Tension-Stress Effect | Ilizarov Principles | Bone Regeneration | Limb Lengthening
- Tension-stress law: gradual traction stimulates bone and soft tissue regeneration
- Corticotomy preserves endosteal blood supply (unlike osteotomy)
- Optimal rate is 1mm/day in 4 increments (0.25mm each)
- Consolidation index: 30-45 days per cm lengthened
- Premature removal causes deformity; delayed removal wastes time
- “Ilizarov developed technique observing dogs with fractures in traction
- “Too fast distraction: non-union; too slow: premature consolidation
- “Gradual nerve stretch is tolerated better than acute (nerves adapt to slow elongation)
- “Blood flow increases 2-3x during distraction phase
Gradual controlled traction stimulates regeneration of bone, soft tissues, nerves, and vessels. Applies tension-stress effect: tension creates biological stimulus for tissue genesis.
Preserve endosteal blood supply via corticotomy (perforations) not osteotomy (complete cut). Medullary blood flow critical for regenerate bone formation.
1mm per day in 4 increments (0.25mm each). Too fast causes fibrous non-union; too slow causes premature consolidation. Frequency matters as much as rate.
30-45 days per cm lengthened for consolidation. Premature frame removal risks fracture through regenerate; delayed removal unnecessary and impacts patient.
Overview and Biological Principles
Distraction osteogenesis is a surgical technique that induces new bone formation between bone segments that are gradually separated by controlled traction. Gavriil Ilizarov developed the modern technique in Russia in the 1950s, establishing the biological law of tension-stress.
The tension-stress law states that gradual, controlled traction on living tissues creates mechanical stress that stimulates and maintains regeneration and active growth of certain tissues. This applies not only to bone but also to soft tissues including muscle, tendon, nerve, and blood vessels.
Ilizarov observed that dogs with fractures treated in traction (distracted) healed with callus formation, while those compressed did not. This led him to systematically study controlled distraction, developing principles now used worldwide for limb lengthening and deformity correction.
- Limb length discrepancy (greater than 2-3 cm)
- Congenital deficiencies (fibular hemimelia, PFFD)
- Post-traumatic shortening
- Bone defects after debridement
- Stature lengthening (controversial)
- No bone graft required
- No donor site morbidity
- Soft tissue adaptation occurs simultaneously
- Deformity correction possible during lengthening
- Weight-bearing often possible during treatment
Mechanisms and Biology
The Tension-Stress Effect
The tension-stress law describes how mechanical forces regulate tissue growth and regeneration. Gradual tension stimulates cellular proliferation, matrix synthesis, and differentiation in multiple tissue types.
Cellular Responses:
- Osteoblast proliferation: Increased in distraction gap
- Angiogenesis: Vessel formation parallels bone columns
- Stem cell recruitment: MSCs migrate to regenerate zone
- Growth factor release: VEGF, BMPs, FGFs upregulated
- Response to Gradual Tension
- Intramembranous ossification along tension lines
- Clinical Significance
- New bone forms without cartilage intermediate
- Response to Gradual Tension
- Sarcomere addition, hyperplasia
- Clinical Significance
- Maintains strength during lengthening
- Response to Gradual Tension
- Axonal elongation 1-2mm/day tolerated
- Clinical Significance
- Gradual stretch better tolerated than acute
- Response to Gradual Tension
- Angiogenesis and vessel elongation
- Clinical Significance
- Blood flow increases 2-3x
Corticotomy vs Osteotomy
The surgical technique for creating the bone division critically affects regeneration quality. Ilizarov emphasized the importance of preserving endosteal blood supply.
- Multiple drill holes through cortex
- Thin osteotome to connect holes
- Preserve medullary contents and endosteal vessels
- Low-energy technique minimizes thermal necrosis
- Endosteal blood supply intact (provides 70-80% of bone blood flow)
- Medullary stem cells available for regeneration
- Faster healing than traditional osteotomy
- Less risk of delayed union or non-union
Using saw or high-speed burr creates heat necrosis and damages endosteal blood supply. This delays healing and risks poor-quality regenerate. Multiple drill holes with thin osteotome is the gold standard technique.
Histology of the Regenerate: The Fibrous Interzone and Its Zones
The evidence describes the regenerate as a "physis-like" structure with "parallel bone columns extending from a central growth zone" — here is that zonal architecture, the basic-science core of distraction osteogenesis.
