Navigating the Transitional Zone
Fracture Types
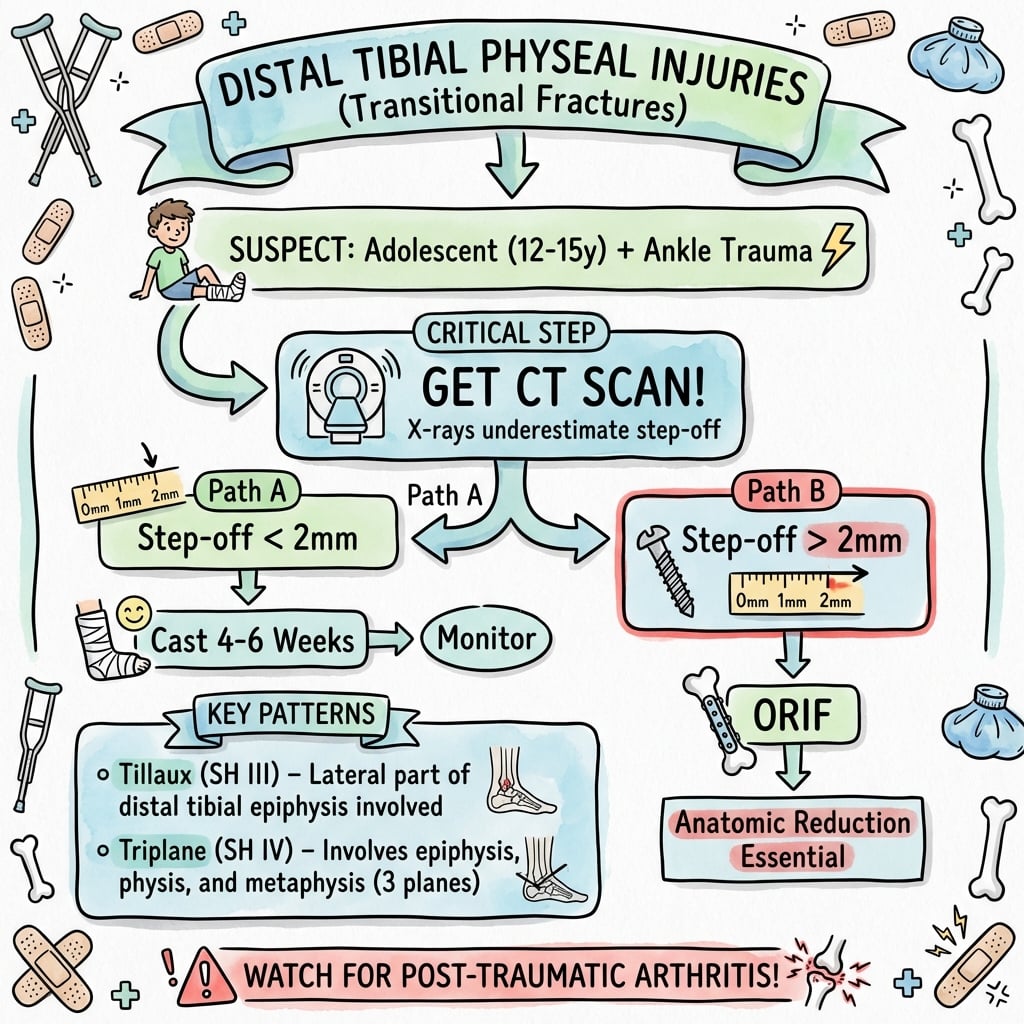
Critical Must-Knows
- Asymmetric Closure: Creates transitional fractures.
- Tillaux: SH III, anterolateral epiphyseal fragment.
- Triplane: SH IV pattern, three-plane fracture.
- 2mm Rule: Greater than 2mm articular step-off needs ORIF.
- Growth Arrest is Less Common: Occurs near skeletal maturity.
