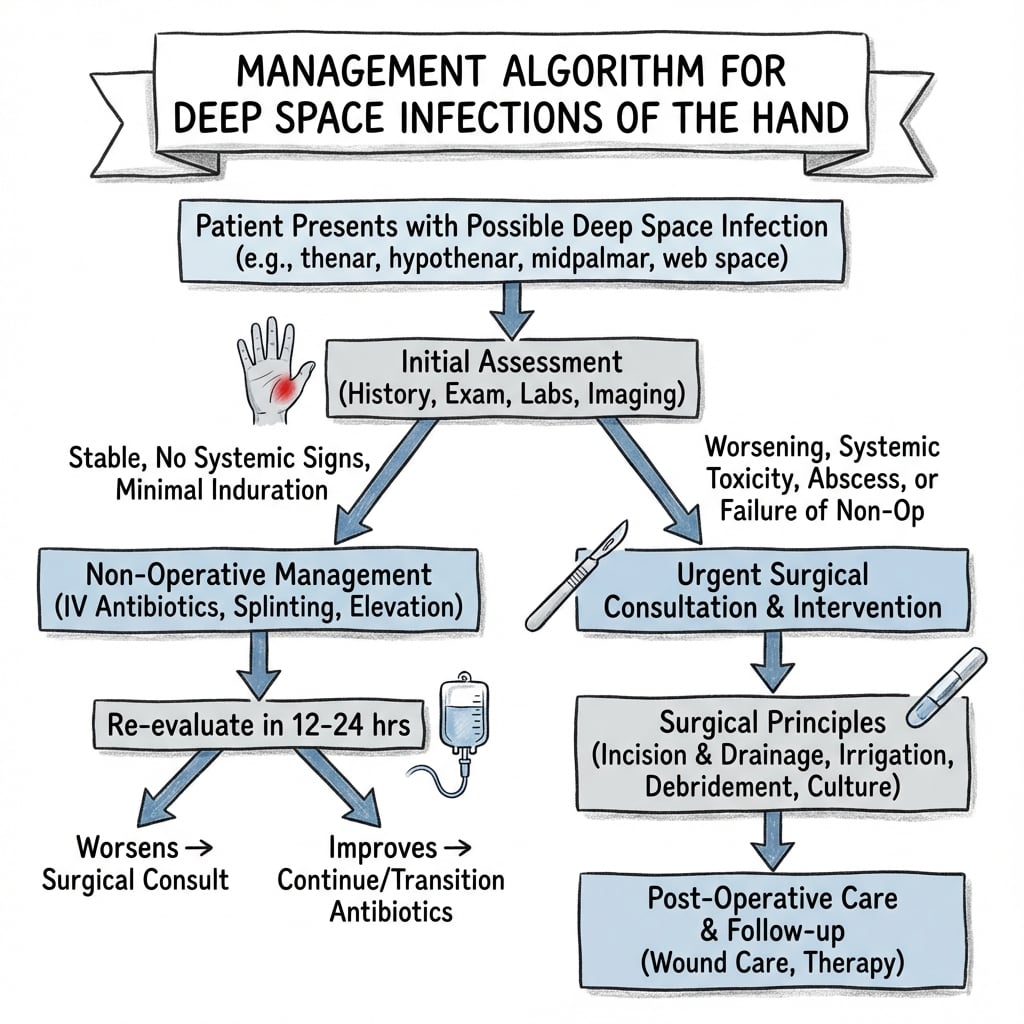
Management Principles
Non-Operative Management
Limited role for antibiotics alone - reserved for very early presentation or specific scenarios.
- Presentation within 24 hours of symptom onset
- Partial Kanavel signs (not all four present)
- Minimal systemic symptoms
- No abscess on imaging
- Reliable patient for close monitoring
- Admit for IV antibiotics and observation
- Reassess every 4-6 hours
- Splint in position of function
- Elevation
- Serial examinations by hand surgeon
- Proceed to surgery if no improvement 12-24 hours OR any worsening
Most Cases Require Surgery: Greater than 80% of patients initially trialed on antibiotics eventually require surgical drainage. Early surgery preferred in most cases.
Surgical Indications
- All four Kanavel signs present
- Fluctuant abscess clinically evident
- Presentation greater than 48 hours with symptoms
- Failed antibiotic trial (no improvement 12-24 hours)
- Systemic toxicity
- Compartment syndrome
- Necrotizing infection suspected
- Emergent (within 6 hours): Necrotizing fasciitis, compartment syndrome, systemic sepsis
- Urgent (within 24 hours): Established tenosynovitis, deep space abscess
- Semi-urgent (24-48 hours): Early tenosynovitis on antibiotic trial
Empiric Antibiotic Selection
Antibiotic selection must cover most likely organisms while awaiting culture results.
