Pyogenic Infection of the Flexor Sheath
- Definition: Acute pyogenic infection of the flexor tendon sheath
- Definition: A surgical emergency because the closed space increases pressure, leading to tendon ischaemia and necrosis
- Mechanism: Bacterial proliferation within the synovial sheath → Increased pressure → Disruption of vincula blood supply → Tendon necrosis + Rupture
- Management: Early (less than 24-48h): IV Antibiotics + Elevation (Michon I)
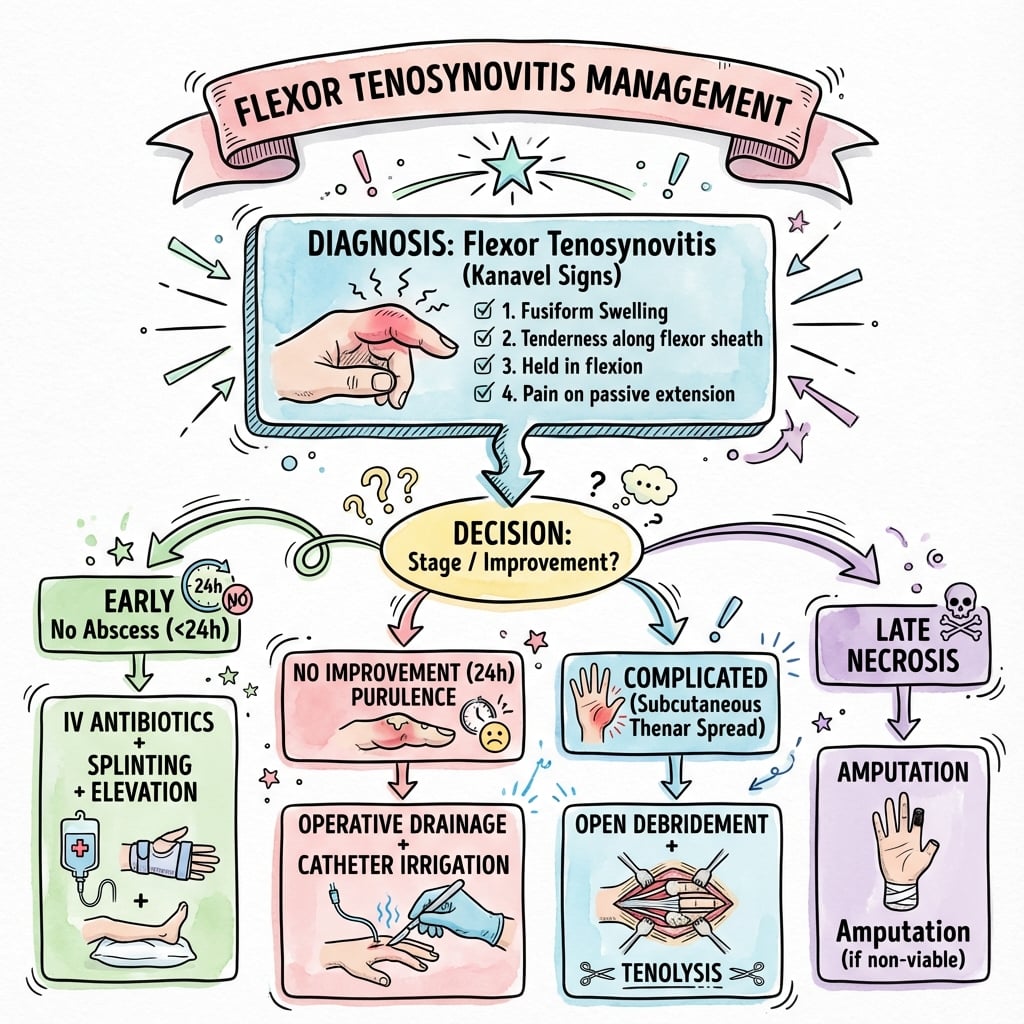
- “Clinical diagnosis! Kanavel's signs (Fusiform swelling, Flexed posture, Percussion tenderness, Pain on passive extension - most specific)
- “US can confirm fluid
- “Good if treated early
- “Delay leads to tendon necrosis, rupture, stiffness, and amputation
Flexor Tenosynovitis
Pain on passive extension is the most specific Kanavel sign. It stretches the inflamed sheath directly. Fusiform swelling is the most sensitive (earliest) sign.
