Degenerative | Mucous Cyst | Heberden's Node | Joint Destruction
- Heberden's nodes are osteophytes at DIP joint - pathognomonic for OA
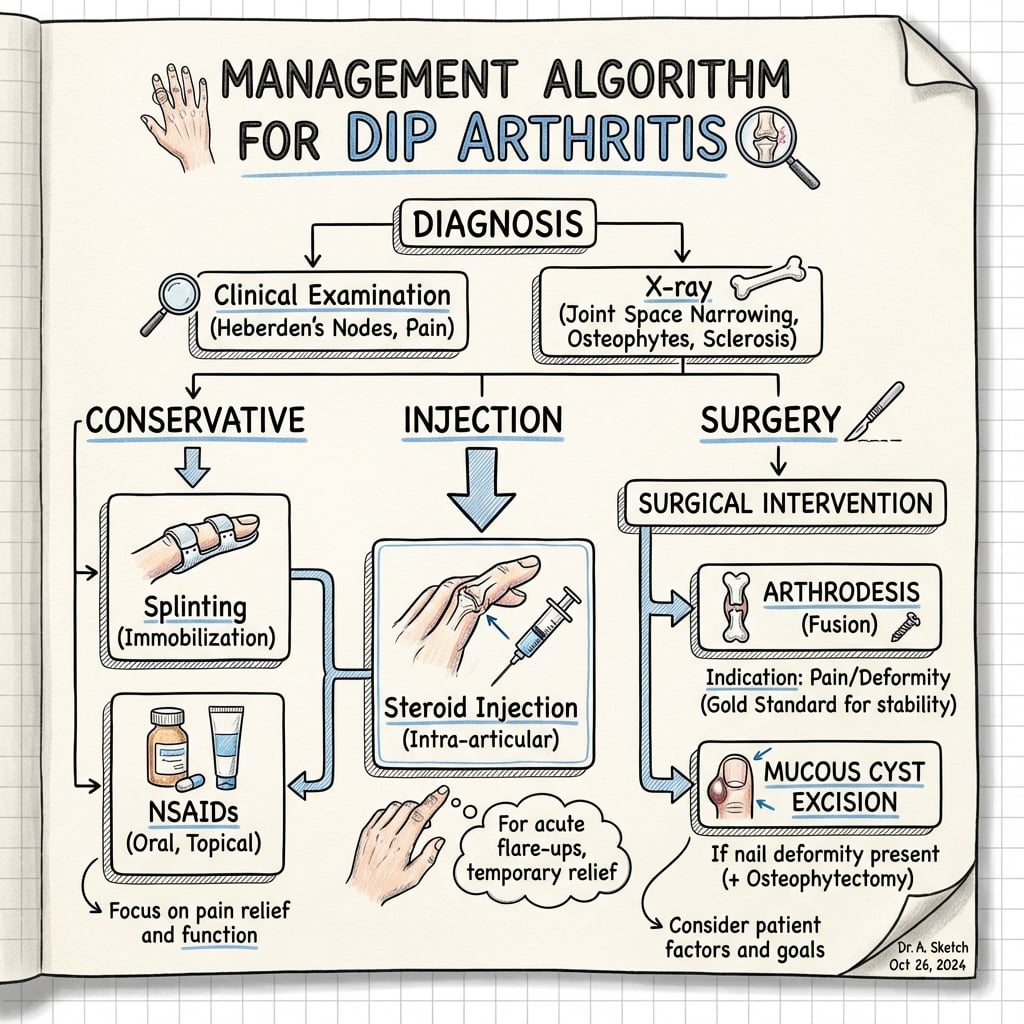
- Mucous cyst communicates with DIP joint in nearly all cases
- Arthrodesis is gold standard for painful end-stage DIP OA
- Nail deformity from mucous cyst pressure requires cyst excision + osteophytectomy
- Pin fixation for 6 weeks post-fusion is standard
- “Terminal tendon divides into lateral bands inserting on base of distal phalanx
- “Mucous cyst excision must include osteophyte debridement
- “Silicone arthroplasty is a niche motion-preserving option for low-demand patients; fusion is default
- “Fusion position: 10-20 degrees flexion for index, 30-40 for ring/small
Characteristic of OA at the DIP. Its counterpart, the Bouchard's node, is the same osteoarthritic osteophyte at the PIP (also OA - NOT rheumatoid). Rheumatoid arthritis, by contrast, characteristically spares the DIP.
