Ulnar-Sided Wrist Pain | Post-Traumatic | Salvage Procedures
- Articulation between ulnar head and sigmoid notch critical for forearm rotation
- Post-traumatic most common cause (distal radius malunion)
- Clinical triad: ulnar-sided pain, restricted rotation, DRUJ crepitus/instability
- Conservative first: activity modification, NSAIDs, splinting, injection
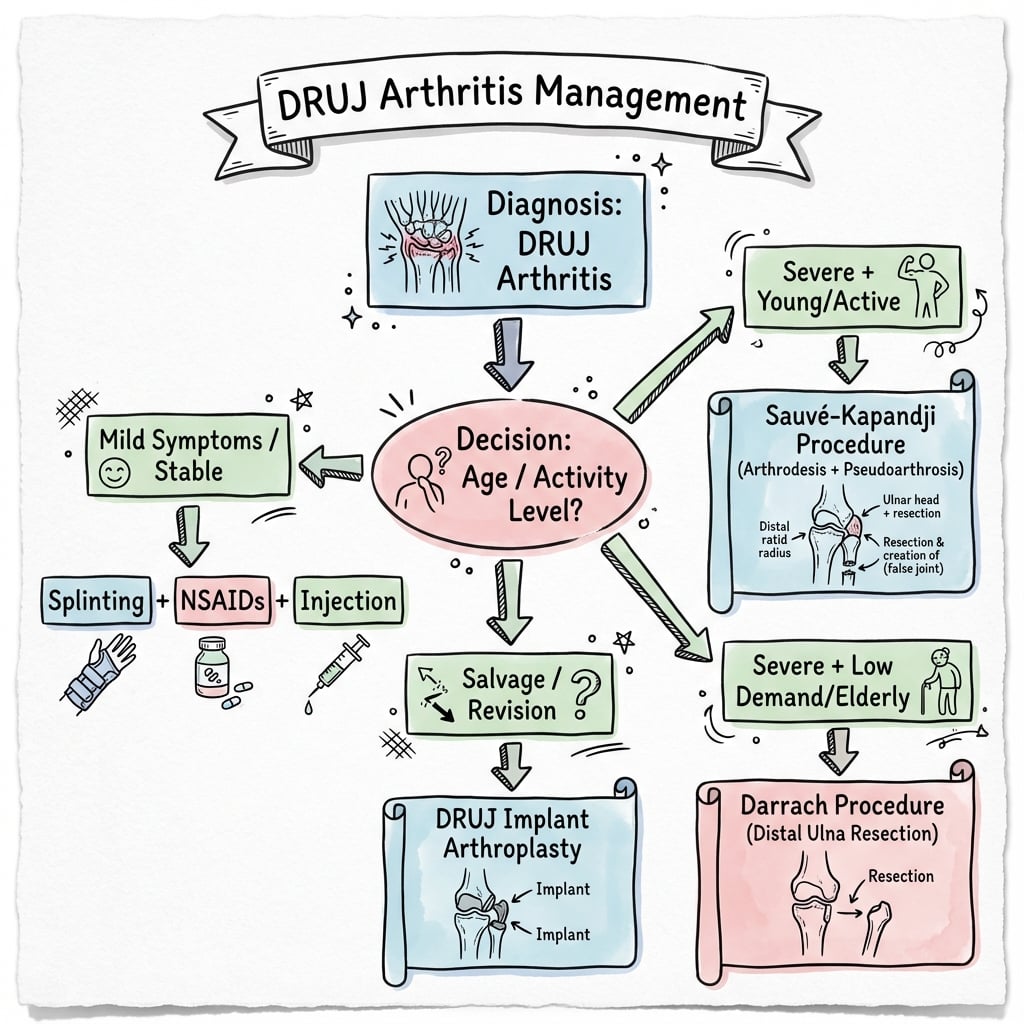
- Surgical: Darrach (elderly), Sauve-Kapandji (younger), hemiresection, arthroplasty
- “Piano key sign - dorsal displacement of ulnar head
- “CT best for sigmoid notch assessment
- “Always assess for TFCC tears, Essex-Lopresti injury
- “Know indications and complications for each salvage procedure
DRUJ Arthritis (Distal Radioulnar Joint Arthritis)
Core Exam Knowledge
- Anatomic basis: Articulation between ulnar head and sigmoid notch of radius, critical for forearm rotation
- Common etiology: Post-traumatic (80% - distal radius malunion most common), inflammatory arthritis, primary osteoarthritis
- Clinical triad: Ulnar-sided wrist pain, painful restricted forearm rotation, DRUJ crepitus and instability
- Investigation essentials: PA and lateral wrist radiographs, CT for sigmoid notch assessment, bilateral comparison views
- Conservative first-line: Activity modification, NSAIDs, splinting in neutral rotation, corticosteroid injection
- Surgical decision-making: Darrach (elderly, low-demand), Sauvé-Kapandji (younger, higher-demand), hemiresection (intermediate), DRUJ arthroplasty (selective cases)
Clinical Examination: DRUJ tenderness, pain with pronation/supination, piano key sign (dorsal displacement of ulnar head), grind test positive
Imaging: PA radiograph shows joint space narrowing and ulnar head deformity; CT best visualizes sigmoid notch arthrosis and subluxation
Etiology Recognition: Always assess for distal radius malunion, TFCC tears, Essex-Lopresti injury, inflammatory arthropathy
Surgical Options: Know indications and complications for Darrach, Sauvé-Kapandji, hemiresection-interposition, and DRUJ prosthesis
Incidence and Causes
Incidence and Risk Factors
The condition affects adults across all age groups but is most common in the fifth through seventh decades. Male predominance is noted in post-traumatic cases (reflecting higher trauma incidence), while inflammatory arthropathy cases show female predominance. Occupational risk factors include repetitive forceful gripping with forearm rotation (mechanics, carpenters, assembly workers) and prior wrist trauma (athletes, manual laborers).
