Shoulder Girdle Ablation | Subclavian Vessel Control | Brachial Plexus Division | Oncological Margins
- Subclavian vessels are controlled first - either from anterior (infraclavicular) or posterior (supraclavicular) approach
- Brachial plexus is divided sharply under tension, allowing retraction to reduce neuroma formation
- Anterior approach preferred for oncological cases - better visualization of neurovascular structures
- Posterior approach used when tumour involves anterior chest wall or for massive posterior tumours
- Clavicle division at junction of middle and lateral thirds; scapula removed en bloc with specimen
- “Control subclavian artery BEFORE vein to prevent venous engorgement and bleeding
- “Preserve pectoralis major if oncologically safe - provides soft tissue coverage
- “Divide brachial plexus roots proximally if tumour involves cords or divisions
- “Staged reconstruction with latissimus flap if primary closure not possible
Control subclavian artery FIRST, then vein. Arterial control before venous control prevents limb engorgement and reduces blood loss. Access via infraclavicular approach (anterior) or supraclavicular approach. Know the relationship to scalenus anterior - subclavian artery is posterior, vein is anterior. Thoracic duct on LEFT side must be identified and ligated.
Wide surgical margins are non-negotiable. For sarcomas, aim for at least 2cm soft tissue margin or fascial plane. Biopsy track must be excised en bloc. Do NOT enter the tumour - contamination significantly worsens prognosis. Frozen section margins if needed. Plan incision to allow limb salvage conversion if margins positive.
Level of division depends on tumour extent. For tumours not involving the plexus, divide at the level of cords or divisions. For plexus invasion, divide at root level (requires supraclavicular dissection). Traction neurectomy technique - sharp division under tension, allow proximal retraction. Phantom limb pain occurs in 60-80%.
Upper limb loss causes profound psychological impact. Body image disturbance, loss of independence, occupational implications are significant. Involve psychology/psychiatry EARLY. Prosthetic options are limited but provide cosmesis. Realistic expectation setting is crucial - discuss inability to replicate hand function.