- likely
- MSSA, Streptococcus
- firstLine
- Cefazolin 2g IV q8h
- alternative
- Clindamycin 600mg IV q8h (PCN allergy)
- coverage
- Excellent Gram-positive, no MRSA coverage
- likely
- MRSA, Streptococcus
- firstLine
- Vancomycin 15-20mg/kg IV q8-12h
- alternative
- Linezolid 600mg IV q12h
- coverage
- Broad Gram-positive including MRSA
- likely
- Eikenella, Strep, anaerobes
- firstLine
- Ampicillin-sulbactam 3g IV q6h
- alternative
- Ceftriaxone 1g IV daily PLUS metronidazole 500mg IV q8h
- coverage
- Oral flora, anaerobes, Eikenella
- likely
- Pasteurella, Staph, Strep
- firstLine
- Ampicillin-sulbactam 3g IV q6h
- alternative
- Ceftriaxone 2g IV daily
- coverage
- Pasteurella multocida highly sensitive to PCN
- likely
- Polymicrobial, MRSA, anaerobes
- firstLine
- Vancomycin PLUS piperacillin-tazobactam 4.5g IV q6h
- alternative
- Vancomycin PLUS cefepime 2g IV q8h PLUS metronidazole
- coverage
- Broad spectrum, MRSA, Gram-negatives, anaerobes
- likely
- Vibrio vulnificus, Aeromonas
- firstLine
- Ceftriaxone 2g IV daily PLUS doxycycline 100mg IV q12h
- alternative
- Ciprofloxacin 400mg IV q12h PLUS doxycycline
- coverage
- Vibrio coverage critical (can be fatal)
Culture-Directed Therapy:
- Narrow antibiotics based on culture and sensitivity results
- Typically 7-14 days total therapy
- Transition to oral when clinically improving (48-72 hours)
- Longer duration if osteomyelitis (4-6 weeks)
Management Algorithm
Surgical Techniques
Flexor Tenosynovitis Irrigation and Drainage:
Two main approaches: closed catheter irrigation vs open drainage. Closed technique preferred for early disease, open for established infection or failed closed drainage.
- Early tenosynovitis (less than 48 hours)
- No gross purulence expected
- No tendon necrosis suspected
- Distal Incision: 3-4mm transverse incision at A5 pulley level (flexion crease)
- Proximal Incision: 1cm incision at A1 pulley in palm
- Sheath Identification: Carefully identify flexor sheath at both sites
- Catheter Placement: 8Fr pediatric feeding tube inserted distal, advanced to proximal incision
- Irrigation: 500-1000mL saline flushed through sheath
- Efflux Assessment: Monitor fluid clarity from proximal wound
- Culture: Send purulent fluid for culture
- Catheter Management Options:
- Remove catheter, close wounds (preferred)
- Leave catheter for postoperative irrigation (controversial)
- Presentation greater than 72 hours
- Failed closed irrigation
- Suspected tendon necrosis
- Need for debridement
- Incision: Zigzag (Bruner) incision entire digit length
- Exposure: Elevate skin flaps preserving neurovascular bundles
- Sheath Opening: Open A2 and A4 pulleys in windows
- Inspection: Assess tendon viability, synovium condition
- Irrigation: Copious lavage of entire sheath
- Debridement: Remove necrotic tissue, inflamed synovium
- Assessment: Test tendon integrity with gentle tension
- Closure: Leave wounds open OR loose closure with drains
- A2 and A4 pulleys critical for digit function
- Open windows in pulleys, preserve as much as possible
- If pulley completely destroyed, consider reconstruction later
- Do not sacrifice A2/A4 unless absolutely necessary
- Splint in intrinsic-plus position
- Elevation critical
- IV antibiotics continue 48-72 hours minimum
- Early protected AROM when pain improving (3-5 days)
- Hand therapy for scar management and ROM
- Early drainage (less than 48 hours): 90-95% salvage, full function
- Delayed drainage (greater than 72 hours): 70-80% salvage, stiffness common
- Tendon necrosis: Requires staged reconstruction (graft, arthrodesis)
This comprehensive technique section demonstrates surgical decision-making and technical knowledge examiners expect.
Guidelines, Registries & Global Practice
Global Epidemiology
- Hand infections account for roughly 15-20% of emergency hand presentations worldwide; pyogenic flexor tenosynovitis (PFT) comprises 2.5-9.4% of all hand infections in published series.
