Zone 2 (No Man's Land) | 4-Strand Repair | Early Motion
- Zone 2 = 'No Man's Land' - both tendons in fibrous sheath
- A2 and A4 pulleys are critical (prevent bowstringing)
- 4-strand core suture minimum for early active motion
- Epitendinous suture adds 10-20% strength, improves gliding
- Early active motion reduces adhesions, better outcomes
- “FDP alone if lacerated distal to FDS insertion
- “Core suture 2mm from cut end = optimal strength
- “Early motion: controlled active flexion, passive extension
- “Rupture peak at 7-10 days (weakest point in healing)
'No Man's Land': Both FDP and FDS in tight fibro-osseous sheath. Limited space, high adhesion risk. Historically poor outcomes, now improved with modern techniques and early motion.
A2 pulley (proximal phalanx) and A4 pulley (middle phalanx) are critical for mechanical advantage. Preserve or reconstruct to prevent bowstringing.
4-strand core suture minimum. More strands = stronger repair allowing earlier motion. Epitendinous suture adds strength and improves gliding. Suture 2mm from edge for optimal strength.
Early active motion protocols reduce adhesions. Controlled active flexion, full passive extension. Synergistic exercises. 6 weeks protected motion.
1-5 Fingers to ForearmFlexor Zones
Hook:Zone 1 is finger tip, Zone 5 is forearm - numbers go proximal!
A2-A4Critical Pulleys
Hook:A2 and A4 are even numbers = critical pulleys. A1, A3, A5 are odd = can sacrifice.
STRONGRepair Checklist
Hook:A STRONG repair earns an early-motion programme; a weak one earns a splint.
Overview & Epidemiology
Flexor tendon injuries are common hand-trauma injuries, typically in young working-age men from glass, knives and occupational sharp objects. Zone II is the most frequently injured and most studied zone. Understanding the zone system, repair biomechanics, and rehabilitation principles is essential for optimal outcomes — a digit that does not flex represents a time-sensitive surgical problem.
Pathophysiology & Anatomy
Tendon healing occurs by combined intrinsic (tenocyte-mediated, within the tendon) and extrinsic (from the sheath/surrounding tissue) pathways. Extrinsic healing forms adhesions that restrict gliding — the central biological problem in zone II. Repairs are weakest at roughly 7-10 days as collagen remodels, the period of peak rupture risk. Controlled tendon excursion biases healing toward the intrinsic pathway, which underpins early-motion rehabilitation.
Anatomy
Flexor Digitorum Profundus (FDP): Inserts on distal phalanx base. Flexes DIP joint.
Flexor Digitorum Superficialis (FDS): Splits around FDP (Camper's chiasm), inserts on middle phalanx. Flexes PIP joint.
Pulley System: A1-A5 (annular) and C1-C3 (cruciate) pulleys. A2 and A4 are critical for mechanical advantage. Others can be sacrificed if necessary.
Zone Classification
Zone 2 (A1 pulley to FDS insertion): The "No Man's Land." Both FDP and FDS tendons lie within the tight fibro-osseous sheath. Historically poor outcomes due to adhesions. Modern repair techniques and early motion have improved results.
Repair Principles: Repair both tendons if possible. Some surgeons debride one slip of FDS if space is tight. Protect A2 and A4 pulleys.
Clinical Presentation
Clinical Examination
FDP Test: Hold PIP extended, ask patient to flex DIP. Tests FDP independently.
FDS Test: Hold other fingers extended (blocking FDP contribution), ask to flex PIP. Tests FDS independently.
Cascading Posture: Normal resting hand has fingers in cascade of increasing flexion. Loss of cascade suggests laceration.
Wound Examination: Location indicates zone. Explore wound if tendon injury suspected (after tourniquet, in OR).
Investigations
Flexor tendon laceration is largely a clinical and operative diagnosis — imaging is adjunctive.
- Plain radiographs: Mandatory after any sharp injury to exclude retained glass/foreign body, fracture or a bony avulsion fleck (suggests FDP avulsion / Jersey finger).
- Ultrasound: Useful for closed or doubtful injuries — confirms tendon continuity, identifies the level of a retracted proximal stump, and is operator-dependent.
