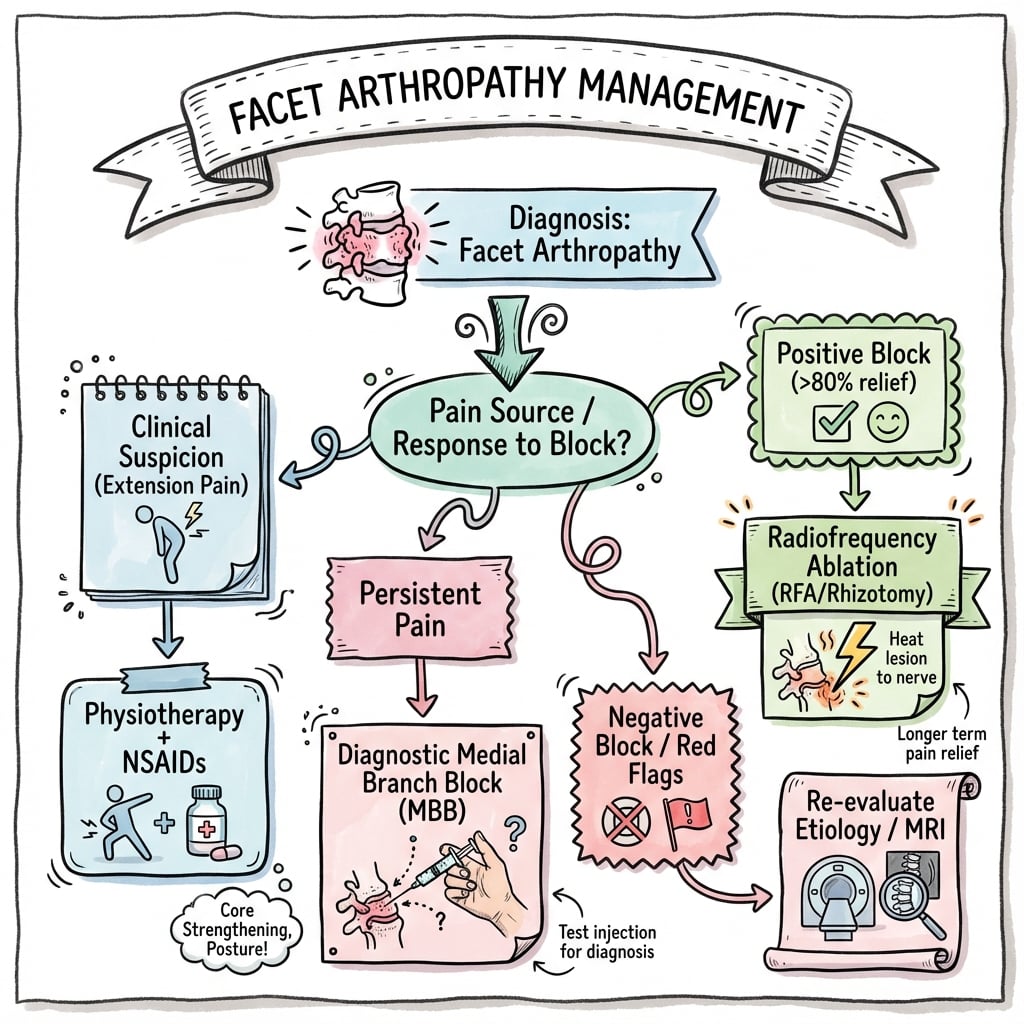
Degenerative Spine Disease | Source of Axial Back Pain | Contribution to Stenosis
- Facet arthropathy is a major contributor to AXIAL MECHANICAL BACK PAIN (not radicular).
- Diagnostic facet joint blocks are the gold standard for diagnosis (80% pain relief threshold).
- Facet hypertrophy contributes to CENTRAL and LATERAL RECESS STENOSIS.
- Conservative management (PT, NSAIDs) is first-line for 6-12 weeks.
- Radiofrequency ablation of medial branch nerves provides 6-12 months relief in 60-70% of patients.