Pathophysiology
The DRUJ is a diarthrodial articulation critical for forearm rotation. The ulnar head (convex) articulates with the sigmoid notch of the radius (concave), with stability provided by the triangular fibrocartilage complex (TFCC), dorsal and volar radioulnar ligaments, interosseous membrane, and joint capsule. Normal forearm rotation requires congruent articular surfaces, intact ligamentous support, and balanced muscle forces.
Dorsal-volar instability of the ulnar head. Indicates DRUJ incompetence.
Ulnar Stump Instability. Avoid Darrach in young/high-demand patients. Use Sauvé-Kapandji instead.
Ulnar Variance. Must be measured on PA view in Neutral Rotation (Pronation increases positive variance).
Anatomy
DRUJ Anatomy
- Ulnar head (convex) articulates with sigmoid notch of radius (concave)
- Sigmoid notch covers only 60-80 degrees of ulnar head circumference
- Ulnar head sits slightly palmar and ulnar to radius
- TFCC (Triangular Fibrocartilage Complex) - primary stabilizer
- Dorsal and palmar radioulnar ligaments
- Interosseous membrane (central band most important)
- Joint capsule and pronator quadratus
- Function
- Concave radial surface for DRUJ
- Clinical Relevance
- Arthritis affects notch cartilage, assess on CT
- Function
- Convex articulation, pivot for rotation
- Clinical Relevance
- Excision (Darrach) or replacement options
- Function
- Primary DRUJ stabilizer
- Clinical Relevance
- Injury leads to instability then arthritis
- Function
- Resists palmar translation in supination
- Clinical Relevance
- Assess stability preoperatively
- Function
- Resists dorsal translation in pronation
- Clinical Relevance
- Key for surgical reconstruction
Staging and Associated Pathology
Staging by Etiology
DRUJ arthritis is staged by etiology to guide treatment. Post-traumatic arthritis (most common) results from distal radius malunion, intra-articular fracture, chronic DRUJ instability, or Essex-Lopresti injury. Inflammatory arthritis includes rheumatoid arthritis (often bilateral with synovitis and bone erosion), psoriatic arthritis, and crystalline arthropathy. Primary osteoarthritis occurs without clear antecedent trauma and is less common. Neuromuscular causes include cerebral palsy and other spasticity disorders with chronic abnormal forces.
Severity Grading
- radiographic
- Mild joint space narrowing, minimal sclerosis
- symptoms
- Intermittent pain, mild rotation loss
- treatment
- Conservative management, activity modification
- radiographic
- Obvious joint space loss, sclerosis, osteophytes
- symptoms
- Regular pain with activities, 30-40% rotation loss
- treatment
- Conservative trial, surgical if failed
- radiographic
- Severe space loss, cysts, deformity, instability
- symptoms
- Constant pain, severe rotation limitation greater than 50%
- treatment
- Surgical reconstruction typically required
- radiographic
- Bone-on-bone, subluxation, ulnar head destruction
- symptoms
- Severe pain and instability, minimal function
- treatment
- Salvage procedure essential
Viva Examination Review
Clinical Examination
- Ulnar-sided wrist pain, worse with rotation
- Difficulty with doorknobs, screwdrivers, wringing towels
- Previous trauma (distal radius fracture most common)
- Inflammatory arthritis history
- DRUJ tenderness (dorsally and ulnarly)
- Crepitus with forearm rotation
- Reduced pronation/supination (quantify loss)
- Piano key sign (dorsal-volar instability)
- DRUJ grind test (axial load with rotation)
- Technique
- Push ulnar head dorsally to volarly
- Positive Finding
- Increased dorsal prominence, reducible
- Significance
- DRUJ instability
- Technique
- Axial load through ulna with rotation
- Positive Finding
- Pain and crepitus
- Significance
- DRUJ arthritis
- Technique
- Stabilize radius, translate ulna
- Positive Finding
- Increased translation vs contralateral
- Significance
- DRUJ instability
- Technique
- Tenderness at ulnar fovea (between FCU and ulnar styloid)
- Positive Finding
- Point tenderness
- Significance
- TFCC foveal tear
Radiographic Workup
Radiographic Evaluation
Standard wrist radiographs (PA, lateral, oblique) form the initial imaging assessment. PA view demonstrates joint space narrowing at the DRUJ, subchondral sclerosis, ulnar head deformity or flattening, and cystic changes in advanced cases. Assessment of ulnar variance is critical, as positive ulnar variance (ulnar head extends beyond radial articular surface) increases DRUJ loading and accelerates arthritis. Comparison with the contralateral uninjured wrist is valuable.
Advanced Imaging
Computed tomography (CT) is the gold standard for detailed assessment of DRUJ arthritis. CT clearly demonstrates sigmoid notch morphology and articular surface irregularity, ulnar head shape and arthrosis, degree of subluxation or dislocation, presence of loose bodies or osteophytes, and quality of bone stock for surgical planning. Bilateral CT with forearm in pronation, neutral, and supination allows assessment of dynamic stability and subluxation patterns.
Magnetic resonance imaging (MRI) evaluates soft tissue structures including TFCC integrity (central perforation, peripheral detachment), extensor carpi ulnaris (ECU) tendon pathology, interosseous membrane injury, and bone marrow edema indicating active arthritic process. MRI is particularly valuable when concomitant soft tissue pathology is suspected or when evaluating younger patients where TFCC repair might be considered.
Diagnostic Injection
Fluoroscopically guided DRUJ corticosteroid injection serves diagnostic and therapeutic purposes. Temporary complete pain relief confirms DRUJ arthritis as the primary pain generator, which is valuable when multiple potential sources exist (ulnar impaction syndrome, TFCC tears, ECU tendinopathy). The injection typically uses corticosteroid (triamcinolone 40mg) with local anesthetic (lidocaine or bupivacaine), injected into the DRUJ space under fluoroscopic guidance.