- MRI: Reserved for complex, chronic or reconstructive planning (gap, sheath scarring, pulley integrity).
- Intraoperative assessment remains the reference standard.
Tendon Evaluation
Look for:
- Complete vs partial laceration (greater than 60% width = functionally complete)
- Level of laceration vs skin wound (tendons may have retracted with the digit position at injury)
- Associated injuries (digital nerves, vessels, bone)
Differential Diagnosis & Mimics
A digit that will not flex is not always a tendon laceration. Distinguishing causes changes the operation, the timing and the consent.
- History / mechanism
- Sharp cut (glass, knife), open wound
- Examination clue
- No active flexion of relevant joint; loss of cascade
- Key discriminator
- Wound over flexor surface; tendon ends visible/retracted
- Action
- Surgical exploration and repair
- History / mechanism
- Sharp cut, weak/painful flexion
- Examination clue
- Flexion present but weak or triggering
- Key discriminator
- Greater than 60% width = functionally complete
- Action
- Repair if over 60%; otherwise trim/observe
- History / mechanism
- Forced extension of flexed DIP (rugby/jersey grab)
- Examination clue
- No active DIP flexion, often no skin wound
- Key discriminator
- Closed injury; Leddy-Packer type; possible bony fleck on X-ray
- Action
- Urgent reinsertion (type I/II earliest)
- History / mechanism
- Atraumatic, gradual catching/locking
- Examination clue
- Palpable A1 nodule, painful clicking
- Key discriminator
- No wound; intermittent locking not fixed loss
- Action
- Splint/steroid; A1 release if refractory
- History / mechanism
- Laceration proximal to muscle, or compression
- Examination clue
- Motor loss with sensory deficit in nerve territory
- Key discriminator
- Tendon intact on exploration; sensory map abnormal
- Action
- Nerve repair; treat cause
- History / mechanism
- Old injury, Dupuytren, prior trauma
- Examination clue
- Passive AND active motion both lost
- Key discriminator
- Tendon glides but joint will not move passively
- Action
- Address joint, not tendon
Management
Principles:
- Minimum 4-strand repair for early active motion (more strands = stronger)
- Suture placed 2mm from cut end for optimal strength
- Locking suture configuration adds strength
- 3-0 or 4-0 braided non-absorbable suture
Common Techniques: Modified Kessler, Strickland, Savage, cruciate.
Strength: 2-strand ≈ 20N, 4-strand ≈ 40N, 6-strand ≈ 60N. Early active motion requires ~40N.