Thumb and Little Finger sheaths extend into the wrist (Radial and Ulnar bursae). Infection can spread between them via the Space of Parona (deep forearm space), creating a "Horseshoe Abscess".
Index, Middle, and Ring finger sheaths typically terminate distally at the DIPJ and proximally at the A1 pulley (distal palmar crease). They do NOT extend into the wrist.
F-F-T-PKanavel's Cardinal Signs
Hook:Flexor Finger Tendon Pain
A-D-S-I-PPang Poor-Prognosis Factors
Hook:A Diabetic Sheath Is Poor
B-W-S-GExposure-Specific Organisms
Hook:Bites, Water, Soil, Gonorrhoea
Overview & Epidemiology
Pyogenic flexor tenosynovitis (PFT) is an acute bacterial infection within the closed synovial flexor tendon sheath of a digit. It is a surgical emergency: rising pressure in the confined sheath strangles the tendon's blood supply, causing ischaemia, necrosis, adhesions and, in severe cases, amputation.
- Frequency: roughly 2.5-9.4% of all hand infections across published series.
- Demographics: predominantly working-age adults; reflects the dominant penetrating-trauma mechanism. In children it is rarer and Kanavel signs are less reliable.
- Commonest organism: Staphylococcus aureus, with community-acquired MRSA now a major pathogen; organism varies with exposure (see Investigations & Microbiology).
- Prognosis: excellent with treatment inside 24 h and no purulence/ischaemia; amputation rates rise to around 59% once both subcutaneous purulence and digital ischaemia are present (Pang classification).
Sheath Anatomy
- Index, Middle, Ring: Sheath ends at A1 pulley (distal palmar crease level) proximally, and DIPJ distally.
- Thumb: Sheath continues into Radial Bursa (wrist).
- Little: Sheath continues into Ulnar Bursa (wrist).
- The Radial and Ulnar bursae communicate in 50-80% of people via the Space of Parona (deep to flexor tendons in distal forearm).
- Allows spread from Thumb to Little finger (or vice versa) = Horseshoe Abscess.
- Vincula (short and long) enter dorsally.
- High pressure in the sheath tamponades these vessels → Necrosis.
Pathophysiology
The flexor tendon sheath is a closed synovial space with two layers: an outer fibro-osseous tunnel (the annular A1-A5 and cruciate C1-C3 pulleys) and an inner synovial bilaminar sleeve (parietal and visceral) that lubricates and nourishes the FDS and FDP tendons. Infection within this confined space behaves like a compartment syndrome of the digit: as bacteria proliferate, intrasheath pressure rises, and once pressure exceeds the perfusion pressure of the vincular vessels the tendon becomes ischaemic, then necrotic. This is why PFT is a true surgical emergency rather than a simple soft-tissue infection.
Routes of inoculation (in descending frequency): penetrating trauma to the volar aspect of the digit (most common), bites, and haematogenous seeding (classically Neisseria gonorrhoeae in a sexually active patient with no penetrating injury). The most frequent organism overall is Staphylococcus aureus; community-acquired MRSA is now a major pathogen, and polymicrobial or atypical organisms follow specific exposures (soil/plant, water, bite).
Investigations & Microbiology
PFT is fundamentally a clinical diagnosis; investigations support but never delay treatment.
Adjuncts (never delay surgery to obtain them): ultrasound or MRI can confirm fluid within the sheath in equivocal cases; inflammatory markers (WBC, CRP) help track systemic response; plain radiographs exclude radio-opaque foreign body, gas and osteomyelitis. Always send intra-operative fluid/tissue for Gram stain, aerobic and anaerobic culture, and (where exposure suggests) fungal and mycobacterial culture.
