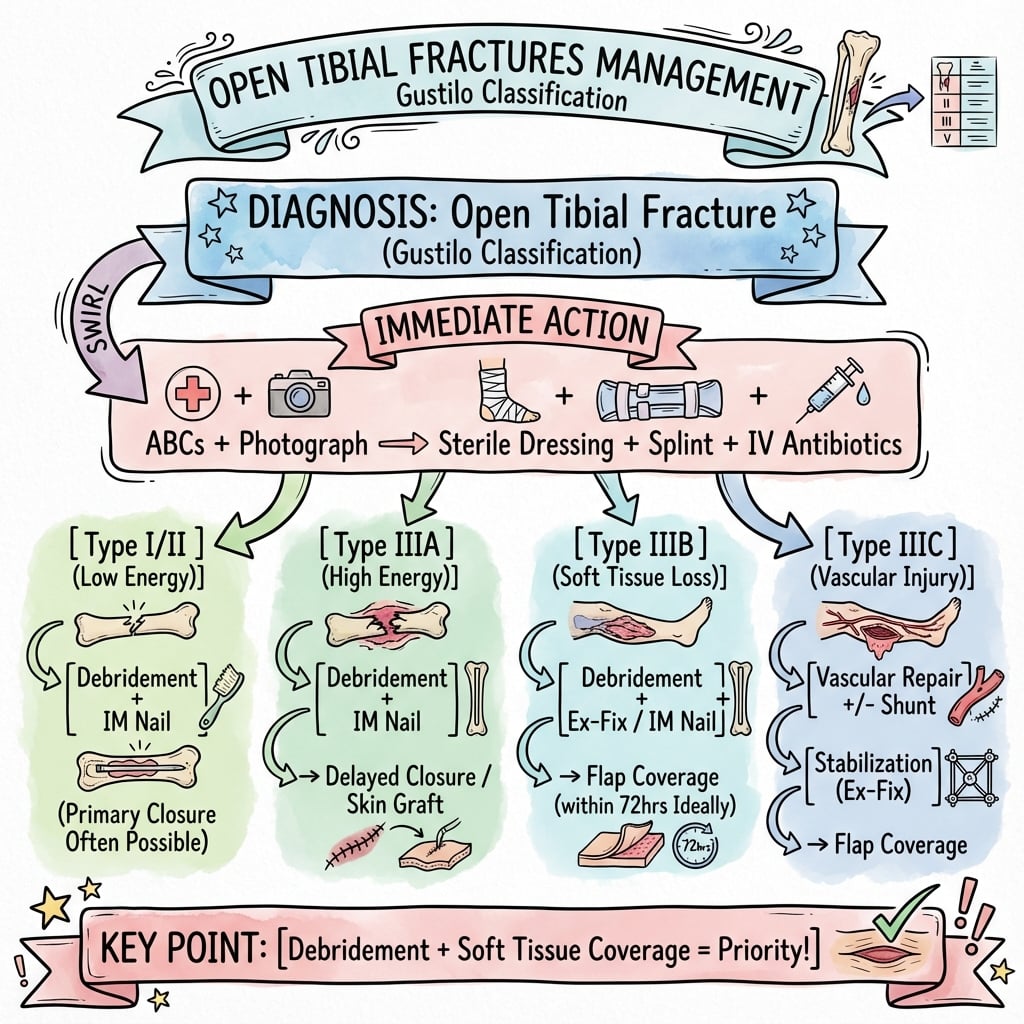
Antibiotic Protocol | Wound Assessment | Soft Tissue Coverage | Fix-or-Flap
- Gustilo-Anderson is assessed INTRAOPERATIVELY - not in ED (wounds deceive)
- Antibiotics within 1 hour - reduces infection more than timing of surgery
- 6-hour rule is MYTH - early antibiotics matter, surgery timing less critical
- IIIB requires flap coverage - involve plastics within 72 hours (fix-or-flap)
- IIIC = vascular injury - revascularization priority, amputation if over 6h warm ischemia
- Farm injuries = add penicillin - Clostridium coverage for gas gangrene
- “Final classification is AFTER debridement in theatre - initial wound size often misleading
- “Antibiotics beat timing - can wait for ideal OR conditions if antibiotics given early
- “4 Cs of muscle viability: Color, Contractility, Consistency, Capacity to bleed
- “NPWT is bridge therapy - definitive coverage still needed by 72 hours
Antibiotics within 1 hour is the single most important intervention. Start in ED immediately upon diagnosis - cefazolin 2g IV for Type I-II, add gentamicin 5mg/kg for Type III.