Viva Imaging Review
Imaging Protocol
- PA (neutral rotation) - assess ulnar variance
- True lateral - DRUJ alignment
- Oblique views if needed
- Sigmoid notch morphology and integrity
- Ulnar head changes
- Degree of subluxation
- Bone stock for surgical planning
- Key Findings
- Joint space narrowing, osteophytes, ulnar variance, subluxation
- When to Order
- All patients, first-line
- Key Findings
- Sigmoid notch detail, subluxation quantification, bone stock
- When to Order
- Preoperative planning, unclear diagnosis
- Key Findings
- TFCC integrity, soft tissue pathology, early arthritis
- When to Order
- TFCC suspected, soft tissue assessment
- Key Findings
- Confirms DRUJ as pain source
- When to Order
- Multiple pain sources, unclear diagnosis


Differential Diagnosis
Ulnar-sided wrist pain is one of the most difficult diagnostic regions in the hand. A diagnostic DRUJ injection that abolishes pain helps confirm the DRUJ as the true pain generator when several causes coexist.
- distinguishing
- Pain and crepitus on loaded rotation, positive grind test
- keyTest
- DRUJ grind, CT of sigmoid notch, diagnostic DRUJ injection
- pitfall
- Coexisting TFCC tear or ulnar impaction muddies the picture
- distinguishing
- Positive fovea sign, click on ulnocarpal stress, often stable DRUJ
- keyTest
- MR arthrogram, wrist arthroscopy
- pitfall
- Chronic foveal tears cause secondary instability then arthritis
- distinguishing
- Positive ulnar variance, lunate/triquetral cysts, pain on ulnar deviation
- keyTest
- PA in neutral rotation for variance, MRI marrow oedema
- pitfall
- Treat with ulnar shortening, not a DRUJ salvage procedure
- distinguishing
- Tenderness over ECU groove, painful snapping on supination
- keyTest
- ECU synergy test, dynamic ultrasound
- pitfall
- Mistaken for DRUJ instability; ECU sits dorsal to ulnar head
- distinguishing
- Pain on LT ballottement and shear, focal LT tenderness
- keyTest
- LT ballottement, fluoroscopy, arthroscopy
- pitfall
- Often coexists with TFCC and ulnar impaction (ulnocarpal abutment)
- distinguishing
- Volar-ulnar pain, tenderness over pisiform, pisotriquetral grind
- keyTest
- 30-degree supinated oblique radiograph, injection
- pitfall
- Pain is volar, not dorsal as in DRUJ disease
Management
Non-Operative Treatment
Non-steroidal anti-inflammatory drugs (NSAIDs) provide symptomatic relief. Topical NSAIDs may be preferred for patients with GI concerns. Splinting in neutral forearm rotation with a long arm splint or Muenster-type orthosis reduces symptoms by limiting rotation, worn during aggravating activities or at night. Custom thermoplastic splints can be fabricated by hand therapists.
Corticosteroid injection into the DRUJ provides temporary relief in 60-70% of patients, lasting weeks to months. Repeat injections may be performed but are generally limited to 2-3 per year. Physical therapy focuses on maintaining range of motion and strengthening forearm and wrist muscles to provide dynamic stability.
Indications for Surgery
Surgery is considered when conservative management fails to control symptoms after 3-6 months, pain significantly limits function or quality of life, progressive instability develops, or patients have high functional demands incompatible with conservative restrictions. Relative contraindications include active infection, severe osteoporosis (compromises fixation for Sauvé-Kapandji), unrealistic expectations, and significant medical comorbidities precluding surgery.
Surgical Options Overview
Darrach Procedure
The Darrach procedure involves excision of the distal ulna (typically 1.5-2.5cm of ulnar head and neck). The technique uses a dorsal or ulnar approach to the DRUJ, subperiosteal dissection to protect the TFCC remnant and ECU tendon, and transection of the ulna at an appropriate level (preserving adequate ulna for forearm function). Soft tissue stabilization with ECU tendon or TFCC remnant coverage of the ulnar stump reduces instability.
Indications for Darrach include elderly low-demand patients (age greater than 60 years), severe DRUJ arthritis with ulnar head destruction, rheumatoid arthritis with bone erosion, and revision of failed other procedures. Advantages include technical simplicity, reliable pain relief, and no implant-related complications. Disadvantages include ulnar stump instability (painful prominence of ulna with gripping), reduced grip strength (10-20% reduction), and cosmetic concerns (visible depression at DRUJ).
Postoperative management involves short arm splint for 2 weeks followed by progressive range of motion. Full activity is typically allowed at 6-8 weeks. Outcomes include good pain relief in 75-85% but with variable grip strength recovery and potential ulnar stump instability requiring subsequent soft tissue stabilization.
Sauvé-Kapandji Procedure
The Sauvé-Kapandji procedure creates a radioulnar fusion at the DRUJ level combined with an ulnar pseudarthrosis proximal to the fusion site. The technique involves exposure of the DRUJ, preparation of articular surfaces (radius sigmoid notch and ulnar head), fusion of radius to ulna in neutral rotation using K-wires or compression screw, and creation of a 1-1.5cm segment of ulna resection proximal to the fusion (allowing forearm rotation through the pseudarthrosis).
Postoperative management includes long arm cast or splint for 4-6 weeks until fusion is evident, followed by protected motion for 2-4 additional weeks. Full unrestricted activity is allowed at 3-4 months. Outcomes are generally excellent with 85-90% patient satisfaction, good pain relief, and maintained rotation (80-90% of contralateral side).
Hemiresection-Interposition Arthroplasty (Bowers)
The Bowers procedure involves resection of the ulnar head articular surface (removing approximately 50% of the head) with soft tissue interposition (typically palmaris longus autograft or allograft). The technique preserves the ulnar styloid and TFCC attachments while removing the arthritic ulnar head dome. Interposition material is secured between the remaining ulna and radius to prevent bone-on-bone contact and provide cushioning.