- “Pain worse with EXTENSION and ROTATION (loads the facets).
- “Tenderness over facet joints (2-3 cm lateral to midline).
- “Single-level facet pain is rare; usually multi-level disease.
- “MRI changes correlate poorly with symptoms - clinical diagnosis is key.
Overview and Epidemiology
Definition Facet arthropathy (zygapophyseal joint osteoarthritis) is degenerative disease of the posterior synovial joints of the spine, characterized by cartilage loss, subchondral sclerosis, osteophyte formation, and capsular hypertrophy. It is a major contributor to axial mechanical low back pain and spinal stenosis.
Epidemiology
- Prevalence: Present in 40-85% of adults over 60 on imaging (many asymptomatic).
- Contribution to LBP: Facets responsible for 15-40% of chronic low back pain cases.
- Level Distribution: L4/5 (most common) greater than L5/S1 greater than L3/4.
- Progression: Accelerated by obesity, heavy labor, prior spine surgery (adjacent segment disease).
L4/5 is the most mobile lumbar segment and bears the highest biomechanical stress. It is the fulcrum for lumbar lordosis and experiences maximum extension/rotation moments. This explains why L4/5 facet arthropathy and degenerative spondylolisthesis are most common at this level.
Anatomy and Biomechanics

Facet Joint Anatomy
- Type: Synovial diarthrodial joint with hyaline cartilage.
- Orientation: Sagittal in lumbar spine (resists rotation), coronal in thoracic (allows rotation).
- Innervation: Dual innervation by medial branches of dorsal rami from levels above and below (e.g., L4/5 facet innervated by L3 and L4 medial branches).
- Capsule: Richly innervated with mechanoreceptors and nociceptors.
Biomechanical Function
- Load Sharing: Facets bear 0-16% of axial load in neutral position, increasing to 40% in extension.
- Motion Control: Primary resistors of rotation and excessive translation.
- Stability: Prevent anterior translation of superior vertebra (resist shear).
Resection of greater than 50% of the facet joint (especially the pars interarticularis) during decompression surgery significantly increases risk of postoperative instability and may require prophylactic fusion. Always assess preoperative facet joint integrity and plan fusion if extensive facetectomy is needed.
- Courses over SAP-TP junction (superior articular process and transverse process).
- Target for diagnostic blocks and radiofrequency ablation.
- Dual innervation means TWO levels must be blocked/ablated per joint.
- Example: L4/5 facet requires L3 and L4 medial branch blocks.
- Disc degeneration → Loss of height → Increased facet load.
- Facet arthropathy → Synovial hypertrophy → Instability.
- Instability → Subluxation → Spondylolisthesis.
- Stenosis → Facet hypertrophy + ligamentum flavum thickening.
Pathophysiology
Degenerative Cascade
Facet arthropathy develops through a well-defined degenerative cascade:
- Initiation: Primary cartilage wear from aging, repetitive loading, or trauma triggers chondrocyte dysfunction.
- Synovial Inflammation: Cartilage breakdown products stimulate synovitis, causing pain and joint effusion.
- Subchondral Changes: Bone sclerosis and subchondral cyst formation develop as cartilage protection is lost.
- Osteophyte Formation: Marginal osteophytes form as a compensatory response to increased stress.
- Capsular Hypertrophy: Joint capsule thickens, contributing to lateral recess stenosis.
- Instability: Advanced degeneration may lead to subluxation and dynamic instability.
Disc-Facet Relationship
The disc and facet joints form a "three-joint complex" at each spinal level:
- Disc degeneration leads to loss of height, increasing facet joint load
- Increased facet load accelerates facet degeneration
- Facet degeneration causes posterior element instability
- Instability further accelerates disc degeneration (vicious cycle)
Stenosis Mechanism
Facet hypertrophy contributes to spinal stenosis through:
- Central Stenosis: Bilateral facet hypertrophy with ligamentum flavum thickening creates "trefoil" canal
- Lateral Recess Stenosis: Superior articular process hypertrophy compresses traversing nerve root
- Foraminal Stenosis: Subluxation and osteophytes narrow the neural foramen
Classification Systems
Modified Fujiwara Radiographic Grading
The Fujiwara classification grades facet arthropathy based on plain radiographs and CT imaging.