Gustilo-Anderson is assessed in theatre after thorough debridement. Small external wound can mask severe deep injury. Document final classification in op note.
Type IIIB has exposed bone/hardware without adequate soft tissue. Early plastics involvement is critical - fix-or-flap within 72 hours dramatically reduces infection.
Type IIIC has arterial injury requiring repair. This is limb-threatening regardless of wound size. Revascularization within 6 hours of warm ischemia to prevent amputation.
Overview and Epidemiology
Incidence
- Tibial diaphysis is the most common open long-bone fracture because of its subcutaneous anteromedial surface
- Open fractures are roughly 3% of all fractures in a large epidemiological series (Court-Brown et al, 2386 open fractures over 15 years)
- Most open fractures are actually low-energy: only 22.3% are caused by road-traffic accidents or falls from height; the rest are predominantly low-energy injuries, especially in older patients (Court-Brown et al)
- Bimodal pattern: high-energy open fractures cluster in younger males; low-energy open fractures in older females
Mechanism of Injury
- High energy: motor-vehicle and motorcycle crashes, pedestrian-versus-vehicle, falls from height - produce the larger, more contaminated Type III injuries
- Low energy: simple falls and twisting injuries - can still breach skin over the subcutaneous tibia (often Type I)
- Contaminated environments: agricultural, marine and combat injuries carry distinct organism profiles and demand broader cover
Risk Factors for Infection
- Type IIIB/IIIC classification
- Delay in antibiotics over 1 hour
- Inadequate debridement
- Delay in soft tissue coverage beyond 72 hours
- Smoking, diabetes, peripheral vascular disease
- Farm or water contamination
- Prevalence
- 15-20%
- Infection Rate
- 0-2%
- Union Rate
- Over 95%
- Amputation
- Rare
- Prevalence
- 35-40%
- Infection Rate
- 2-5%
- Union Rate
- 90-95%
- Amputation
- Under 1%
- Prevalence
- 25-30%
- Infection Rate
- 5-10%
- Union Rate
- 85-90%
- Amputation
- 2-5%
- Prevalence
- 10-15%
- Infection Rate
- 10-25%
- Union Rate
- 70-80%
- Amputation
- 5-15%
- Prevalence
- 5-10%
- Infection Rate
- 25-50%
- Union Rate
- 50-70%
- Amputation
- 25-50%
Anatomy and Pathophysiology
Tibial Anatomy Relevant to Open Fractures
- Subcutaneous anteromedial surface: Minimal soft tissue coverage over medial tibia
- Watershed zone distally: Poor blood supply to distal third
- Single bone of weight-bearing: High mechanical demands
- Nutrient artery: Enters posterior cortex, runs proximally - supplies inner 2/3
- Periosteal vessels: Supply outer 1/3 of cortex
- Endosteal supply: Disrupted by IM nailing but usually adequate healing
The leg has 4 compartments - all at risk in open tibial fractures:
- Anterior: Tibialis anterior, EDL, EHL, deep peroneal nerve
- Lateral: Peroneus longus and brevis, superficial peroneal nerve
- Superficial posterior: Gastrocnemius, soleus, plantaris
- Deep posterior: Tibialis posterior, FDL, FHL, posterior tibial nerve/vessels
Pathophysiology of Open Fractures
- Extends beyond visible wound margins
- High-energy mechanisms create larger zones of devitalized tissue
- Periosteal stripping compromises blood supply to bone
- Contamination = presence of bacteria (inevitable)
- Infection = bacterial multiplication with tissue invasion
- Goal: Prevent contamination from becoming infection
- 0-6 hours: Contamination phase - bacteria present but not established
- 6-12 hours: Bacterial multiplication begins
- Over 12 hours: Biofilm formation, infection establishing
- Early antibiotics prevent bacterial establishment regardless of surgery timing
Classification Systems
Gustilo-Anderson Classification (Assessed Intraoperatively)
The Gustilo-Anderson classification is ALWAYS assessed in the operating theatre after debridement and thorough wound inspection. Never definitively classify from the ED - wounds are deceptive and deep injury extent is only apparent at surgery.
Type III Subclassification - Defining the IIIA/B/C Split
- 87 Type III open fractures. The original single Type III grouping was too broad, so it was split into IIIA (adequate soft-tissue cover), IIIB (extensive soft-tissue loss with periosteal stripping/bone exposure) and IIIC (arterial injury requiring repair). Wound-sepsis rates were 4%, 52% and 42% and amputation rates 0%, 16% and 42% respectively.