Indications include intermediate-age patients (45-65 years), moderate DRUJ arthritis with preserved ulnar styloid and TFCC, and patients desiring stability without fusion. Advantages include preservation of TFCC attachment providing stability, less extensive than Darrach (preserves more ulna), and maintained forearm rotation. Disadvantages include technically demanding, potential for inadequate resection with recurrent pain, and interposition material attenuation over time with symptom recurrence.
Outcomes are good to excellent in 70-80% of patients at short to intermediate term (2-5 years), with some reports of declining results at longer follow-up. The procedure serves as an intermediate option between conservative management and more extensive salvage procedures.
DRUJ Prosthetic Arthroplasty
DRUJ prosthetic replacement uses implants that reconstruct the ulnar head with a metal stem and articular component. Several designs exist including constrained (linked radius and ulna components) and unconstrained (ulnar head replacement only) systems. The procedure involves DRUJ exposure, excision of arthritic ulnar head, preparation of ulnar canal for stem, and implantation of the prosthesis with secure fixation.
Indications include younger patients with isolated DRUJ arthritis and intact TFCC, failed prior DRUJ procedures requiring revision, and high functional demands requiring maximal function preservation. Advantages include maintained DRUJ anatomy and stability, good forearm rotation, and potential for improved outcomes over ulnar head excision. Disadvantages include implant cost, risk of loosening or failure (10-15% at 5-10 years), polyethylene wear, and technical challenges with revision if needed.
Long-term outcome data is limited compared to established procedures like Darrach and Sauvé-Kapandji. The procedure is reserved for carefully selected patients in centers with expertise in DRUJ arthroplasty.
Management Algorithm
Surgical Technique
Key Surgical Techniques
- Dorsal approach between 5th and 6th compartments
- Subperiosteal exposure of distal ulna
- Excise 1.5-2.5 cm of distal ulna
- Soft tissue stabilization (ECU sling or capsular interposition)
- Close capsule and retinaculum
- Dorsal approach to DRUJ
- DRUJ fusion with lag screws (2 x 3.5mm or 4.0mm)
- Create 10mm pseudarthrosis proximal to fusion
- Soft tissue stabilization of proximal ulna stump
- Ulna Resection
- Distal 1.5-2.5 cm
- Key Technical Points
- Oblique cut, soft tissue stabilization critical
- Ulna Resection
- 10mm segment proximal to DRUJ
- Key Technical Points
- Fuse DRUJ, create pseudarthrosis, stabilize stump
- Ulna Resection
- 2-4mm articular surface
- Key Technical Points
- Preserve ulnar styloid, interpose soft tissue
- Ulna Resection
- Ulnar head only
- Key Technical Points
- Size matching critical, preserve soft tissues
Complications
Surgical Complications
Ulnar Stump Instability: Common after Darrach (30-40%), especially in younger patients; prevent with adequate soft tissue stabilization; treat symptomatic cases with tendon stabilization procedures
Nonunion after Sauvé-Kapandji: Occurs in 5-10%; usually at the fusion site; requires revision with bone graft and rigid fixation if symptomatic
Nerve Injury: Dorsal sensory ulnar nerve at risk with all approaches; protect during dissection; painful neuromas may require excision and burial
Stiffness: May occur after any procedure; prevent with early motion protocols; aggressive therapy if excessive
Implant-Related: Loosening, wear, breakage with DRUJ prosthesis; requires surveillance and revision surgery if symptomatic
Early complications include wound healing problems (infection, dehiscence, hematoma), nerve injury (dorsal sensory branch of ulnar nerve most common), and early instability. Late complications include ulnar stump instability after Darrach (30-40% incidence, higher in younger active patients), nonunion after Sauvé-Kapandji fusion (5-10%), persistent or recurrent pain (10-20% across all procedures), prosthesis loosening or wear (10-15% at 5-10 years for DRUJ arthroplasty), and complex regional pain syndrome (rare, less than 5%).
Outcomes and Prognosis
Patient satisfaction and functional outcomes vary by procedure and patient selection. Darrach procedure achieves good pain relief in 75-85% but with variable grip strength (typically 80-90% of contralateral) and risk of ulnar stump instability especially in younger patients. Sauvé-Kapandji achieves excellent outcomes in 85-90% with good pain relief, maintained rotation (80-90%), and stable DRUJ, making it preferred for younger active patients.
Hemiresection-interposition achieves good to excellent outcomes in 70-80% at intermediate follow-up but may deteriorate over longer term. DRUJ prosthetic arthroplasty has promising early results but limited long-term data; preliminary reports suggest 80-85% satisfaction at 5 years with 10-15% revision rate.
Factors predicting better outcomes include appropriate procedure selection for patient age and activity level, absence of inflammatory arthropathy, good bone stock, and realistic patient expectations. Poor prognostic factors include workers' compensation or litigation, unrealistic expectations, severe osteoporosis, and active smoking (affects healing).