- Central fibrous interzone (FIZ). A radiolucent central band of longitudinally-oriented type I/III collagen with fibroblast-like and undifferentiated mesenchymal cells, aligned along the tension vector. It is the germinal/growth zone from which new bone forms in both directions — the true "physis-like" layer, though it is neither a physis nor endochondral.
- Zones of microcolumn formation (primary mineralization front) flank the FIZ on each side: osteoblasts lay osteoid on the aligned collagen scaffold, mineralising into parallel bone microcolumns (primary spicules) that grow toward the interzone. This is predominantly intramembranous (no cartilage intermediate), though small amounts of transchondroid/endochondral bone appear with less-stable fixation.
- Zones of remodeling and mature bone lie peripherally, next to the original cortical ends, where the microcolumns are remodelled by osteoclast/osteoblast coupling into lamellar bone with a re-forming medullary canal.
- Why the FIZ matters clinically. The width and radiolucency of the interzone on serial films reflect the balance of distraction versus mineralization: a persistently widening lucent interzone signals distraction outrunning bone formation (too fast), while a disappearing interzone signals premature consolidation (too slow). Adequate stability and blood supply keep the interzone organised and the microcolumns parallel.
Q: What is the histological structure of the distraction regenerate? A: A central fibrous interzone (FIZ) of tension-aligned collagen and mesenchymal/fibroblast-like cells — the germinal zone — flanked on each side by primary mineralization fronts where osteoblasts build parallel bone microcolumns (mostly intramembranous), then peripheral zones of remodeling into lamellar bone. A widening lucent FIZ = distracting too fast; a vanishing FIZ = premature consolidation.
Differential of a Failing Distraction
A radiolucent or abnormal distraction gap is not one diagnosis. Distinguishing the cause changes management entirely — slowing, pausing, compressing, or revising. The following differential is high-yield for vivas.
- Likely Cause
- Distraction too fast (fibrous regenerate)
- Distinguishing Features
- Gap enlarges faster than bone forms; columns sparse
- Action
- Pause 3-5 days, then resume at 0.5-0.75mm/day
- Likely Cause
- Premature consolidation (rate too slow / latency too long)
- Distinguishing Features
- Resistance to distraction; early bone bridge
- Action
- Increase rate transiently or re-osteotomise if bridged
- Likely Cause
- Inadequate fixation / excess shear
- Distinguishing Features
- Motion at gap, hourglass or cyst formation
- Action
- Improve frame stability; reduce micromotion
- Likely Cause
- Host factors (smoking, diabetes, NSAIDs, malnutrition)
- Distinguishing Features
- Systemically slow healer; otherwise correct setup
- Action
- Optimise host; consider adjuncts; slow rate
- Likely Cause