- Anterior Approach
- Preferred - direct access to vessels
- Posterior Approach
- Alternative if anterior chest involved
- Recommendation
- Default to anterior approach
- Anterior Approach
- May require chest wall resection
- Posterior Approach
- Preferred - avoids tumour manipulation
- Recommendation
- Posterior approach safer
- Anterior Approach
- Preferred - vessels controlled early
- Posterior Approach
- Risk of tumour spillage
- Recommendation
- Anterior approach preferred
- Anterior Approach
- Requires supraclavicular extension
- Posterior Approach
- Better access to proximal roots
- Recommendation
- Combine approaches as needed
- Anterior Approach
- Rapid vascular control
- Posterior Approach
- May be faster for debridement
- Recommendation
- Depends on injury pattern
- Anterior Approach
- May have scarring in vessels
- Posterior Approach
- Alternative if anterior scarred
- Recommendation
- Plan based on imaging and history
SAVBNStructures to Control
Hook:SAVBN - Save the patient by controlling vessels in order: S-Artery, V-Vein, B-Plexus, N-thoracic duct
Overview and Epidemiology
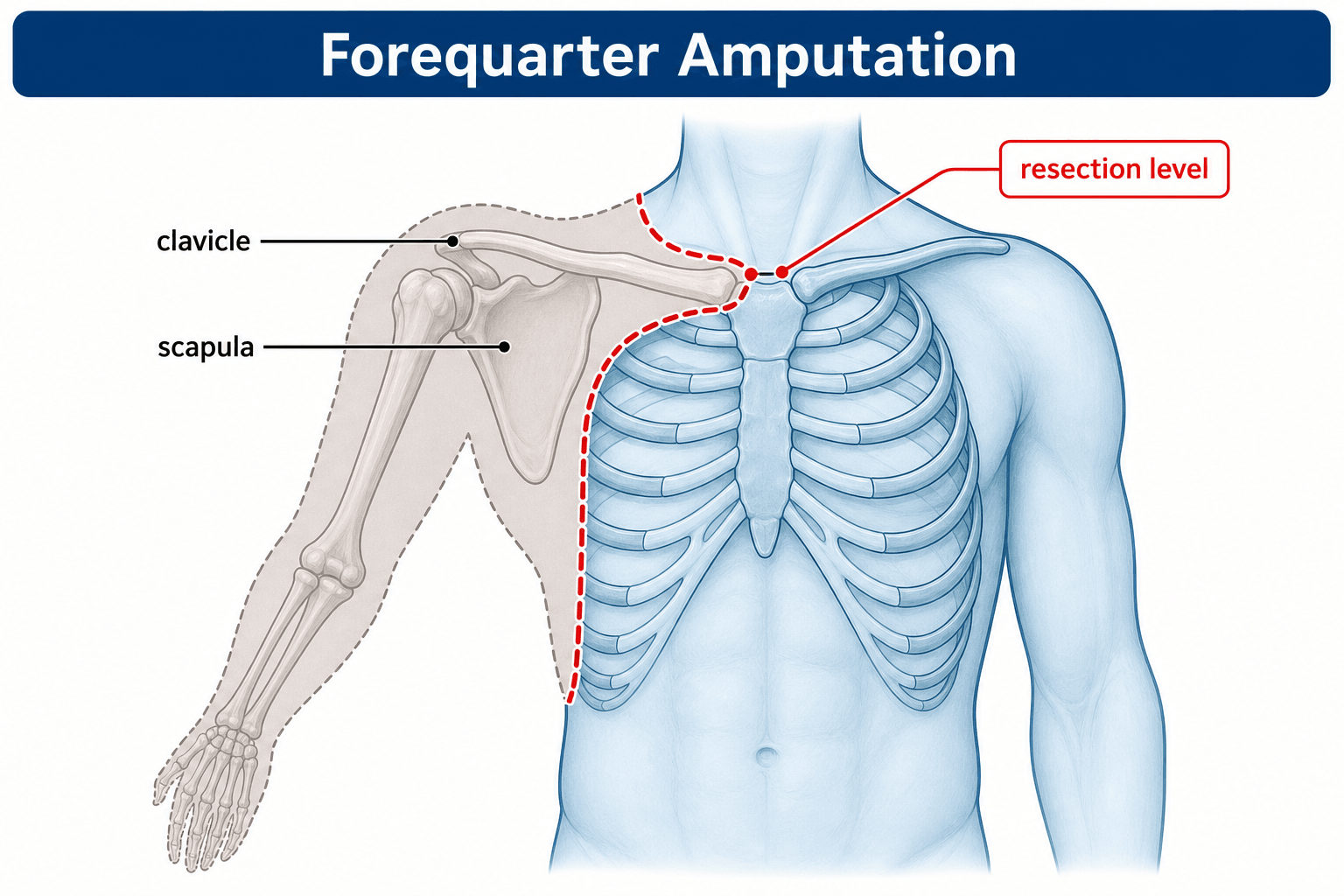
Forequarter amputation (interscapulothoracic amputation) is the ablation of the entire upper extremity including the scapula and lateral clavicle. First described by Ralph Cuming in 1808 and refined by Paul Berger in 1887, it represents the most radical amputation of the upper limb.
Epidemiology:
- Rare procedure - most major centres perform fewer than 5 per year
- Approximately 90% of cases are for oncological indications
- Malignant tumours: soft tissue sarcomas, bone sarcomas, metastatic disease
- Peak age: Bimodal - young adults (primary sarcomas) and elderly (metastatic disease)
- Male slight predominance (1.5:1)
Forequarter amputation removes the entire shoulder girdle (scapula, lateral clavicle, humerus, and all soft tissues) leaving a smooth chest wall. Shoulder disarticulation preserves the scapula and clavicle, disarticulating at the glenohumeral joint. Forequarter is required when tumour involves the scapula, proximal humerus with soft tissue extension, or brachial plexus invasion.