Wound Size: Under 1cm
Mechanism: Low energy
Soft Tissue: Minimal muscle damage, clean
Key Features:
- Inside-out injury pattern
- Usually puncture wound
- Minimal contamination
Management:
- Cefazolin 2g IV
- Primary closure often possible
- Good prognosis (infection under 2%)
Proper technique and attention to detail ensure optimal outcomes.
Differentiating IIIA from IIIB
- Type IIIA
- Over 10cm or segmental
- Type IIIB
- Over 10cm or segmental
- Type IIIA
- Adequate soft tissue available
- Type IIIB
- **Bone/hardware exposed**
- Type IIIA
- May be stripped but muscle present
- Type IIIB
- Significant stripping, no coverage
- Type IIIA
- Variable (often high-energy)
- Type IIIB
- Often severely contaminated
- Type IIIA
- Usually primary or DPC
- Type IIIB
- **Flap required**
- Type IIIA
- Case by case
- Type IIIB
- **Mandatory early referral**
- Type IIIA
- 5-10%
- Type IIIB
- 10-25%
Type IIIC - Vascular Injury
Defining feature: Arterial injury requiring repair, regardless of wound size
- Absent or diminished distal pulses
- Cool, pale foot
- Prolonged capillary refill over 3 seconds
- Ankle-brachial index under 0.9 (if measurable)
- Warm ischemia time over 6 hours leads to high amputation rate
- Consider shunting for temporary perfusion if delay to definitive repair
- Revascularization before or concurrent with skeletal stabilization
Gustilo-Anderson is the universal language, but a strong answer also states its major limitation and the modern alternative:
- Poor interobserver reliability: agreement on the Gustilo-Anderson grade is only moderate at best (kappa often around 0.5-0.6), and it lumps several distinct injury features into a single grade. It is also a post-debridement judgement, so it cannot be applied reliably in the ED.
- The OTA Open Fracture Classification (OTA-OFC) was created to address this. Instead of one grade it scores each injury component separately - skin, muscle, arterial injury, contamination, and bone loss - each graded (e.g. mild/moderate/severe). This captures, for example, that a small skin wound can accompany severe muscle devitalisation, and it has shown better reliability and prognostic value for outcomes such as amputation, infection and the need for flap coverage.
- How to use both: still classify Gustilo-Anderson (everyone speaks it and it drives antibiotic choice), but recognise it is imperfect and that component-based grading (OTA-OFC) better describes the injury and predicts outcome.
Exam point: cite Gustilo-Anderson but flag its moderate interobserver reliability and that the OTA-OFC grades skin/muscle/arterial/contamination/bone-loss separately with better reproducibility and prognostic value.
Clinical Assessment
Initial ED Assessment
Open fractures are limb-threatening injuries but ATLS principles still apply. Complete primary and secondary survey before focusing on the open fracture. Associated injuries are common in high-energy trauma.
- ATLS assessment - polytrauma common with high-energy mechanisms
- Hemorrhage control if active bleeding
- Compartment syndrome assessment (pain out of proportion, passive stretch pain)
- Neurovascular examination - document before and after any manipulation
- Photograph wound - single high-quality photo, then cover
- Cover with saline-soaked gauze - do not probe or explore in ED
- Align and splint - reduces bleeding and prevents further contamination
- Check tetanus status - administer if not up to date
- Administer antibiotics - WITHIN 1 HOUR of presentation
Differential Diagnosis and Mimics
The diagnosis of an open fracture is usually obvious, but the critical reasoning is distinguishing what you are actually dealing with, because each scenario changes management.
- Discriminating Features
- Skin intact when cleaned; no communication with fracture
- Why It Matters
- Not an open fracture - antibiotic/theatre urgency differs
- Discriminating Features
- Wound communicates with fracture; fat globules/bone visible
- Why It Matters
- Needs early antibiotics, debridement, coverage
- Discriminating Features
- Pain out of proportion, pain on passive stretch, tense compartments - can coexist with open fracture
- Why It Matters
- Open wound does NOT decompress all compartments; needs fasciotomy
- Discriminating Features
- Absent pulses, cool/pale foot, ABI under 0.9 after realignment
- Why It Matters
- Limb-threatening - revascularisation priority
- Discriminating Features
- Non-reconstructable bone/soft tissue, prolonged warm ischaemia, unstable polytrauma
- Why It Matters
- Salvage may be worse than amputation - shared decision
- Discriminating Features
- Crepitus, rapidly spreading erythema, systemic toxicity, pain out of proportion
- Why It Matters
- Surgical emergency - radical debridement, not routine cover
Investigations and Imaging

Antibiotic Therapy
Early antibiotics are the single most important intervention to prevent infection. Studies consistently show antibiotics within 1 hour reduce infection more than timing of surgical debridement. Start in ED - do not wait for theatre.