- Pin-site or deep infection
- Distinguishing Features
- Local signs, pyrexia, raised CRP
- Action
- Treat infection; pin care; debride if deep
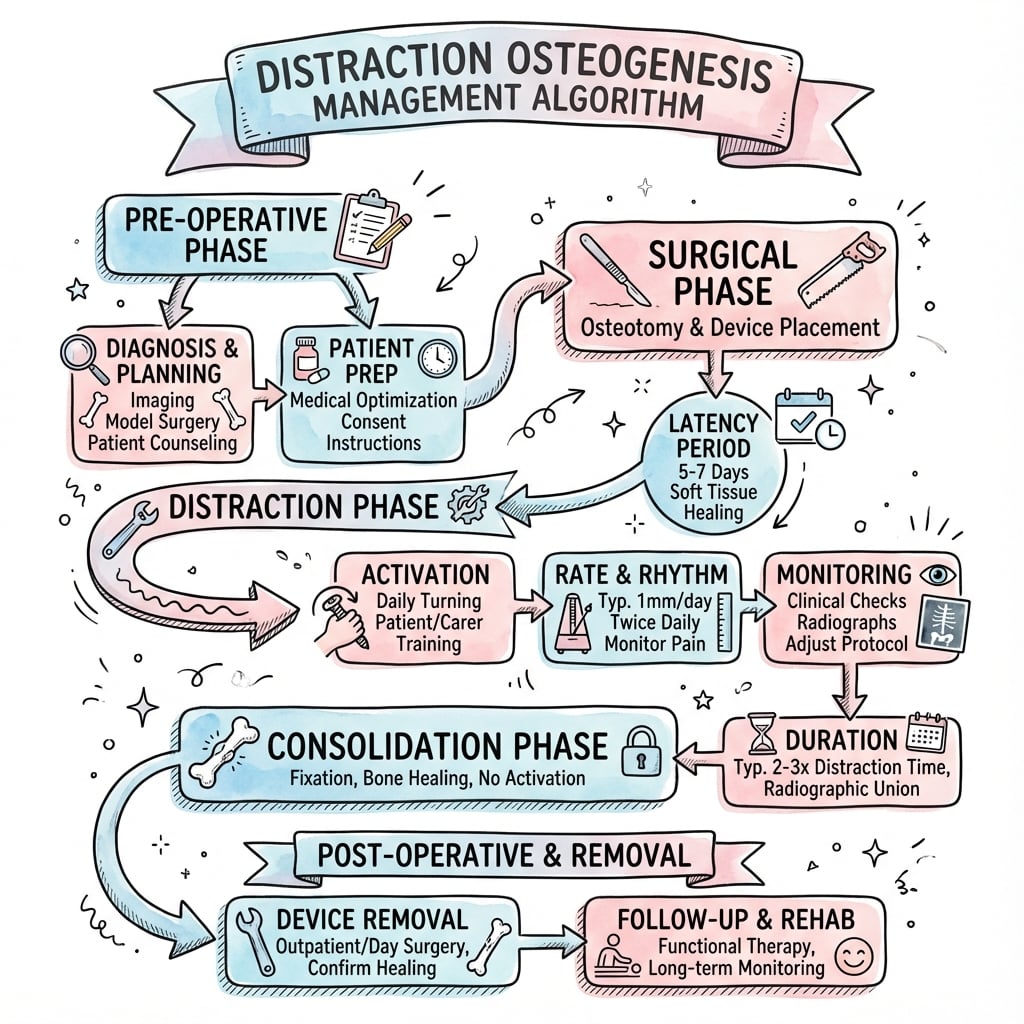
Management Algorithm
Clinical Application and Technique
Phase 1: Latency Period
Latency Phase (5-7 Days)
Corticotomy performed using multiple drill holes connected with thin osteotome. Frame applied with wires or half-pins achieving rigid stability. Soft tissue closure.
Hematoma formation in distraction gap. Inflammatory response recruits cells. Mesenchymal stem cells begin migration. Blood clot provides scaffold.
Fibrin network organizing. Early fibroblastic proliferation. Vascular buds forming. Tissue ready for distraction stimulus.
Optimal Duration:
- Standard: 5-7 days
- Younger children: 5 days (faster healing)
- Older patients or smokers: 7-10 days
- Revision/scarred bone: 10-14 days
Phase 2: Distraction Period
The distraction phase is when gradual lengthening occurs, stimulating bone regeneration through tension-stress effect.
Optimal Distraction Parameters
Standard Protocol:
- Rate: 1 mm per day total
- Rhythm: 4 increments of 0.25 mm each (every 6 hours)
- Speed: Slow, controlled turns of frame
Why 1mm/day?
- Faster: Fibrous tissue forms instead of bone (non-union)
- Slower: Premature mineralization blocks lengthening
- 1mm/day matches regeneration rate of bone columns
Why 4 Times Daily?
- Frequency maintains biological stimulus
- Prevents premature consolidation between distractions
- Better quality regenerate than once-daily distraction
- Reduces pain compared to single large increment
When to modify rate:
- Nerve traction symptoms: Slow to 0.75mm/day or pause 3-5 days
- Poor regenerate on X-ray: Slow to 0.5mm/day
- Premature consolidation: Increase to 1.5mm/day briefly
- Children under 5: Can tolerate 1.5mm/day
Phase 3: Consolidation Period
After achieving desired length, the frame remains in place while regenerate bone mineralizes and gains strength.
Consolidation Phase
Woven bone continues forming. Mineralization begins at margins and progresses centrally. Regenerate still mechanically weak - cannot bear full loads without frame support.
Progressive mineralization visible on radiographs. Cortices forming along periphery. Three cortices rule: wait until 3 of 4 cortices visible on AP and lateral X-rays.
Cortical maturation continuing. Medullary canal reestablishing. Safe for frame removal once 3 cortices mature and patient pain-free.
- Standard: 30-45 days per centimeter lengthened
- Example: 5cm lengthening requires 150-225 days consolidation
- Children: 30 days/cm (faster)
- Adults: 40-45 days/cm
- Smokers, diabetes: 50+ days/cm
Must see 3 of 4 cortices (AP and lateral views) before considering frame removal. Fourth cortex will mature after removal.
Phase 4: Remodeling
After frame removal, bone continues remodeling for months to years, gradually achieving normal architecture.