Indications:
- Soft tissue sarcomas: MFH, synovial sarcoma, liposarcoma with proximal extension
- Bone sarcomas: Osteosarcoma, chondrosarcoma, Ewing sarcoma when limb salvage not possible
- Metastatic disease: Renal cell carcinoma, melanoma with local invasion
- Failed limb salvage: Local recurrence after previous surgery
- Brachial plexus invasion: Pancoast tumour extension
- Trauma: Brachial plexus avulsion with flail anaesthetic limb
- Vascular catastrophe: Unreconstructible axillary/subclavian injury
- Infection: Necrotizing fasciitis, gas gangrene, severe sepsis
- Radiation necrosis: Brachial plexopathy with non-functional painful limb
- Palliative: Fungating tumour causing suffering
Contraindications (Relative):
- Distant metastatic disease (relative - may still be palliative indication)
- Poor general health precluding major surgery
- Chest wall invasion requiring pneumonectomy (very high mortality)
- Patient refusal after informed consent
- Inadequate soft tissue for closure
Anatomy
Key Anatomical Structures
Understanding the anatomy is critical for safe forequarter amputation. The procedure involves controlling major neurovascular structures and dividing muscular attachments systematically.
Arterial Anatomy
- Becomes axillary artery at lateral border of first rib
- Relationship to scalenus anterior muscle is critical:
- First part: Medial to scalenus anterior (3 branches)
- Second part: Behind scalenus anterior (1 branch - costocervical trunk)
- Third part: Lateral to scalenus anterior (1 branch - dorsal scapular sometimes)
- Control is achieved infraclavicularly or supraclavicularly
- Subclavian vein is ANTERIOR to scalenus anterior
- More superficial than artery - encountered first in dissection
- Fragile wall - handle carefully
- Left side: Thoracic duct enters at junction with internal jugular vein
On the LEFT side, the thoracic duct must be identified and ligated. It enters the venous system at the junction of the left subclavian and internal jugular veins. Injury causes chylothorax - persistent lymphatic leak into the chest. If damaged, ligate proximally and distally.
Clinical Presentation and Assessment
Presentation by Aetiology
Oncological Presentation
- Progressively enlarging mass in proximal upper limb or shoulder girdle
- Pain - present in 50-70% of sarcomas at presentation
- Neurological symptoms if brachial plexus involved
- Vascular symptoms if axillary vessels compressed/invaded
- Mass greater than 5 cm
- Deep to fascia
- Increasing in size
- Painful
- Recurrence after previous excision
- Tumour involving neurovascular bundle that cannot be reconstructed
- Brachial plexus invasion by tumour
- Massive soft tissue involvement precluding functional limb
- Pathological fracture with extensive contamination
- Failed previous limb salvage with local recurrence
- Patient preference after informed discussion
Limb salvage is preferred when oncologically equivalent. Forequarter amputation is indicated when: (1) Neurovascular bundle involved and unreconstructible, (2) Brachial plexus invaded by tumour, (3) Massive soft tissue involvement, (4) Local recurrence after previous limb salvage. The decision is made by the MDT including orthopaedic oncologist, medical oncologist, radiation oncologist, and radiologist.
Preoperative Workup
Preoperative Assessment Protocol
Essential for malignancy:
- MRI of entire limb (local staging, skip lesions)
- CT chest (pulmonary metastases)
- PET-CT if indicated (distant staging)
- Biopsy confirmation (prior to any surgery)
- Review biopsy track for excision planning
- MDT discussion and consensus
All cases:
- Clinical pulse examination
- Doppler assessment
- CT angiography (vessel involvement by tumour, anatomy)
- Plan for vessel ligation level
- Cardiac risk assessment
Critical for outcomes:
- Dominant hand assessment
- Occupational therapy input (ADL assessment)
- Psychological assessment (mandatory before elective amputation)
- Realistic expectations discussion
- Prosthetic options counselling
- Social work input (financial, vocational)
Preoperative checklist:
- Full blood count, coagulation, group and screen (crossmatch 4 units)
- Renal and liver function
- Cardiac assessment (echo if indicated)
- Nutritional status (albumin greater than 30 g/L)
- Smoking cessation
- Anaesthetic review
Differential: Choosing the Right Shoulder-Girdle Procedure
The key "differential" for the examiner is not a diagnosis but which ablative/resective option fits the tumour. Forequarter amputation sits at the radical end of a spectrum.
