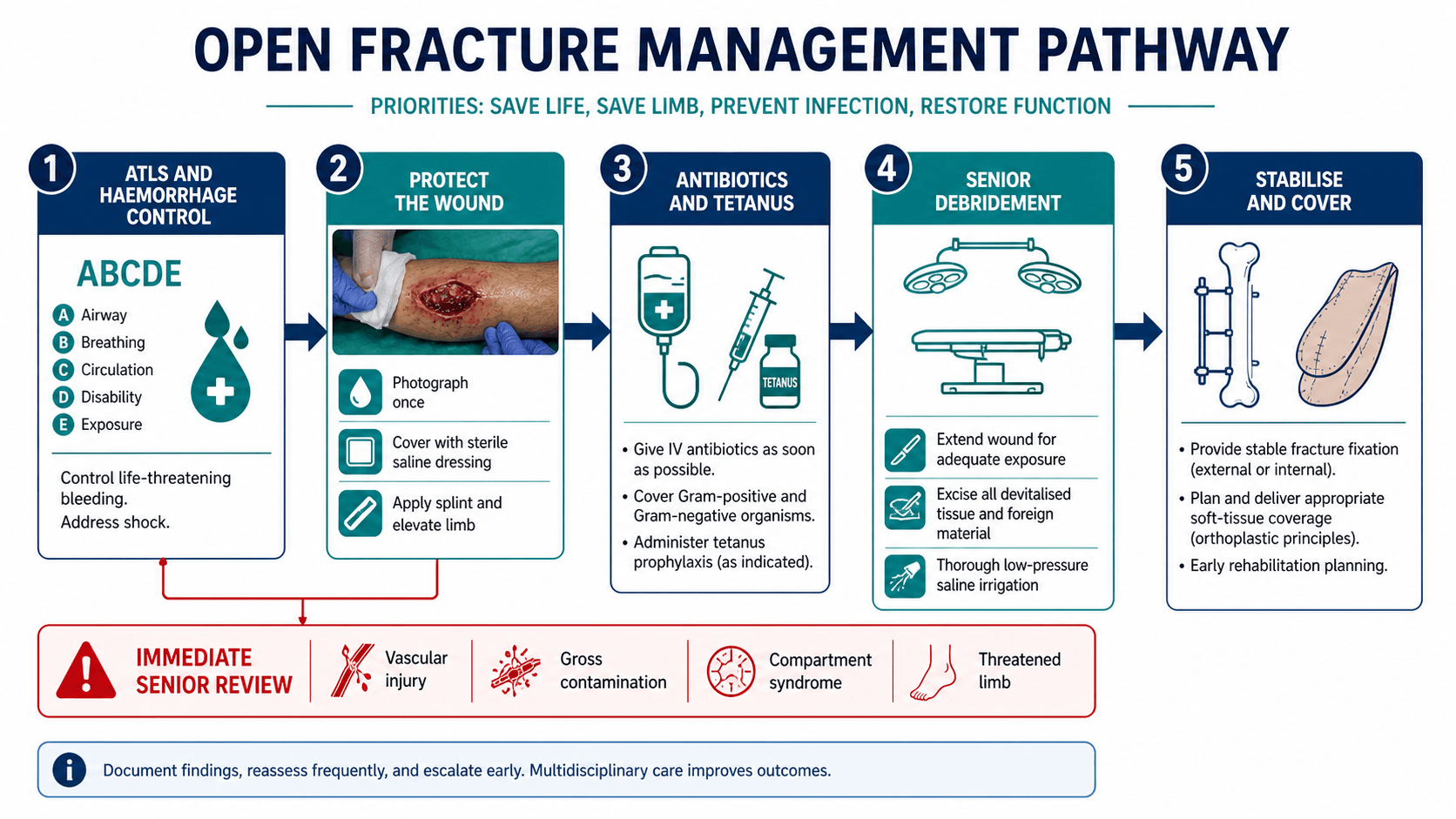
Save life, save limb, prevent infection, restore function
- An open fracture is any fracture that communicates with the outside environment through a skin or mucosal wound.
- The skin wound may be small; the zone of injury is defined by the energy transfer, contamination, vascularity and soft-tissue viability.
- Do not repeatedly inspect the wound in the emergency department. Photograph it once, cover it, splint the limb and move to senior-led care.
- Antibiotics and tetanus prophylaxis are emergency treatments; debridement and fixation are operative treatments.
- Type IIIB is a soft-tissue reconstruction problem as much as a fracture problem; fixation and flap planning must be coordinated.
- “Final Gustilo-Anderson grade is most reliable after operative debridement, not from the first emergency department photograph.
- “The old six-hour rule is not a substitute for senior decision-making. Vascular injury, gross contamination, compartment syndrome and threatened skin change the urgency.
- “High-pressure lavage can damage tissue; contemporary evidence supports low-pressure saline irrigation rather than aggressive pulsatile washing.
- “MESS and similar scores can support discussion, but they do not decide amputation alone.
Open Fracture Classification and Management
Open fracture care begins like major trauma care: save life first, then limb, then function. The common failure is to focus on the wound size and forget haemorrhage, ischaemia, contamination, compartment syndrome, devitalised tissue and the soft-tissue plan.
Overview/Epidemiology
An open fracture is a fracture that communicates with the external environment. The communication may be obvious, with exposed bone and soft-tissue loss, or subtle, with a small puncture wound created by a sharp fracture spike.
The important concept is not just "skin wound plus fracture". It is the zone of injury:
- devitalised skin and subcutaneous tissue
- crushed or contaminated muscle
- periosteal stripping
- exposed bone or implant
- vascular injury
- nerve injury
- compartment syndrome risk
- bacterial contamination
- systemic trauma physiology
The skin hole is often a poor marker of the real injury. A small inside-out wound from a low-energy tibial fracture behaves differently from a small high-velocity gunshot wound, farm injury or crush wound.
Open fractures occur across a broad trauma spectrum. In younger adults they often follow road trauma, falls from height, motorcycle injuries, industrial trauma, sport and ballistic injury. In older adults, low-energy falls can still create open fractures because skin and soft tissue are fragile. The tibia is the classic high-yield bone because the anteromedial border is subcutaneous and soft-tissue cover is limited.
Anatomy/Biomechanics
Open fractures matter because the surgeon is treating four linked problems:
- Contamination: bacteria and foreign material enter the wound at the time of injury.
- Devitalised tissue: dead muscle and bone become a culture medium and prevent healing.
- Instability: motion at the fracture increases pain, bleeding, soft-tissue damage and infection risk.