- Community-acquired MRSA accounts for 30-73% of hand infection cultures across US, UK and Asian series (Chung et al. found 30% in a paediatric cohort), with higher rates in deeper, more severe abscesses.
- Risk is concentrated in manual, agricultural, fishing and food-handling occupations; penetrating trauma is the dominant mechanism.
- Regional exposures change the microbiology: warm coastal/marine injury raises Vibrio vulnificus and Aeromonas risk; soil-contaminated agricultural wounds favour polymicrobial and clostridial contamination; aquarium/fish-tank exposure suggests Mycobacterium marinum in chronic cases.
- Outcomes correlate strongly with time to surgical decompression and with the Pang tissue-based group (purulence and digital ischaemia drive amputation risk).
Side-by-Side Society Guidance
- empiric
- Cover S. aureus incl. MRSA in purulent/severe infection; add gram-negative/anaerobe cover for bites and contaminated wounds
- mrsa
- Vancomycin (or linezolid/daptomycin) when MRSA suspected or local prevalence high
- note
- Emphasises incision and drainage as primary for abscesses; antibiotics adjunctive
- empiric
- Flucloxacillin-based cover for MSSA/Strep; co-amoxiclav for bites; add vancomycin/teicoplanin if MRSA risk
- mrsa
- Glycopeptide where MRSA prevalent or prior colonisation
- note
- Early hand-unit referral and washout within 24h widely advocated
- empiric
- Locally available beta-lactam (e.g. cloxacillin) +/- aminoglycoside; metronidazole for anaerobes
- mrsa
- Guided by local resistance data; vancomycin often restricted
- note
- Earlier surgical drainage emphasised where IV antibiotic supply and monitoring are limited
- Universal principle across all guidelines: deep space infections and established PFT are surgical problems - antibiotics are adjunctive and must not delay drainage.
- De-escalate to culture-directed therapy at 48-72 hours; transition to oral when clinically improving; extend to 4-6 weeks only if osteomyelitis is confirmed.
High- vs Limited-Resource Variation
- High-resource: point-of-care ultrasound, MRI for complex extent, 24/7 hand-surgery cover, closed catheter irrigation systems, formal hand therapy and splinting pathways.
- Limited-resource: clinical diagnosis predominates, plain radiographs to exclude foreign body/gas, lower threshold for early open drainage given constrained IV antibiotic supply and monitoring, and reliance on oral step-down (flucloxacillin/dicloxacillin, co-amoxiclav, clindamycin, trimethoprim-sulfamethoxazole for MRSA).
- Delayed presentation - common in remote and low-access settings - is the dominant modifiable driver of tendon necrosis and amputation everywhere.
Rehabilitation and Expected Recovery
- PFT with early surgery: typically 6-8 weeks to functional recovery.
- Deep space abscess: 4-8 weeks.
- Horseshoe abscess: 3-6 months, often with residual stiffness.
- Hand therapy (edema control, custom splinting, graded motion) materially improves final range of motion; telerehabilitation extends access where in-person services are scarce.
Special Considerations
Necrotizing Fasciitis
Life-threatening soft tissue infection requiring emergent surgical debridement. High mortality (20-30%) if delayed diagnosis.
Clinical Features:
- Pain out of proportion to examination
- Rapid progression (hours)
- Systemic toxicity (fever, tachycardia, hypotension)
- Skin changes: bullae, ecchymosis, crepitus
- Decreased sensation over affected area
LRINEC Score (Laboratory Risk Indicator for Necrotizing Fasciitis) - six routine labs (Wong et al. 2004):
- CRP greater than 150 mg/L: 4 points
- WBC: 1 point if 15-25, 2 points if over 25 (per mm³)
- Haemoglobin: 1 point if 11-13.5, 2 points if under 11 (g/dL)
- Sodium under 135 mmol/L: 2 points
- Creatinine over 1.6 mg/dL (greater than 141 micromol/L): 2 points
- Glucose over 180 mg/dL (greater than 10 mmol/L): 1 point
- Score 5 or less: low risk (under 50% probability)
- Score 6-7: intermediate risk
- Score 8 or more: high risk (over 75% probability)
- A score of 6 or more had positive predictive value 92% and negative predictive value 96% - but a low score does NOT exclude necrotising fasciitis when clinical suspicion is high
- Emergent surgery: Extensive debridement all necrotic tissue
- Broad-spectrum antibiotics: Vancomycin + piperacillin-tazobactam + clindamycin
- ICU admission: Resuscitation and vasopressor support
- Serial debridements: Return to OR every 24-48 hours
- Amputation: May be necessary for source control
Necrotizing Fasciitis Cannot Wait: This is a surgical emergency requiring operative debridement within 6 hours of diagnosis. Antibiotics and resuscitation alone are inadequate. Finger-test positive (easy blunt dissection along fascia), dishwater pus, and tissue necrosis confirm diagnosis. Delay increases mortality exponentially. Call senior help and proceed to operating room immediately.