Clinical Pearls
- "Know the closure pattern (Central-Medial-Lateral)
- "Tillaux vs Triplane distinction
- "CT is essential for transitional fractures
- "ORIF if step-off greater than 2mm
Clinical Imaging
Imaging Gallery


The 2mm Rule
ORIF Threshold
greater than 2mm articular displacement mandates surgery. Intra-articular malunion leads to arthritis. Anatomical reduction is the goal.
Imaging Trap
CT is essential. Standard X-rays underestimate displacement in transitional fractures (3D geometry).
Tillaux vs Triplane
| Feature | Tillaux | Triplane |
|---|---|---|
| Type III | Type IV | |
| Single plane (horizontal) | Three planes | |
| Anterolateral epiphysis | Variable (2-4 part) | |
| 12-15 years | 12-15 years | |
| ORIF if greater than 2mm | ORIF if greater than 2mm |
CMLPhyseal Closure Pattern
| C | Central Closes first (around age 12) |
| M | Medial Closes second |
| L | Lateral Closes last (Tillaux fragments from here) |
| C | Central Closes first (around age 12) |
| M | Medial Closes second |
| L | Lateral Closes last (Tillaux fragments from here) |
Hook:CML - Central, Medial, Lateral (like a leukemia you don't want).
AITTillaux Features
| A | Anterolateral Location of the fragment |
| I | Intra-articular SH Type III |
| T | Transitional Occurs during physeal closure |
| A | Anterolateral Location of the fragment |
| I | Intra-articular SH Type III |
| T | Transitional Occurs during physeal closure |
Hook:AIT - Anterolateral, Intra-articular, Transitional.
TFCTriplane Features
| T | Three Planes Sagittal, Coronal, Axial |
| F | Four Parts (or 2-3) Variable comminution |
| C | CT Essential X-ray underestimates |
| T | Three Planes Sagittal, Coronal, Axial |
| F | Four Parts (or 2-3) Variable comminution |
| C | CT Essential X-ray underestimates |
Hook:TFC - Three planes, Four parts, CT essential.
Overview/Epidemiology
Distal Tibial Physeal Injuries occur in two main contexts:
- Standard Salter-Harris Fractures: Similar to other physes.
- Transitional Fractures (Tillaux, Triplane): Unique to adolescents due to asymmetric physeal closure.
- Epidemiology:
- Transitional fractures occur between ages 12-15 years.
- More common in boys (due to later physeal closure).
- Standard SH injuries can occur at any age.
- Mechanism:
- External rotation is the most common mechanism for transitional fractures.
- The AITFL (anterior inferior tibiofibular ligament) avulses the anterolateral epiphysis.
Anatomy and Pathomechanics
Physeal Closure Pattern The distal tibial physis closes asymmetrically over 18 months:
- Central: First to close (approximately age 12-14).
- Medial (Anteromedial): Closes next.
- Lateral (Posterolateral): Last to close (approximately age 14-16).
Tillaux Fracture
- The lateral physis is still open when the external rotation force occurs.
- The AITFL attaches to the anterolateral epiphysis.
- External rotation avulses the anterolateral fragment (SH Type III).
Triplane Fracture
- More complex pattern with fracture in three planes.
- Sagittal (through the epiphysis - like Tillaux).
- Horizontal (through the physis).
- Coronal (through the metaphysis - like SH II).
- Can be 2-part, 3-part, or 4-part.
Classification Systems
Standard Salter-Harris
Applied to the Distal Tibia (non-transitional):
Type I: Through the physis only. May be occult.
Type II: Most common in younger children. Metaphyseal fragment.
Type III/IV: Intra-articular. Require anatomical reduction.
Clinical Assessment
History:
- Mechanism: Twisting (external rotation)? Inversion? Direct trauma?
- Age: Transitional fractures occur at ages 12-15.
Physical Exam:
- Inspection: Swelling, ecchymosis, deformity.
- Palpation: Tenderness over the physis (anterolateral for Tillaux).
- ROM: Limited by pain.