- Soft-tissue envelope failure: exposed bone, tendon, implant or dead space cannot reliably heal without durable cover.
The outcome is not determined by one step. Infection, nonunion, malunion, chronic osteomyelitis, flap failure, stiffness, chronic pain and amputation are reduced by the combined system: early antibiotics, careful debridement, stable fixation, vascularised coverage and rehabilitation.
Bone healing requires biology and stability. Open fractures damage both. Periosteal stripping, segmental bone loss and devitalised fragments reduce biology; comminution and soft-tissue disruption reduce the ability to obtain stable fixation without further injury. The fixation method must restore length, alignment and rotation while preserving blood supply and soft-tissue reconstruction options.
A puncture wound near a fracture is an open fracture until proven otherwise. If the wound is close to the fracture haematoma, treat it as open unless a senior clinician can confidently exclude communication.
Classification Systems
Classification should communicate severity and guide treatment, but it must not replace clinical judgement. The key systems are Gustilo-Anderson, OTA Open Fracture Classification and the underlying AO/OTA fracture pattern.
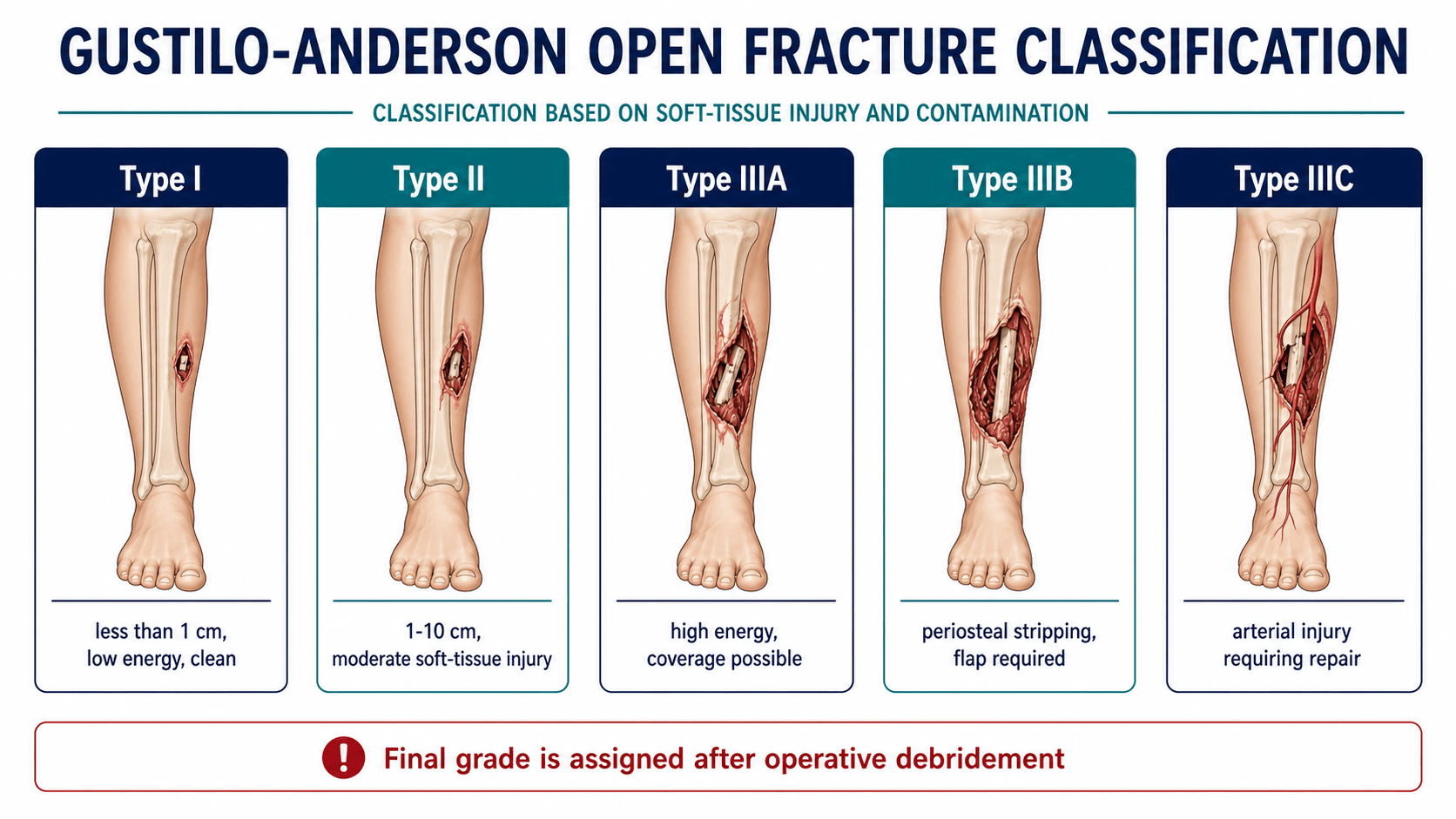
- Typical injury
- Small clean wound, low energy, simple fracture pattern
- Soft-tissue implication
- Minimal soft-tissue stripping
- Management implication
- Antibiotics, tetanus review, debridement and stable fixation
- Typical injury
- Larger wound without severe Type III features
- Soft-tissue implication
- Moderate soft-tissue injury
- Management implication
- Debridement and fixation; closure only if tissue is viable and tension-free
- Typical injury
- High-energy injury, segmental or comminuted pattern, but coverage possible
- Soft-tissue implication
- Soft tissue can cover bone after debridement
- Management implication
- Senior debridement, stable fixation and early closure or coverage
- Typical injury
- Extensive soft-tissue loss, periosteal stripping or exposed bone
- Soft-tissue implication
- Vascularised flap usually required
- Management implication
- Orthoplastic plan for fixation and flap; avoid fixation that compromises coverage
- Typical injury
- Arterial injury requiring repair
- Soft-tissue implication
- Limb survival depends on perfusion and global injury
- Management implication
- Urgent vascular strategy, temporary shunt or repair, fixation, fasciotomy when indicated and coverage
Gustilo-Anderson limitations
The system is useful but imperfect:
- interobserver reliability is only moderate
- the grade often changes after operative debridement
- wound size alone can mislead
- contamination, host factors and fracture biology are not fully captured
- Type IIIB includes a broad range of injuries
Gustilo classification: reliability
- Orthopaedic surgeons shown standardised wound images achieved only moderate interobserver agreement on Gustilo grade.