Antibiotic Protocol:
- First-Line Regimen
- Cefazolin 2g IV q8h
- Duration
- 24-48h post-closure
- Additional Coverage
- -
- First-Line Regimen
- Cefazolin 2g IV q8h
- Duration
- 24-48h post-closure
- Additional Coverage
- -
- First-Line Regimen
- Cefazolin 2g + Gent 5mg/kg
- Duration
- 72h or until closure
- Additional Coverage
- -
- First-Line Regimen
- Above + Penicillin 4MU IV q4h
- Duration
- As above
- Additional Coverage
- Clostridium
- First-Line Regimen
- Consider fluoroquinolone
- Duration
- As above
- Additional Coverage
- Gram negatives
If penicillin allergic:
- Type I-II: Clindamycin 900mg IV q8h
- Type III: Clindamycin + aminoglycoside or aztreonam
- Single photograph - high quality, ruler for scale
- Do not explore - save for theatre
- Saline-soaked gauze - iodine-soaked is controversial
- Impervious cover - prevents repeated exposure
- Splint - reduces bleeding, contamination, pain
- Multiple wound inspections (increases contamination)
- Probing in ED (introduces bacteria)
- Packing with betadine (tissue toxicity debated)
- Delaying antibiotics for any reason
Proper technique and attention to detail ensure optimal outcomes.
Management
Management Algorithm
- ATLS primary and secondary survey
- Antibiotics within 1 hour
- Tetanus prophylaxis
- Photo-document wound then cover
- Align and splint
- Theatre booking
- Type I-II: Urgent (within 24 hours)
- Type III: Same-day theatre
- Type IIIB: Early plastics consult
- Type IIIC: Immediate OR with vascular
Conservative vs Operative
Conservative management is NOT appropriate for open tibial fractures. All require:
- Surgical debridement
- Skeletal stabilization
- Definitive soft tissue coverage
Decision Points:
- Primary vs staged fixation (depends on contamination)
- Wound closure timing (primary vs delayed)
- Need for flap coverage (IIIB always requires)
Wound Management
- Primary closure often possible
- Delayed primary closure (DPC) at 3-5 days if any contamination
- DPC preferred (close at 48-72h if wound clean)
- Split-thickness skin graft if tension
- May close primarily if clean
- More commonly DPC or local flap
- Cannot close - bone exposed
- Requires muscle flap ± skin graft
- Target coverage by 72 hours
Proper technique and attention to detail ensure optimal outcomes.
Surgical Technique
Step-by-Step Surgical Approach:
1. Wound Extension
- Extend wound to visualize full zone of injury
- Longitudinal incisions (respect fasciocutaneous perforators)
- Must see healthy tissue in all directions
- Avoid transverse incisions across tibia
2. Skin and Subcutaneous Tissue
- Excise non-viable skin edges (limited excision)
- Remove contaminated subcutaneous tissue
- Be conservative with skin - can always take more later
- Sharp debridement preferred
3. Fasciotomy Consideration
- Low threshold for prophylactic fasciotomy in Type III
- 4-compartment release if any concern for CS
- Better to do and not need than miss compartment syndrome
- Two-incision technique: anterolateral and posteromedial
4. Muscle Debridement
- Apply the 4 Cs: Color, Consistency, Contractility, Capacity to bleed
- All four must be present to consider viable
- Serial debridement often needed (planned second look at 48h)
- Err on side of debridement - necrotic muscle causes infection
5. Bone Debridement
- Remove completely loose, devitalized fragments without soft tissue
- Preserve attached fragments if any periosteal blood supply
- Large structural fragments may need to stay despite questionable viability
- Minimal periosteal stripping from viable bone
6. Irrigation
- High volume, low pressure (bulb syringe or gravity 30cm above wound)
- 3L for Type I, 6L for Type II, 9+L for Type III
- Normal saline (soap additives no benefit per FLOW trial)
- Pulsatile lavage may drive bacteria deeper - avoid
Proper technique and attention to detail ensure optimal outcomes.