- What is removed / spared
- Entire arm, scapula and lateral clavicle removed; no hand
- Key indication
- Plexus/vessel encasement, chest-wall extension, failed salvage
- Functional result
- No hand function; mainly cosmetic prosthesis, low uptake
- What is removed / spared
- Arm removed at glenohumeral joint; scapula and clavicle retained
- Key indication
- Distal tumour not involving scapula/plexus roots
- Functional result
- No hand; better stump contour than forequarter
- What is removed / spared
- Proximal humerus, scapula resected; neurovascular bundle and hand spared
- Key indication
- Tumour with a free neurovascular bundle
- Functional result
- Flail but sensate, useful hand (MSTS around 70%)
- What is removed / spared
- Proximal humerus only; deltoid/cuff spared where possible
- Key indication
- Contained bone tumour, no soft-tissue breach
- Functional result
- Best preserved shoulder and hand function
Surgical Technique
Anterior (Berger) Approach
- Standard approach for most oncological cases
- Preferred when tumour is posterior
- Provides early vascular control
- Better visualization of neurovascular structures
- Semi-lateral decubitus or supine with sandbag
- Arm free-draped
- Access to both anterior and posterior chest
- Start at sternoclavicular joint
- Along clavicle to acromioclavicular joint
- Curve inferolaterally around deltoid
- Continue down medial arm to axilla
- Return across chest wall below pectoralis
Anterior Approach Operative Steps
Incise skin along marked line.
Raise skin flaps anteriorly and posteriorly.
Preserve pectoralis major if oncologically safe.
Identify clavicle and prepare for osteotomy site.
Critical step - control vessels BEFORE mobilization.
Incise clavipectoral fascia below clavicle.
Identify subclavian/axillary artery - control with vessel loops.
Identify subclavian/axillary vein - control with vessel loops.
Ligate and divide artery FIRST, then vein.
On LEFT side, identify and ligate thoracic duct.
Divide clavicle at junction of middle and lateral thirds.
Use oscillating saw or Gigli saw.
Clear periosteum to prevent bone regrowth.
Smooth cut edges with rasp.
Lateral fragment stays with specimen.
Level of division depends on tumour extent.
Standard: Divide cords in axilla.
If plexus involved: Divide at trunk level or root level.
Apply gentle traction to each cord/trunk.
Sharp transection with fresh blade.
Allow proximal retraction.
Divide pectoralis major (or reflect if preserving).
Divide pectoralis minor from coracoid.
Divide subclavius muscle.
Release all anterior attachments of specimen.
Turn patient or work posteriorly.
Divide trapezius along medial scapular border.
Divide rhomboid major and minor.
Divide levator scapulae.
Divide serratus anterior from chest wall.
Divide latissimus dorsi (or preserve for flap).
Remove specimen en bloc.
Confirm haemostasis - inspect chest wall carefully.
Check for pleural injury.
Myoplasty: Approximate residual muscles over chest wall.
Closed suction drains.
Skin closure - consider flap if defect large.
Postoperative Care and Rehabilitation
Immediate Postoperative Care
- ICU or high-dependency monitoring
- Monitor for haemorrhage (drain output, haemoglobin)
- Chest X-ray to exclude pneumothorax
- DVT prophylaxis (mechanical and pharmacological)
- Analgesia: Multimodal approach (regional block if possible)
- Psychological support initiated
- Mobilization with physiotherapy
- Wound inspection at 48 hours
- Drain removal when output less than 30 ml/24 hours
- Respiratory physiotherapy
- Psychology review
- Wound care instructions
- Physiotherapy exercises
- Outpatient psychology follow-up
- Prosthetic referral when wound healed
- Oncology follow-up for adjuvant therapy
Prosthetic Rehabilitation
- Lightweight, realistic appearance
- No active function
- Improves body image and clothing fit
- Most commonly chosen option
- Body-powered or myoelectric
- Limited function compared to lower limb prosthetics
- Requires significant training
- Heavy, often abandoned
Upper limb prosthetics cannot replicate hand function. Unlike lower limb prosthetics which can restore walking, upper limb prosthetics provide limited functional restoration. Many patients adapt to one-handed function rather than using prosthesis. Cosmetic benefit is primary value for most.
