Anaerobic Glycolysis | Matrix Turnover | Mechanotransduction | Catabolic-Anabolic Balance
- Chondrocytes rely on anaerobic glycolysis (95% of ATP) due to avascular nature
- Oxygen tension 1-5% in deep zones; hypoxia induces HIF pathway
- Diffusion from synovial fluid limits cartilage thickness to 1-2mm
- Matrix turnover slow: collagen II half-life 10-15 years, aggrecan 3-24 years
- Mechanical loading essential: cyclic compression enhances metabolism
- “Chondrocytes in OA switch to catabolic phenotype (MMPs up, TIMP down)
- “Glucose transporter GLUT-1 critical for anaerobic metabolism
- “IL-1 and TNF-alpha are major catabolic cytokines
- “Hydrostatic pressure and shear stress activate mechanoreceptors
95% of energy from glycolysis due to avascular cartilage. Chondrocytes adapted to low oxygen (1-5% in deep zones). Glucose is primary fuel source via GLUT-1 transporter.
Nutrients diffuse from synovial fluid and subchondral bone. Maximum diffusion distance limits cartilage to 1-2mm thickness in adults. Mechanical loading enhances nutrient transport.
Slow turnover: collagen II half-life 10-15 years. Aggrecan turnover faster (3-24 years) but still slow. Limited repair capacity due to low metabolic rate.
Mechanical loading regulates metabolism. Cyclic compression enhances matrix synthesis. Static compression or excessive load induces catabolism. Integrins and primary cilium are mechanosensors.
Overview
Chondrocytes are the sole cell type in articular cartilage, responsible for synthesizing and maintaining the extensive extracellular matrix. Despite comprising only 1-2% of tissue volume, they maintain a matrix 50-100 times their own volume through continuous metabolic activity.
The cartilage environment presents unique challenges: avascularity necessitates anaerobic metabolism, limited diffusion constrains tissue thickness, and absence of nerves eliminates pain signals from early damage. Chondrocytes have adapted specialized metabolic pathways to function in this hypoxic, avascular, aneural niche.
Understanding chondrocyte metabolism explains why cartilage has limited repair capacity (slow matrix turnover), why injuries are often asymptomatic initially (aneural), and why loading patterns affect joint health (mechanotransduction). It guides treatment strategies including activity modification, viscosupplementation, and emerging biologics.
- Superficial: Flat cells, collagen parallel to surface
- Middle: Round cells, oblique collagen fibers
- Deep: Columns perpendicular to surface
- Calcified: Interface with subchondral bone
- Avascular: No blood supply after skeletal maturity
- Aneural: No pain fibers (silent injuries)
- Alymphatic: No lymphatic drainage
- Low cell density: 1-2% volume, widely separated cells

Physiology and Core Concepts
Anaerobic Glycolysis
Chondrocytes derive 95% of their ATP from anaerobic glycolysis (Embden-Meyerhof pathway) rather than oxidative phosphorylation. This adaptation reflects the low oxygen environment of cartilage.
Oxygen Tension Gradient:
- Synovial fluid/superficial zone: 5-10% O2
- Middle zone: 3-5% O2
- Deep zone: 1-3% O2 (hypoxic)
- Calcified zone: Under 1% O2
- ATP Yield
- 2 ATP per glucose
- Usage in Chondrocytes
- 95% of energy production
- Advantage in Cartilage
- Functions in hypoxia
- ATP Yield
- 36 ATP per glucose
- Usage in Chondrocytes
- 5% of energy production
- Advantage in Cartilage
- Efficient but needs O2
- ATP Yield
- Variable
- Usage in Chondrocytes
- Emergency energy reserve
- Advantage in Cartilage
- Rapid mobilization
Glucose Transport:
- GLUT-1 transporter on chondrocyte membrane
- Insulin-independent glucose uptake
- Facilitated diffusion from synovial fluid
- Rate-limiting step in energy production
This glucose reliance is a hallmark of chondrocyte metabolism.
Diabetes affects cartilage metabolism: Altered glucose homeostasis and advanced glycation end products (AGEs) impair chondrocyte function. Diabetic patients have higher OA rates partly due to metabolic dysfunction.
Oxidative Stress and Mitochondrial Dysfunction
The catabolic cascade names iNOS as an IL-1-induced enzyme and the controversies section flags mitochondrial dysfunction in OA, but the redox arm of chondrocyte metabolism - which is, after all, a metabolism topic - is never developed. It is the link between the cell's energy machinery and matrix breakdown.