Always check for nail deformity. The cyst communicates with the joint.
Index 10-20° (Pinch), Small 30-40° (Grip). Incorrect angle causes functional loss.
Overview and Epidemiology
Distal Interphalangeal (DIP) Joint Arthritis is the most common form of hand arthritis, predominantly affecting elderly women. It is approximately 10 times more common than rheumatoid arthritis affecting the DIP joint. The condition manifests as Heberden's nodes - bony enlargements at the DIP joints that are pathognomonic for osteoarthritis.
Why DIP Arthritis Matters Clinically: DIP arthritis significantly impacts fine motor function and can cause nail deformities when associated with mucous cysts. While many patients manage conservatively, those requiring surgery benefit from highly successful arthrodesis with 90% fusion rates and excellent pain relief. Recognition of mucous cyst-joint communication is critical for surgical planning.
Demographics
- Age: Predominantly over 60 years.
- Gender: 70% female predominance.
- Occupation: Repetitive manual labor increases risk.
- Genetic: Familial clustering in 40-50% (Hereditary HOA).
Nodal Generalised Hand Osteoarthritis
DIP arthritis is rarely an isolated joint problem - the Heberden's nodes, the female-over-60 demographic and the familial clustering all point to a single unifying entity that the topic relies on but never names: nodal generalised osteoarthritis. The radiograph above (DIP osteophytes plus thumb-base arthritis) is the classic picture.
The phenotype. Nodal generalised OA is a distinct, strongly heritable, female-predominant polyarticular form of OA whose target joints are the DIPs, the PIPs and the thumb base (first CMC). It is defined clinically by its nodes:
- Joint
- DIP
- What it is
- Dorsal/dorsolateral osteophyte - the hallmark of this topic
- Joint
- PIP
- What it is
- The same osteoarthritic osteophyte one joint more proximal (see pip-joint-arthritis)
- Joint
- First CMC (trapeziometacarpal)
- What it is
- Basal-joint OA - the third target joint (see thumb-cmc-arthritis)
Why it matters clinically:
- It is typically bilateral, symmetrical and polyarticular, with a strong family history (the 40-50% familial clustering noted above) - the pattern itself is diagnostic and usually needs no serology.
- When you see one painful Heberden's DIP, examine all the finger interphalangeal joints and the thumb base - you will usually find the wider nodal pattern, which both confirms primary OA and reframes the consultation (reassure the patient it is "wear-and-tear" nodal OA, not rheumatoid).
- It carries a better long-term prognosis than the aggressive erosive subset and is managed the same way joint-by-joint.
Treat a Heberden's DIP as the visible tip of nodal generalised OA - examine the PIPs (Bouchard's) and the thumb base (squaring) as well. The bilateral, symmetrical, polyarticular nodal pattern with a positive family history is itself the diagnosis of primary hand OA and removes any need for inflammatory serology.
Pathophysiology
Anatomy and Biomechanics
- Joint Type: Ginglymus (hinge joint). Range of motion 0-80 degrees.
- Articular Surface: Bicondylar head of middle phalanx (P2) articulates with biconcave base of distal phalanx (P3).
- Capsule: Thin dorsal capsule, thicker volar plate which prevents hyperextension.
- Relationship to Nail Matrix: The germinal matrix of the nail fold extends proximally to within 1-2 mm of the insertion of the extensor tendon. This close proximity explains why dorsal osteophytes compress the matrix, causing nail deformities.
Tendons:
- Terminal Extensor: Formed by the convergence of lateral bands. Inserts on the dorsal lip of P3.
- Flexor Digitorum Profundus (FDP): Inserts on the volar base of P3.
Biomechanical Stability: Unlike the PIP joint, the DIP joint has relatively short collateral ligaments. Stability is provided significantly by the articular conformity ("Cup and Cone" geometry). Loss of cartilage leads to instability, often manifesting as radial or ulnar deviation. Because the DIP joint is the terminal link in the kinematic chain, its stability is crucial for precision pinch (index finger) and power grip locking (ulnar digits).