Psychological Support
- Body image disturbance is profound
- Loss of independence for bilateral activities
- Occupational implications (may not return to previous work)
- Social and intimacy concerns
- Phantom limb sensations and pain
- Preoperative counselling and assessment
- Postoperative support and monitoring
- Peer support groups
- Long-term psychological follow-up
- Treatment for depression, PTSD if needed
Patients undergoing major upper limb amputation are at increased risk of depression and suicide. This is particularly true for traumatic amputations in young patients. Early psychological intervention, ongoing monitoring, and appropriate psychiatric referral are essential components of care.
Guidelines, Registries & Global Practice
Global Epidemiology
Forequarter (interscapulothoracic) amputation is rare worldwide; even high-volume sarcoma centres perform only a handful per year. The largest contemporary oncologic series (MD Anderson, 47 cases over 11 years) confirms its rarity and that sarcoma is the dominant indication (around 79%), with recurrent disease and metastasis common at presentation. With the global shift toward limb-sparing surgery, the absolute number of forequarter amputations has fallen and most are now performed for failed salvage, neurovascular/plexus encasement, or palliation.
Side-by-Side Guideline Comparison
- Position on radical amputation
- Limb salvage first; amputation only when salvage cannot achieve clear margins or function
- Practical emphasis
- All suspected sarcomas to a specialist sarcoma MDT before biopsy
- Position on radical amputation
- Wide excision is standard; amputation reserved for unresectable neurovascular involvement
- Practical emphasis
- Reference-centre management, pre-treatment biopsy by the operating team
- Position on radical amputation
- Function- and margin-driven; amputation when limb salvage compromises oncological control
- Practical emphasis
- Neoadjuvant chemo/radiotherapy to enable salvage where possible
- Position on radical amputation
- Tikhoff-Linberg or extra-articular resection preferred when neurovascular bundle is free
- Practical emphasis
- Forequarter reserved for plexus/vessel encasement or chest-wall extension
There is broad international agreement: limb salvage is the default, forequarter amputation is reserved for tumours that cannot be excised with clear margins while preserving a functional limb, and every elective case passes through a specialist sarcoma MDT with biopsy performed at (or directed by) the treating centre.
Registry and Outcome Notes
No joint-replacement-style registry tracks amputations; outcome data come from national/regional cancer registries and single-centre sarcoma series. Reported figures cluster around a 5-year overall survival of roughly 20-30% (driven heavily by metastatic status at presentation), local recurrence in the region of 15-20%, and major complication rates of 20-30%. Prosthetic uptake is consistently low across series — a key counselling point.
High- vs Limited-Resource Practice Variation
- Typical pattern
- Neoadjuvant therapy, advanced imaging (MRI/PET-CT, CT angiography), free-flap reconstruction, formal psychology and prosthetic services
- Typical pattern
- Later presentation with larger/fungating tumours, more palliative and infective indications, primary or local-flap closure, restricted prosthetic access
In limited-resource settings forequarter amputation is more often performed for advanced or palliative disease and for life-threatening infection (necrotising fasciitis, gas gangrene), where rapid source control outweighs reconstructive ambition. Regardless of setting, early psychological support, occupational therapy for one-handed adaptation, and access to peer support remain core to recovery.
Controversies and Areas of Uncertainty
- Amputation vs limb salvage: With modern neoadjuvant therapy and reconstruction, the threshold for forequarter amputation keeps rising. Tikhoff-Linberg resection achieves comparable oncological control with a far more useful limb when the neurovascular bundle is free (Voggenreiter 1999), so the decision is increasingly about plexus/vessel involvement rather than tumour size alone.
- Extended forequarter (chest-wall resection): Whether to extend resection into the chest wall is debated. The largest series found better survival in extended cases — but largely because those patients had less metastatic disease, so the apparent benefit may reflect selection rather than the operation itself (Roubaud 2023).
- Role in brachial plexus avulsion: Amputation for the flail, painful, anaesthetic arm is contentious. It can relieve mechanical and shoulder pain, but neuropathic/phantom pain may persist or emerge, so it is never guaranteed to abolish pain and demands rigorous psychological selection.
- Phantom-pain prevention: Preventive perioperative regional analgesia and NMDA blockade reduce early phantom pain but with no durable long-term benefit (Schley 2006); mirror therapy helps refractory pain (Chan 2007). No single regimen is established as standard.