Reactive oxygen and nitrogen species (ROS/RNS). Even though chondrocytes are mainly glycolytic, they retain functional mitochondria that generate ROS, and inflammatory signalling (IL-1beta, TNF-alpha) induces inducible nitric oxide synthase (iNOS/NOS2), producing large amounts of nitric oxide (NO). NO combines with superoxide to form peroxynitrite, a potent oxidant. At physiological levels ROS act as signalling molecules; in excess they overwhelm the antioxidant defences (superoxide dismutase, catalase, glutathione) and become catabolic:
- Source
- iNOS, induced by IL-1beta/TNF-alpha
- Catabolic effect
- Inhibits aggrecan and collagen II synthesis, activates MMPs, and promotes chondrocyte apoptosis
- Source
- Dysfunctional mitochondria; NADPH oxidases
- Catabolic effect
- Oxidise matrix and proteins, activate catabolic MAPK/NF-kappaB signalling, drive senescence
- Source
- NO + superoxide
- Catabolic effect
- Strong oxidant causing protein nitration and cell death
- Source
- Constitutive
- Catabolic effect
- Protective; their decline with age tips the balance toward catabolism
The mitochondrial link. With ageing and in OA, mitochondrial function declines (reduced respiratory-chain activity, mitochondrial DNA damage), which raises ROS output, lowers the reserve capacity for oxidative ATP, and promotes chondrocyte senescence and apoptosis. This is why the "purely anaerobic" textbook line is a simplification - the mitochondria matter most not for routine ATP but as a source of damaging ROS and a driver of age-related catabolism, connecting ageing, oxidative stress and the senescent (SASP) phenotype.
Chondrocytes are glycolytic for ATP but still hold mitochondria - and in OA those mitochondria, plus IL-1-induced iNOS-derived nitric oxide, generate ROS/RNS that inhibit matrix synthesis, activate MMPs and drive apoptosis and senescence. Falling antioxidant defences with age tip the balance. This redox axis is the metabolic bridge between ageing, mitochondrial dysfunction and the catabolic OA phenotype.
CAGEMajor Matrix Components Synthesized
Hook:Chondrocytes live in a CAGE of collagen and aggrecan!
Matrix Turnover and Regulation
Anabolic Pathways
Chondrocytes continuously synthesize extracellular matrix components to maintain cartilage structure and function.
- Growth factors: IGF-1, TGF-beta, BMPs
- Mechanical signals: Cyclic compression, hydrostatic pressure
- Transcription factors: SOX9, RUNX2 (early stages)
- Anti-inflammatory: IL-4, IL-10, IL-13
- Collagen II: Synthesized in RER, secreted as procollagen, cleaved extracellularly.
- Aggrecan: Core protein + GAG addition in Golgi, secreted and aggregated with hyaluronan.
- Minor collagens: IX, XI (regulate fibril formation), VI (pericellular matrix).
Collagen II Synthesis and Assembly
SOX9 activates COL2A1 gene. mRNA transcribed and processed. Exported to rough endoplasmic reticulum.
Pro-alpha chains synthesized on ribosomes. Hydroxylation of proline and lysine residues (requires vitamin C). Glycosylation occurs.
Three pro-alpha1(II) chains align via C-propeptides. Triple helix formation proceeds from C to N terminus. Procollagen secreted.
N and C propeptides cleaved by specific proteinases. Collagen molecules self-assemble into fibrils. Cross-linking by lysyl oxidase stabilizes.
Chondrocyte Hypertrophy and the Endochondral Programme in OA
The OnePager lists "hypertrophic" as a chondrocyte metabolic state and the phenotype table flags RUNX2, collagen X and the "tidemark advance", but the actual hypertrophic programme - and why it matters in osteoarthritis - is never developed. It is a favourite basic-science link between development and disease.