Diabetic Hand Infections
Patients with diabetes develop more severe infections with worse outcomes.
- Impaired immune function
- Peripheral neuropathy (delayed presentation)
- Vascular insufficiency
- Polymicrobial infections common
- MRSA higher prevalence
- Lower threshold for surgical drainage
- Broader spectrum empiric antibiotics
- More extensive debridement
- Longer antibiotic duration
- Tighter glucose control perioperatively
- Higher amputation rate
Bite Wounds
Special category requiring specific antibiotic coverage and aggressive management.
- Most dangerous bite (worst outcomes)
- Eikenella corrodens characteristic
- "Fight bite" - closed fist injury (MCP joint often involved)
- High infection rate (15-30%)
- Antibiotics: Ampicillin-sulbactam
- Cat bites: Deep penetrating, Pasteurella multocida
- Dog bites: Crush injury, polymicrobial
- Antibiotics: Ampicillin-sulbactam covers both
- Copious irrigation
- Surgical debridement
- Leave wounds open (delayed primary closure 3-5 days)
- Antibiotics minimum 7 days
- Assess for joint involvement (MCP from fight bite)
MCQ Practice Points
Q: Why does pyogenic flexor tenosynovitis cause tendon necrosis so rapidly?
A: The intrasynovial flexor tendon is largely avascular and depends on the vinculae and synovial fluid diffusion for nutrition. Pus within the closed sheath raises intrathecal pressure above capillary perfusion pressure, producing ischaemia within 24-48 hours. Beyond 72 hours irreversible necrosis begins. This is why decompression and irrigation are time-critical - the sheath is a closed compartment, not merely an abscess cavity.
Q: What is the horseshoe (and collar-stud) abscess, and which structures must be drained?
A: A horseshoe abscess is the communication of infection between the radial bursa (flexor pollicis longus sheath of the thumb) and the ulnar bursa (small-finger flexor sheath extending into the palm) via Parona's space in the distal forearm. Adequate treatment requires drainage of all three sites - thumb sheath, small-finger sheath, AND Parona's space - or the infection persists. A collar-stud (collar-button) abscess is distinct: a web-space infection that tracks between the palmar and dorsal subcutaneous compartments through the intermetacarpal space, requiring drainage on both volar and dorsal sides.
Q: How does the Pang classification guide prognosis in PFT?
A: The three-tier Pang system (JBJS Am 2007) stratifies by tissue findings, not time alone. Group I (no subcutaneous purulence or digital ischaemia): best prognosis, 0% amputation, ~80% total active motion. Group II (purulence, no ischaemia): 8% amputation, ~72% TAM. Group III (purulence plus digital ischaemia): 59% amputation, ~49% TAM. Digital ischaemia is the single most ominous finding.
Q: A patient steps on a fish bone / sustains an oyster-shell laceration and develops rapidly progressive hand infection - what organism and cover must you not miss?
A: Marine exposure raises the risk of Vibrio vulnificus (and Aeromonas), which can cause fulminant, potentially fatal necrotising soft-tissue infection. Empirical cover must add a tetracycline (doxycycline) plus a third-generation cephalosporin (ceftriaxone) - standard staphylococcal regimens miss it. Combine with urgent surgical assessment.
At a Glance
Deep space infections of the hand are surgical emergencies requiring urgent drainage. The four key anatomical spaces are thenar, hypothenar, midpalmar (largest), and Parona's space (quadrilateral space at distal forearm). Flexor tenosynovitis is diagnosed by Kanavel's four cardinal signs: fusiform swelling, semi-flexed digit posture, tenderness along the flexor sheath, and pain with passive extension. Horseshoe abscess occurs when infection spreads between radial and ulnar bursae through Parona's space. MRSA prevalence (30-50%) requires empiric vancomycin coverage. Delayed treatment leads to tendon necrosis (tenosynovium is sole blood supply), joint destruction, and potential amputation.
THMDeep Space Boundaries - THM-P
Hook:THM-P organizes the four major deep spaces from radial to ulnar plus proximal
STEPKanavel Four Signs - STEP
Hook:Take a STEP toward urgent surgery when these signs present
DRAINSurgical Drainage - DRAIN
Hook:DRAIN the deep spaces correctly
Summary
Deep space infections of the hand represent surgical emergencies requiring urgent recognition and aggressive treatment. Understanding the anatomical boundaries of the thenar, midpalmar, hypothenar, and Parona spaces enables appropriate surgical drainage planning. Flexor tenosynovitis, diagnosed by Kanavel four cardinal signs, requires urgent surgical drainage within 24-48 hours to prevent tendon necrosis and digital amputation.