- Process
- Cortical thickening
- Radiographic Appearance
- Increased density, defined cortices
- Process
- Medullary canal formation
- Radiographic Appearance
- Central lucency developing
- Process
- Complete remodeling
- Radiographic Appearance
- Normal bone architecture restored
Clinical Relevance and Applications
Limb Length Discrepancy
The most common indication for distraction osteogenesis is limb length discrepancy exceeding 2-3 cm. Distraction avoids need for bone graft and allows simultaneous soft tissue adaptation.
Advantages in LLD:
- No graft harvest morbidity
- Precise control of final length
- Can correct angular deformity simultaneously
- Soft tissues lengthen gradually
- Often allows weight-bearing during treatment
Bone Defects
Large bone defects from trauma, infection, or tumor resection can be managed with distraction osteogenesis using bone transport technique.
Bone Transport:
- Corticotomy performed proximal or distal to defect
- Bone segment transported through defect at 1mm/day
- Regenerate forms in transport zone
- Segment docks with opposite end when defect filled
Stature Lengthening
Cosmetic stature lengthening is controversial but increasingly requested, particularly in countries where it's culturally valued.
Cosmetic lengthening in normal individuals raises ethical questions:
- Significant morbidity (9-12 months in frames)
- Complication rates 30-40%
- Risk of permanent nerve injury
- Psychological assessment essential
- Most professional societies advise caution
Only proceed after extensive counseling about risks, timeline, and functional impact.
The Distraction, Consolidation and Healing Indices
The topic quotes a "consolidation index of 30-45 days/cm", a Paley "lengthening index of about one month/cm", and Nasto's magnetic-nail figures — these are distinct, defined metrics worth separating.
- Distraction index = time in the distraction (lengthening) phase per centimetre gained (days/cm). At the standard 1 mm/day it is inherently about 10 days/cm (a centimetre takes ten 1-mm days), so it is largely fixed by the protocol.
- Consolidation index = time from the end of distraction until the regenerate is mature (the three-cortices rule) per centimetre, roughly 30-45 days/cm — slower in adults, smokers and diabetics, faster in children. This is the variable, biology-dependent index.
- Healing index (external-fixation index) = the total time the frame is on per centimetre gained (distraction plus consolidation combined) — Paley's "lengthening index", classically about one month/cm for a single-level lengthening without deformity. It is the single most useful benchmark for counselling and for comparing devices.
- Why they matter. They quantify progress and expose problems: a rising consolidation index flags a poor regenerate or adverse host factors, and a lower healing index is precisely why implantable magnetic nails (a consolidation index around 25 days/cm in the Nasto series) are attractive versus external fixators. Audit outcomes by reporting length gained against goal alongside these indices.
Q: Distinguish the distraction, consolidation and healing indices. A: Distraction index = days/cm during lengthening (about 10 at 1 mm/day). Consolidation index = days/cm from end-of-distraction to three-cortices maturity (about 30-45, slower in adults/smokers). Healing (external-fixation) index = total frame time per cm (Paley's ~1 month/cm) — the best single benchmark; a lower value favours magnetic nails over frames.
Guidelines, Registries & Global Practice
Global Epidemiology
- Limb length discrepancy is the commonest indication; congenital causes (fibular hemimelia, PFFD, hemihypertrophy), post-traumatic physeal arrest, and post-infective shortening dominate paediatric practice worldwide.
- Bone transport for segmental defects is most prevalent where high-energy trauma and chronic osteomyelitis are common, including many limited-resource settings, making the inexpensive ring fixator a globally important tool.
- Cosmetic stature lengthening clusters in specific cultural and economic contexts and carries the highest medico-legal scrutiny.
Side-by-Side Guidance and Society Positions
- Emphasis
- Ring-fixator deformity correction and bone transport
- Practical Recommendation
- 1mm/day in 4 steps; corticotomy preserving endosteum; three-cortices rule before frame removal
- Emphasis
- Open-fracture and bone-loss reconstruction pathways
- Practical Recommendation
- Manage segmental loss in specialist limb-reconstruction units with combined ortho-plastic input
- Emphasis
- Complication classification and lengthening indices
- Practical Recommendation
- Audit using problems/obstacles/complications; consider magnetic IM nails where deformity is minimal
- Emphasis
- Patient selection and informed consent
- Practical Recommendation
- Caution with cosmetic lengthening; multidisciplinary and psychological assessment
Registry and Outcome Notes
- No dedicated arthroplasty-style registry exists for distraction osteogenesis; evidence is driven by single-centre and multicentre series rather than national implant registries.