The hypertrophic programme. Terminal (hypertrophic) differentiation is the normal end-point of the growth-plate chondrocyte, driven by a switch in transcription factors away from SOX9 and toward RUNX2 (and MEF2C). The hypertrophic chondrocyte enlarges and switches its matrix output:
- Resting / anabolic chondrocyte
- SOX9 (with SOX5/6)
- Hypertrophic chondrocyte
- RUNX2, MEF2C; SOX9 falls
- Resting / anabolic chondrocyte
- Collagen II
- Hypertrophic chondrocyte
- Collagen X (a hypertrophy marker)
- Resting / anabolic chondrocyte
- Aggrecan, collagen II
- Hypertrophic chondrocyte
- Alkaline phosphatase, MMP-13, VEGF
- Resting / anabolic chondrocyte
- Maintained, resilient
- Hypertrophic chondrocyte
- Mineralised; vascular invasion and replacement by bone
Why it matters in OA. Healthy articular chondrocytes are normally held in a stable, non-hypertrophic state - they resist this terminal programme for life. In osteoarthritis they abnormally re-activate the endochondral/hypertrophic programme: RUNX2 rises, collagen X and MMP-13 appear, alkaline phosphatase and VEGF promote calcification and vascular invasion, and the result is tidemark duplication and advance, thickening of the calcified-cartilage layer, and osteophyte formation. In effect the OA articular chondrocyte "recapitulates endochondral ossification" - the same process that builds the growth plate, now driving joint destruction. (The developmental detail of the growth plate itself is covered in physis-growth-plate-anatomy and ossification-intramembranous-endochondral; here the focus is the metabolic phenotype switch.)
Articular chondrocytes normally resist hypertrophy for life. In OA they re-run the endochondral programme: a SOX9 → RUNX2 switch turns on collagen X, MMP-13, alkaline phosphatase and VEGF, causing matrix calcification, vascular invasion, tidemark advance and osteophytes. "OA chondrocytes recapitulate endochondral ossification" is the one-line answer.
SUBSChondrocyte Nutrient Sources
Hook:Cartilage gets nutrition from SUBS-titutes for blood vessels!
Mechanotransduction
Mechanical loading is a critical regulator of chondrocyte metabolism. Physiological loading maintains cartilage health; abnormal loading contributes to degeneration.
Mechanosensors
Chondrocytes detect mechanical stimuli through multiple mechanisms:
- Primary Cilium: Solitary non-motile organelle projects from cell surface. Bends with matrix deformation.
- Integrins: Link cytoskeleton to matrix. Alpha5-beta1 (fibronectin) and alpha10-beta1 (collagen II).