Empirical antibiotics (start immediately after taking cultures, then refine on sensitivities):
- Likely organism
- S. aureus (incl. CA-MRSA), Streptococcus
- Empirical cover
- Anti-staphylococcal agent; add MRSA cover (vancomycin or clindamycin) where CA-MRSA prevalent
- Likely organism
- Eikenella corrodens, anaerobes, oral flora
- Empirical cover
- Amoxicillin-clavulanate (or equivalent beta-lactam/beta-lactamase inhibitor)
- Likely organism
- Pasteurella multocida
- Empirical cover
- Amoxicillin-clavulanate
- Likely organism
- Mycobacterium marinum, Vibrio, Aeromonas
- Empirical cover
- Prolonged atypical cover; send for mycobacterial culture
- Likely organism
- Sporothrix schenckii (fungal), Pantoea agglomerans
- Empirical cover
- Antifungal if fungal confirmed; prolonged cultures
- Likely organism
- Neisseria gonorrhoeae
- Empirical cover
- Ceftriaxone; consider disseminated gonococcal infection

Classification
Clinical Presentation
PFT is a clinical diagnosis resting on Kanavel's four cardinal signs (see mnemonic above): fusiform "sausage" swelling of the whole digit, the finger held semi-flexed at rest, tenderness along the volar flexor sheath, and pain on passive extension (the most specific sign). Onset is typically 2-5 days after a penetrating volar injury, with progressive throbbing pain, swelling and erythema.
Caveat: the complete quartet is not always present, particularly early or in children (all four in only about a third of paediatric cases). A high index of suspicion and treatment on clinical grounds is essential — do not wait for the full picture.

Management
Prognostic Factors & Clinical Classification (Landmark)
- Retrospective study of 75 patients with pyogenic flexor tenosynovitis
- Five factors predicting poor outcome: age over 43, diabetes/PVD/renal failure, subcutaneous purulence, digital ischaemia, polymicrobial infection
- Three-tier classification: Group I (no purulence/ischaemia) 0% amputation, 80% return of total active motion
- Group II (subcutaneous purulence, no ischaemia) 8% amputation, 72% TAM
- Group III (purulence AND ischaemia) 59% amputation, only 49% TAM
Closed-Catheter Irrigation vs Open Drainage
- Retrospective comparison of 47 cases of pyogenic flexor tenosynovitis
- Open drainage in 32 patients, closed-catheter irrigation (CCI) in 15
- Complications more frequent with open drainage (n=9) than CCI (n=3), but difference not statistically significant
- CCI produced smaller wounds with less scarring
Continuous Irrigation with Local Anaesthetic & Early Motion
- Two-incision closed-sheath irrigation with a postoperative continuous bupivacaine (marcaine) pain pump in 9 patients (mean age 42.8 years)
- Mean hospital stay 2.8 days; no recurrent infections
- 7 of 9 patients regained full total active motion; the other two reached 125 and 105 degrees
- Improved analgesia enabled an early aggressive postoperative therapy protocol
Microbiology & Limits of Kanavel Signs (Paediatric)
- 32 children treated surgically for PFT over 14 years at a tertiary children's hospital
- All four Kanavel signs present in only 34%; at least three in 62%; flexed posturing least common (41%)
- Commonest organisms: MRSA 38%, MSSA 22%, Pasteurella multocida 13%; polymicrobial in 19%
- All MRSA isolates sensitive to vancomycin and trimethoprim-sulfamethoxazole; 83% to clindamycin
Evaluation & Treatment Controversies (Review)
- Narrative review of background, microbiology and treatment of PFT
- No standardised algorithm exists for the need, timing, or type of surgery
- Complication and amputation rates remain high despite prompt treatment
- Roles of local antibiotics and adjunctive corticosteroids remain unproven and need further study
Management Algorithm
Complications
Hand Infections Differential
Chronic Granulomatous Flexor Tenosynovitis (the Indolent Mimic)
Everything above describes acute pyogenic flexor tenosynovitis. A separate, easily missed entity is chronic granulomatous flexor tenosynovitis caused by slow-growing organisms — atypical mycobacteria (classically Mycobacterium marinum after water/fish exposure; also M. tuberculosis and M. kansasii) and fungi (Sporothrix schenckii, and regionally Histoplasma and Coccidioides). The same exposure organisms flagged in the microbiology table behave completely differently in the sheath, and recognising the pattern is a favourite exam discriminator.