- The system is useful but limited, and studies based on it should be interpreted with caution.
- Photographic and operative reassessment improve, but do not eliminate, grading disagreement.
OTA Open Fracture Classification
The OTA system separates:
- skin injury
- muscle injury
- arterial injury
- contamination
- bone loss
This is more descriptive than a single Gustilo grade and can be useful for research and detailed handover. In clinical practice, the best approach is to document both: the AO/OTA fracture pattern plus an open-fracture soft-tissue assessment.
High-energy open fracture where viable soft tissue can cover bone after debridement. It is not simply any wound greater than 10 cm.
Clinical Assessment
The first assessment is structured, not wound-centred.
Primary survey
Use trauma principles:
- control life-threatening haemorrhage
- assess airway, breathing and circulation
- treat shock
- identify chest, abdominal, pelvic, head and spinal injuries
- document limb perfusion and neurology before and after manipulation
Limb assessment
Record:
- mechanism and contamination environment
- time of injury and time of antibiotics
- wound location, size and skin viability
- exposed bone, tendon, implant or joint
- deformity, compartment tension and pain pattern
- pulses, capillary refill, Doppler signals and limb temperature
- motor and sensory function of named nerves
- associated dislocation or joint involvement
- patient factors: diabetes, smoking, vascular disease, immunosuppression and frailty
Emergency department actions
Do these early:
- photograph the wound once for the record
- remove gross surface contamination only if it can be done without exploring the wound
- cover with sterile saline-moistened dressing
- apply a splint that restores length and protects soft tissue
- give analgesia
- start antibiotics according to local open-fracture protocol
- review tetanus status
- elevate the limb when safe
- escalate early to orthopaedic, plastic surgery, vascular surgery and anaesthesia teams when needed
Do not probe the wound repeatedly. Do not perform bedside "washouts" that give false reassurance. Definitive debridement requires anaesthesia, lighting, instruments, haemostasis and senior judgement.
Differential and discriminators
The "differential" in open fracture care is twofold: deciding whether a wound communicates with the fracture, and recognising the coexisting limb-threatening problems that change urgency.
- Suggestive features
- Any wound near the fracture haematoma, bleeding fat or fracture air on radiograph
- Why it changes management
- Treat as open until excluded; mandates antibiotics, tetanus and debridement
- Suggestive features
- Pain out of proportion, pain on passive stretch, tense compartments; an open wound does not decompress all compartments
- Why it changes management
- Requires urgent fasciotomy independent of the open wound
- Suggestive features
- Absent pulses, expanding haematoma, ischaemic or cool limb, abnormal ankle-brachial index
- Why it changes management
- Limb-threatening; needs urgent shunt or repair before or alongside fixation
- Suggestive features
- Warm ischaemia time prolonged, segmental muscle loss, insensate foot, gross contamination
- Why it changes management
- Triggers senior salvage-versus-amputation discussion
- Suggestive features
- Morel-Lavallee lesion, fluctuant skin, marginal viability over a closed fracture
- Why it changes management
- High infection and skin-necrosis risk even without a through-and-through wound
- Suggestive features
- Rapidly spreading erythema, crepitus, systemic toxicity after contaminated injury
- Why it changes management
- Surgical emergency needing radical debridement and broad antibiotics
Investigations
Plain radiographs
Obtain radiographs of the injured segment with the joint above and below. Look for:
- fracture location and pattern
- comminution and segmental bone loss
- intra-articular extension
- associated dislocation
- foreign bodies
- gas in soft tissues
- pre-existing implants or bone disease
CT
CT is useful when the fracture involves a joint, the pelvis, the hindfoot, the distal tibia, the distal femur, the acetabulum or complex periarticular anatomy. CT should not delay limb-saving vascular intervention.
Vascular imaging
Hard signs of vascular injury require urgent senior action. CT angiography is appropriate when the patient is stable and the diagnosis or operative plan requires vascular mapping.
Hard signs include:
- active haemorrhage
- expanding haematoma
- absent distal perfusion
- ischaemic limb
- bruit or thrill
Laboratory tests
Blood tests support operative planning and resuscitation:
- full blood count
- electrolytes and renal function
- coagulation profile
- group and screen or crossmatch
- lactate and base deficit in major trauma
- creatine kinase when crush or compartment syndrome is suspected
Do not swab the open wound in the emergency department to guide initial antibiotic choice. The organisms cultured later from fracture-related infection often differ from early surface contamination.
Management Algorithm
Open fracture management is best taught as a staged decision pathway.
ATLS assessment, haemorrhage control, neurovascular documentation, wound photograph, sterile dressing, splint, antibiotics and tetanus prophylaxis.
1. Immediate priorities
- resuscitate the patient
- control haemorrhage
- cover and splint the limb
- give antibiotics and tetanus prophylaxis
- assess neurovascular status
- identify threatened limb, compartment syndrome and gross contamination
2. Decide urgency
Immediate senior operative attention is required for:
- vascular compromise
- compartment syndrome
- uncontrolled bleeding
- gross contamination such as farm, sewage or aquatic exposure
- traumatic amputation or near-amputation
- severe crush injury
- threatened skin envelope
Other open fractures still require formal debridement, but the safest timing is the earliest appropriate time with the right team, equipment and theatre environment.
3. Plan the debridement
Plan:
- incision extensions before starting
- tourniquet strategy
- vascular control if needed
- plastic surgery involvement when coverage is likely
- fixation method
- whether fasciotomy is indicated
- whether bone loss needs staged reconstruction planning
4. Stabilise the skeleton
The fixation choice is driven by:
- fracture location and pattern
- contamination
- soft-tissue coverage requirement
- patient physiology
- vascular repair needs
- future flap access
- anticipated bone reconstruction
5. Achieve durable soft-tissue cover
Closure is not the same as cover. The goal is a viable, tension-free soft-tissue envelope that eliminates dead space and protects bone, tendon, joint and implants.
I would treat the patient first, start antibiotics early, photograph and cover the wound, document neurovascular status, splint the limb, then proceed to senior-led debridement, skeletal stabilisation and orthoplastic soft-tissue reconstruction based on the zone of injury.
Antibiotics and Tetanus
Antibiotics reduce infection risk and should be given as soon as possible after recognition of an open fracture. Do not wait for imaging, wound classification or theatre.