- Ion Channels: Mechanosensitive calcium channels (Piezo1, Piezo2).
Load-Dependent Responses
- Metabolic Effect
- Anabolic
- Matrix Response
- Increased synthesis
- Clinical Example
- Normal daily activity
- Metabolic Effect
- Anabolic
- Matrix Response
- Enhanced proteoglycan
- Clinical Example
- Swimming, water therapy
- Metabolic Effect
- Catabolic
- Matrix Response
- Increased MMPs
- Clinical Example
- Prolonged standing, obesity
- Metabolic Effect
- Catabolic
- Matrix Response
- Matrix breakdown
- Clinical Example
- Running on concrete, trauma
- Metabolic Effect
- Catabolic
- Matrix Response
- Atrophy
- Clinical Example
- Casting, bed rest
Optimal Loading:
- Moderate cyclic compression (10-15% strain)
- Frequency 0.5-1 Hz approximates walking
- Enhances matrix synthesis and nutrient transport
- Activates anabolic signaling pathways
This explains why moderate exercise is protective for cartilage while both excessive loading and immobilization are detrimental.
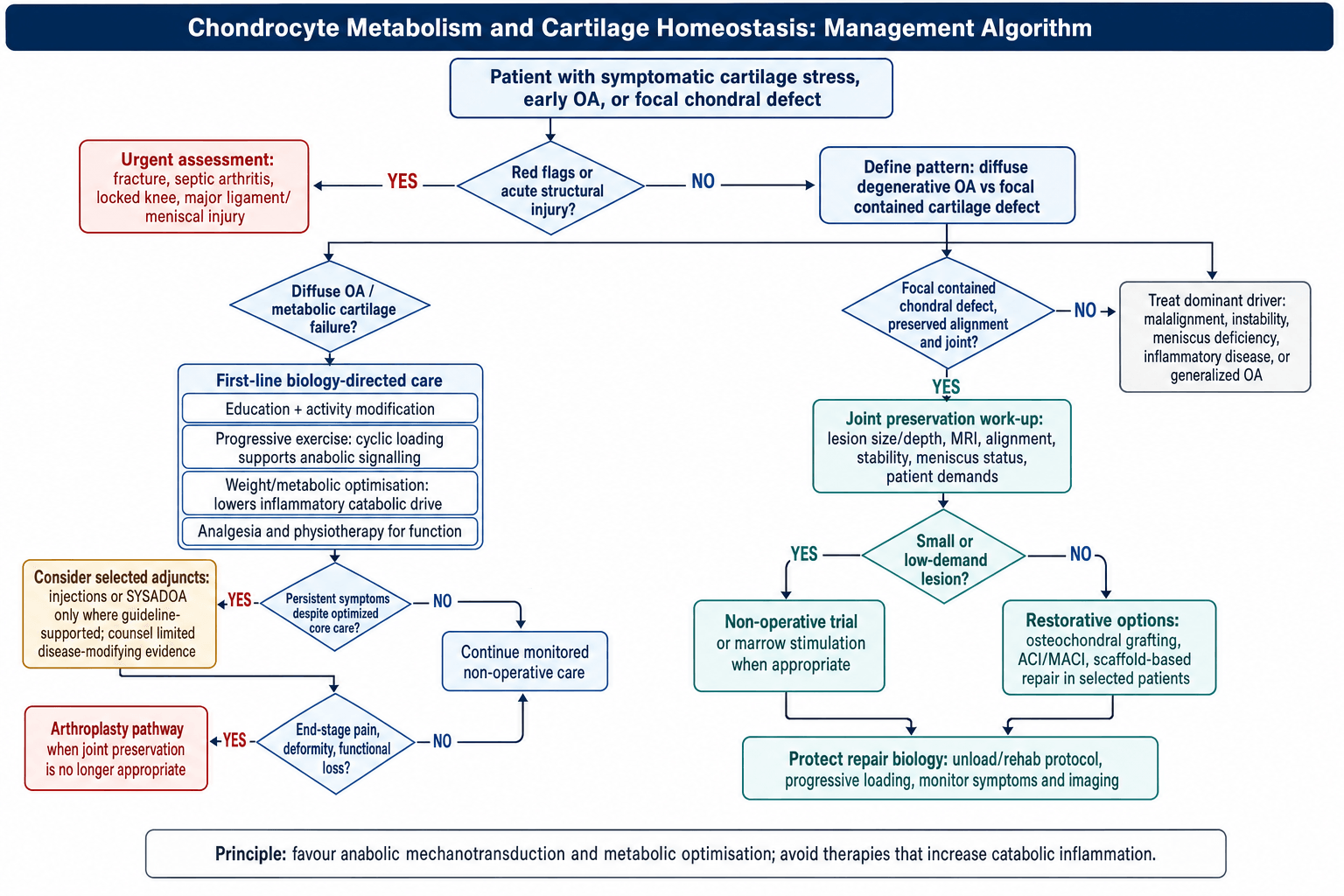
Management Algorithm
Clinical Relevance
Osteoarthritis Pathophysiology
OA represents a shift toward catabolic metabolism with failed attempts at repair.
Metabolic Changes in OA:
- Increased MMP-13 and ADAMTS expression.
- Decreased TIMP (protease inhibitors).
- Elevated IL-1beta and TNF-alpha.
- Attempted anabolic response (clusters of cells).
- Progression to chondrocyte apoptosis.
The vicious cycle of OA: Mechanical injury → Cell damage → IL-1beta release → MMP upregulation → Matrix degradation → Abnormal loading → More injury. Breaking this cycle is the goal of disease-modifying OA drugs (none currently approved).
Therapeutic Targets
Understanding chondrocyte metabolism guides therapeutic strategies:
- Viscosupplementation: Hyaluronic acid injections to improve lubrication and potentially stimulate endogenous production.
- Corticosteroids: Potent anti-inflammatory effect but can inhibit chondrocyte metabolism if used frequently.
- PRP (Platelet Rich Plasma): Delivers anabolic growth factors (TGF-beta, IGF-1) to shift balance.
- Future Targets: Senolytics (removing senescent cells), Wnt pathway inhibitors, aggrecanase (ADAMTS5) inhibitors.
Distinguishing Chondrocyte Metabolic States
A common viva and MCQ task is to separate the chondrocyte phenotypes that dominate in health, ageing and disease. Each has a characteristic transcription factor profile, matrix output and clinical correlate.