- Prosthetic value: Across series, prosthetic uptake after forequarter amputation is very low; whether to invest in functional myoelectric devices or accept a lightweight cosmetic prosthesis (or none) is an individualised, often controversial decision.
Extended Forequarter Amputation
The controversies and the Roubaud series name 'extended forequarter amputation' and the anatomy notes en bloc rib resection, but the body never defines this distinct, larger operation.
- What it is. An extended forequarter amputation is a standard forequarter plus en bloc resection of part of the chest wall (ribs, intercostal muscles and sometimes parietal pleura), for a tumour that has invaded the chest wall or thoracic inlet beyond the shoulder girdle.
- What it needs. It requires thoracic and reconstructive surgery involvement, chest-wall reconstruction (synthetic mesh with a myocutaneous flap) to restore integrity and prevent flail or herniation, and formal management of the pleural space with a chest drain. Morbidity, especially respiratory, is higher than a standard forequarter.
- The survival caveat. In the largest series, extended cases appeared to have better survival than standard forequarter - but because they had a lower metastatic burden, so the apparent benefit reflects patient selection, not the bigger operation (Roubaud). Extended forequarter is justified only when it can still deliver a clear margin in locally confined disease.
Q: What is an extended forequarter amputation, and does it improve survival?
A: An extended forequarter is a standard forequarter plus en bloc chest-wall resection (ribs, with or without intercostals and parietal pleura), for a tumour invading the chest wall or thoracic inlet beyond the shoulder girdle. It needs thoracic and reconstructive surgery, chest-wall reconstruction (mesh plus a myocutaneous flap to prevent flail or herniation) and pleural-space management (chest drain), with higher (respiratory) morbidity. In the largest series (Roubaud) extended cases appeared to have better survival - but this reflected selection (they had a lower metastatic burden), not the operation, so it is justified only when it delivers a clear margin in locally confined disease.
CLAVICLE SCAPULAForequarter Amputation - Anterior Approach Steps
Hook:Follow the CLAVICLE first, then sweep around to the SCAPULA - the two bones you're removing
TIPSForequarter Amputation Indications
Hook:TIPS for when the limb must go - Tumour leads the way
Recognising the Unresectable Shoulder-Girdle Tumour
The Wittig series names a specific triad that signals an unresectable shoulder-girdle tumour, but the body only refers generically to 'neurovascular involvement'.
- The decision hinges on the neurovascular bundle. Whether a shoulder-girdle tumour needs a forequarter amputation or can be salvaged (Tikhoff-Linberg) turns on one question: is the neurovascular bundle (axillary and subclavian vessels and the brachial plexus) free or encased? A free bundle allows a limb-sparing resection; an encased bundle mandates forequarter amputation (or palliation).
- The Wittig triad of unresectability. Clinically, the combination of limb pain, motor loss and an obliterated axillary vein (on venography or cross-sectional imaging) indicates brachial plexus infiltration and unresectability - in the Wittig series the axillary vein was obliterated in every patient and plexus encasement was confirmed at exploration.
- Confirm on imaging. Contrast-enhanced MRI and CT angiography/venography map vessel and plexus involvement before surgery; loss of the fat plane around, or frank encasement of, the vessels and plexus is what converts a potential salvage into a forequarter.
Q: How do you recognise a shoulder-girdle tumour that needs a forequarter amputation rather than limb salvage?
A: The decision turns on the neurovascular bundle (axillary/subclavian vessels + brachial plexus) - a free bundle allows limb-sparing (Tikhoff-Linberg) resection, an encased bundle mandates forequarter (or palliation). Clinically the Wittig triad - limb pain + motor loss + an obliterated axillary vein (on venography/imaging) - signals brachial plexus infiltration and unresectability (in Wittig's series the axillary vein was obliterated in every patient, with plexus encasement confirmed at exploration). Confirm with contrast MRI and CT angiography/venography - loss of the peri-vascular fat plane or vessel/plexus encasement is what converts a salvage into a forequarter.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 45-year-old woman presents with a large high-grade soft tissue sarcoma involving the proximal humerus, deltoid, and extending to the brachial plexus on MRI. CT chest shows no pulmonary metastases. The MDT has recommended forequarter amputation. How would you counsel this patient and describe your surgical approach?”