- Indications
- Type IIIB/C, temporary
- Advantages
- Minimal implant, allows wound access
- Disadvantages
- Pin site infection, malunion
- Indications
- Type I-IIIA, clean
- Advantages
- Definitive, load-sharing
- Disadvantages
- Infection risk if contaminated
- Indications
- Type IIIB after coverage
- Advantages
- Definitive after soft tissue healed
- Disadvantages
- Two procedures required
- Indications
- Periarticular, IIIC
- Advantages
- Anatomic reduction
- Disadvantages
- Extensive dissection, devascularization
Soft Tissue Coverage
Timing - Fix-or-Flap Principle
Godina Principle - Fix and Flap Within 72 Hours
- 532 extremity reconstructions stratified by timing. Free-flap failure 0.75% when transferred within 72 hours vs 12% at 72h-3 months. Post-operative infection 1.5% vs 17.5%. Bone-healing 6.8 vs 12.3 months and hospital stay 27 vs 130 days favouring early coverage.
Timing Recommendations:
- Under 72 hours: Optimal window - lowest infection and flap failure
- 72h - 7 days: Intermediate risk - still reasonable outcomes
- Over 7 days: Increased infection, flap failure, and non-union rates
Flap Selection by Location
- Primary Flap
- Gastrocnemius rotation
- Alternative
- Free flap
- Notes
- Medial head most common
- Primary Flap
- Soleus muscle flap
- Alternative
- Gastrocnemius if reach
- Notes
- Longer arc of rotation
- Primary Flap
- Free tissue transfer
- Alternative
- Propeller flaps if small
- Notes
- Watershed zone - poor local options
Flap Details
- Proximal tibial coverage
- Can reach to mid-tibia in some cases
- Medial head most commonly used (larger)
- Based on sural artery (from popliteal)
- Harvest through medial incision
- Rotate into wound, skin graft over muscle
- Reliable blood supply
- Minimal donor site morbidity
- Some ankle plantarflexion weakness
Proper technique and attention to detail ensure optimal outcomes.
Complications
Infection
- Type IIIB/C classification
- Antibiotic delay over 1 hour
- Inadequate debridement
- Delayed soft tissue coverage
- Smoking, diabetes
- Prevention is key (early antibiotics, adequate debridement)
- Culture-directed antibiotics if infection develops
- May need repeat debridement
- Consider antibiotic beads or cement spacers
- Hardware removal if infection persists
Non-union
- Type III injury
- Bone loss
- Infection
- Smoking
- Inadequate fixation
- Exchange nailing
- Plate augmentation
- Bone grafting (autograft, RIA)
- Masquelet technique for segmental defects
- Free vascularized fibula for massive defects
Compartment Syndrome
Open fractures can still develop compartment syndrome! The wound does not adequately decompress all 4 compartments. Maintain high index of suspicion and low threshold for fasciotomy in Type III injuries.
Amputation
Consider primary amputation if:
- Crush injury with non-viable limb (MESS score over 7)
- Prolonged warm ischemia (over 6 hours)
- Severe polytrauma where limb salvage compromises life
- Mangled extremity with no prospect of function
MESS Score: Mangled Extremity Severity Score
- Skeletal/soft tissue injury
- Limb ischemia
- Shock
- Patient age
- Score over 7 predicts amputation, but imperfect predictor
The topic uses the MESS to frame the amputation decision, but the examinable evidence is the Lower Extremity Assessment Project (LEAP), which fundamentally changed how this decision is understood:
- Function is similar either way: at 2 and 7 years, patients who underwent limb salvage and those who had amputation had broadly equivalent functional outcomes (Sickness Impact Profile scores), with high complication and re-operation rates in both groups - salvage is not automatically the "better" choice.
- Severity scores poorly predict and should not dictate the decision: LEAP found that lower-extremity injury-severity scores (including the MESS) had poor sensitivity/specificity for who ultimately needs amputation - a high MESS supports but must not mandate amputation. The earlier "MESS over 7 = amputate" teaching is too rigid.
- What actually drives outcome: patient and psychosocial factors - return to work, self-efficacy, social support, education, smoking, and the presence of an insensate plantar foot (and notably, initial plantar insensation does NOT reliably predict a poor long-term sole) - influenced outcome more than the limb decision itself.
- Implication: the salvage-versus-amputation decision is a shared, multidisciplinary, patient-centred decision (orthoplastic + vascular + patient), informed by but not dictated by scores; counsel that a salvaged limb often means multiple operations and a long rehabilitation for function comparable to a well-fitted prosthesis.
Exam point: quote LEAP - salvage and amputation give similar long-term function, injury-severity scores (MESS) predict poorly and should guide not dictate, and psychosocial factors dominate outcome - so the decision is a shared one, not a number.