Quick Review Summary
DRUJ Arthritis Overview
- Degenerative or post-traumatic arthritis of the distal radioulnar joint
- Ulnar head articulates with sigmoid notch of radius
- Critical for forearm pronation/supination
- Ulnar-sided wrist pain with rotation
- Painful restricted pronation/supination
- DRUJ tenderness and crepitus
- Piano key sign (dorsal-volar instability)
- Frequency
- 60-70%
- Characteristics
- Most common, assess for malunion correction
- Frequency
- 10-15%
- Characteristics
- Chronic instability leads to arthritis
- Frequency
- 10-15%
- Characteristics
- RA, psoriatic arthritis, bilateral
- Frequency
- 5-10%
- Characteristics
- No clear antecedent trauma
Complications
Complications by Procedure
- Ulnar stump instability (most common, 20-30%)
- Radioulnar impingement
- ECU subluxation
- Weakness of grip
- Persistent pain
- Proximal stump instability (similar to Darrach)
- Nonunion of DRUJ fusion (5-10%)
- ECU irritation
- Hardware prominence
- Darrach
- 20-30%
- Sauvé-Kapandji
- 10-15%
- Ulnar Head Replacement
- 5-10%
- Darrach
- 10-20%
- Sauvé-Kapandji
- 10-15%
- Ulnar Head Replacement
- 10-15%
- Darrach
- N/A
- Sauvé-Kapandji
- 5-10%
- Ulnar Head Replacement
- N/A
- Darrach
- 15-20%
- Sauvé-Kapandji
- 10-15%
- Ulnar Head Replacement
- 10-15%
Postoperative Care
Postoperative Protocol
- Short arm splint 2 weeks
- Active ROM from 2 weeks
- Strengthening from 6 weeks
- Full activity 8-12 weeks
- Above elbow splint 2 weeks (supination)
- Short arm splint 2-6 weeks
- Active ROM from 6 weeks (after fusion confirmation)
- Strengthening from 8 weeks
- Full activity 12-16 weeks
- Darrach
- 2 weeks
- Sauvé-Kapandji
- 6 weeks
- Darrach
- 2-4 weeks
- Sauvé-Kapandji
- 6-8 weeks
- Darrach
- 6 weeks
- Sauvé-Kapandji
- 8-10 weeks
- Darrach
- 8-12 weeks
- Sauvé-Kapandji
- 12-16 weeks
Outcomes
Outcome Data
- Pain relief: 80-85%
- Patient satisfaction: 70-80%
- Grip strength: 70-80% of contralateral
- Rotation: Generally maintained or improved
- Fusion rate: 90-95%
- Pain relief: 85-90%
- Patient satisfaction: 80-85%
- Rotation: 80-90% of preoperative (through pseudarthrosis)
- Darrach
- 80-85%
- Sauvé-Kapandji
- 85-90%
- Ulnar Head Replacement
- 80-85%
- Darrach
- 70-80%
- Sauvé-Kapandji
- 80-85%
- Ulnar Head Replacement
- 80-85%
- Darrach
- 70-80%
- Sauvé-Kapandji
- 75-85%
- Ulnar Head Replacement
- 80-90%
- Darrach
- 15-20%
- Sauvé-Kapandji
- 10-15%
- Ulnar Head Replacement
- 10-15%
Guidelines, Registries & Global Practice
DRUJ arthritis is a clinical and radiographic diagnosis with no single society "guideline" governing it; practice is shaped by hand-surgery society teaching (ASSH, BSSH, FESSH, IFSSH) and by the absence of high-level comparative evidence. The principles below apply to candidates sitting any international fellowship examination (FRCS, FRACS, EBOT/FEBOT, ABOS, DNB/MS, MRCS, SICOT).
Global Epidemiology
- Post-traumatic disease (distal radius malunion, chronic DRUJ instability, Essex-Lopresti injury) is the dominant cause worldwide; inflammatory arthropathy is the next largest group and primary osteoarthritis is uncommon.
- Distal radius fractures are among the most common upper-limb fractures globally and are rising with population ageing, so the at-risk pool for secondary DRUJ arthritis is large and growing.
- Inflammatory (rheumatoid) DRUJ disease is declining in high-income settings as early biologic disease-modifying therapy reduces joint destruction, but remains a frequent indication where access to such therapy is limited.
Side-by-Side Practice Comparison
- approach
- Darrach excision favoured (poor bone precludes reliable fusion or implant)
- rationale
- Reliable pain relief, simple, tolerant of poor bone stock
- approach
- Sauvé-Kapandji or ulnar head replacement
- rationale
- Preserve ulnocarpal support, grip and rotation; avoid stump convergence
- approach
- Corrective distal radius osteotomy ± ulnar shortening
- rationale
- Address the cause before sacrificing the joint
- approach
- Ulnar head / total DRUJ arthroplasty in specialist centres
- rationale
- Restores stability that excision cannot; needs expertise and bone stock
Registry and Evidence Notes
- There is no dedicated international DRUJ implant registry; survivorship data come from single-centre and multicentre series rather than national joint registries (which capture hip, knee and increasingly shoulder arthroplasty).
- The best long-term implant data are prospective multicentre series of the Herbert ulnar head prosthesis showing durable stability at over 10 years, contrasted with high complication rates when DRUJ implants are combined with total wrist fusion.
High- vs Limited-Resource Practice Variation
- Well-resourced settings: ready access to CT, MR arthrography and arthroscopy for diagnosis; ulnar head and total DRUJ implants and hand therapy available; corrective osteotomy offered for malunion.
- Limited-resource settings: diagnosis rests on plain radiographs and clinical tests; the Darrach and Sauvé-Kapandji procedures dominate because they need no implants and tolerate poor bone; prosthetic arthroplasty and specialised hand therapy may be unavailable, raising the threshold for surgery and favouring durable, low-cost salvage.
Controversies & Areas of Uncertainty
DRUJ salvage surgery rests almost entirely on Level IV case series; no randomised trial has compared the main procedures, so several questions remain genuinely unresolved.
- Darrach versus Sauvé-Kapandji in the active patient. Both rely on the same soft-tissue stabilisation and both can develop a painful, convergent proximal ulnar stump. Sauvé-Kapandji preserves the ulnar head and ulnocarpal support and is generally preferred in younger, higher-demand patients, but high-quality comparative data are lacking and stump instability is not reliably abolished by either.
- Failed distal ulna resection is hard to salvage. Symptomatic radioulnar convergence after Darrach is a recognised, poorly solved problem.
- Ulnar head and total DRUJ implants restore stability that excision arthroplasties cannot, with durable long-term results in well-selected wrists, but registry-level survivorship data are scarce and complication/explantation rates rise sharply when combined with total wrist fusion.