Early aggressive surgical intervention is the cornerstone of management, with antibiotics playing an adjunctive role. Empiric antibiotic coverage must include MRSA given 30-50% community prevalence, with adjustment based on clinical scenario (bite wounds, marine exposure, immunocompromised). Surgical technique must achieve complete drainage while preserving critical structures including A2/A4 pulleys and neurovascular bundles.
Delayed diagnosis or inadequate surgical drainage results in devastating complications including stiffness, tendon necrosis, amputation, and rarely necrotizing fasciitis with significant mortality. The hand surgeon must maintain a high index of suspicion, perform systematic examination for Kanavel signs and deep space involvement, and proceed expeditiously to operative drainage when indicated rather than prolonging ineffective antibiotic trials.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old construction worker presents to emergency 3 days after puncture wound to palm. He has throbbing pain, swelling of the palm with loss of the normal concavity, and difficulty moving his ring and small fingers which are held flexed. He has marked dorsal hand swelling. Temperature is 38.5°C. What is your diagnosis and management?”
“A 28-year-old woman presents with 12 hours of increasing small finger pain and swelling. She recalls a small cut 2 days ago while gardening. Examination shows the small finger held in 30 degrees of flexion, fusiform swelling of the entire digit, exquisite tenderness along the flexor sheath, and severe pain with any attempt at passive extension. What is your diagnosis and immediate management?”
Kanavel Four Signs - STEP
- Swelling fusiform (sausage-shaped entire digit)
- Tenderness along flexor tendon sheath
- Extension passive causes severe pain
- Posture flexed (semiflexion 20-30°)
- All four signs = surgical emergency drainage within 24h
- Beyond 72h: tendon necrosis risk dramatically increased
Anatomical Space Boundaries
- Thenar: Radial to midpalmar septum (from 3rd MC)
- Midpalmar: Ulnar to septum, most common infection
- Hypothenar: Over hypothenar muscles, least common
- Parona: Distal forearm quadrilateral space
- Midpalmar septum: From 3rd metacarpal to palmar fascia
- Loss of palmar concavity = midpalmar infection
Surgical Drainage Indications
- All four Kanavel signs present (urgent)
- Presentation greater than 48 hours (urgent)
- Failed 12-24h antibiotic trial (urgent)
- Fluctuant abscess on examination
- Systemic toxicity or sepsis (emergent)
- Necrotizing fasciitis suspected (emergent within 6h)
Empiric Antibiotics
- Community-acquired: Cefazolin 2g IV q8h
- MRSA risk: Vancomycin 15-20mg/kg IV q8-12h
- Human bite: Ampicillin-sulbactam 3g IV q6h
- Cat/dog bite: Ampicillin-sulbactam (Pasteurella)
- Diabetic/polymicrobial: Vancomycin + pip-tazo
- Narrow based on cultures at 48-72h
Flexor Tenosynovitis Surgery
- Closed irrigation: Early (less than 48h), 8Fr catheter A5 to A1
- Open drainage: Delayed, Bruner incision, window A2/A4
- Preserve A2 and A4 pulleys (critical for function)
- Early AROM at 3-5 days prevents adhesions
- Tendon blood supply from vinculae - pressure causes necrosis
- Expected: 90-95% salvage if early, 70-80% if delayed
Deep Space Drainage Approaches
- Thenar: Dorsal first web (avoid palmar structures)
- Midpalmar: Volar incision ulnar ring ray OR dorsal
- Hypothenar: Volar over hypothenar eminence
- Parona/horseshoe: Requires THREE incisions (thumb, small, forearm)
- All spaces: Penrose drain, leave open/loose closure
- Elevation and early motion critical postoperatively
Horseshoe Abscess
- Radial bursa (thumb FPL) + ulnar bursa (small finger) + Parona space
- Requires drainage all THREE sites or fails
- Parona space: Forearm incision between FPL and FDS/FDP
- High morbidity: stiffness 50-70%, prolonged recovery
- Multiple debridements often required
- Amputation risk 5-10% despite treatment
Necrotizing Fasciitis
- Pain out of proportion, rapid progression, systemic toxicity
- Bullae, ecchymosis, crepitus, decreased sensation
- LRINEC score greater than 6: high risk
- Emergent debridement within 6 hours (mortality 20-30%)
- Antibiotics: Vancomycin + pip-tazo + clindamycin
- Serial debridements q24-48h, ICU admission, may need amputation