Pathogenesis
The pathophysiologic cascade begins with cartilage degradation from mechanical stress and aging. Chondrocyte apoptosis leads to matrix metalloproteinase release, causing progressive cartilage loss. Subchondral bone responds with sclerosis and osteophyte formation - the hallmark Heberden's nodes.
Formation of Mucous Cyst: Degeneration leads to osteophyte formation at the joint margin. This osteophyte can pierce the joint capsule, allowing synovial fluid to herniate dorsally. This herniated sac becomes encapsulated, forming a Mucous Cyst (Ganglion). The cyst sits between the extensor tendon and the nail matrix, causing nail grooving via direct pressure (longitudinal groove). The connection with the joint is often a tortuous stalk, acting as a one-way valve where fluid enters the cyst but cannot return to the joint, leading to cyst enlargement.
- Mechanism
- Age-related cartilage degeneration
- Features
- Multiple digits, symmetric
- Mechanism
- Intra-articular fracture
- Features
- Single digit, history of trauma
- Mechanism
- Inflammatory cascade
- Features
- Rapid progression, 'Seagull' sign
Classification
Radiographic Grading of DIP OA
A simple descriptive radiographic grade (akin to a Kellgren-Lawrence reading) guides treatment.
- Radiographic Features
- Joint space narrowing, no osteophytes
- Management
- Conservative (Splint/NSAID)
- Radiographic Features
- Osteophytes present, sclerosis
- Management
- Injection / Procedure
- Radiographic Features
- Bone-on-bone, deformity, cysts
- Management
- Arthrodesis
Utility: This descriptive grade correlates well with symptoms.
Eponym caution: the Eaton (Eaton-Littler / Eaton-Glickel) classification is the staging system for thumb carpometacarpal (basal joint) OA, not the DIP - see
thumb-cmc-arthritis. It is sometimes loosely (and incorrectly) applied to finger interphalangeal OA; for the DIP, use a plain descriptive radiographic grade as above.
Clinical Presentation
History
- Pain: Worse with activity (pinch), relieved by rest.
- Stiffness: Short duration (under 30 mins) morning stiffness.
- Deformity: "Knobby fingers" (Heberden's).
- Function: Difficulty with fine motor tasks (buttons, needles).
Examination
- Heberden's Nodes: Bony hard swellings at dorsolateral joint margin.
- Mucous Cyst: Translucent, fluid-filled mass dorsally (often between nail fold and joint).
- Nail Deformity: Longitudinal groove/ridge denotes cyst pressure on matrix.
- ROM: Crepitus, loss of flexion.
- Deviation: Often radially deviated or flexed.
Investigations
Imaging
Plain Radiographs are the gold standard.
- Views: PA, Lateral, Oblique.
- Findings:
- Joint space narrowing.
- Subchondral Sclerosis.
- Osteophytes (Heberden's).
- Subchondral Cysts.
- Alignment (Deviation).
No Need for MRI: Plain X-rays are sufficient for diagnosis and surgical planning. MRI is only indicated if tumor or infection is suspected (rare).


Differential Diagnosis
- Key Differentiators
- Heberden's nodes, no systemic symptoms
- Imaging Features
- Osteophytes, Sclerosis, Normal density
- Key Differentiators
- Nail pits, rash, dactylitis (sausage digit)
- Imaging Features
- "Pencil-in-cup", Periostitis, Osteolysis
- Key Differentiators
- Acute flare, Tophi (white chalky deposit)
- Imaging Features
- Punched out erosions with overhanging edges
- Key Differentiators
- Spares DIP (usually), symmetric MCP/PIP
- Imaging Features
- Juxta-articular osteopenia, erosions
Note: Systemic review is mandatory.
Why Rheumatoid Arthritis Spares the DIP
The differential and the mnemonics repeatedly assert that "RA spares the DIP", but never explain why - and that explanation is itself a classic exam question.
The reason is synovium. Rheumatoid arthritis is a synovial disease: the inflammatory pannus arises in synovium-rich joints and tenosynovial sheaths. The joints with the most synovium - the MCPs, PIPs, wrists, and the ulnar styloid/DRUJ - are therefore its targets. The DIP joint has relatively little synovium and is characteristically spared by RA. The corollary is the high-yield rule:
- Think
- Osteoarthritis (Heberden)
- Clue
- Osteophytes, no systemic features
- Think
- Psoriatic arthritis
- Clue
- The one inflammatory arthritis that DOES attack the DIP ('pencil-in-cup')
- Think
- Rheumatoid arthritis
- Clue
- DIP involvement argues AGAINST RA
Two caveats worth stating:
- Psoriatic arthritis is the exception - it characteristically targets the DIP (with adjacent nail disease), which is why the topic flags it as the key inflammatory mimic of DIP OA.