How it differs from acute pyogenic disease:
- Acute pyogenic PFT
- Days after penetrating injury
- Chronic granulomatous tenosynovitis
- Insidious over weeks to months
- Acute pyogenic PFT
- Full or near-full quartet
- Chronic granulomatous tenosynovitis
- Usually absent/muted; boggy, doughy, relatively painless swelling
- Acute pyogenic PFT
- Marked; systemically unwell
- Chronic granulomatous tenosynovitis
- Minimal erythema; usually afebrile
- Acute pyogenic PFT
- Pus
- Chronic granulomatous tenosynovitis
- Thickened granulomatous synovium, often with rice bodies (fibrinous loose bodies — also seen in tuberculous and rheumatoid tenosynovitis)
- Acute pyogenic PFT
- Emergency decompression of a closed-space "compartment"
- Chronic granulomatous tenosynovitis
- Elective tenosynovectomy + prolonged organism-specific drugs
Diagnosis demands a high index of suspicion (it mimics a ganglion, sprain, or rheumatoid tenosynovitis). Send tissue for histology (granulomatous synovitis — caseating in TB, non-caseating with atypical mycobacteria) and prolonged culture: mycobacterial culture held for weeks, with M. marinum requiring lower incubation temperatures (around 30-32°C), and fungal cultures held similarly long. PCR speeds identification. MRI shows tenosynovial thickening and the rice bodies.
Management is not emergency irrigation. The cornerstone is open tenosynovectomy (debulking the granulomatous synovium) combined with prolonged organism-specific therapy — multidrug antimycobacterial treatment (for example clarithromycin with rifampicin/ethambutol for M. marinum, or standard antituberculous therapy for TB tenosynovitis, typically months) or appropriate antifungals. Surgery debulks; the medical therapy cures, and stopping early invites recurrence. The detailed antimicrobial regimens and systemic atypical-mycobacterial disease are developed in the dedicated atypical-mycobacterial-infection topic.
Mimics You Must NOT Incise
The differential table above lists the infective conditions that share the FT picture. Just as important for the exam (and for patient safety) are the mimics where incision and drainage is the wrong answer — taking one of these to theatre causes harm.
- Clue it is NOT pyogenic FT
- Clustered vesicles/vesicopustules on an erythematous base with a burning/itching prodrome; clear-to-honey vesicle fluid rather than tense purulent sheath distension; passive extension comparatively well tolerated; classic in healthcare/dental workers and thumb-sucking children
- Why surgery is wrong
- Self-limiting (resolves over 2-3 weeks); incision is unnecessary and risks bacterial superinfection and viral spread. Diagnose with Tzanck smear or viral PCR; manage supportively ± aciclovir
- Clue it is NOT pyogenic FT
- "Pseudo-septic" intense erythema and swelling but a history of crystal disease; radiograph may show a calcific deposit; aspirate yields crystals, not pus
- Why surgery is wrong
- Treat the crystal arthropathy (NSAIDs/colchicine, treat the calcific deposit); a washout adds morbidity without addressing the cause
Look for grouped vesicles rather than a uniformly tense, fusiform, pus-filled sheath. Pain on passive extension is muted compared with true PFT. Ask about HSV exposure, recent oral herpes, or occupational risk.
Herpetic whitlow is viral and self-limiting — incising it is unnecessary, can seed secondary bacterial infection, and historically was warned to risk systemic spread. The fuller disease course is covered in the dedicated herpetic-whitlow topic.
Guidelines, Registries & Global Practice
Global epidemiology. PFT accounts for roughly 2.5-9.4% of all hand infections depending on the series; most patients are working-age adults, reflecting the dominant penetrating-trauma mechanism. S. aureus (including community-acquired MRSA in many regions) is the leading pathogen worldwide, with exposure-specific organisms (Pasteurella after bites, atypical mycobacteria/Vibrio after water, gonococcus when no trauma).
Guidance, side by side. There is no single dedicated international society guideline for PFT; management is anchored in hand-surgery literature and general infection principles.
- Position on PFT
- Clinical diagnosis on Kanavel signs; prompt empirical IV antibiotics with MRSA cover; surgical decompression/irrigation for established disease; no standardised operative algorithm
- Position on PFT
- Urgent senior assessment, early antibiotics, theatre for source control; specialist hand unit involvement
- Position on PFT
- Source control is paramount: decompress the closed space early to prevent tendon ischaemia
- Position on PFT
- Empirical regimens stratified by exposure (bite, water, MRSA risk); culture-directed de-escalation
Registry note. No arthroplasty/implant registry applies to PFT; it is a soft-tissue infection, so "registry evidence" is replaced here by published institutional case series (Pang N=75; Gutowski N=47; Brusalis N=32).