- Neurovascular: Document status.
- Fibula: Check for associated fibular fracture.
Investigations
Imaging:
- X-ray (AP, Lateral, Mortise): Standard. May show widening or fragment.
- CT Scan with 3D Reconstruction: ESSENTIAL for transitional fractures. X-ray underestimates displacement.
- Allows measurement of articular step-off and surgical planning.
Management Algorithm
Non-Displaced (Step-off Less Than 2mm)
- Below-Knee Cast: For 4-6 weeks.
- Non-weight bearing initially.
- Close follow-up with X-rays at 1-2 weeks.
Surgical Techniques
Closed Reduction and Percutaneous Fixation (Tillaux)
Indications: Displaced Tillaux amenable to closed reduction.
Technique: Under fluoroscopy, internally rotate the foot to reduce the anterolateral fragment. If anatomical reduction is achieved (confirmed on mortise and lateral), pass a 4.0mm cannulated screw from anterolateral to posteromedial under fluoroscopic guidance, staying within the epiphysis and parallel to the joint.
Post-op: Below-knee cast for 4-6 weeks. Post-op CT to confirm reduction.
Key Surgical Points
- Always obtain post-op CT to confirm reduction.
- Screw fixation is superior to K-wires for compression.
- Screw placement should be parallel to the joint and avoid crossing the physis.
Complications
| Complication | Rate | Prevention/Management |
|---|---|---|
| Malunion | Low if ORIF is done | Anatomical reduction. Post-op CT confirmation. |
| Post-Traumatic Arthritis | Risk with greater than 2mm step-off | Anatomical reduction. |
| Growth Arrest | Low (fractures occur near maturity) | Monitor if significant growth remaining. |
| Wound Complications | Rare | Careful soft tissue handling. |
| Hardware Irritation | Occasional | May require screw removal. |
Postoperative Care
- Immobilization: Below-knee cast for 4-6 weeks.
- Weight Bearing: Non-weight bearing initially, then WBAT at 4-6 weeks.
- Post-Op CT: Essential to confirm reduction, especially for triplane.
- Follow-Up: At 2 weeks (wound check), 6 weeks (cast removal), and 3 months.
- Growth Surveillance: Less critical than at other physes due to near-skeletal maturity.
Outcomes/Prognosis
- Non-Displaced: Excellent outcomes with casting.
- Displaced (Anatomically Reduced): Good outcomes. Low arthritis risk.
- Malunited (Greater Than 2mm): Risk of post-traumatic arthritis.
- Growth Arrest: Uncommon because these fractures occur near skeletal maturity. If significant growth remains, monitor.
Controversies & Areas of Uncertainty
- The 2 mm threshold is convention, not high-level evidence. It derives from articular-step extrapolation and small series; no randomised data define the exact cut-off. Some authors accept up to 2.5 mm in the very mature ankle, while others reduce any visible step in a younger adolescent. Know that it is a pragmatic threshold examiners expect, but be ready to justify deviation by remaining growth and articular location.
- Routine CT vs selective CT. CT clearly changes classification and the operative decision in transitional fractures (Eismann, Nenopoulos), but it irradiates the immature skeleton. Practice varies between obtaining CT on all suspected transitional fractures and reserving it for those that appear displaced on radiographs.
- Closed vs open reduction for the displaced Tillaux. Closed reduction (internal rotation) with percutaneous screw fixation can succeed, but periosteal or AITFL interposition may block it. There is no consensus on how many closed attempts are acceptable before converting to open reduction; repeated forceful manipulation itself raises physeal-arrest risk.
- Need for, and timing of, post-operative CT. Post-operative CT confirms reduction but adds radiation; some surgeons rely on intra-operative fluoroscopy and arthroscopic visualisation instead.
- Growth surveillance. Because these injuries cluster near maturity, the value of prolonged Harris-line/scanogram follow-up is debated - displacement and SH II pattern (not the transitional patterns) are the real arrest predictors (Leary).