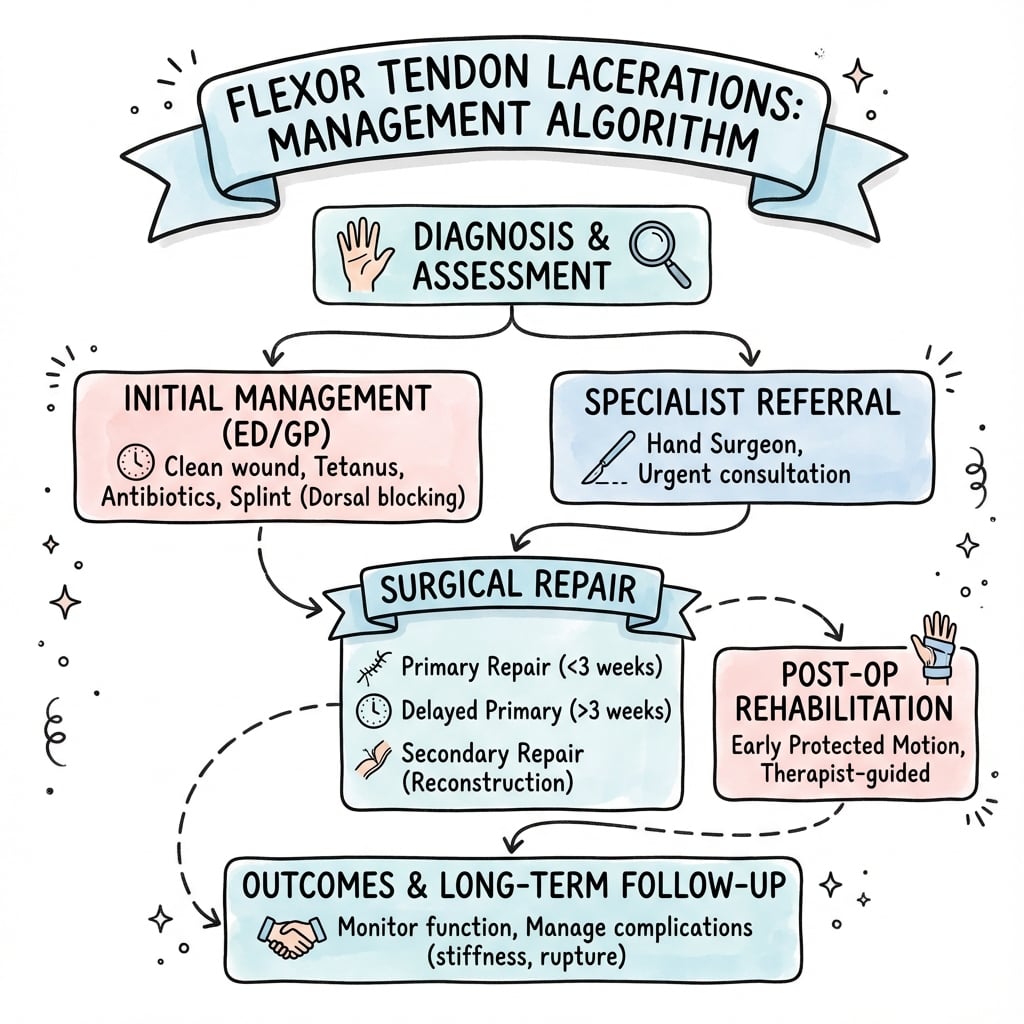
Management Algorithm
Complications
Adhesions: Most common problem. Limit gliding. May require tenolysis.
Rupture: Peak at 7-10 days (weakest point in healing). Requires re-repair.
Stiffness: From adhesions or joint involvement. Address with therapy/tenolysis.
Bowstringing: If critical pulleys (A2, A4) not preserved or over-vented. Reduces mechanical advantage and excursion.
Pulley Reconstruction & the Biomechanics of Bowstringing
This topic repeatedly says to "preserve or reconstruct A2 and A4" and lists bowstringing as a complication, but the underlying mechanics — and what to actually do when a critical pulley is destroyed — decide whether a technically sound tendon repair becomes a working finger.
Why bowstringing matters
The annular pulleys hold the flexor tendon against the phalanges. This keeps the line of pull close to the bone, which minimises the moment arm at each joint and conserves tendon excursion — a given amount of muscle shortening is spent flexing the joints rather than lifting the tendon off the skeleton. When a long pulley (A2 or A4) is lost, the tendon lifts away from the bone and takes the chord across the flexing joint instead of following its arc:
- Excursion is wasted on the bowstring path, so the same FDP contraction produces less distal flexion — the fingertip can no longer reach the palm (loss of composite fist).
- The increased moment arm makes the proximal joint flex preferentially, producing an apparent flexion contracture and a weak, inefficient grip.
- A visible, palpable bowstring lifting off the volar finger is the late clinical sign.
A2 (over the proximal phalanx) and A4 (over the middle phalanx) matter most because they span the longest bony segments and resist the greatest bowstringing force; A1, A3 and A5 can be sacrificed with impunity.
How much pulley is enough — venting versus reconstruction
Modern practice (Tang, in the Evidence Base below) shows the system tolerates judicious venting: A2 may be partially incised over a length no greater than 1.5 to 2 cm, and A4 may be vented entirely, without observed bowstringing or functional loss. That defines the safe ceiling for incising a pulley to expose or deliver a repair. Beyond it — when both critical pulleys, or a long segment of one, are destroyed by trauma, infection or a failed repair — the pulley must be reconstructed to restore the tendon-to-bone relationship.