- Findings
- Normal facet joint
- Clinical Correlation
- Asymptomatic
- Treatment
- None
- Findings
- Joint space narrowing, sclerosis
- Clinical Correlation
- Minimal symptoms
- Treatment
- Conservative
- Findings
- Moderate osteophytes, joint erosion
- Clinical Correlation
- Symptomatic facet pain
- Treatment
- Conservative, Blocks, RFA
- Findings
- Severe osteophytes, subchondral cysts, subluxation
- Clinical Correlation
- Stenosis, instability
- Treatment
- Decompression +/- Fusion
MRI and CT findings of facet arthropathy correlate POORLY with symptoms. Many asymptomatic patients have Grade 3 changes. Clinical diagnosis relies on history, exam, and diagnostic blocks, not imaging severity alone.
Clinical Assessment
- Pain Pattern: Axial mechanical low back pain, worse with extension/rotation.
- Relieving Factors: Flexion, sitting, rest.
- Aggravating Factors: Prolonged standing, walking, extension activities.
- Pseudo-radicular Pain: Pain may radiate to buttock/thigh (rarely below knee).
- Morning Stiffness: Common (inflammatory component).
- Night Pain: Rare (if present, consider other pathology).
- Inspection: Loss of lumbar lordosis (protective flexion posture).
- Palpation: Tenderness 2-3cm lateral to midline over facet joints.
- Range of Motion: Pain with extension and ipsilateral rotation.
- Extension-Rotation Test: Standing extension + rotation reproduces pain.
- Neurological Exam: Usually normal (unless concomitant stenosis/radiculopathy).
- Straight Leg Raise: Negative (unless concurrent disc herniation).
Atypical features suggesting alternative diagnosis:
- Night pain, constitutional symptoms: Infection, malignancy.
- Progressive neurological deficit: Stenosis, cauda equina syndrome.
- Young age (under 40): Inflammatory spondyloarthropathy, infection.
- Trauma history: Fracture, instability.
- No mechanical pattern: Visceral referred pain, systemic disease.
The Extension-Rotation Test is highly specific for facet pain. Have patient stand, extend lumbar spine, then rotate toward painful side. Reproduction of typical pain suggests facet-mediated pain. Sensitivity increases if combined with paraspinal tenderness over facet joints.
Investigations

Diagnostic Imaging Protocol
- AP and Lateral: Assess alignment, disc height, osteophytes.
- Flexion-Extension Lateral: Dynamic instability (greater than 3mm translation or greater than 10 degrees angulation).
- Oblique Views: Visualize facet joint space, pars interarticularis.
- Findings: Joint space narrowing, sclerosis, osteophytes, vacuum phenomenon.
- T2 Sagittal/Axial: Facet joint effusion (high signal), cartilage loss.
- T1: Subchondral sclerosis (low signal), fatty infiltration.
- STIR: Bone marrow edema (active inflammation).
- Key Finding: Facet hypertrophy with ligamentum flavum thickening causing trefoil canal.
- Indications: Metallic artifact on MRI, detailed bony anatomy needed.
- Findings: Excellent visualization of osteophytes, subchondral cysts, joint orientation.
- Grading: Use Fujiwara classification based on CT.
- Indications: Discordant imaging and clinical findings, suspected facet pain.
- Findings: Increased tracer uptake indicates active inflammation.
- Use: Guides diagnostic block selection in multi-level disease.
Controlled Diagnostic Medial Branch Blocks are the gold standard for confirming facet-mediated pain. 80% pain relief with concordant physical exam provocation is required. Two separate blocks (using short-acting and long-acting anesthetic) reduce false-positive rate from 40% to under 10%.