- Role of corrective radius osteotomy. When DRUJ arthritis is early and driven by a correctable distal radius malunion, osteotomy may halt progression and defer salvage; the threshold of arthrosis beyond which osteotomy fails is not well defined.
Key Mnemonics
RADIO ProblemsDRUJ Arthritis Etiologic Factors
Hook:RADIO problems lead to DRUJ arthritis - think of the distal RADIUS as the key player
DASH SolutionsDRUJ Arthritis Surgical Procedures
Hook:When conservative treatment fails, use DASH Solutions for DRUJ arthritis
TIPLEDifferential for Ulnar-Sided Wrist Pain
Hook:TIPLE causes mimic DRUJ arthritis - exclude each before committing to a salvage operation
Viva Grading Review
DRUJ Arthritis Classification
By Etiology:
- Post-traumatic (most common - 60-70%)
- Inflammatory (RA, psoriatic)
- Degenerative (primary osteoarthritis)
- Secondary to instability
- Radiographic Findings
- Minimal joint space narrowing, preserved sigmoid notch
- Clinical Features
- Mild pain with activity, minimal ROM loss
- Treatment Options
- Conservative management, consider malunion correction
- Radiographic Findings
- Moderate narrowing, early osteophytes, ulnar head changes
- Clinical Features
- Moderate pain, 20-40% rotation loss
- Treatment Options
- Address etiology, consider hemiresection or Sauvé-Kapandji
- Radiographic Findings
- Bone-on-bone, sigmoid notch erosion, ulnar head deformity
- Clinical Features
- Severe pain, greater than 50% rotation loss, instability
- Treatment Options
- Darrach, Sauvé-Kapandji, or prosthesis
MCQ Practice Points
Q: What are the causes of DRUJ arthritis and how do they affect treatment selection?
A: Causes: (1) Post-traumatic (most common) - distal radius malunion, Essex-Lopresti injury, TFCC tears; (2) Inflammatory - RA (often bilateral, involves carpal joints); (3) Degenerative - primary OA (rare, usually with positive ulnar variance). Treatment selection: Low-demand elderly: Darrach resection. High-demand/young: Matched ulnar head prosthesis, Sauvé-Kapandji, or one-bone forearm. RA with concurrent carpal disease: Consider combined procedures.
Q: What is the Darrach procedure and what are its indications and complications?
A: Darrach procedure: Excision of distal ulna (2-3 cm). Indications: Low-demand elderly patients, rheumatoid arthritis, failed previous DRUJ procedures. Contraindications: Young, active patients; heavy laborers; need for forearm stability. Complications: Ulnar stump instability (painful clicking, snapping - most common); Radioulnar impingement; Weakness of grip; ECU subluxation. Modifications (soft tissue stabilization, capsular interposition) reduce instability risk.
Q: What is the Sauvé-Kapandji procedure and when is it preferred over Darrach?
A: Sauvé-Kapandji: DRUJ fusion with proximal ulnar pseudarthrosis (segment excision creates "floating" proximal ulna). Advantages over Darrach: Preserves ulnar head for ulnocarpal support; Better cosmesis (no ulnar stump); Maintains TFCC insertion. Indications: Younger, active patients; Need for ulnar-sided wrist stability. Complications: Proximal stump instability (similar to Darrach - requires soft tissue stabilization); Pseudarthrosis of fusion; ECU irritation.
Q: What are the options for ulnar head replacement in DRUJ arthritis?
A: Matched ulnar head arthroplasty (e.g., First Choice, Herbert): Replaces arthritic ulnar head while preserving DRUJ articulation. Advantages: Maintains forearm stability, grip strength, and ulnocarpal support. Indications: Young/active patients with isolated DRUJ arthritis and intact sigmoid notch. Requirements: Adequate sigmoid notch cartilage, stable soft tissues. Complications: Loosening, instability (requires adequate soft tissue tension), sigmoid notch erosion.
Q: How does ulnar variance affect DRUJ arthritis and treatment planning?
A: Positive ulnar variance: Ulnar impaction syndrome, increases ulnocarpal loading. May require ulnar shortening osteotomy if DRUJ preserved, or consider shortening with arthroplasty. Negative ulnar variance: Often post-traumatic (radius malunion with shortening). May require radius osteotomy to correct alignment before DRUJ procedure. Neutral variance: Isolated DRUJ procedure usually sufficient. Variance assessment on neutral rotation PA radiograph essential for surgical planning.
Why Radioulnar Convergence Happens After Distal Ulna Resection
The whole of the "painful clicking stump" viva turns on radioulnar convergence, and a followUp asks why it happens - but the pathomechanics are never set out.
- The ulna is a load-bearing strut. The intact distal ulna and its DRUJ articulation act as a lateral buttress that keeps the radius and ulna apart and shares axial and rotational load across the forearm. Removing the distal ulna (Darrach) - or leaving only a short, poorly-supported stump - removes that spacer.
- Dynamic muscle forces then pull the bones together. The interosseous membrane, pronator quadratus and the wrist/finger muscles bridging the radius and ulna generate a convergent (radius-toward-ulna) force, especially under grip and forearm rotation. With the distal buttress gone, the residual ulna is drawn toward the radius and the two bones abut and impinge - the painful clicking "rubbing" the patient describes, seen as convergence on grip/stress radiographs.
- Why it is worse in the young and high-demand. Greater muscle power and higher loading generate larger convergent forces, so a Darrach in a young manual worker is far more likely to become symptomatic - which is exactly why Sauvé-Kapandji (preserving the ulnar head and ulnocarpal support) or an implant is preferred in this group.
- Static resection alone does not fix it. Simply shortening the ulna further worsens convergence; the problem is the lost articulation and dynamic imbalance, not bone length.