- Location
- Proximal phalanx
- Why it matters
- Longest pulley; largest bowstring force; conserves excursion
- Safe handling
- Partial vent up to 1.5 to 2 cm only
- If destroyed
- Reconstruct — loss poorly tolerated
- Location
- Middle phalanx
- Why it matters
- Holds the tendon over the PIP-to-DIP segment
- Safe handling
- May be vented entirely if needed for gliding
- If destroyed
- Reconstruct if both A2 and A4 are gone
- Location
- MCP / PIP / DIP volar plates
- Why it matters
- Minor mechanical contribution
- Safe handling
- Can be released or sacrificed
- If destroyed
- No reconstruction needed
Reconstruction techniques
Pulley reconstruction recreates a smooth retinacular loop that holds the tendon (or, in staged cases, the Hunter rod) against the phalanx:
- Encircling free-graft loop — a strip of tendon graft (palmaris longus, a discarded slip of FDS, excised flexor tendon, or a toe extensor) is passed around the phalanx and sutured to itself. At the proximal phalanx the loop is passed deep to the extensor mechanism; over the middle phalanx it can lie superficial to it.
- Weave through the pulley rim (Weilby) — a graft is woven through the surviving rim remnants of the original pulley, useful when a partial pulley remains.
- Extensor-retinaculum graft (Lister) — a segment of dorsal extensor retinaculum is used, placing its smooth synovial surface against the gliding tendon.
Pulley reconstruction is integral to stage 1 of a two-stage Hunter-rod reconstruction, where the pulleys are rebuilt around the silicone rod so the later tendon graft glides correctly; the graft and staged technique themselves belong to flexor tendon reconstruction.
Q: What is the minimum pulley required to prevent clinically important bowstringing? A: A competent A2 and A4 (preserved or reconstructed) are the practical minimum for normal mechanics. The safe ceiling for incising them is Tang's venting limit — A2 partially over no more than 1.5 to 2 cm, A4 entirely — beyond which reconstruction is required. Loss of both critical pulleys, or of a long segment of A2, is poorly tolerated and bowstrings.
Rehabilitation
Principle: Controlled early motion reduces adhesion formation and improves final range of motion. Requires strong repair (4+ strands).
Protocol (Typical):
- Dorsal blocking splint (wrist flexed 20-30°, MCP 50-70°, IP extended)
- Active flexion, full passive extension
- 4-6 times daily exercises
- Progress to place-and-hold, then active motion
- 6 weeks protected, then progressive strengthening
Outcomes: Superior to immobilization with reduced adhesions.
Measuring the Outcome: Strickland & Tang Criteria
Outcome of a flexor repair is graded by active interphalangeal motion, because the whole point of repair is a finger that bends. The vivas and evidence on this page quote "good or excellent" results and a "TAM over 175" target without defining them — examiners expect the candidate to state the actual measurement.
Total Active Motion (TAM)
TAM is the global metric: the sum of active flexion at the MCP, PIP and DIP joints, minus any extension deficit (fixed flexion) at those joints. It captures both how far the finger flexes and how much it fails to straighten.
The Strickland–Glogovac formula
For a flexor repair, outcome is conventionally expressed as a percentage of normal interphalangeal motion, since the FDS and FDP act across the PIP and DIP. The Strickland–Glogovac formula is:
Percentage of normal = (active PIP flexion + active DIP flexion − PIP and DIP extension deficit) ÷ 175 × 100
The denominator 175 is the assumed normal combined IP arc (roughly 100 degrees at the PIP plus 75 degrees at the DIP). The result is then banded:
- Original Strickland
- 85 to 100%
- Modified Strickland
- 75 to 100%
- Original Strickland
- 70 to 84%
- Modified Strickland
- 50 to 74%
- Original Strickland
- 50 to 69%
- Modified Strickland
- 25 to 49%
- Original Strickland
- under 50%
- Modified Strickland
- under 25%
The modified Strickland system uses the same formula with more lenient bands, so the same finger scores a grade higher than under the original — which is why a paper must state which version it used when it reports "good/excellent" rates.
Tang criteria
The newer Tang grading (the system used in the zone-2 series cited in the Evidence Base) likewise sorts results into excellent, good, fair, poor and failure, but is built around the active flexion actually achieved and the residual extension loss, and reflects modern strong-core, early-active-motion outcomes. It is the system behind the "52 of 60 fingers good or excellent" result quoted on this page.