Evidence Base
- Defining description of the triplane epiphyseal fracture in 15 children (mean age 13 years)
- Triplane accounted for 6% of 237 consecutive ankle epiphyseal fractures
- Tomography clarified the three-plane geometry; the lateral fragment carried a posterior metaphyseal spike and attached fibula
- At mean 26 months, 3 of 14 had premature symmetrical closure but under 0.5 cm shortening and no angular deformity
- 25 triplane fractures rated by 5 readers with radiographs alone then with CT
- Rapariz classification reliability rose from poor (kappa 0.17) to moderate (kappa 0.41) once CT was added
- CT changed the fracture pattern in 46%, moved displacement across the 2 mm threshold in 39%, and changed the operative decision in 27% of ratings
- 64 intra-articular distal tibial fractures (32 SH III/IV, 32 transitional) read blinded on radiographs then CT
- CT changed the treatment decision in 24 of 64 patients
- Impact was greatest for transitional fractures; minimal change for SH III/IV
- 124 distal tibial physeal fractures; premature physeal closure (PPC) in 12.1%
- 67% of all PPC occurred in SH II fractures; none in SH I or Tillaux
- Each 1 mm of initial displacement carried a relative risk of 1.15 for PPC (P less than 0.01)
- Nondisplaced distal tibial physeal fractures can be treated nonoperatively
- Residual physeal gapping over 3 mm after reduction suggests entrapped periosteum and predicts PPC
- Open reduction of displaced SH III/IV preserves joint congruity and limits physeal arrest
- Systematic review of 13 studies, 114 adolescent Tillaux fractures (mean follow-up 42.8 months)
- Outcomes were excellent across ORIF, CRIF and arthroscopic fixation
- Radiographic deformity (incongruity, angulation, shortening) occurred only in nonoperatively managed fractures left with 2 mm residual displacement; no premature physeal closure in any group
Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
The Tillaux Fracture
"14-year-old with ankle pain after a twisting injury playing soccer. X-ray shows an anterolateral fragment of the distal tibial epiphysis. CT shows 3mm of articular step-off."
This is a **Juvenile Tillaux fracture** - a Salter-Harris Type III fracture of the anterolateral distal tibial epiphysis. The 3mm step-off exceeds the 2mm threshold. Management: **ORIF**. I would attempt closed reduction under fluoroscopy first. If successful, I would place a percutaneous cannulated screw. If closed reduction fails, I would perform an open reduction via an anterolateral approach and fix with a screw. Post-op CT to confirm reduction. Cast for 4-6 weeks.
The Triplane Fracture
"13-year-old with ankle injury after a fall. X-ray shows a fracture through the physis with a metaphyseal fragment. CT shows a 3-part triplane fracture with 4mm step-off."
This is a **Triplane fracture** - a Salter-Harris Type IV pattern with fracture lines in three planes. The 4mm step-off is unacceptable. Management: **ORIF**. I would attempt closed reduction, but given the complexity (3-part), open reduction is likely needed. I would use an anterolateral and possibly anteromedial approach to visualize all fragments. Fix with cannulated screws. Post-op CT is mandatory. Cast for 4-6 weeks.
Non-Displaced Tillaux
"15-year-old with ankle pain. X-ray shows a probable Tillaux fracture. CT shows 1.5mm of articular step-off."
This is a **non-displaced Tillaux fracture**. The step-off is less than 2mm, which is acceptable. Management: **Below-knee cast** for 4-6 weeks. Non-weight bearing initially. Close follow-up with X-rays at 1-2 weeks to ensure no displacement. No ORIF is needed unless displacement increases.
Growth Arrest After Tillaux
"14-year-old, 1 year after a Tillaux fracture. Now has slight valgus of the ankle and 0.5cm LLD."