- Coexisting OA confuses the picture: elderly rheumatoid patients very commonly also have nodal OA Heberden's nodes, so finding DIP osteophytes in a known RA patient usually reflects concomitant OA rather than RA attacking the DIP.
RA is a synovial disease that targets synovium-rich joints (MCP, PIP, wrist) and spares the synovium-poor DIP. So a DIP-dominant arthritis means osteoarthritis (bony Heberden's nodes) or psoriatic arthritis (the one inflammatory disease that loves the DIP, with nail changes) - not rheumatoid.
Management
CYSTMucous Cyst Management
Hook:CYST excision needs osteophyte (Spur) removal
Surgical Technique
Step-by-Step: DIP Arthrodesis
Precise technique is required to prevent non-union.
1. Exposure
- Incision: H-shaped or T-shaped incision is best. The transverse limb should be distal to the DIP crease to allow good skin retraction.
- Tendon: Tenotomy of the terminal extensor tendon. It can be split longitudinally or transected (since it will be fused).
- Collaterals: Release collateral ligaments to allow full access.
2. Joint Preparation (The 'Cup and Cone')
- Principles: Maximize bone contact surface area.
- Distal Phalanx (Cup): Use a small high-speed burr or correct sized reamer to create a concave surface.
- Middle Phalanx (Cone): Shape the head of P2 into a convex cone.
- Fit: The two surfaces should lock together ("Morse Taper" effect) at the desired angle.
3. Fixation
- Headless Compression Screw:
- Insert guide wire retrograde through P3 to the tip.
- Reduce joint at desired angle.
- Drive guide wire antegrade into P2 isthmus.
- Measure and insert screw (e.g. Acutrak Mini or Micro).
- Pros: Compression, no external metalwork.
- Cons: Cost, difficult hardware removal.
- K-Wires:
- Use two 0.045 inch wires (parallel or crossed).
- Crossed wires provide better rotational control.
- Pros: Cheap, easy to remove in clinic.
- Cons: Pin tract infection risk, lack of compression.
4. Closure
- Check alignment under fluoroscopy.
- Repair tendon (optional).
- 5-0 Nylon for skin.
- Protective splint.
Video: Confirm reduction on screen.
FLIPFusion Position by Finger
Hook:FLIP your finger position
Post-Operative Rehabilitation Protocol
Phase 1: Protection (0-6 Weeks)
- Goals: Protect fusion, wound healing.
- Immobilization: Pin-protecting splint (Stax or Thermoplastic).
- Activity: Keep dry. Gentle motion of PIP joint (isolation exercises).
- Follow-up: X-ray at 6 weeks. If union visible and K-wires present, remove wires.
Phase 2: Remobilization (6-12 Weeks)
- Goals: Desensitize tip, restore function.
- Activity: Begin using finger for light pinch.
- Therapy: Scar desensitization massage. Coban wrapping for edema control.
Phase 3: Strengthening (3 months+)
- Goals: Return to full unprotected use.
- Activity: Full manual labor allowed once radiographic union is solid.
Patient Education and Expectations
Managing patient expectations is critical for satisfaction.
What to Expect After Surgery
- Pain: Severe pain usually subsides within 3-4 days. Pivot to simple analgesia (Paracetamol) early.
- Swelling: The finger will remain swollen for 3-6 months. This is normal.
- Stiffness: The PIP joint may become stiff from disuse. Early motion of the PIP is mandatory.
- Hardware: If K-wires are used, they may protrude. Keep them clean and dry. Infection requires immediate removal.
Long Term Outcomes
- Fusion: Once fused, the pain is gone. The finger will not bend at the tip.
- Function: Most patients (90%) are very satisfied and would have the surgery again. Grip strength improves because the pain is gone.
- Complications: There is a small risk (5-10%) that the bone does not knit (Non-union). This may require a second surgery.