Q: How do you report a flexor tendon repair outcome? A: As TAM, or more specifically for IP motion the Strickland–Glogovac percentage: active (PIP + DIP) flexion minus extension deficit, divided by 175, times 100. "Good or excellent" means little to an examiner unless you can give the formula and say whether you are using the original or the modified bands.
Guidelines, Registries & Global Practice
Global epidemiology: Flexor tendon lacerations are common hand-trauma injuries, predominantly affecting young working-age men, most often from glass, knives and occupational sharp objects. Zone II is the most frequently injured and most studied zone. The dominant injury pattern reflects manual work and domestic glass injuries worldwide, so the burden is highest in working populations and in regions with high rates of interpersonal and occupational sharp trauma.
Side-by-side guidance (recommendations converge more than they differ):
- Emphasis
- Timing and specialist referral
- Practical position
- Primary repair ideally within days; refer to a hand unit; structured therapy-led rehabilitation
- Emphasis
- Repair strength and protected motion
- Practical position
- Multi-strand core repair supporting early controlled motion; hand-therapy partnership
- Emphasis
- Strong tensioned core + venting + EAM
- Practical position
- Well-tensioned 4-6 strand core, judicious A2/A4 venting, intraoperative gliding test, early active motion
- Emphasis
- WALANT and out-of-splint motion
- Practical position
- Increasing use of wide-awake repair with intraoperative active testing and freer early motion
Registry note: There is no dedicated international flexor-tendon registry equivalent to the arthroplasty registries (NJR, AJRR, AOANJRR, SHAR). Best evidence therefore comes from multicentre cohorts and meta-analyses, which consistently report rupture rates of roughly 4-12% and good/excellent outcomes around 70-90% with modern strong-core repair and early active motion.
High- vs limited-resource practice variation: In well-resourced settings, repair is performed under loupe/microscope magnification with hand-therapy-supervised early active motion and, increasingly, WALANT. In limited-resource or remote settings, delayed primary or staged repair, simpler 2-strand techniques and immobilisation-based rehabilitation are more common because of restricted theatre access and limited specialist hand therapy — a recognised driver of higher adhesion and stiffness rates rather than a difference in principle.
Controversies & Areas of Uncertainty
Flexor tendon surgery is one of the most opinion-driven areas in hand surgery; examiners use these debates to separate safe from outstanding candidates.
- How critical are A2 and A4 really? The classic teaching that A2 and A4 must never be touched has softened. Tang's principle of judicious venting (A2 partially under 1.5-2cm, A4 entirely) reports no bowstringing or functional loss and is now mainstream, yet the safe limit of venting before mechanical disadvantage appears is still debated.
- Strand number — strong enough vs too bulky. More strands increase strength and resist gapping, but extra core passes add bulk and gliding resistance and prolong surgery. Many units now favour a well-tensioned 4- or 6-strand repair rather than chasing maximal strand counts.
- Suture caliber. Larger 3-0 suture intuitively seems stronger, but cadaver data show it fails by pulling through the tendon; 4-0 may give a more reliable suture-tendon interface in average-sized tendons.
- How much (and what kind of) peripheral suture? A formal circumferential epitendinous suture adds strength and smooths the repair, but tensioned strong-core series suggest only sparse peripheral stitches are needed, questioning routine elaborate epitendinous work.
- Should the FDS be repaired in zone II? Repairing both tendons restores independent PIP/DIP control but crowds the sheath and risks adhesions; some surgeons excise one FDS slip to make room. Evidence does not clearly favour either approach.
- Rehabilitation regime. True early active motion, place-and-hold, relative-motion-flexion orthoses and early passive motion all have advocates; the best protocol for a given repair strength and patient reliability is not settled.
- Anaesthesia. WALANT permits intraoperative active testing and is cost-effective, but high-quality comparative outcome data versus traditional anaesthesia remain limited.
MCQ Practice Points
Q: Why is Zone 2 called "No Man's Land"? A: Both FDP and FDS tendons are within the tight fibro-osseous sheath. Limited space leads to high adhesion risk and historically poor outcomes (now improved with modern techniques).