“A 28-year-old motorcyclist sustained a complete brachial plexus avulsion (C5-T1) 18 months ago. His arm is flail and anaesthetic. He has severe chronic neuropathic pain despite maximal medical therapy and has requested amputation. How would you approach this case?”
“During a forequarter amputation for a proximal sarcoma, you encounter brisk bleeding when dividing tissues in the infraclavicular region. Describe your management.”
Indications
- Tumour (90%): Proximal sarcoma, plexus invasion, failed limb salvage
- Trauma: Brachial plexus avulsion with useless painful limb
- Infection: Necrotizing fasciitis, gas gangrene (life before limb)
- Palliative: Fungating tumour, intractable pain
Approach Selection
- Anterior (Berger): Standard for oncology, early vessel control
- Posterior (Littlewood): Anterior chest wall involvement
- Combined: Large tumours, plexus invasion at roots
Critical Surgical Steps
- Control subclavian ARTERY first, then VEIN (prevents engorgement)
- Left side: Identify and ligate thoracic duct (prevents chylothorax)
- Clavicle division: Junction of middle and lateral thirds
- Brachial plexus: Divide at cords (standard) or roots (if invaded)
- Preserve pectoralis major if oncologically safe for coverage
Vascular Relations
- Subclavian artery: POSTERIOR to scalenus anterior
- Subclavian vein: ANTERIOR to scalenus anterior
- Thoracic duct: Left side only, enters at subclavian-IJV junction
Flap Options
- Pectoralis major: First choice if preserved
- Latissimus dorsi: Versatile if available
- Free flap: Large defects, irradiated field
Complications
- Haemorrhage: Meticulous vessel control, have blood ready
- Chylothorax: Left side thoracic duct injury - ligate
- Pneumothorax: Chest wall dissection - CXR post-op
- Phantom limb pain: 60-80%, multimodal treatment
- Psychological: Depression, body image - mandatory psychology
Prosthetics
- Cosmetic: Most common choice, lightweight, improves body image
- Functional: Limited utility, heavy, often abandoned
- Key message: Cannot replicate hand function
Key Numbers
- Phantom limb pain: 60-80%
- 5-year survival (sarcoma): 30-40%
- Local recurrence: 15-20%
- Return to employment: 70%
Evidence Base and Key Studies
Forequarter Amputation for High-Grade Shoulder Girdle Tumours (Royal Orthopaedic Hospital)
- Retrospective review of 20 forequarter amputations for Enneking IIB-III tumours (15 curative, 5 palliative)
- Overall 5-year survival 21.2%; curative cases 30.2%; median survival after palliative amputation 20.6 months
- Eight patients died within 2 years (4 of whom had palliative surgery)
- Two deaths were unrelated (septicaemia and suicide), underscoring psychological risk
- None of the patients used an artificial prosthesis, yet the operation retained a useful palliative and curative role
Palliative Forequarter Amputation for Metastatic Carcinoma of the Shoulder Girdle
- Eight patients with unresectable metastatic carcinoma (breast, squamous cell, hypernephroma, unknown primary) all presenting with intractable pain and a useless limb
- Venography showed axillary vein obliteration in every patient; the triad of pain, motor loss and obliterated axillary vein indicated unresectable brachial plexus infiltration
- All patients had dramatic pain relief and life-threatening haemorrhage/sepsis was alleviated
- Epineural bupivacaine catheters were used for postoperative analgesia
- No instances of phantom limb pain or adverse psychological reactions in this palliative cohort
Reconstruction of Forequarter and Extended Forequarter Amputations (Largest Oncologic Series)
- 47 oncologic forequarter (33) and extended forequarter (14) amputations at MD Anderson, 2008-2019 — the largest series to date
- Sarcoma in 79%; 34% presented with recurrent disease and 40% had distant metastases
- Median defect 351 cm2; flap reconstruction needed in 64%; immediate complications 17%, delayed 26%