Disclaimer: Recovery timelines vary by patient comorbidity and compliance.
Complications
- Incidence
- 5-10%
- Management
- Revision fusion vs Accept (fibrous union)
- Incidence
- 1-2%
- Management
- Antibiotics / Pin removal
- Incidence
- 5%
- Management
- Nail plate removal / Matrix repair
- Incidence
- Rare
- Management
- Corrective osteotomy
- Incidence
- 5-30%
- Management
- Re-excision + Osteophytectomy
Recurrence Risk: Mucous cyst recurrence is almost exclusively due to failure to remove the osteophyte. The osteophyte acts as a "can opener" on the capsule. It must be debrided down to the shaft level.
Intraoperative Troubleshooting
- Bone too soft: Augment with K-wires if screw threads strip.
- Nail bed injury: Repair germinal matrix with 6-0 absorbable suture immediately to prevent nail ridge.
- Malrotation: Check finger cascade in flexion before final fixation. Clinical check is better than X-ray for rotation.
Guidelines, Registries & Global Practice
Global Epidemiology
- Hand OA is among the most prevalent forms of OA worldwide; the DIP joint is the single most commonly affected hand joint.
- Strong female predominance and a steep rise after the sixth decade are consistent across population cohorts (e.g. Framingham, Rotterdam).
- Familial clustering is well recognised, supporting a heritable component to nodal hand OA.
Guidance Compared
- Position relevant to DIP OA
- First-line non-pharmacological care plus topical NSAIDs; intra-articular corticosteroid as adjunct; surgery for refractory disease
- Position relevant to DIP OA
- Core treatment is education, exercise and topical NSAIDs; oral NSAIDs at lowest effective dose; reserve referral for persistent functional limitation
- Position relevant to DIP OA
- Topical NSAIDs preferred over oral for hand OA; chondroitin may relieve symptoms; routine imaging not required for diagnosis
- Position relevant to DIP OA
- Arthrodesis is the reference operation for end-stage painful DIP OA; fixation choice (screw vs wire) at surgeon discretion
Registry & Practice Variation
- There is no dedicated implant registry for DIP arthroplasty (low volumes, predominantly fusion), so outcome data come from case series and systematic reviews rather than registry survivorship.
- High-resource settings: greater use of headless compression screws and hand-therapy-led rehabilitation.
- Limited-resource settings: K-wire fixation predominates due to cost and ease of clinic removal; topical/oral analgesia and splinting carry most of the non-operative burden where injectables or therapy access is limited.
Controversies & Areas of Uncertainty
- Fusion vs arthroplasty: Fusion is the long-standing default, but pooled arthroplasty data report high satisfaction (~98%) with ~7% reoperation. There is no high-quality randomised comparison, so the choice remains driven by demand, digit and patient preference rather than evidence hierarchy.
- Optimal fixation: Headless compression screws give compression and avoid exposed metalwork, but carry a small risk of iatrogenic phalangeal fracture from screw-to-bone size mismatch; K-wires remain cheap and removable but expose the patient to pin-tract infection. No single construct is proven superior across all digits.
- Acceptance of fibrous nonunion: A substantial proportion of radiographic nonunions are pain-free (Stern, more than half). Whether to revise an asymptomatic stable fibrous union is debated; many surgeons observe rather than reoperate.
- Mucous cyst technique: Whether routine skin excision and flap coverage are needed, or whether simple decompression with osteophyte removal suffices, varies between units. The consensus point is that osteophyte removal is the recurrence-determining step.
- Emerging options: Bioabsorbable (e.g. magnesium) implants that obviate removal, and pyrocarbon/surface replacements, are early-stage with no durable comparative data. Regenerative injections (BMAC, PRP) for early disease remain Level IV/V and unproven.
At a Glance
DIP joint arthritis is the most common site of primary osteoarthritis in the hand, affecting 70% of women over 60. Characterized by Heberden's nodes (dorsal osteophytes), it typically presents with pain, stiffness, and deformity. Mucous cysts arise from the joint and can cause nail deformity. Treatment is primarily conservative (90% respond to NSAIDs and splinting), with DIP arthrodesis reserved for refractory cases. Key decision: fuse in functional position (index 10-20° for pinch, small finger 30-40° for grip).