- Magnetic intramedullary lengthening nail data (e.g. PRECICE-type devices) report lower pin-site morbidity than external fixators but require post-market surveillance for mechanical and metallosis concerns.
- Outcomes are benchmarked using the distraction index (days/cm during lengthening) and consolidation index (days/cm in frame), with paediatric patients consolidating faster than adults.
High- vs Limited-Resource Practice Variation
- Well-resourced settings: magnetic IM nails, hexapod/computer-assisted frames (Taylor Spatial Frame, TrueLok-Hex), CT-based regenerate assessment, and structured physiotherapy.
- Limited-resource settings: the classic Ilizarov ring fixator remains the workhorse — durable, low-cost, reusable, and effective for transport and deformity correction; patient-led daily distraction and pin-site self-care extend reach where follow-up is sparse.
- Pin-site care principles (regular antiseptic cleansing, early treatment of infection) and VTE awareness during prolonged immobilisation are universal, but specific drug choices follow local antimicrobial stewardship and availability.
Controversies and Areas of Uncertainty
Classic teaching mandates 5-7 days, yet a systematic review of distraction protocols suggests latency may be unnecessary in some models. Optimal latency by age, bone, and device remains debated.
Higher frequency improves regenerate at a given rate, and automated/continuous distraction may be superior in principle, but robust human comparative data versus standard 4x daily manual distraction are limited.
Implantable nails reduce pin-site morbidity, but lack registry-level long-term data and raise device-specific concerns (mechanical failure, metallosis, cost). Best indication boundaries are still being defined.
BMPs, PRP, bisphosphonates, low-intensity ultrasound, and bone-marrow aspirate have all been trialled to accelerate consolidation. Evidence is heterogeneous and none is standard of care.
Ethically contested. High complication rates and prolonged morbidity in otherwise healthy people mean many societies advise caution; thresholds and consent standards vary internationally.
Plain-film three-cortices judgement is subjective. CT, DEXA, and ultrasound are proposed for objective maturity assessment but are not yet universally validated criteria for frame removal.
MCQ Practice Points
Q: What is the standard distraction rate in distraction osteogenesis? A: 1 mm per day in 4 increments of 0.25mm each (every 6 hours). This rate balances bone regeneration capacity with soft tissue tolerance.
Q: What is the consolidation index and typical value? A: 30-45 days per centimeter lengthened - the time required in frame during consolidation phase before safe removal. Children 30 days/cm, adults 40-45 days/cm.
Q: Why is corticotomy preferred over osteotomy in distraction osteogenesis? A: Preserves endosteal blood supply which provides 70-80% of bone blood flow. Multiple drill holes connected with osteotome maintains medullary contents and stem cells critical for regeneration.
Q: What is Ilizarov's tension-stress law? A: Gradual controlled traction on living tissues creates mechanical stress that stimulates and maintains regeneration of bone, soft tissues, nerves, and blood vessels. Foundation principle of distraction osteogenesis.
Q: What radiographic criterion indicates safe frame removal? A: Three of four cortices visible on AP and lateral radiographs, along with consolidation index of 30-45 days/cm. Fourth cortex matures after removal.
At a Glance
Distraction osteogenesis is based on Ilizarov's tension-stress law: gradual controlled traction stimulates regeneration of bone, soft tissues, nerves, and vessels. The process follows four phases: latency (5-7 days post-corticotomy allowing hematoma formation), distraction (lengthening at 1mm/day in 4 increments of 0.25mm), consolidation (30-45 days per cm lengthened, approximately 3× distraction time), and remodeling. A corticotomy (multiple perforations) preserves the endosteal blood supply unlike a complete osteotomy. Critical principle: rate and rhythm matter—too fast causes fibrous non-union, too slow causes premature consolidation. Blood flow increases 2-3× during distraction. The technique enables limb lengthening, deformity correction, bone transport, and nonunion treatment.
LDCRFour Phases of Distraction Osteogenesis
Hook:Like Drawing out taffy - Latency lets it set, Distraction pulls it apart, Consolidation hardens it, Remodeling perfects it!
STABLESPrinciples of Distraction Osteogenesis (Ilizarov)
Hook:STABLES - Like a horse in a stable, the bone needs stability and careful nurturing to grow!



Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“Examiner asks: Describe the biological principles of distraction osteogenesis and the phases involved.”