Postoperative Care
Antibiotic Duration
- Continue 24-48 hours post-closure
- Can discontinue if wound closed and clean
- Continue 72 hours or until definitive closure
- May extend if ongoing wound issues
- No benefit beyond 72h in closed wounds
- Continue penicillin for 7 days
- Higher risk of late Clostridium complications
Wound Monitoring
- Monitor for compartment syndrome (even with open wound)
- Watch for signs of infection (fever, increased pain, discharge)
- Neurovascular checks every 4 hours
- Consider second-look surgery if concern
- NPWT changed every 48-72 hours
- Inspect wound at each change
- Document progression toward closure
- Plan definitive coverage within 72 hours
Weight-Bearing Protocol
- Touch weight-bearing initially
- Progress as tolerated once callus visible
- Usually 6-8 weeks to partial WB
- Touch to partial weight-bearing initially
- Full weight-bearing once callus bridging 3 cortices
- Usually 8-12 weeks for Type I-II, 12-16 weeks for Type III
- Non-weight-bearing for 2 weeks (flap healing)
- Then progress as per fracture stability
Rehabilitation
- Early ankle/knee ROM to prevent stiffness
- Quadriceps strengthening from day 1
- Gait training with assistive devices
- Address return to work/sport expectations early
Outcomes/Prognosis
Union Rates by Type
- Union Rate
- Over 95%
- Time to Union
- 16-20 weeks
- Infection Rate
- 0-2%
- Secondary Procedures
- 5-10%
- Union Rate
- 90-95%
- Time to Union
- 20-24 weeks
- Infection Rate
- 2-5%
- Secondary Procedures
- 10-20%
- Union Rate
- 85-90%
- Time to Union
- 24-32 weeks
- Infection Rate
- 5-10%
- Secondary Procedures
- 20-30%
- Union Rate
- 70-80%
- Time to Union
- 32-40 weeks
- Infection Rate
- 10-25%
- Secondary Procedures
- 40-60%
- Union Rate
- 50-70%
- Time to Union
- 40+ weeks
- Infection Rate
- 25-50%
- Secondary Procedures
- 60-80%
Infection Outcomes
- Usually responds to debridement and antibiotics
- May require hardware removal if persistent
- Can still achieve union with appropriate treatment
- More difficult to eradicate
- Often requires hardware removal
- May need chronic suppressive antibiotics
- Risk of non-union significantly increased
Functional Outcomes
- Most patients return to pre-injury function
- 80-90% satisfied with outcome
- Return to work: 3-6 months average
- Good function in 70-80%
- May have some ankle/subtalar stiffness
- Return to work: 6-9 months
- Only 50-60% achieve good function
- High rate of chronic pain
- Return to work: 9-18 months, many with restrictions
- Amputation may give better function than poor salvage
Prognostic Factors
- Younger age (under 50)
- Non-smoker
- No medical comorbidities
- Early soft tissue coverage
- Adequate initial debridement
- Type IIIB/C classification
- Smoking
- Diabetes, PVD
- Delayed coverage beyond 7 days
- Bone loss over 2cm
- Infection
Long-term Considerations
- Post-traumatic arthritis in 20-30% (especially with intra-articular extension)
- Chronic pain in 30-40% of Type III
- Leg length discrepancy possible with bone loss
- Need for eventual hardware removal in 10-20%
Guidelines, Registries & Global Practice
Global Epidemiology
- Figure
- ~3%
- Source
- Court-Brown et al, 2386 open fractures over 15 years
- Figure
- Tibial diaphysis
- Source
- Subcutaneous anteromedial surface
- Figure
- 22.3% (most are LOW energy)
- Source
- Court-Brown et al
- Figure
- High-energy in younger males; low-energy in older females
- Source
- Court-Brown et al
Open fractures are a global problem with the heaviest burden in low- and middle-income countries (road-traffic trauma), where access to early antibiotics, theatre and microsurgical coverage is the principal driver of outcome variation rather than any difference in classification or technique.