The exact regimen depends on local antimicrobial guidance, allergy status, renal function, contamination and resistance patterns. A practical framework is:
- Coverage principle
- Gram-positive cover is essential
- Practical note
- Many protocols use a first-generation cephalosporin or equivalent local regimen
- Coverage principle
- Broader cover including gram-negative organisms is commonly used
- Practical note
- Coordinate dosing and duration with local trauma, microbiology or infectious diseases protocol
- Coverage principle
- Add anaerobic and clostridial cover
- Practical note
- Requires more aggressive debridement and low threshold for repeat inspection
- Coverage principle
- Consider water-specific organisms
- Practical note
- Marine and freshwater injuries may require different antimicrobial cover
- Coverage principle
- Culture-guided treatment after adequate sampling
- Practical note
- Do not rely on superficial wound swabs
Tetanus status should be checked and prophylaxis given according to local immunisation guidance. Antibiotics are not a substitute for debridement.
Antibiotic prophylaxis in open fractures
- Open fractures carry an increased infection risk from soft-tissue damage and environmental contamination, with rates rising across Gustilo grades.
- The Gustilo-Anderson grade has historically guided regimen choice: gram-positive cover for low-grade injuries and broader gram-negative cover for high-grade injuries.
- Optimal duration and choice remain non-standardised; coverage of nosocomial and multidrug-resistant organisms is an active research area.
Debridement
The purpose of debridement is to convert a contaminated traumatic wound into a surgically clean, viable wound that can heal or be reconstructed.
Operative preparation
Before incision:
- review imaging and planned extensions
- confirm antibiotics and tetanus plan
- prepare for vascular control if needed
- position the patient for fracture access and possible flap planning
- prep widely to allow extension, fasciotomy, external fixation and flap harvest when relevant
- obtain intraoperative photographs if useful for team communication
Surgical technique
Perform debridement systematically:
- Extend the traumatic wound along safe lines to expose the zone of injury.
- Excise non-viable skin edges conservatively but decisively.
- Remove foreign material, gravel, clothing, grass and gross contamination.
- Open fascial planes and inspect each compartment when required.
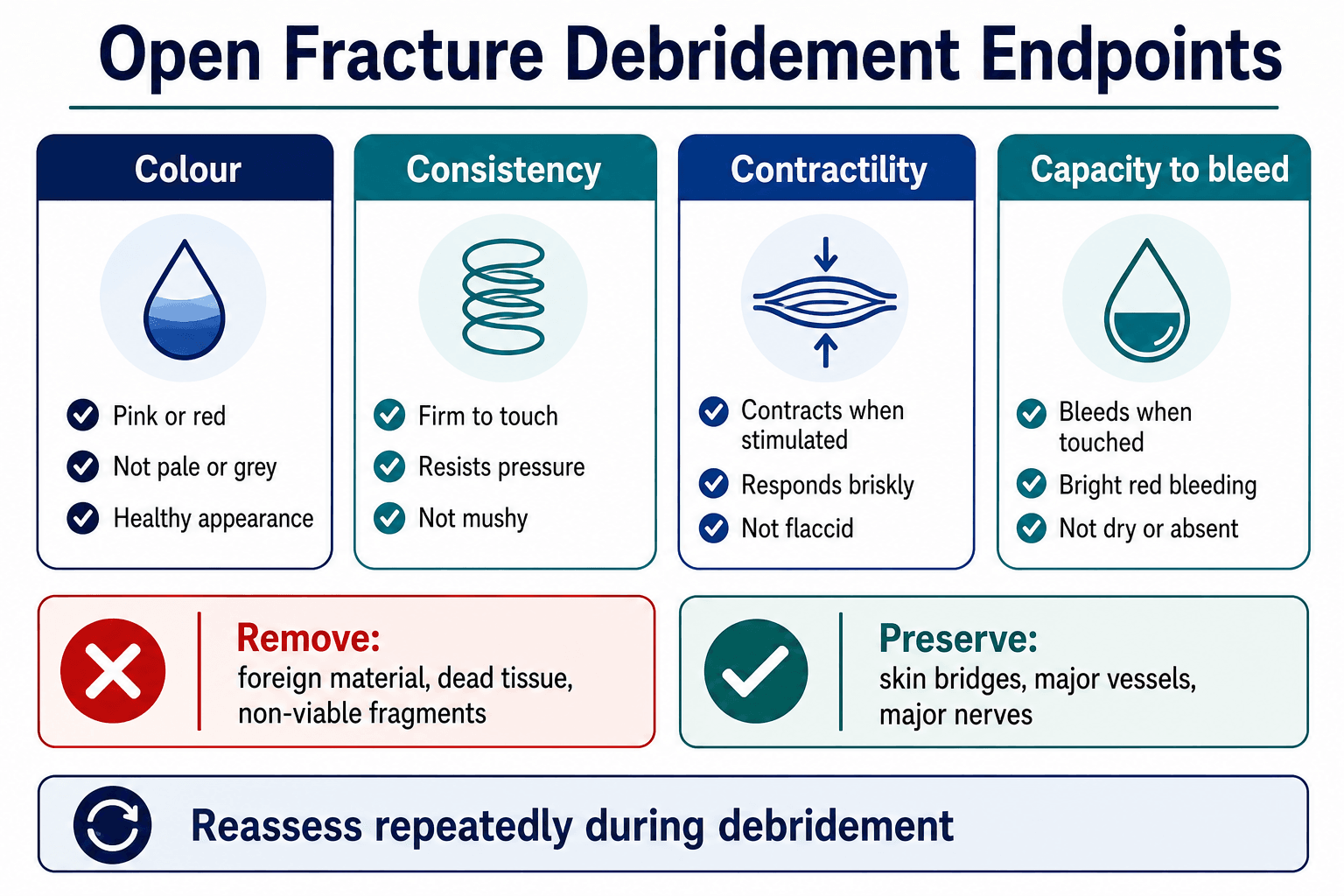
- Assess muscle viability using colour, consistency, contractility and capacity to bleed.
- Excise devitalised muscle until the remaining tissue is viable.
- Remove loose, avascular, contaminated bone fragments that have no soft-tissue attachment.
- Preserve major articular fragments and attached bone when reconstruction requires them.
- Irrigate with low-pressure saline after excising devitalised tissue.
- Reassess the wound after tourniquet release if a tourniquet was used.
- Decide whether the wound is suitable for closure, temporary dressing, negative pressure dressing, bead pouch, planned second look or flap coverage.
Irrigation
Irrigation removes loose debris and dilutes contamination, but it does not replace excision of devitalised tissue. Low-pressure saline irrigation is preferred. High-pressure lavage can drive bacteria deeper and damage viable tissue.