Q: Why does radioulnar convergence develop after distal ulna resection? A: The distal ulna and its DRUJ articulation normally act as a lateral strut keeping the radius and ulna apart and sharing load. Once it is resected, the interosseous membrane, pronator quadratus and bridging muscles pull the residual ulna toward the radius under grip and rotation, so the two bones abut and impinge (painful clicking; convergence on grip radiographs). It is worse in young, high-demand patients (greater convergent force) and is NOT solved by further ulnar shortening - hence Sauvé-Kapandji or an implant is preferred in this group.
Stabilising the Unstable Ulnar Stump
The complications list and the failed-Darrach viva name several soft-tissue stabilisations for a painful convergent stump - ECU/FCU tenodesis, pronator quadratus interposition, distal radioulnar ligament reconstruction - but a followUp asks you to describe one, and none is developed.
- ECU (or FCU) tenodesis sling (dynamic). A distally-based slip of extensor carpi ulnaris (or flexor carpi ulnaris) is passed through a drill hole in the residual ulna and looped around it (a Breen-Jupiter type ECU/FCU tenodesis), tethering the stump and adding a dynamic checkrein that resists convergence during grip. It is the workhorse both as a primary adjunct at the Darrach and for a symptomatic stump.
- Pronator quadratus interposition. The pronator quadratus is mobilised and wrapped or interposed between the radius and the ulnar stump, providing a vascularised soft-tissue cushion that resists bony abutment - simple, and often combined with a tenodesis.
- Distal radioulnar ligament reconstruction (Adams-Berger). A free tendon graft (palmaris longus) is passed through bone tunnels in the radius and ulna to recreate the dorsal and palmar radioulnar ligaments and restore a stable articulation; this is used where the ulnar head is retained (instability without full excision) rather than for a bare stump.
- When soft tissue is not enough. In a well-selected wrist with adequate bone stock and an intact/reconstructable sigmoid notch, converting to an ulnar head or total DRUJ prosthesis restores a true stable articulation more reliably than any tenodesis; a one-bone forearm (see the radioulnar-synostosis topic) is the last-resort salvage that trades all forearm rotation for a stable, painless forearm.
Q: Describe a soft-tissue stabilisation for a painful unstable ulnar stump after Darrach. A: The most useful is an ECU (or FCU) tenodesis sling - a distally-based tendon slip passed through a drill hole in the residual ulna and looped around it (Breen-Jupiter type) to tether the stump and dynamically resist convergence. Alternatives are a pronator quadratus interposition/wrap (a vascularised cushion between radius and stump) and, where the ulnar head is retained, an Adams-Berger distal radioulnar ligament reconstruction with a palmaris graft. If soft tissue fails and bone stock/sigmoid notch allow, convert to an ulnar head/total DRUJ implant; a one-bone forearm is the last resort.
At a Glance
DRUJ arthritis is degenerative or post-traumatic arthritis of the distal radioulnar joint, most commonly following distal radius malunion (60-70% of cases). It presents with ulnar-sided wrist pain, crepitus, and restricted forearm pronation/supination. The piano key sign (dorsally prominent ulna) and DRUJ grind test are key examination findings. Treatment options include activity modification and NSAIDs for mild disease, progressing to surgery for refractory cases: Darrach procedure (ulnar head resection) for low-demand elderly patients, Sauvé-Kapandji (DRUJ fusion with proximal ulna pseudarthrosis) for younger active patients, or DRUJ arthroplasty in select cases.
Distal radius malunion alters DRUJ biomechanics through several mechanisms including dorsal angulation increasing load on dorsal sigmoid notch, radial shortening creating positive ulnar variance and increased DRUJ pressure, and articular step-off creating point loading and accelerated cartilage wear. Chronic DRUJ instability from TFCC insufficiency leads to abnormal kinematics with repetitive subluxation, synovitis, and progressive cartilage degeneration.
Patient Presentation
History
Patients typically present with ulnar-sided wrist pain that is activity-related and worse with forearm rotation, gripping, and loading. Specific aggravating activities include turning doorknobs, using screwdrivers, wringing towels, push-ups, and keyboard use. Pain may radiate proximally into the forearm or distally into the ulnar digits. Mechanical symptoms including clicking, catching, or popping with rotation suggest instability or loose bodies.
History of antecedent trauma (particularly distal radius fracture) should be elicited, including mechanism, treatment received (operative versus non-operative), and healing complications. Patients may report progressive worsening over months to years since the initial injury. In inflammatory arthropathy cases, systemic symptoms and involvement of other joints should be documented.
Physical Examination
Inspection: Swelling over ulnar wrist (usually mild), prominence of ulnar head (dorsal subluxation), muscle atrophy (rare unless chronic severe pain)
Palpation: DRUJ tenderness (dorsally and volarly over ulnar head), crepitus with forearm rotation, ulnar styloid tenderness (TFCC involvement)
Range of Motion: Measure active pronation and supination with elbow flexed 90 degrees, compare to contralateral side; typical loss of 30-50% motion in each direction
Provocative Tests: Piano key sign (dorsal-volar translation of ulnar head), DRUJ grind test (axial compression with pronation/supination), ulnar fovea sign (TFCC pathology)
Stability Assessment: Dorsal-volar translation compared to contralateral wrist in neutral, pronation, and supination
Neurovascular: Assess ulnar nerve function, ulnar artery (Guyon canal), dorsal sensory ulnar nerve branches
The DRUJ grind test is performed by stabilizing the distal radius with one hand while grasping the ulnar head with the other, applying axial compression and rotating through pronation and supination. Crepitus and reproduction of pain indicate DRUJ arthritis. The piano key sign assesses DRUJ stability by applying dorsal and volar directed forces to the ulnar head while stabilizing the radius, looking for excessive translation and reproduction of symptoms.