Major Guidelines Side by Side
- Antibiotics
- Within 1 hour; cephalosporin for all, add gentamicin for high-grade; orthoplastic input
- Debridement timing
- No mandatory 6-hour rule; debride on a planned list with senior ortho + plastics
- Soft-tissue coverage
- Definitive cover within 72 hours where possible; single-stage fix-and-flap encouraged
- Antibiotics
- Early antibiotics emphasised; gram-positive cover for all, add gram-negative for Type III; aminoglycoside/penicillin for gross contamination
- Debridement timing
- Urgent but not strictly within 6 hours; emergent for vascular injury or gross contamination
- Soft-tissue coverage
- Early coverage; supports staged management for severe wounds
- Antibiotics
- Early antibiotic prophylaxis; debridement, stabilisation, coverage as core principles
- Debridement timing
- Adequate debridement prioritised over rigid clock
- Soft-tissue coverage
- Reconstructive ladder; ex-fix to definitive once soft tissues allow
- Antibiotics
- Co-amoxiclav or cefuroxime within 1 hour; reassess in theatre
- Debridement timing
- No fixed 6-hour cut-off; combined ortho-plastic decision
- Soft-tissue coverage
- Skeletal + soft-tissue reconstruction on the same list when feasible
Where guidance genuinely differs it is in emphasis, not direction: all converge on early antibiotics, thorough debridement and early specialist soft-tissue cover. The once-dogmatic 6-hour debridement rule is not endorsed by any current major guideline (Crowley et al; Pollak/LEAP).
Practice Variation
- High-resource systems run combined orthoplastic units allowing single-stage fix-and-flap, lowering deep infection and flap failure (Godina principle).
- Limited-resource settings more often rely on staged external fixation, serial debridement and delayed or local-flap coverage; transfer delay to a definitive centre is a key predictor of infection (Pollak/LEAP).
- Antibiotic regimens vary by local antimicrobial-resistance patterns; the principle (early gram-positive cover for all, broaden for high-grade and contaminated wounds) is universal even where specific agents differ.
Registry and System Evidence
There is no implant registry specific to open tibial fractures equivalent to the arthroplasty joint registries. System-level evidence instead comes from major trauma networks and trial collaboratives (FLOW, SPRINT, LEAP), which underpin the move away from high-pressure/soap irrigation and the rigid 6-hour rule toward early antibiotics and orthoplastic coverage.
Special Considerations
Farm Injuries
Farm injuries carry significant risk of Clostridium perfringens (gas gangrene) and tetani. ADD high-dose penicillin to standard regimen: Penicillin G 4 million units IV q4-6h.
Specific considerations:
- Organic contamination (soil, manure)
- Higher bacterial loads
- Clostridium species common in soil
- More aggressive debridement required
- Consider hyperbaric oxygen if gas gangrene develops
Pediatric Open Tibial Fractures
- Classification same as adults
- Better healing potential
- Lower infection rates
- More likely to tolerate non-operative management for Type I
- Growth plate injuries may affect management
Segmental Injuries
- Automatically classified as at least Type IIIA
- Higher non-union risk
- Often need specialized fixation (IM nail with blocking screws)
- May need bone transport for bone loss
Viva Scenarios
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“32-year-old motorcyclist, MVA 2 hours ago. 15cm wound over tibial shaft, exposed bone, contaminated with gravel. Foot is warm with palpable pulses.”
“22-year-old, fall from height. Severely angulated tibial fracture with 8cm wound. Foot is cool and pale, no palpable pulses, capillary refill 5 seconds.”
“45-year-old farmer, tractor rollover 4 hours ago. Type II open tibial fracture (6cm wound), heavily contaminated with soil and manure. Neurovascularly intact.”
MCQ Practice Points
Q: When is Gustilo-Anderson classification definitively assessed?
A: Intraoperatively, after thorough debridement and wound inspection. Never in ED - wounds are deceptive and deep injury extent is only apparent in theatre.
Q: What antibiotics are indicated for a Type IIIB open tibial fracture on a farm?
A: Cefazolin 2g IV + Gentamicin 5mg/kg IV + Penicillin G 4MU IV. Penicillin is added for Clostridium coverage (tetanus/gas gangrene) in farm injuries with organic contamination.
Q: What flap is used for soft tissue coverage of the proximal third of the tibia?
A: Gastrocnemius rotation flap (medial head most commonly). Middle third = soleus. Distal third = free flap (latissimus dorsi, ALT).
Q: What defines a Type IIIC open fracture?
A: Arterial injury requiring repair, regardless of wound size or soft tissue injury. This is a limb-threatening emergency requiring urgent revascularization within 6 hours of warm ischemia.
Q: Is the 6-hour rule for debridement of open fractures evidence-based?
A: No - this is a myth. Studies show early antibiotics (within 1 hour) are more important than timing of surgical debridement. Surgery can be delayed for appropriate OR conditions if antibiotics given early.