4 CsMuscle Viability
Hook:Viable muscle is pink, firm, contracts and bleeds.
FLOW trial: wound irrigation in open fractures
- Reoperation rates were similar across high, low and very-low irrigation pressure (13.2 percent vs 12.7 percent vs 13.7 percent).
- Castile soap had a higher reoperation rate than normal saline (14.8 percent vs 11.6 percent; hazard ratio 1.32).
- Very-low-pressure saline is an acceptable low-cost option; additives offer no advantage.
Skeletal Stabilisation
The fixation plan should stabilise bone while protecting the soft-tissue reconstruction plan.
- Best suited to
- Immediate temporary emergency stabilisation
- Advantages
- Fast, reduces pain and soft-tissue motion
- Risks or limitations
- Not definitive for unstable injuries
- Best suited to
- Damage control, severe contamination, vascular repair, unstable physiology or temporary fixation before flap
- Advantages
- Fast, keeps implants away from contaminated zone, allows wound access
- Risks or limitations
- Pin-site infection, malalignment, patient burden, later conversion issues
- Best suited to
- Many open tibial and femoral shaft fractures after debridement when soft tissues allow
- Advantages
- Load-sharing, alignment control, early mobilisation
- Risks or limitations
- Infection risk if used through contaminated field or without coverage plan
- Best suited to
- Periarticular fractures, articular reconstruction or selected metaphyseal patterns
- Advantages
- Anatomic reduction and stable fixation
- Risks or limitations
- Implant exposure risk; requires careful soft-tissue handling
- Best suited to
- Bone loss, infection, severe soft-tissue compromise, deformity, segmental defects
- Advantages
- Allows gradual correction, compression, transport and weight-bearing in selected cases
- Risks or limitations
- Complex care, pin-tract problems, prolonged treatment
Practical decision-making
Use external fixation when the patient or limb is not ready for definitive internal fixation. Use internal fixation when the wound has been adequately debrided, contamination is controlled, soft-tissue cover is planned and the construct will help rehabilitation.
For a severe open tibial fracture, the best fixation is often the fixation that makes the flap and bone reconstruction possible, not the fixation that looks ideal on the radiograph alone.
SPRINT: prognostic factors after tibial nailing
- In open fractures, reamed nailing carried a higher risk of adverse events (odds ratio 3.26) whereas unreamed nailing did not reach significance.
- High-energy mechanism, stainless-steel nails, a residual fracture gap and early full weight-bearing each increased the risk of negative outcomes.
- Open fractures managed without complex secondary wound reconstruction had markedly fewer adverse events.
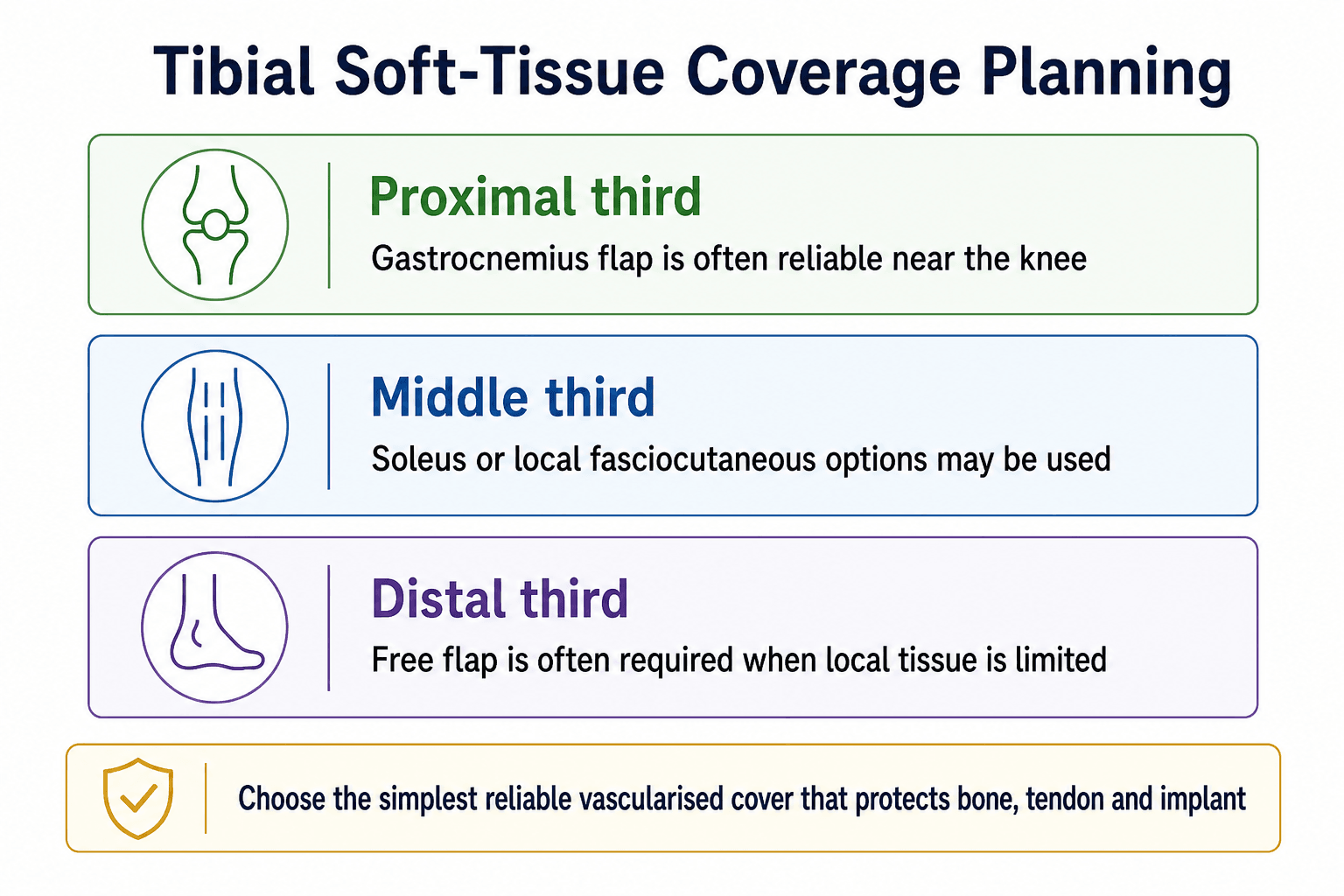
Soft-Tissue Coverage
Soft-tissue coverage is the decisive step in severe open fractures. Exposed bone without periosteum, exposed tendon, exposed joint and exposed implants require vascularised cover.