Management Algorithm
Conservative Management (First-Line for 6-12 Weeks)
Goal: Reduce inflammation, improve function, avoid surgery.
Conservative Treatment Pathway
- Activity Modification: Avoid extension-based activities.
- NSAIDs: Regular dosing for anti-inflammatory effect (2-4 weeks).
- Physical Therapy: Core strengthening, flexion-based exercises, manual therapy.
- Modalities: Heat, ice, TENS (symptomatic relief).
- Continuing PT: Proprioceptive training, functional restoration.
- Weight Loss: If BMI over 30 (reduces facet load).
- Bracing: Lumbar corset for symptom control (not long-term).
- Reassessment: If no improvement, consider interventional options.
Favorable prognostic factors for conservative management: Age under 50, symptom duration under 6 months, BMI under 30, absence of stenosis, good compliance with PT. Approximately 40-60% achieve satisfactory relief with conservative treatment alone.

Conventional vs Cooled Radiofrequency Ablation
Both the interventional pathway and the viva follow-ups invoke "conventional versus cooled RFA" without defining the difference. The distinction is one of lesion geometry, which in turn dictates how the electrode must be positioned relative to the medial branch.
Conventional (thermal) RFA heats the active tip to roughly 80-90°C for 60-90 seconds. The thermal lesion forms radially around the shaft of the active tip and extends only minimally beyond its end. Because the hottest zone hugs the side of the cannula, the electrode must be placed parallel and tangential to the nerve as it crosses the SAP-TP junction, to capture the greatest length of medial branch. Lesion size grows with a larger-gauge cannula, a longer active tip, higher temperature, and longer duration; several overlapping lesions are often made to allow for anatomical variability in the exact course of the nerve.
Cooled (water-cooled) RFA circulates chilled water through the electrode to prevent charring and the impedance rise that limits conventional lesions. This deposits more energy and creates a larger, more spherical lesion that projects distally beyond the tip (typically run at a set tip temperature near 60°C). The larger lesion volume permits a more perpendicular approach and, in theory, more reliable capture of a variably located nerve, at the cost of longer procedure time and higher consumable cost. Comparative trials are limited and have not established clear clinical superiority of one modality over the other.
Lesioning discipline — regardless of modality, sensory stimulation (50 Hz, seeking concordant paraesthesia at low voltage) and motor stimulation (2 Hz, confirming the absence of lower-limb muscle contraction that would signal proximity to the ventral ramus) are performed before ablation to confirm safe, accurate targeting.
Pulsed RFA (bursts keeping tissue below roughly 42°C, non-neurodestructive) is generally considered insufficient for durable medial branch denervation and is not the standard for facet pain; continuous thermal or cooled lesioning is preferred.
The commonest technical cause of a "failed" RFA is a lesion that misses the nerve. A conventional thermal lesion is largest around the shaft of the active tip, so the electrode must lie parallel to the medial branch; a cooled electrode makes a larger lesion that extends beyond the tip, tolerating a more perpendicular approach. Understanding lesion geometry — not just target temperature — explains why placement technique, active-tip length, and multiple lesions drive success.
Intra-Articular Facet Injection vs Medial Branch Block
The interventional pathway develops only medial branch blocks, yet the FACTS trial, the multispecialty consensus, and the guideline table all contrast intra-articular (IA) facet injection with medial branch block (MBB). Distinguishing the two — and knowing why one is chosen before ablation — is a common viva point.
- Intra-articular facet injection places local anaesthetic (with or without corticosteroid) directly into the facet joint capsule under fluoroscopic or CT guidance. Joint capacity is small (approximately 1-2 mL); over-distension can rupture the capsule. It anaesthetises the joint itself and carries a therapeutic aspiration (the steroid), though evidence for durable benefit is weak.
- Medial branch block anaesthetises the medial branch nerves that supply the joint, not the joint cavity, using a small volume (0.5-1 mL) at the SAP-TP junction of the two segmental nerves involved (dual innervation).