This suggests **growth arrest** from the Tillaux fracture, though this is uncommon because the injury occurs near skeletal maturity. I would obtain a **scanogram** and **bone age** to estimate remaining growth. If the child is nearly skeletally mature, the LLD and angular deformity may not worsen significantly. If significant growth remains, I would consider **bar excision** (if less than 50%) or guided growth. The small LLD may not require treatment. The valgus may need monitoring or eventual osteotomy if it progresses.
MCQ Practice Points
Anatomy MCQ
Q: Which part of the distal tibial physis closes first? A: Central. Then medial, then lateral (CML pattern).
Classification MCQ
Q: A Tillaux fracture is which Salter-Harris type? A: Type III. It involves the physis and epiphysis only.
Classification MCQ
Q: A Triplane fracture is which Salter-Harris type? A: Type IV. It involves the metaphysis, physis, and epiphysis.
Treatment MCQ
Q: What is the threshold for operative treatment in transitional fractures? A: Greater than 2mm of articular step-off.
Closure Pattern MCQ
Q: In what order does the distal tibial physis close? A: Central, Medial, Lateral (CML) - this asymmetric closure creates transitional fractures.
Imaging MCQ
Q: What imaging modality best defines transitional fracture anatomy? A: CT scan - essential to determine fracture pattern (2-part vs 3-part triplane) and articular step-off.
Guidelines, Registries & Global Practice
Global epidemiology
- Distal tibial physeal fractures are among the most common physeal injuries, peaking in the adolescent growth spurt (girls roughly 8-14, boys roughly 10-16 years).
- Triplane fractures represent approximately 5-10% of paediatric ankle physeal injuries (6% in the original Cooperman/Spiegel series); Tillaux is rarer and seen in the narrower 12-15 year window.
- Mechanism is overwhelmingly low-energy sport/recreational external rotation; both patterns reflect the ascending (central to medial to lateral) physeal closure sequence rather than a discrete injury entity.
Where guidance converges (society and consensus positions)
| Body | Position on transitional ankle fractures |
|---|---|
| AAOS / POSNA (US) | CT recommended for displaced intra-articular and transitional patterns; anatomical articular reduction with greater than 2 mm step-off as the operative trigger. |
| BOA / BSCOS (UK) | Cross-sectional imaging for intra-articular paediatric ankle fractures; restore joint congruity, screw fixation outside the closing physis where possible. |
| AO Foundation | Same 2 mm articular incongruity threshold; epiphyseal/metaphyseal screws kept parallel to and out of the open physis; reduce articular fragment first. |
| EFORT / European paediatric consensus | Endorses CT-guided planning and anatomical reduction; emphasises avoiding repeated forceful manipulations (periosteal interposition risk). |
There is no genuine guideline-level disagreement on the core principles: the 2 mm threshold, CT for transitional patterns, and anatomical articular reduction are universal. Differences are in access, not recommendation.
Registry note: There is no dedicated implant registry for paediatric transitional ankle fractures (these are low-volume, screw-only constructs). The evidence base is therefore case series and systematic review rather than registry survivorship - this is itself an exam point distinguishing it from arthroplasty topics.
High- vs limited-resource practice variation
- Well-resourced: routine pre-operative CT with 3D reconstruction, arthroscopic-assisted or fluoroscopic percutaneous cannulated-screw fixation, and confirmatory post-operative CT.
- Limited-resource: reliance on plain mortise/lateral radiographs and stress/internal-rotation views, with a lower threshold for open reduction when CT is unavailable to confirm the closed result. The principle (anatomical articular reduction) does not change; only the imaging confirmation does.
DISTAL TIBIAL PHYSEAL INJURIES
Clinical summary
KEY FACTS
- •45% Tibial Growth
- •Central-Medial-Lateral Closure
- •Tillaux = SH III
- •Triplane = SH IV
TILLAUX
- •Anterolateral fragment
- •AITFL avulsion
- •External rotation
- •Age 12-15
TRIPLANE
- •3 Planes (S/H/C)
- •2-4 Parts
- •CT Essential
- •Age 12-15
TREATMENT
- •Less than 2mm: Cast
- •Greater than 2mm: ORIF
- •Post-Op CT
- •4-6 Week Immob
Deep Dive: CT Imaging for Transitional Fractures
Why is CT Essential?