Coverage ladder
The reconstructive option must match the defect:
- delayed primary closure only when viable, clean and tension-free
- split-thickness skin graft only when there is a vascularised bed
- local flap when local tissue is viable and reaches without tension
- regional flap for predictable local coverage
- free flap for large defects, distal-third tibial wounds, exposed implants or limited local options
Timing
Early coverage is preferred when the wound is clean, the patient is stable and the orthoplastic team is available. Many systems target definitive closure or coverage within 72 hours for severe lower-limb open fractures when feasible.
If early cover is unsafe, the reason should be explicit: patient physiology, contamination requiring repeat debridement, uncertain tissue viability, vascular status, or lack of appropriate reconstructive resources. Delay should not be passive.
Orthoplastic principles
For Type IIIB and IIIC injuries:
- orthopaedic and plastic surgeons should plan together
- fixation should not block the flap pedicle or inset
- external fixator pins must avoid flap donor and recipient zones
- dead space must be eliminated
- bone grafting should wait until infection risk and soft-tissue cover are controlled
- rehabilitation must be included in the plan from the start
Godina: early microsurgical reconstruction
- Free-flap transfer within 72 hours had a flap failure rate of 0.75 percent versus 12 percent at 72 hours to 3 months and 9.5 percent beyond 3 months.
- Early coverage had far lower infection (1.5 percent vs 17.5 percent), faster bone healing and fewer operations.
- This established the principle that earlier vascularised coverage improves outcomes in complex extremity trauma.
Surgical Technique
This is a general open fracture debridement framework. Specific fixation and flap technique depends on the bone, wound and patient.
Position and prep so the team can access the wound, fracture, vascular structures, fasciotomy zones and potential flap territory.
Position and setup
- Position to allow access to the wound, fracture, vascular structures and potential flap zones.
- Use a radiolucent table when fixation imaging is required.
- Prep and drape widely enough for extension, fasciotomy, external fixation and donor sites.
- Ensure antibiotics have been given.
- Confirm availability of implants, external fixator, vascular instruments and plastic surgery support when needed.
Approach
- Use the traumatic wound but extend it safely.
- Avoid creating narrow skin bridges.
- Raise flaps only as needed and preserve perforators when possible.
- Do not make incisions that compromise future flap design.
Debridement sequence
- Skin and subcutaneous tissue: excise clearly non-viable edges.
- Fascia: open as needed to inspect compartments.
- Muscle: use the four Cs.
- Tendon: preserve viable tendon but cover it with vascularised tissue if exposed.
- Nerve and vessel: identify, protect and involve relevant teams for repair.
- Bone: remove loose avascular fragments; preserve reconstructable articular fragments and attached fragments.
- Joint: irrigate and debride if the wound communicates with the joint.
Stabilisation
- Restore length, alignment and rotation.
- Choose fixation that respects the wound and coverage plan.
- Keep external fixator pins away from future flap and incision zones.
- Confirm alignment and implant position.
Closure or temporary dressing
Close only if:
- debridement is complete
- tissue is viable
- there is no concerning contamination
- closure is tension-free
- it will not trap dead space
If not, use a deliberate temporary strategy such as negative pressure wound therapy, bead pouch or planned second-look dressing according to local practice and reconstructive plan.
Complications
- Why it happens
- Contamination, devitalised tissue, dead space, unstable fixation or delayed cover
- Prevention or response
- Early antibiotics, meticulous debridement, stability, vascularised coverage and culture-guided treatment if infection develops
- Why it happens
- Bone loss, infection, smoking, instability, severe soft-tissue injury
- Prevention or response
- Stable fixation, manage infection, bone grafting or reconstruction when soft tissues are ready
- Why it happens
- Persistent infection in bone or sequestrum
- Prevention or response
- Debridement, dead-space management, stable reconstruction and targeted antibiotics
- Why it happens
- Poor vessel selection, tension, infection, haematoma, venous congestion
- Prevention or response
- Orthoplastic planning, careful inset, monitoring and urgent re-exploration when compromised
- Why it happens
- Crush, reperfusion, bleeding or swelling
- Prevention or response
- Serial examination, fasciotomy when indicated
- Why it happens
- Inadequate reduction, prolonged immobilisation, pain and soft-tissue scarring
- Prevention or response
- Appropriate fixation, early rehabilitation and alignment checks
Follow-up priorities
Follow-up should check:
- wound healing and flap viability
- pin sites or surgical wounds
- inflammatory markers when infection is suspected
- fracture alignment and progression to union
- neurovascular function
- joint range of motion
- pain and psychological recovery
- readiness for bone grafting, transport, frame adjustment or staged reconstruction
Postoperative Care
Postoperative care is not passive observation. It is active surveillance for infection, vascular compromise, compartment syndrome, fixation failure and soft-tissue failure.
First 24-48 hours
- repeat neurovascular observations
- monitor pain pattern and compartment risk
- check dressings, splints, external fixator pins and plaster pressure areas
- review antibiotic plan and renal function
- confirm tetanus prophylaxis has been completed
- discuss planned second-look debridement or flap timing
- start thromboprophylaxis according to injury and patient risk
- involve physiotherapy and occupational therapy early
After coverage or closure
- monitor flap colour, capillary refill, turgor and Doppler signal where applicable
- protect the flap from pressure and shear
- maintain fracture alignment and fixation stability
- progress weight-bearing according to fixation, bone loss and soft-tissue reconstruction
- plan bone grafting, Masquelet stage two, bone transport or frame adjustment when required
Follow-up
Follow-up should check wound healing, flap viability, inflammatory markers when infection is suspected, radiographic progression to union, alignment, joint stiffness, pain, nerve recovery, psychological recovery and readiness for further reconstruction.
Outcomes/Prognosis
Outcome depends on injury energy, contamination, soft-tissue loss, vascular injury, host factors, infection control and rehabilitation. A Type I open fracture in a healthy patient can heal uneventfully. A Type IIIB or IIIC tibial fracture may require repeated operations, flap coverage, staged bone reconstruction and prolonged rehabilitation.
Poor prognostic features include:
- vascular injury
- crush or segmental muscle loss
- severe contamination
- bone loss
- delayed antibiotics or inadequate debridement
- unstable fixation
- delayed or failed soft-tissue cover
- smoking, diabetes, malnutrition or immunosuppression
- psychological distress and poor social support
The realistic goals are union, infection control, durable cover, limb alignment, joint motion, pain reduction and useful function. The radiograph is only one part of outcome.