At a Glance
- Classification
- Type I
- Antibiotics
- Cefazolin 2g IV
- Coverage
- Primary closure
- Key Action
- Debride, close, splint
- Classification
- Type II
- Antibiotics
- Cefazolin 2g IV
- Coverage
- DPC at 48-72h
- Key Action
- Serial debridement PRN
- Classification
- Type IIIA
- Antibiotics
- Cefazolin + gent
- Coverage
- Usually primary
- Key Action
- Consider external fixator
- Classification
- Type IIIB
- Antibiotics
- Cefazolin + gent
- Coverage
- Flap required
- Key Action
- Plastics consult day 1
- Classification
- Type IIIC
- Antibiotics
- Cefazolin + gent
- Coverage
- After vascular
- Key Action
- Immediate OR + vascular
- Classification
- Any type +
- Antibiotics
- Add penicillin 4MU
- Coverage
- Depends on type
- Key Action
- Clostridium coverage
CGPOpen Fracture Antibiotics
Hook:CGP for open fractures - Cef for all, Gent for III, Pen for farms!
4 CsMuscle Viability Assessment
Hook:All 4 Cs must be present - debride any muscle that fails ANY criterion!
G-S-FTibial Flap Locations
Hook:GSF from proximal to distal - Gastroc, Soleus, Free flap for the watershed distal tibia!
IIIABCType III Features
Hook:A for Adequate, B for Bone exposed, C for Circulation - ABC of Type III!
Classification (in theatre)
- I: Under 1cm, clean, low energy
- II: 1-10cm, moderate
- IIIA: Over 10cm but adequate coverage
- IIIB: Bone exposed - needs flap
- IIIC: Vascular injury - emergency
Antibiotics (within 1 hour)
- All: Cefazolin 2g IV
- Type III: Add Gentamicin 5mg/kg
- Farm: Add Penicillin 4MU
- Duration: 24-72h until closure
- 6-hour surgery rule is MYTH
Debridement
- Extend wound for visualization
- 4 Cs for muscle viability
- High-volume, low-pressure irrigation
- Saline only (no soap benefit)
- Serial debridement for Type III
Flap Coverage (Fix-or-Flap 72h)
- Proximal: Gastrocnemius
- Middle: Soleus
- Distal: Free flap (lat dorsi, ALT)
- NPWT is bridge, not definitive
- Early plastics involvement
Type IIIC Emergencies
- Realign limb immediately
- Warm ischemia under 6 hours
- Ex-fix then vascular repair
- Consider shunting if delay
- Fasciotomy for reperfusion
Evidence Base
6-Hour Rule Has No Robust Evidence Base
- Systematic review of the timing of debridement and closure for lower-limb open fractures found no convincing evidence that debridement within 6 hours reduces infection. The historical 'six-hour rule' is not supported by the available data.
FLOW Trial - Irrigation Pressure and Solution
- 2447 patients, 2-by-3 factorial RCT. Reoperation rates were similar across high, low and very-low irrigation pressure (about 13%), so very-low pressure is an acceptable low-cost option. Castile soap had a HIGHER reoperation rate than normal saline (14.8% vs 11.6%, hazard ratio 1.32, P=0.01).
Immediate Antibiotics Minimise Type III Infection
- 137 Type III open tibia fractures. On multivariate analysis, antibiotics beyond 66 minutes (odds ratio 3.78) and wound coverage beyond 5 days (odds ratio 7.39) independently predicted deep infection. Time to debridement was NOT associated with infection. Infection was 2.8% when both antibiotics and coverage were early vs 40.5% when both were delayed.
Early Antibiotics - The Patzakis Landmark
- Analysis of 1104 open fracture wounds. The single most important factor in reducing infection was early administration of antibiotics with gram-positive and gram-negative activity, more influential than any other studied variable.
SPRINT Trial - Reamed vs Unreamed Nailing
- 1319 tibial shaft fractures randomised to reamed vs unreamed nailing. In OPEN fractures there was no difference in reoperation (relative risk 1.27, 95% CI 0.91-1.78, P=0.16). A benefit of reamed nailing was seen only in CLOSED fractures (relative risk 0.67, P=0.03).
LEAP - Time to Debridement vs Infection
- 315 patients with severe high-energy lower-limb injuries across 8 Level-I centres. Time from injury to debridement was NOT an independent predictor of infection. Time from injury to admission at a definitive trauma centre WAS an independent predictor, supporting early transfer to specialist care.
Gustilo-Anderson Classification (Original)
- Series of 1025 open long-bone fractures. Defined the Type I-III classification and showed Type III infection fell from 44% (retrospective) to 9% (prospective) with debridement, copious irrigation, delayed closure of Type III wounds and prophylactic cephalosporin.