“You are lengthening a 12-year-old's femur for limb length discrepancy. At 3 weeks of distraction (21mm gained), radiographs show a widening radiolucent gap with minimal bone formation. What is your assessment and management?”
“A 15-year-old needs 4 cm of femoral lengthening for a post-traumatic discrepancy with no angular or rotational deformity. The family asks whether they really need an external frame. How do you decide, and how do you counsel them?”
Key Principles (Ilizarov)
- Tension-stress law = gradual traction stimulates regeneration
- Stable fixation with rigid external frame
- Corticotomy (not osteotomy) preserves endosteal blood supply
- Low-energy surgical technique respects biology
Four Phases Timeline
- Latency: 5-7 days (hematoma formation)
- Distraction: 1mm/day in 4 increments (bone regeneration)
- Consolidation: 30-45 days/cm (mineralization)
- Remodeling: months-years (cortical maturation)
Critical Parameters
- Rate: 1mm per day total
- Rhythm: 4 increments of 0.25mm (every 6 hours)
- Consolidation index: 30-45 days per cm
- Three cortices visible before frame removal
Troubleshooting
- Too fast distraction = fibrous non-union (radiolucent gap)
- Too slow distraction = premature consolidation
- Poor regenerate = pause 3-5 days, slow to 0.5mm/day
- Nerve symptoms = slow to 0.75mm/day or pause
Biological Responses
- Bone: intramembranous ossification (no cartilage)
- Blood flow: increases 2-3x during distraction
- Nerves: tolerate 1-2mm/day gradual elongation
- Soft tissues: muscle sarcomeres added, vessels elongate
Evidence Base
Tension-Stress Part II: Rate 1mm/day in 4 Steps Optimal
- Canine tibial study of rates (0.5, 1.0, 2.0 mm/day) and frequencies (1, 4, 60 steps/day)
- 0.5 mm/day frequently caused premature consolidation
- 2.0 mm/day produced undesirable changes within elongating tissues
- 1.0 mm/day gave the best regenerate; higher frequency improved outcome at any given rate
- Regenerate forms as a physis-like central growth zone with parallel bone columns
Tension-Stress Part I: Stability and Soft-Tissue Preservation
- Canine tibial experiments varying fixation stability and preservation of periosteum/marrow/medullary blood supply
- Both greater fixator stability and maximal soft-tissue preservation enhanced bone formation
- New bone forms parallel to the tension vector, even with lateral (perpendicular) distraction
- Damage to bone marrow inhibited osteogenesis, confirming the role of marrow elements
- Established the biological rationale for low-energy corticotomy over osteotomy
Blood Flow Surges During Distraction Osteogenesis
- Ten dogs, tibial lengthening, technetium scintigraphy quantifying regional blood flow
- Flow at the distraction site rose to nearly 10x control, peaking at 2 weeks
- Settled to 4-5x control through the rest of distraction, then 2-3x during consolidation
- Distal tibia (away from the gap) showed a similar amplitude and pattern of increased flow
- Supports Ilizarov's idea that distraction can heal hypovascular nonunions and osteomyelitis
Problems, Obstacles and Complications Classification
- 46 patients, 60 limb segments lengthened (mean 5.6 cm, range 1-16 cm)
- Difficulties classified as problems (no surgery), obstacles (surgery to resolve), and true complications
- 27 true complications; original goals achieved in 57 of 60 segments; satisfaction 94%
- Defined complication spectrum: contracture, subluxation, axial deviation, nerve/vessel injury, premature/delayed consolidation, nonunion, pin-site, hardware failure, refracture
- Lengthening index roughly one month/cm for single-level lengthening without deformity
Systematic Review of Optimal Distraction Protocols
- Systematic review of single-variable distraction studies (PubMed 1973-2007)
- 1 mm/day confirmed as the optimal rate (halved in very small animals such as rats)
- A continuous rhythm gave better regenerate than intermittent distraction
- Recommended consolidation period of 6-8 weeks for craniofacial models
- A latency period may not be mandatory in all settings
Magnetic Intramedullary Nail (PRECICE 2) Lengthening
- Multicentre retrospective series, 26 paediatric patients, 26 nails (21 femur, 5 tibia)
- Mean achieved lengthening 44.4 mm versus 49.4 mm goal
- Nail accuracy 91.1% and reliability 88.5%
- Distraction index 11.9 days/cm and consolidation index 25.1 days/cm
- Low complication burden but watch for joint subluxation and mechanical failure