Why MBB is preferred as the prognostic test before RFA: the medial branch is the exact structure that radiofrequency ablation denervates, so a positive MBB maps directly onto the RFA target, whereas a positive IA injection does not. The 2020 multispecialty consensus concluded that MBB is more predictive of RFA success than IA injection. In the FACTS RCT, positive-block rates were similar for IA (54%) and MBB (55%), and post-RFA responder rates were also similar (51% for IA vs 56% for MBB) — but neither block was therapeutic, reinforcing that blocks are used to select candidates rather than to treat.
- Intra-Articular Facet Injection
- Facet joint cavity
- Medial Branch Block
- Medial branch nerve (SAP-TP junction)
- Intra-Articular Facet Injection
- 1-2 mL (small joint capacity)
- Medial Branch Block
- 0.5-1 mL per level
- Intra-Articular Facet Injection
- No (joint, not nerve)
- Medial Branch Block
- Yes (same nerve RFA denervates)
- Intra-Articular Facet Injection
- Lower (per consensus)
- Medial Branch Block
- Higher — preferred selection test
- Intra-Articular Facet Injection
- Weak (steroid aspiration)
- Medial Branch Block
- Not therapeutic (diagnostic/prognostic)
When asked which block to use before RFA, answer medial branch block: it anaesthetises the same nerve the ablation will destroy, so it predicts the RFA response more faithfully than an intra-articular injection. Both blocks are prognostic, not therapeutic (FACTS) — their role is patient selection, and stricter relief thresholds trade fewer false positives for more false negatives.
Complications
- Incidence
- 20-30% at 10 years post-fusion
- Risk Factors
- Long fusion constructs, sagittal imbalance
- Management
- Extend fusion if symptomatic
- Incidence
- 10-15%
- Risk Factors
- Over 50% facet resection, preoperative subluxation
- Management
- Revision fusion
- Incidence
- 10-20%
- Risk Factors
- High temperature, prolonged lesion time
- Management
- NSAIDs, neuropathic pain medications, time (usually resolves)
- Incidence
- Variable
- Risk Factors
- Duration over 2 years, psychological factors, litigation
- Management
- Multidisciplinary pain program, psychological support
- Incidence
- Under 1%
- Risk Factors
- Immunosuppression, diabetes
- Management
- Antibiotics, drainage if abscess
Adjacent segment disease occurs in 20-30% of fusion patients within 10 years. Risk factors include long fusion constructs, sagittal imbalance, and obesity. Preserve motion segments when possible; minimize fusion length. Counsel patients preoperatively about long-term risks and need for potential revision surgery.
Outcomes and Prognosis
Conservative Management:
- 40-60% achieve satisfactory improvement with PT, NSAIDs, and activity modification.
- Better outcomes in younger patients (under 50), shorter symptom duration (under 6 months).
Radiofrequency Ablation:
- 60-70% report 50% or greater pain reduction at 6-12 months.
- Average duration of relief: 9-12 months.
- Repeat RFA often effective but diminishing returns after third ablation.
Surgical Fusion:
- 70-80% good to excellent outcomes when performed for structural indications (stenosis, instability).
- Poorer outcomes for isolated facet pain without structural pathology (30-50% satisfaction).
Poor prognostic factors for fusion: Isolated facet pain without stenosis/instability, duration over 2 years, psychological comorbidities (depression, catastrophizing), active litigation/compensation, smoking, obesity (BMI over 35). Comprehensive preoperative assessment and patient selection are critical.
Guidelines, Registries & Global Practice
Global Epidemiology
- Facet osteoarthritis is near-universal with age: CT prevalence rises from roughly 24% under 40 to 89% at 60-69 years (Framingham cohort), with the highest burden at L4-L5.
- Imaging facet OA correlates poorly with symptoms; facet-mediated pain is estimated to account for 10-40% of chronic low back pain, the wide range reflecting differing diagnostic-block criteria.
- Lumbar fusion and facet-intervention rates vary several-fold between countries and even between regions of the same country, reflecting practice variation rather than disease burden.