Q: Which pulleys are critical for flexor tendon function? A: A2 (proximal phalanx) and A4 (middle phalanx). These must be preserved or reconstructed to prevent bowstringing. A1, A3, A5 can be sacrificed if necessary.
Q: What is the minimum core suture for early active motion protocol? A: 4-strand repair. Provides approximately 40N strength needed for controlled early active motion. 2-strand is insufficient (only 20N).
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 30-year-old man cuts his right ring finger on broken glass. He cannot flex his DIP or PIP joints. How do you manage him?”
“A 35-year-old carpenter presents 6 hours after a knife injury to the volar aspect of his left index finger in Zone 2. He has weak but present DIP flexion and full PIP flexion. In theatre, you find the FDS is intact but the FDP has approximately 70% of its width lacerated with 30% still in continuity on the radial side. The A2 pulley is intact. He is reliable and motivated for therapy. How would you manage the FDP and what would you counsel him about rehabilitation?”
“A 28-year-old builder returns to clinic 3 weeks after Zone 2 FDP and FDS repair of his middle finger. He admits he returned to light work against advice and felt a pop 2 days ago. He now has no active DIP or PIP flexion. X-ray shows no bony injury. In theatre, you find both tendons have completely ruptured and the proximal ends have retracted into the palm with significant fraying and degeneration of the tissue at the previous repair site. The tendon ends are mushy and will not hold suture. What are your management options and what would you recommend?”
Zone Classification
- Zone 1: Distal to FDS (FDP only)
- Zone 2: No Man's Land (both in sheath)
- Zone 3: Palm (NV at risk)
- Zone 4: Carpal tunnel
- Zone 5: Forearm
Repair Principles
- 4-strand core suture minimum
- Suture 2mm from cut end
- Epitendinous suture adds 10-20%
- Preserve A2 and A4 pulleys
Rehabilitation
- Early active motion reduces adhesions
- Dorsal blocking splint
- Active flexion, passive extension
- 6 weeks protected motion
Complications
- Adhesions (most common)
- Rupture (peak 7-10 days)
- Stiffness
- Bowstringing
Evidence Base
- Cadaver zone II in situ model (12 hands), each specimen its own control
- Ultimate tensile strength: 2-strand 33.9N, 4-strand 43.0N, 6-strand 78.7N
- 2-strand gapped 2.75mm after 1000 cycles vs 0.30mm (4-strand) and 0.31mm (6-strand)
- Gliding resistance increase after repair was small and not significant
- 72 cadaver FDP tendons, 4-strand modified Kessler, progressive cyclic loading
- All constructs exceeded the ~27N threshold for early active range of motion
- 3-0 suture failed by pullout in 63.5% (looped) and 38.9% (single-strand) of repairs
- 4-0 suture pulled out in only 11.1% (looped) and 0% (single-strand)
- Core suture purchase no shorter than 0.7-1cm in each tendon end, well tensioned
- A2 may be partially vented (incision under 1.5-2cm); A4 may be vented entirely
- Judicious venting did not cause loss of hand function or bowstringing
- Intraoperative extension-flexion test (often WALANT) confirms gliding before closure
- 60 zone II FDP repairs with tensioned 4- or 6-strand core and only 3-4 peripheral stitches
- Pulleys vented as needed; early active flexion started postoperatively
- No repairs ruptured during follow-up of 8-33 months
- 52/60 (87%) fingers achieved good or excellent function by Tang criteria
- Systematic review/meta-analysis: 7 studies, 569 zone II digits
- Early active motion gave greater total active motion than early passive motion
- Higher rupture risk when active flexion-extension was used with a 2-strand repair
- 2-strand technique judged insufficient for active flexion-extension protocols
- Retrospective cohort, 86 fingers, zone I/II primary flexor repair
- Good/excellent 12-week ROM in 56% (WALANT) vs 31% (traditional) — not statistically significant
- Overall rupture rate 11.6%, tenolysis 3.5%, reoperation 9.3%
- Small sample and poor follow-up (41%) limit strength of conclusions