Functional Impact
Functional deficits vary with severity but commonly include difficulty with activities requiring forearm rotation (turning keys, opening jars, using screwdrivers), reduced grip strength due to pain inhibition (20-40% reduction typical), inability to bear weight on extended wrist (push-ups, yoga), and difficulty with keyboard and mouse use. Patients may develop compensatory strategies such as rotating the entire arm from the shoulder rather than forearm rotation.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 55-year-old carpenter presents with ulnar wrist pain 3 years after a distal radius fracture treated non-operatively. Examination reveals DRUJ tenderness, crepitus, and 50% loss of forearm rotation. Radiographs show DRUJ arthritis with dorsal malunion of the radius. Conservative management has failed. What are your surgical options and which would you recommend?”
“A 72-year-old retired woman with rheumatoid arthritis presents with painful DRUJ arthritis affecting her dominant hand. She has tried NSAIDs and corticosteroid injection with temporary relief only. Radiographs show severe DRUJ arthritis with ulnar head erosion. She has low functional demands. What is your management approach?”
“A 48-year-old manual worker had a Darrach resection of the distal ulna 18 months ago for post-traumatic DRUJ arthritis. He now has ulnar-sided pain, a painful click on gripping and rotation, and feels the forearm bones 'rub together'. Radiographs show convergence of the proximal ulnar stump towards the radius on grip views. How do you assess and manage this?”
Definition and Anatomy
- Arthritis of distal radioulnar joint (ulnar head articulates with sigmoid notch of radius)
- Critical for forearm rotation (pronation/supination)
- Etiology: Post-traumatic 80% (distal radius malunion most common), inflammatory arthritis 10-15%, primary OA 5-10%
- Often associated with TFCC pathology, ECU tendinopathy
Clinical Presentation
- Ulnar-sided wrist pain worse with forearm rotation, gripping, loading
- Painful restricted pronation/supination (30-50% loss typical)
- DRUJ tenderness, crepitus with rotation
- Piano key sign (dorsal-volar instability of ulnar head)
- DRUJ grind test positive (axial load with rotation)
- Difficulty with doorknobs, screwdrivers, wringing towels
Investigation Protocol
- PA and lateral wrist radiographs: Joint space narrowing, subchondral sclerosis, ulnar head deformity, assess ulnar variance
- GOLD STANDARD: CT scan (sigmoid notch morphology, articular surface detail, degree of subluxation, bone stock assessment)
- MRI: TFCC integrity, soft tissue pathology
- Diagnostic injection: Confirms DRUJ as pain source
- Bilateral comparison views valuable
Conservative Management
- First-line for early-moderate arthritis
- Activity modification (avoid forceful rotation, push-ups)
- NSAIDs for symptom relief
- Splinting in neutral rotation (Muenster-type orthosis) during activities
- Corticosteroid injection (60-70% temporary relief)
- Success rate 40-50% in early disease
- Surgery if 3-6 months conservative treatment fails
Surgical Options - By Patient
- DARRACH (ulnar head excision): Age greater than 60, low-demand, rheumatoid arthritis, severe bone erosion - Simple, reliable pain relief but ulnar stump instability and reduced grip
- SAUVÉ-KAPANDJI (radioulnar fusion + pseudarthrosis): Age less than 60, high-demand, good bone stock - Stable DRUJ, maintained rotation, best outcomes but technical with nonunion risk 5-10%
- HEMIRESECTION-INTERPOSITION (Bowers): Age 45-65, intermediate demands - Preserves TFCC, less extensive but variable long-term results
Sauvé-Kapandji Technique
- Create radioulnar fusion at DRUJ level (prepare articular surfaces, fix with screw/K-wires in neutral rotation)
- Create 1-1.5cm ulnar pseudarthrosis proximal to fusion (allows forearm rotation through this site)
- Advantages: Stable DRUJ, maintained rotation via pseudarthrosis, excellent pain relief, good grip strength
- Recovery: 3-4 months to full activity
- Fusion rate 90-95%, Satisfaction 85-90%
Key Complications
- Darrach: Ulnar stump instability (30-40%, especially younger patients), reduced grip strength (10-20%)
- Sauvé-Kapandji: Nonunion at fusion site (5-10%), ulnar stump instability if excessive proximal resection
- General: Nerve injury (dorsal sensory ulnar nerve), persistent pain (10-20%), wound complications, CRPS (less than 5%)
Viva Talking Points
- Emphasize post-traumatic etiology (distal radius malunion most common)
- CT scan gold standard imaging
- Conservative first-line (3-6 months)
- Surgical selection by patient age and demand: Darrach for elderly/low-demand, Sauvé-Kapandji for younger/high-demand
- Know Sauvé-Kapandji technique (fusion + pseudarthrosis)
- Ulnar stump instability main concern with Darrach
- Assess for associated TFCC, ECU pathology
Evidence Base
Key Evidence
- Darrach WE (1913): Original description
- High complication rates in young, active patients
- Remains reliable for elderly, low-demand patients
- Sauvé and Kapandji (1936): Original description
- Better outcomes in younger patients vs Darrach
- Fusion rate 90-95%
- Procedure
- Ulnar head excision
- Key Finding
- Original description of procedure
- Procedure
- DRUJ fusion + pseudarthrosis
- Key Finding
- Preserves ulnocarpal support
- Procedure
- Hemiresection-interposition
- Key Finding
- Alternative for moderate arthritis
- Procedure
- Sauvé-Kapandji vs Darrach
- Key Finding
- S-K superior in younger patients
Additional Resources and Further Reading
Practical Notes
Hand therapy is critical for both conservative and postoperative management. Customised splinting in neutral rotation, grip and forearm strengthening, and functional retraining optimise outcomes regardless of healthcare setting. In work-related cases, detailed causation assessment, graduated return-to-work planning, and ergonomic modification of forearm-rotation-heavy tasks support recovery.
This topic provides comprehensive, globally applicable coverage of DRUJ arthritis for international fellowship examinations, emphasising aetiology recognition, patient-specific surgical selection, and evidence-based management of this common yet challenging wrist condition.