- X-rays only show two planes. Transitional fractures are three-dimensional.
- CT accurately measures articular step-off (the critical 2mm threshold).
- CT identifies the number of fragments (2-part vs 3-part vs 4-part triplane).
- 3D reconstruction aids surgical planning.
What to Look For on CT:
- Articular step-off: Measure on axial and sagittal images.
- Fracture pattern: Identify all fragments.
- Physeal involvement: Extent of physeal injury.
- Fibular injury: Often associated.
Post-Op CT:
- Mandatory to confirm anatomical reduction.
- Repeat if there is any concern about reduction quality.
Self-Assessment Quiz
Parent's Guide: Understanding Transitional Fractures
What is a transitional fracture? A transitional fracture is a type of ankle fracture that occurs in adolescents as the growth plate is closing. The growth plate does not close all at once - it closes in stages. During this transition, certain fracture patterns can occur.
What are Tillaux and Triplane fractures? These are the two main types of transitional fractures. They involve the ankle joint, and if the fracture is significantly displaced, surgery is needed to prevent arthritis.
How is displacement measured? A CT scan is used to measure exactly how much the fracture has shifted. If the shift is more than 2mm, surgery is usually recommended.
What is the treatment?
- If less than 2mm shifted: A cast for 4-6 weeks.
- If more than 2mm shifted: Surgery to realign the bones (screws are often used).
What is the outcome? Most patients do very well. Because these fractures occur near the end of growth, growth problems are uncommon.
Rehabilitation Protocol
Phase 1: Immobilization (0-6 weeks)
- Below-knee cast.
- Non-weight bearing initially.
- Toe wiggling and calf pumps.
Phase 2: Early Mobilization (6-10 weeks)
- Cast removal.
- Ankle ROM exercises (dorsiflexion, plantarflexion).
- Progressive weight bearing.
Phase 3: Strengthening (10-16 weeks)
- Resistance exercises (theraband).
- Proprioception and balance training.
- Gait normalization.
Phase 4: Return to Sport (4-6 months)
- Sport-specific training.
- Full ROM and strength.
- Clearance by surgeon.
Differential Diagnosis
The adolescent with a twisted, swollen ankle after sport is the classic crossover - distinguishing a transitional fracture from a "sprain" is the high-yield decision.
Adolescent Ankle Pain After Twisting Injury
| Diagnosis | Key clinical clue | Imaging finding | Pitfall |
|---|---|---|---|
| Anterolateral joint-line tenderness, age 12-15 | SH III anterolateral epiphyseal fragment; CT for step | Missed on AP if undisplaced - get mortise view | |
| Diffuse swelling, age 12-15 | Physeal line plus posterior metaphyseal fragment; three planes on CT | Radiograph underestimates parts and step | |
| Tenderness over the whole physis, younger child | Physeal widening +/- metaphyseal (Thurston-Holland) fragment | SH I may be radiographically occult | |
| Medial joint-line tenderness | Vertical epiphyseal split medially | Highest arrest risk of the SH patterns - reduce anatomically | |
| Point tenderness over distal fibula | SH I fibula or avulsion | Often coexists with tibial injury - examine both | |
| Pain on squeeze/external-rotation stress | Tibiofibular clear-space widening | Rare in open physes; suspect with high fibular tenderness | |
| Tenderness over ATFL, not the physis | Radiograph normal | Diagnosis of exclusion - physeal tenderness means fracture until proven otherwise |
Comparison: Distal Tibia vs Other Physes
Distal Tibia vs Distal Femur
| Feature | Distal Tibia | Distal Femur |
|---|---|---|
| 45% of tibia | 70% of femur | |
| Low (near maturity) | High (30-50%) | |
| Tillaux, Triplane | Rare | |
| Articular reduction | Physis protection |