- Diagnostic blocks
- MBB preferred over IA; prognostic not therapeutic
- RFA
- Reasonable in well-selected patients after positive block(s)
- Fusion for axial LBP
- Not addressed (interventional focus)
- Diagnostic blocks
- Do not offer imaging-guided injections for non-specific LBP
- RFA
- RFA only after positive diagnostic block and within strict criteria
- Fusion for axial LBP
- Do not offer fusion for non-specific LBP outside a trial
- Diagnostic blocks
- Controlled MBB to confirm facet source
- RFA
- Option after confirmed facet pain
- Fusion for axial LBP
- Reserve for instability/stenosis, not isolated facet pain
- Diagnostic blocks
- Diagnostic blocks to select candidates
- RFA
- Modest, time-limited benefit acknowledged
- Fusion for axial LBP
- Structural indications only; emphasise shared decision-making
- National registries (e.g. UK, US, Scandinavian spine registries) track fusion volumes and revision; degenerative disease dominates indications.
- Rising fusion rates without proportional outcome gains have prompted payer scrutiny and value-based selection criteria worldwide.
- There is no implant registry analogue for RFA; outcomes depend heavily on patient selection and technique.
- Well-resourced settings: Fluoroscopy/CT-guided diagnostic blocks and RFA readily available; MRI used to exclude alternative pathology.
- Limited-resource settings: Diagnosis is largely clinical; emphasis on exercise, NSAIDs, and weight management; interventional procedures and fusion are reserved for clear structural indications.
- Universal principle: Conservative care first; reserve fusion for documented instability or stenosis, not pain alone.
Key documentation requirements:
- Adequate trial of conservative management (typically 6-12 weeks) before interventional treatments.
- Informed consent for RFA: Explain time-limited relief (commonly 6-12 months when effective), the need for repeat procedures, and a substantial non-response rate.
- Informed consent for fusion: Adjacent segment disease risk (20-30% at 10 years), realistic outcome expectations, and alternatives.
- Patient selection for fusion: Document a structural indication (stenosis, instability), not isolated pain. Fusion for isolated facet pain is controversial and associated with poor outcomes.
- Shared decision-making: Record discussion of risks, benefits, alternatives, and patient preferences.
Common medicolegal pitfalls include fusion for isolated pain without structural pathology, an inadequate conservative trial before surgery, and failure to counsel about adjacent segment disease.
Controversies and Areas of Uncertainty
The RFA efficacy debate Observational series and earlier reviews report 50% or greater relief in 60-70% of well-selected patients, but the two highest-quality pragmatic RCTs (FACTS 2018 and MINT 2017) found no clinically important benefit over sham/exercise. Critics argue MINT used a liberal 50% block threshold and possibly suboptimal lesioning; proponents of the RCTs argue prior series were confounded by selection bias and placebo response. The honest exam answer: RFA may help carefully selected patients but the strongest evidence is sobering, and routine use is not supported.
Diagnostic block threshold (50% vs 80%) No consensus exists. An 80% (dual-block) standard maximises specificity but yields more false negatives and is costly; a single 50% block (used in MINT) increases sensitivity but raises false positives to 30-40%. Guidelines deliberately leave this to local protocol.
Is "isolated facet pain" a real entity? Facet OA almost always coexists with disc degeneration (three-joint complex), and imaging facet OA does not correlate with pain. Whether a purely facet-mediated pain phenotype exists - and whether it ever justifies fusion - remains contested. Fusion for axial pain alone is widely discouraged.
Grading reliability Inter-rater agreement for the Fujiwara (MRI) and Pathria (CT) grading systems is only fair to moderate, limiting their use for treatment decisions.
Mnemonics
FACETFacet Joint Pain Features
Hook:FACET pain has classic postural features that distinguish it from discogenic pain.
BLOCKMedial Branch Block Technique
Hook:BLOCK technique ensures accurate diagnosis before considering radiofrequency ablation.