High- vs limited-resource practice variation. Where ultrasound/MRI and 24-h theatre access exist, equivocal cases are confirmed on imaging and drained promptly, favouring digit salvage. In limited-resource settings, delayed presentation, restricted theatre access and lack of MRSA-active or atypical-organism cover increase the rate of Michon III disease, tendon necrosis and amputation, mirroring the poor-prognosis groups described by Pang.
Controversies & Areas of Uncertainty
There is no consensus treatment algorithm for PFT; the following questions are genuinely unresolved and are favourite examiner territory.
- Antibiotics alone vs early surgery. Truly early disease (within roughly 24-48 h, serous Michon I, no purulence) may settle with IV antibiotics, elevation and splinting, with surgery reserved for failure to improve at 24 h. Once purulence or full Kanavel signs are established, antibiotics alone are inadequate. The threshold for non-operative management is not standardised.
- Closed-catheter irrigation vs open drainage. No randomised trial exists. Comparative data (Gutowski) show no significant outcome difference; closed irrigation causes less scarring but risks under-drainage if flow is poor. Stage III or loculated infection mandates open debridement.
- Continuous postoperative irrigation vs single intraoperative washout. Leaving an indwelling irrigation catheter is common practice but unproven; some series report equivalent results with a single thorough intraoperative washout, avoiding catheter-related morbidity.
- Adjuncts. The roles of intrasheath/local antibiotics and adjunctive corticosteroids (to reduce adhesion and stiffness) remain experimental and are not recommended outside study settings.
- Duration and route of antibiotics. Optimal IV duration before oral switch and total course length are not defined; practice ranges widely (often IV for 48-72 h then oral to complete around 10-14 days), guided by clinical response and cultures.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 40-year-old gardener presents with a painful, swollen index finger 2 days after pricking it on a rose thorn. The finger is uniformly swollen and held in flexion. Attempting to straighten it causes severe pain. How do you manage this?”
“A 32-year-old presents to the emergency department with a 3-day history of progressive pain and swelling in the little finger following a needle-stick injury at work. On examination, the little finger demonstrates all four Kanavel signs. You also notice some tenderness and swelling in the distal palm and radial aspect of the wrist. The thumb appears normal. The patient is systemically well. How would you assess and manage this case?”
“A 58-year-old diabetic man presents 5 days after sustaining a puncture wound to his ring finger while working on his car. He initially ignored it but now has severe pain and swelling. Examination shows a dusky, tense ring finger with all four Kanavel signs. The finger feels cool and capillary refill is sluggish at 4 seconds. He has limited passive motion. He is febrile at 38.9 degrees with WBC 18,000. You take him urgently to theatre and find murky brownish fluid, necrotic-appearing synovium, and the flexor tendons appear grey and non-viable. What is your assessment and how do you proceed?”
Kanavel's Signs
- 1. Fusiform swelling
- 2. Flexed posture
- 3. Tenderness along sheath
- 4. Pain on passive extension (Key)
Anatomy
- Index/Middle/Ring: Ends at A1
- Thumb: Radial Bursa
- Little: Ulnar Bursa
- Connection: Space of Parona
Treatment
- Early: IV Abx + Elevation
- Established: Sheath Irrigation
- Late/Necrotic: Open Debridement
References
- Kanavel AB. Infections of the Hand. Lea & Febiger; 1912.
- Pang HN, Teoh LC, Yam AKT, et al. Factors affecting the prognosis of pyogenic flexor tenosynovitis. J Bone Joint Surg Am. 2007;89(8):1742-8. PMID 17671013.
- Gutowski KA, Ochoa O, Adams WP. Closed-catheter irrigation is as effective as open drainage for treatment of pyogenic flexor tenosynovitis. Ann Plast Surg. 2002;49(4):350-4. PMID 12370638.
- Gaston RG, Greenberg JA. Use of continuous marcaine irrigation in the management of suppurative flexor tenosynovitis. Tech Hand Up Extrem Surg. 2009;13(4):182-6. PMID 19956043.
- Brusalis CM, Thibaudeau S, Carrigan RB, et al. Clinical characteristics of pyogenic flexor tenosynovitis in pediatric patients. J Hand Surg Am. 2017;42(5):388.e1-388.e5. PMID 28341068.
- Chapman T, Ilyas AM. Pyogenic flexor tenosynovitis: evaluation and treatment strategies. J Hand Surg Am. 2019;44(11):981-985. PMID 31272698.