Guidelines, Registries & Global Practice
Open fracture care follows the same evidence-based principles worldwide, but the named guidelines emphasise different aspects. The shared message is a coordinated trauma pathway: early resuscitation, prompt antimicrobial prophylaxis to local policy, tetanus assessment, senior orthoplastic decision-making and early transfer to a unit with combined orthopaedic, plastic, vascular and rehabilitation capability.
Global epidemiology
- Open fractures account for an estimated 3 to 4 percent of all fractures, with the tibial diaphysis the most common site because of its subcutaneous anteromedial border.
- A bimodal pattern is typical: high-energy injury in younger men (road and motorcycle trauma, industrial and ballistic injury) and low-energy fragility injury in older adults.
- Infection risk rises with Gustilo grade, from roughly 0 to 2 percent in Type I and II to over 10 percent in Type III, and is highest in IIIB injuries.
Side-by-side guidelines
- Antibiotic emphasis
- Within 1 hour of injury; IV co-amoxiclav or cephalosporin to local policy
- Debridement and coverage
- Debridement on a scheduled trauma list (immediate for contamination, ischaemia or compartment syndrome); definitive fixation and cover within 72 hours
- Distinctive point
- Combined orthoplastic decision-making and centralised care are explicit standards
- Antibiotic emphasis
- Early gram-positive cover, broaden for higher grades
- Debridement and coverage
- Urgent but not arbitrary six-hour debridement; staged management for severe injury
- Distinctive point
- Strong endorsement of low-pressure saline irrigation after FLOW
- Antibiotic emphasis
- Early systemic prophylaxis tailored to grade and contamination
- Debridement and coverage
- Damage-control external fixation when physiology or soft tissues are unfavourable, converting when safe
- Distinctive point
- Fixation chosen to protect the soft-tissue envelope and biology
- Antibiotic emphasis
- Grade-based regimens with local antimicrobial stewardship
- Debridement and coverage
- Emphasis on orthoplastic networks and early definitive cover
- Distinctive point
- Supports regionalised severe-trauma services
Registry and network evidence
- National audit data (for example the UK orthoplastic networks built around BOAST standards) show lower deep-infection and flap-failure rates when severe open tibial fractures are managed in combined orthoplastic centres rather than by repeated unplanned debridements.
- Fixation-related outcomes for open tibial fractures are tracked through trauma databases and trial cohorts (SPRINT) rather than arthroplasty registries; the consistent signal is that the soft-tissue plan, not the implant alone, drives results.
High- versus limited-resource practice
- Where orthoplastic, vascular and microsurgical services are available, the goal is early single-stage debridement, definitive fixation and free-tissue cover.
- In limited-resource or austere settings, staged external fixation, planned second-look debridement, local flaps and earlier consideration of amputation for non-salvageable limbs are pragmatic and appropriate.
- The universal non-negotiables are early antibiotics, tetanus cover, thorough debridement, skeletal stability and avoidance of tension closure over a contaminated wound.
Common Traps
- A small wound does not mean a minor open fracture.
- Type IIIB means a flap is required; it is not just "a bad wound".
- Type IIIC is vascular injury requiring repair, and it may also need flap coverage.
- The final Gustilo grade is most reliable after debridement.
- Antibiotics are urgent; debridement should be senior-led and properly resourced.
- Irrigation alone is not debridement.
- Do not close a wound under tension to make the operation look complete.
- Do not put external fixator pins through future flap territory.
- Do not let a limb-salvage score replace judgement and patient-centred counselling.
Special Situations
Gustilo IIIC and vascular injury
The treatment sequence depends on ischaemia time, haemorrhage control, patient physiology and surgical resources.
Key principles:
- control bleeding
- restore perfusion quickly using temporary shunt or definitive repair when appropriate
- stabilise the skeleton enough to protect the repair
- perform fasciotomy when ischaemia-reperfusion or compartment risk is significant
- decide salvage versus amputation through senior multidisciplinary judgement
Compartment syndrome
Open fracture does not protect against compartment syndrome. Compartment syndrome is a clinical diagnosis supported by pressure measurement when the patient cannot be examined reliably.
Farm, soil and sewage contamination
These injuries require:
- broader antimicrobial cover according to local policy
- aggressive removal of contamination
- planned second-look debridement when viability is uncertain
- awareness of clostridial infection and necrotising infection
Ballistic injury
Management depends on energy transfer, contamination, neurovascular injury, fracture stability and joint involvement. Low-energy civilian gunshot wounds are not the same as high-energy military or close-range shotgun injuries.
Paediatric open fractures
Children have better healing potential but still require adult-level principles: antibiotics, tetanus review, debridement when indicated, stable fixation and soft-tissue care. Beware physeal injury, non-accidental injury and growth disturbance.
Limb Salvage and Amputation
Severe open lower-limb trauma requires honest discussion. Salvage is not automatically better than amputation, and amputation is not automatically a failure. The decision is individual and must include the patient when possible.
Consider:
- life-threatening physiology
- warm ischaemia time
- muscle viability
- tibial nerve function
- foot sensation and plantar skin viability
- contamination
- bone loss
- reconstructive options
- expected number of operations
- rehabilitation capacity
- pain, occupation, family support and patient goals
Scoring systems such as MESS can structure thinking, but they are not accurate enough to decide treatment alone.
LEAP: factors in amputation versus reconstruction
- Of 527 severe lower-limb injuries, 408 were salvaged and 119 underwent amputation (55 immediate, 64 delayed).
- Soft-tissue injury severity had the greatest impact on the salvage-versus-amputation decision.
- Absence of plantar sensation and soft-tissue injury, not bone loss, were the dominant predictors of limb status.
Limb salvage may involve multiple operations, infection risk, flap care, bone reconstruction, prolonged non-weight-bearing, chronic pain and late amputation. Counselling should be realistic and documented.
MCQ Practice Points
Q: What defines a Gustilo IIIB open fracture? A: Exposed bone or implant, periosteal stripping, dead space or soft-tissue loss requiring flap coverage. Wound size alone is not the defining feature.
Q: What is the first treatment that should not wait for theatre? A: Systemic antibiotics, with tetanus assessment and prophylaxis according to local guidance. Operative debridement remains essential but antibiotics should begin early.
Q: What did the FLOW trial change in everyday practice? A: It supported low-pressure saline irrigation and moved practice away from aggressive pressure lavage and soap solutions as default choices.
Q: Does an open wound exclude compartment syndrome? A: No. Compartment syndrome can occur with open fractures, especially after crush injury, reperfusion, high-energy tibial fractures and swelling under tight dressings or casts.