FUSESurgical Indications for Facet Disease
Hook:FUSE criteria: when conservative and interventional treatments fail, or structural decompression requires fusion.
MCQ Practice Points
Q: The L4/5 facet joint receives dual innervation from which medial branch nerves? A: L3 and L4 medial branch nerves. Each facet joint is innervated by medial branches from the levels above and below. This is why diagnostic blocks and RFA must target TWO levels per joint (e.g., L3 and L4 for L4/5 facet).
Q: What percentage of pain relief is required from a diagnostic medial branch block to confirm facet-mediated pain? A: 80% pain relief with concordant provocation maneuvers. Single blocks have a 30-40% false-positive rate, so two separate blocks (using anesthetics with different durations) are recommended to reduce false positives to under 10%.
Q: What percentage of axial load do facet joints bear during lumbar extension? A: Up to 40% of axial load during extension. In neutral position, facets bear 0-16% of load. Extension increases facet loading dramatically, which explains why facet arthropathy causes extension-based pain.
Q: What is the average duration of pain relief following successful radiofrequency ablation for facet-mediated pain? A: 6-12 months (average 9-12 months) in 60-70% of patients with positive diagnostic blocks. Relief is temporary; RFA can be repeated when pain recurs, though efficacy may diminish after the third ablation.
Q: What is the primary indication for fusion in the setting of facet arthropathy? A: Structural indications: spondylolisthesis, stenosis requiring extensive facetectomy (over 50% of facet), or documented dynamic instability. Fusion for isolated facet pain without structural pathology is controversial and generally NOT recommended based on current evidence.
Q: What is the incidence of adjacent segment disease following lumbar fusion at 10 years? A: 20-30% of patients develop symptomatic adjacent segment disease within 10 years of fusion. Risk factors include long fusion constructs, sagittal imbalance, and patient factors (obesity, smoking). This highlights the importance of preserving motion segments when possible.
At a Glance
- Facet Arthropathy
- Extension/Rotation worse
- Discogenic Pain
- Flexion worse
- Facet Arthropathy
- Paraspinal (2-3cm from midline)
- Discogenic Pain
- Midline or bilateral buttock
- Facet Arthropathy
- Rare beyond knee (pseudo-radicular)
- Discogenic Pain
- Axial or leg pain (if herniation)
- Facet Arthropathy
- Facet hypertrophy, subchondral sclerosis
- Discogenic Pain
- Disc desiccation, Modic changes, annular tears
- Facet Arthropathy
- Medial branch block (80% relief)
- Discogenic Pain
- Provocative discography (controversial)
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 62-year-old male presents with 6 months of low back pain worse with extension and prolonged standing. Pain radiates to right buttock but not below knee. Neurological exam normal. MRI shows Grade 2 facet arthropathy at L4/5 and L5/S1. How would you assess and manage this patient?”
“The patient from Scenario 1 returns after 8 weeks of conservative treatment with minimal improvement. He requests 'something more' for pain relief. How would you counsel him regarding interventional options?”
“A 68-year-old female with L4/5 facet arthropathy, Grade 1 degenerative spondylolisthesis, and central stenosis presents with neurogenic claudication (walking 50 meters). Previous RFA provided 8 months of relief but pain recurred. MRI shows trefoil canal with facet hypertrophy contributing to stenosis. How would you manage this patient?”