Key Facts
- Severity
- Grade I-II
- Treatment
- NSAIDs + splinting
- Key Pearl
- 90% respond to conservative management
- Severity
- Grade II-III
- Treatment
- Procedures
- Key Pearl
- Corticosteroid injection (3-6 mo relief)
- Severity
- Grade III
- Treatment
- DIP arthrodesis
- Key Pearl
- 90% fusion rate, excellent pain relief
- Severity
- Any grade
- Treatment
- Cyst excision + Osteophytectomy
- Key Pearl
- Must remove spur to prevent recurrence
HEBERDENDIP Arthritis Features
Hook:HEBERDEN nodes are the hallmark of DIP arthritis
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 68-year-old lady presents with a painful, deformed index finger DIP joint. X-rays show bone-on-bone arthritis. She asks about 'joint replacement' so she can keep moving it suitable.”
“A 50-year-old female presents with a burst mucous cyst on her middle finger. The area is red and discharging.”
“A manual labourer underwent DIP arthrodesis with crossed K-wires 4 months ago. He has mild discomfort and the radiograph shows persistent lucency across the fusion site without hardware failure.”
Key Concepts
- **Heberden Node**: Osteophyte at DIP
- **Bouchard Node**: Osteophyte at PIP (Also in OA)
- **Mucous Cyst**: Ganglion + OA (Connects to joint)
Radiographic Grade
- **Grade I**: Narrowing
- **Grade II**: Osteophytes
- **Grade III**: Deformity
- *(Eaton staging = thumb CMC, not DIP)*
Fusion Angles
- **Index**: 0-10 degrees
- **Middle**: 20 degrees
- **Ring/Small**: 30-40 degrees
Evidence Base
DIP/IP Arthrodesis: Complication Analysis
- 139 patients, 181 arthrodeses (144 finger DIP, 37 thumb IP)
- 21 nonunions (~12%); crossed K-wires, interfragmentary wire and Herbert screw had similar nonunion rates
- 13 of 21 nonunions were pain-free; major complications (nonunion/malunion/deep infection/osteomyelitis) in 20%
- Inadequate bone stock/resection, premature pin removal and infection predisposed to nonunion
Silicone Interpositional Arthroplasty of the DIP Joint
- Review of 38 digits, mean age 58 years, implants in situ a mean of 10 years
- Less than 10% of implants required removal over the follow-up period
- Mean retained DIP motion of 33 degrees with preserved stability
- Concluded arthroplasty relieves degenerative pain while retaining motion versus arthrodesis
Mucous Cyst Excision With Joint Debridement and Flap Coverage
- Prospective cohort of 35 patients with 37 digital mucous cysts
- Cyst excision plus joint debridement, capsulectomy and osteophyte removal; defect closed with local flap
- Only 1 of 37 cysts recurred at mean 4-year follow-up; preoperative nail ridging resolved in 7 of 9 digits
- Satisfaction improved (4.3 to 6.8) and pain fell (4.7 to 2.3) with no flap necrosis or joint stiffness
References
- Stern PJ, Fulton DB. Distal interphalangeal joint arthrodesis: an analysis of complications. J Hand Surg Am. 1992;17(6):1139-45. PMID: 1430956.
- Wilgis EF. Distal interphalangeal joint silicone interpositional arthroplasty of the hand. Clin Orthop Relat Res. 1997;(342):38-41. PMID: 9308522.
- Hojo J, Omokawa S, Shigematsu K, et al. Patient-based outcomes following surgical debridement and flap coverage of digital mucous cysts. J Plast Surg Hand Surg. 2016;50(2):111-4. PMID: 26541935.
- Ingoe HMA, O'Hare JF, Middleton A. A functional angle of up to 35 degrees at the distal interphalangeal joint can be achieved with headless compression screw fusion. J Hand Surg Asian Pac Vol. 2018;23(3):377-381. PMID: 30282554.
- Xu J, Gilpin B, McCarron L, et al. Distal interphalangeal joint arthroplasty - a systematic review. J Hand Surg Asian Pac Vol. 2023;28(3):409-414. PMID: 37501548.
- Fan Z, Chang L, Su X, et al. Treatment of mucous cyst of the distal interphalangeal joint with osteophyte excision and joint debridement. Front Surg. 2022;8:767098. PMID: 35145989.