- Key Drivers
- SOX9, IGF-1, balanced load
- Matrix Effect
- Synthesis = degradation
- Markers
- Collagen II, aggrecan
- Clinical Correlate
- Healthy adult cartilage
- Key Drivers
- TGF-beta, BMP, cyclic load
- Matrix Effect
- Synthesis greater than degradation
- Markers
- Increased proteoglycan
- Clinical Correlate
- Early loading response, immature cartilage
- Key Drivers
- IL-1beta, TNF-alpha, static/impact load
- Matrix Effect
- Degradation greater than synthesis
- Markers
- MMP-13, ADAMTS-5, low TIMP
- Clinical Correlate
- Progressive osteoarthritis
- Key Drivers
- RUNX2, MMP-13, Wnt, low SOX9
- Matrix Effect
- Calcification, collagen X
- Markers
- Collagen X, alkaline phosphatase
- Clinical Correlate
- Growth plate, OA tidemark advance
- Key Drivers
- Ageing, oxidative stress, DNA damage
- Matrix Effect
- Catabolic secretome
- Markers
- p16INK4a, IL-6, MMPs
- Clinical Correlate
- Age-related OA; senolytic target
Guidelines, Registries & Global Practice
The clinical relevance of chondrocyte metabolism is realised through osteoarthritis and cartilage-repair practice. The biology is universal, but how it is translated into guidelines and procedures varies worldwide.
Global Epidemiology
- Osteoarthritis affects an estimated 595 million people worldwide (Global Burden of Disease 2021), making it a leading global cause of disability in older adults.
- The knee is the most commonly affected large joint; prevalence rises sharply with age and obesity.
- Burden is rising fastest in low- and middle-income countries as populations age and obesity increases.
Society Guidance Drawing on Cartilage Biology
- Position on Core OA Biology-Linked Therapies
- Core: exercise, weight loss, education; conditional pharmacology
- Notable Stance
- Strong emphasis on load and metabolic optimisation
- Position on Core OA Biology-Linked Therapies
- Strong evidence for exercise and weight loss; HA injections not recommended for routine knee OA
- Notable Stance
- Skeptical of viscosupplementation
- Position on Core OA Biology-Linked Therapies
- Therapeutic exercise as first-line; advises against intra-articular HA
- Notable Stance
- Does not endorse hyaluronic acid
- Position on Core OA Biology-Linked Therapies
- Stepwise algorithm; supports symptomatic slow-acting drugs (SYSADOA) in some patients
- Notable Stance
- More permissive of glucosamine/chondroitin
There is broad international agreement that mechanical and metabolic optimisation (exercise, weight loss) is first-line because it directly targets the anabolic loading biology described above. Divergence centres on injectables and symptomatic slow-acting agents.
Registries & Cartilage-Repair Practice
- No major registry tracks chondrocyte biology directly, but joint replacement registries (NJR, AJRR, AOANJRR, SHAR, NZJR) record the end-stage of failed cartilage homeostasis and benchmark arthroplasty outcomes.
- Cartilage-repair registries (e.g. the German cartilage registry KnorpelRegister DGOU) capture outcomes of biologically driven procedures such as autologous chondrocyte implantation (ACI) and matrix-assisted ACI (MACI).
High- vs Limited-Resource Practice Variation
- High-resource settings: access to cell-based cartilage repair (ACI/MACI), osteochondral grafting and PRP; structured weight-loss and exercise programmes.
- Limited-resource settings: management is dominated by activity modification, analgesia and physiotherapy, with earlier reliance on arthroplasty once available because biologic repair options are scarce or unaffordable.
- Universal, low-cost interventions (exercise, weight management) carry the strongest evidence and are equitable globally.
Controversies & Areas of Uncertainty
Several long-standing debates in cartilage biology remain unresolved and are favourite examiner territory because they reward candidates who can argue both sides.
The textbook "95% glycolytic" figure is a simplification. Chondrocytes possess functional mitochondria and basal oxidative phosphorylation persists, but ATP yield is dominated by glycolysis. Mitochondrial dysfunction is increasingly implicated in OA, so the picture is more nuanced than "purely anaerobic".
Mechanical malalignment and metabolic/inflammatory drivers (obesity, IL-1, AGEs, metabolic syndrome) are not mutually exclusive. The dominant view (Loeser 2012) is that mechanical injury and low-grade inflammation converge on a final common catabolic chondrocyte pathway.
Despite compelling animal data (e.g. ADAMTS5 knockout), human aggrecanase, MMP and IL-1 inhibitor trials have not delivered approved disease-modifying drugs. Heterogeneous OA phenotypes, late presentation and the slow matrix turnover that blunts measurable response are leading explanations.
Clearing p16-positive senescent cells reduced OA in animal models, but a phase 2 intra-articular senolytic (UBX0101) failed to meet its primary endpoint, tempering early enthusiasm. Whether senescence is cause or consequence remains debated.
MCQ Practice Points
Q: What percentage of chondrocyte ATP comes from anaerobic glycolysis? A: 95% - Chondrocytes rely predominantly on glycolysis due to the avascular, hypoxic environment of cartilage. Only 5% comes from oxidative metabolism.