- Median overall survival 21 months and 5-year overall survival 28.1%
- Metastasis at presentation was the strongest predictor of death (OR 3.98); extended forequarter cases had better survival owing to lower metastatic burden
Tikhoff-Linberg (Limb-Sparing) Resection vs Forequarter Amputation
- 19 consecutive interscapulothoracic (Tikhoff-Linberg) resections for shoulder-girdle tumours, mean follow-up 6.3 years
- Mean Musculoskeletal Tumor Society functional score 72% in survivors with a retained, functional hand
- Major procedure-related complications (1 infection, 2 local recurrences) in 3 of 19 patients
- 12 of 19 patients alive with no evidence of disease at follow-up
- Authors concluded limb-sparing resection is oncologically comparable and functionally superior to forequarter amputation
Continuous Brachial Plexus Block plus Memantine to Prevent Phantom Pain (RCT)
- Randomised double-blind trial in 19 patients with acute traumatic upper-limb amputation
- All received continuous brachial plexus ropivacaine analgesia for at least 7 days
- Added memantine (NMDA antagonist) reduced phantom limb pain prevalence and intensity at 4 weeks and 6 months
- No benefit was sustained at 12 months and no effect on established pain
- Supports early, aggressive perioperative regional analgesia for traumatic amputees
Phantom Pain and Phantom Sensations in Upper Limb Amputees
- Survey of 124 upper-limb amputees (80% response) in the Netherlands
- Phantom pain prevalence 51%, phantom (non-painful) sensations 76%, stump pain 49%
- 64% reported moderate to severe suffering from phantom pain
- Strong association between phantom pain and both phantom sensations (RR 11.3) and stump pain (RR 1.9)
- Only 4 patients had received any medical treatment for phantom pain
Mirror Therapy for Phantom Limb Pain (RCT)
- Randomised crossover trial comparing mirror therapy, covered mirror and mental visualisation
- Mirror therapy produced significant reduction in phantom limb pain
- Patients in the non-mirror groups who crossed over to mirror therapy also improved
- Low-cost, non-pharmacological adjunct with no significant adverse effects
- Established mirror therapy as a recognised option for refractory phantom pain
References
-
Bhagia SM, Elek EM, Grimer RJ, Carter SR, Tillman RM. Forequarter amputation for high-grade malignant tumours of the shoulder girdle. J Bone Joint Surg Br. 1997;79(6):924-926. PMID 9393905.
-
Wittig JC, Bickels J, Kollender Y, Kellar-Graney KL, Meller I, Malawer MM. Palliative forequarter amputation for metastatic carcinoma to the shoulder girdle region. J Surg Oncol. 2001;77(2):105-113. PMID 11398163.
-
Roubaud MS, Mericli AF, Adelman DM, Hanasono MM, Lewis VO, Moon BS. Reconstruction of forequarter and extended forequarter amputations: indications and outcomes. Plast Reconstr Surg. 2023;152(1):194-205. PMID 36728500.
-
Voggenreiter G, Assenmacher S, Schmit-Neuerburg KP. Tikhoff-Linberg procedure for bone and soft tissue tumors of the shoulder girdle. Arch Surg. 1999;134(3):252-257. PMID 10088563.
-
Kooijman CM, Dijkstra PU, Geertzen JH, Elzinga A, van der Schans CP. Phantom pain and phantom sensations in upper limb amputees: an epidemiological study. Pain. 2000;87(1):33-41. PMID 10863043.
-
Schley M, Topfner S, Wiech K, et al. Continuous brachial plexus blockade in combination with the NMDA receptor antagonist memantine prevents phantom pain in acute traumatic upper limb amputees. Eur J Pain. 2006;11(3):299-308. PMID 16716615.
-
Chan BL, Witt R, Charrow AP, et al. Mirror therapy for phantom limb pain. N Engl J Med. 2007;357(21):2206-2207. PMID 18032777.
-
Malawer MM, Sugarbaker PH. Musculoskeletal Cancer Surgery: Treatment of Sarcomas and Allied Diseases. Springer; 2001.
-
Canale ST, Beaty JH. Campbell's Operative Orthopaedics. 12th ed. Elsevier; 2013.
-
Damron TA, Sim FH. Forequarter amputation. In: Simon MA, Springfield D, eds. Surgery for Bone and Soft-Tissue Tumors. Lippincott-Raven; 1998.