At a Glance Table
- What to decide
- Resuscitation, haemorrhage control and transfer needs
- Why it matters
- Life-threatening injury takes priority over limb reconstruction
- What to decide
- Vascular injury, compartment syndrome, crush, contamination or threatened skin
- Why it matters
- These findings change urgency and the senior team required
- What to decide
- Gustilo-Anderson grade after debridement and OTA open fracture descriptors
- Why it matters
- Soft tissue determines infection risk, closure, flap need and fixation strategy
- What to decide
- Splint, external fixation, nail, plate or circular frame
- Why it matters
- Stability protects soft tissue and enables reconstruction
- What to decide
- Primary closure, graft, local flap, regional flap or free flap
- Why it matters
- Exposed bone, tendon, joint or implant needs durable vascularised cover
COVERFirst Emergency Moves
Hook:Cover the wound and cover the patient with the right early treatments.
BLASTType III Red Flags
Hook:A BLAST injury needs senior orthoplastic thinking early.
4 CsDebridement Endpoint
Hook:If muscle fails the four Cs, it usually should not stay.
Clinical Scenarios
Practise clinical reasoning and management decisions out loud
“A patient has a closed-looking tibial shaft fracture with a 4 mm puncture wound over the anteromedial tibia. How do you manage it?”
“A young patient has an open tibial fracture with exposed bone and periosteal stripping but intact pulses.”
“A patient has a mangled leg, open tibial fracture and absent distal pulses after a crush injury.”
Emergency actions
- ATLS assessment and haemorrhage control.
- Photograph once, cover with sterile dressing and splint.
- Document pulses, Doppler, capillary refill, sensation and motor function.
- Give antibiotics and tetanus prophylaxis early.
Classification
- Use Gustilo-Anderson as shared language.
- Assign final grade after debridement when possible.
- IIIA: coverage possible after debridement.
- IIIB: flap required.
- IIIC: arterial repair required.
Operation
- Extend the wound for exposure.
- Remove foreign material and devitalised tissue.
- Use the four Cs for muscle viability.
- Use low-pressure saline irrigation after excision.
- Choose fixation that supports the soft-tissue plan.
Reconstruction
- Primary closure only if viable, clean and tension-free.
- Exposed bone or implant requires vascularised coverage.
- Plan severe tibial injuries with plastic surgery early.
- Follow for infection, union, alignment, flap health and function.
“Open fracture care succeeds when antibiotics, debridement, stabilisation and soft-tissue coverage are treated as one coordinated reconstruction pathway.”
Evidence Base and Controversies
The evidence base supports principles rather than a single rigid protocol.
Early antibiotics, adequate debridement, stable fixation and durable soft-tissue cover are consistent priorities across the literature.
Exact debridement timing, irrigation volume, local antibiotics, fixation conversion timing and salvage versus amputation require context-specific decisions.
Outcomes improve when severe open fractures are managed by coordinated trauma, orthopaedic, plastic surgery, vascular, anaesthetic and rehabilitation teams.
Areas of genuine uncertainty
- Timing of debridement. The historical six-hour rule is not supported by pooled data; antibiotic timing and debridement quality matter more than a rigid clock, though elective delay is still discouraged.
- Irrigation. FLOW settled the pressure and additive debate in favour of low-pressure saline, but optimal volume remains unstandardised.
- Local antibiotics. Antibiotic-loaded beads, cement and powders are widely used for dead-space management, but high-level comparative evidence for routine use is still maturing.
- Single-stage versus staged fixation. Fix-and-flap in one stage suits clean wounds and stable patients; staged external fixation remains appropriate for contamination or unfavourable physiology.
- Salvage versus amputation. No score reliably decides this; the choice is individualised.
Timing of debridement and infection
- No significant difference in infection rate between early and delayed operative debridement across the time thresholds studied.
- Findings held across Gustilo grades, depth of infection and anatomical site.
- The historical six-hour rule has little support, but elective delay is still not recommended.
Evolution and interpretation of Gustilo-Anderson
- The original 1976 classification was modified by Gustilo in 1984 to add the Type III subgroups (IIIA, IIIB, IIIC).
- Descriptors have drifted subtly across four decades of literature, contributing to inconsistent application.
- Newer modifications stratify IIIB by vascular and reconstructive outcomes, but their longevity is unproven.
Negative Pressure Wound Therapy: What the Evidence Actually Shows
The topic repeatedly lists negative pressure wound therapy (NPWT) as a temporary dressing option between debridement and definitive cover, but never says what it does or what the evidence shows - and the evidence is a high-yield, counter-intuitive exam point.
- What it is and where it fits. NPWT applies a sealed foam or gauze dressing connected to suction, creating a partial vacuum over the wound. It removes exudate, reduces oedema and dead space, and provides a temporary sealed cover between debridements while the definitive soft-tissue plan is arranged. It is a temporising dressing, not a definitive reconstruction, and does not cover exposed bone, tendon, joint or implant - those still need vascularised flap cover.
- The pivotal negative trial. For years NPWT was assumed to reduce infection in open fractures, but the WOLLF randomised controlled trial tested this directly in severe open lower-limb fractures and found no reduction in deep infection and no improvement in disability or quality of life versus standard dressings, and no cost benefit. The examinable message is that NPWT does not substitute for thorough debridement, skeletal stability and early definitive vascularised cover - the things that actually control infection.
- How to use it honestly. NPWT remains a reasonable, convenient interim dressing (it manages exudate and protects the wound between trips to theatre), but it must not be used to justify delaying definitive coverage or to compensate for an inadequate debridement. The Godina principle - early definitive cover - still governs outcome.
WOLLF: negative pressure wound therapy in open fractures
- 460 adults with a severe open lower-limb fracture randomised to NPWT (n=226) versus standard dressing (n=234) after the first debridement.
- No difference in Disability Rating Index at 12 months (45.5 vs 42.4; mean difference -3.9, 95 percent CI -8.9 to 1.2; P=0.13).
- No difference in deep surgical-site infection (7.1 percent vs 8.1 percent) or quality of life, and no cost benefit.
- The findings do not support routine NPWT for severe open fractures.
Q: What did the WOLLF trial show about negative pressure wound therapy in open fractures? A: In severe open lower-limb fractures, NPWT after the first debridement did not reduce deep infection or improve 12-month disability or quality of life versus standard dressings. NPWT is a temporary dressing between debridements, not a substitute for thorough debridement, stable fixation and early vascularised coverage.