Key Anatomy
- Synovial diarthrodial joint with hyaline cartilage
- Dual innervation: L4/5 facet = L3 and L4 medial branches
- Medial branch courses over SAP-TP junction (target for blocks/RFA)
- Facets resist 0-16% load (neutral), 40% load (extension)
Classification
- Fujiwara Grade 0 = Normal
- Grade 1 = Narrowing, sclerosis → Conservative
- Grade 2 = Osteophytes, erosion → Conservative, Blocks, RFA
- Grade 3 = Severe changes, cysts, subluxation → Decompression +/- Fusion
Diagnosis
- Clinical: Extension/rotation pain, paraspinal tenderness, no radiculopathy
- Imaging: MRI/CT shows facet changes (poor symptom correlation)
- Gold standard: Medial branch blocks (80% relief threshold)
- Confirmatory: Two separate blocks (reduces false positives to under 10%)
Treatment Algorithm
- Conservative 6-12 weeks: PT, NSAIDs, activity modification (40-60% success)
- Diagnostic blocks: 80% relief confirms facet pain
- RFA: 6-12mo relief in 60-70% (can repeat, diminishing returns after 3rd)
- Fusion: ONLY for stenosis, spondylolisthesis, or over 50% facetectomy needed
Surgical Pearls
- Resection over 50% facet = high instability risk (consider fusion)
- Fusion for isolated facet pain WITHOUT stenosis/instability = controversial, poor outcomes
- TLIF/PLIF for stenosis + instability (addresses both pathologies)
- Counsel about adjacent segment disease (20-30% at 10 years)
Complications
- RFA neuritis: 10-20% (temporary, resolves with time)
- Adjacent segment disease: 20-30% at 10 years post-fusion
- Postoperative instability: 10-15% if over 50% facet removed without fusion
- Chronic pain syndrome: multifactorial (duration, psychological factors)
Evidence Base and Key Trials
Cochrane Review: Radiofrequency Denervation for Chronic Low Back Pain
- 23 RCTs (N=1309); 13 (56%) at low risk of bias; overall evidence very low to moderate quality
- Facet RFA showed moderate-quality evidence of a greater short-term effect on pain than placebo (MD -1.47, 95% CI -2.28 to -0.67)
- Low-quality evidence for short- and long-term functional benefit vs placebo
- No high-quality evidence that RFA provides meaningful pain relief; effect sizes small and below typical clinical thresholds
FACTS RCT: Facet Blocks Are Diagnostic, Not Therapeutic
- 229 patients randomised 2:2:1 to intra-articular facet injection, medial branch block, or saline
- No therapeutic difference between blocks and placebo at 1 month (mean NRS reduction 0.7 in all three groups)
- Positive-block rates higher with active injectate (54% intra-articular, 55% medial branch) than placebo (30%)
- After RFA, positive-responder rate at 3 months was higher in block groups (51-56%) than placebo (24%), suggesting blocks have prognostic value
MINT RCT: RFA Adds No Clinical Benefit to Exercise
- Three pragmatic multicentre RCTs (N=681) of patients with a positive diagnostic block, randomised to exercise +/- RFA
- Facet joint trial: mean pain difference at 3 months -0.18 (95% CI -0.76 to 0.40), below the prespecified MCID of 2 points
- No clinically important improvement from RFA for facet, sacroiliac, or combination-source pain
- Findings do not support RFA for chronic low back pain from these sources
Framingham Study: Facet OA Prevalence and Pain Discordance
- Community-based CT study of 188 adults (aged 40-80) from the Framingham Heart Study
- High prevalence of facet OA: 59.6% of men, 66.7% of women; rising with age (24% under 40 to 89% at 60-69)
- Highest prevalence at L4-L5 (45.1%), then L5-S1 (38.2%), L3-L4 (30.6%), L2-L3 (15.1%)
- No association between CT facet OA at any level and low back pain
Biomechanics: Disc and Facet Degeneration Alter Segmental Motion
- Cadaveric study of 110 lumbar motion segments with MRI/CT grading and 3D motion analysis
- Segmental motion (especially axial rotation) increased with disc degeneration up to grade IV, then decreased at grade V
- Facet cartilage degeneration and subchondral sclerosis independently altered segmental motion, with sex differences
- Osteophyte severity showed no significant association with segmental motion
Multispecialty Consensus: Lumbar Facet Joint Interventions
- International multispecialty working group; 17 questions, 100% committee consensus via modified Delphi
- Medial branch blocks are more predictive of RFA success than intra-articular injections
- Facet blocks have prognostic rather than therapeutic value; stricter selection improves RFA outcomes at the cost of more false negatives
- No single history/exam/imaging finding reliably diagnoses facet pain in isolation