Q: Which glucose transporter is critical for chondrocyte energy metabolism? A: GLUT-1 - Insulin-independent facilitated diffusion transporter that allows glucose uptake from synovial fluid in the avascular cartilage.
Q: What is the major catabolic cytokine driving cartilage degradation in osteoarthritis? A: Interleukin-1 beta (IL-1beta) - Upregulates MMP-13 and ADAMTS-4/5, downregulates matrix synthesis, and shifts chondrocytes to catabolic phenotype via NF-kappaB pathway.
Q: What is the half-life of collagen type II in articular cartilage? A: 10-15 years - Extremely slow turnover explains limited repair capacity. Aggrecan turnover is faster (3-24 years) but still slow.
Q: Which organelle serves as the primary mechanosensor in chondrocytes? A: Primary Cilium - A solitary, non-motile cilium that projects into the matrix and deflects with load, triggering intracellular signaling.
Q: Which transcription factor is stabilized by the hypoxic environment of cartilage? A: HIF-1alpha - Hypoxia-Inducible Factor 1-alpha plays a critical role in chondrocyte survival and anabolic function under low oxygen conditions.


Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“Examiner asks: Explain how chondrocytes generate energy given the avascular nature of cartilage.”
“A patient asks why you recommend moderate exercise for their early knee osteoarthritis, given that loading damages cartilage.”
“An examiner asks you to explain, at the cellular level, why articular cartilage is lost in osteoarthritis and why we still have no disease-modifying drug.”
Energy Metabolism
- **Glycolysis**: 95% of ATP (Anaerobic)
- **Glucose Transport**: GLUT-1 (Insulin independent)
- **Hypoxia**: HIF-1alpha regulates survival
Nutrition
- **Source**: Synovial fluid diffusion
- **Limit**: 1-2mm thickness
- **Enhancer**: Cyclic pumping action
Matrix Regulation
- **Anabolic**: TGF-beta, IGF-1, SOX9
- **Catabolic**: IL-1, TNF-alpha, MMP-13
- **Mechanosensor**: Primary Cilium, Integrins
Evidence Base
Chondrocyte Energy Metabolism Is Glucose-Driven, Not Oxygen-Driven
- Bovine chondrocytes in agarose monitored for glucose/oxygen uptake and lactate output
- Lactate production predictable from glucose alone; oxygen tension did not influence lactate output
- Confirms anaerobic glycolysis is the dominant ATP pathway in chondrocytes
- Glucose availability, not oxygen, is the rate-limiting substrate for metabolism
HIF-1alpha Drives Anaerobic Glycolysis and Matrix Synthesis
- HIF-1alpha-null epiphyseal chondrocytes cannot maintain ATP under hypoxia
- HIF-1alpha is required for glycolysis under both aerobic and anaerobic conditions
- Loss of HIF-1alpha reduces aggrecan and collagen II mRNA and protein under low oxygen
- Links the hypoxic niche directly to extracellular matrix production
References
-
Sengers BG, Heywood HK, Lee DA, et al. Nutrient utilization by bovine articular chondrocytes. J Biomech Eng. 2005. PMID 16248305.
-
Pfander D, Cramer T, Schipani E, Johnson RS. HIF-1alpha controls extracellular matrix synthesis by epiphyseal chondrocytes. J Cell Sci. 2003. PMID 12665562.
-
Grodzinsky AJ, Levenston ME, Jin M, Frank EH. Cartilage tissue remodeling in response to mechanical forces. Annu Rev Biomed Eng. 2000. PMID 11701528.
-
Fitzgerald JB, Jin M, Dean D, Grodzinsky AJ, et al. Mechanical compression of cartilage explants induces multiple time-dependent gene expression patterns. J Biol Chem. 2004. PMID 14960571.
-
Goldring MB. The role of the chondrocyte in osteoarthritis. Arthritis Rheum. 2000. PMID 11014341.
-
Glasson SS, Askew R, Sheppard B, Morris EA, et al. Deletion of active ADAMTS5 prevents cartilage degradation in a murine model of osteoarthritis. Nature. 2005. PMID 15800624.
-
Lee W, Leddy HA, Guilak F, Liedtke W, et al. Synergy between Piezo1 and Piezo2 channels confers high-strain mechanosensitivity to articular cartilage. Proc Natl Acad Sci USA. 2014. PMID 25385580.
-
Loeser RF, Goldring SR, Scanzello CR, Goldring MB. Osteoarthritis: a disease of the joint as an organ. Arthritis Rheum. 2012. PMID 22392533.