Biology of Bone Repair
- Primary Healing: Requires absolute stability (less than 2% strain) + gap less than 0.1mm. Mechanism: Cutting Cones.
- Secondary Healing: Occurs with relative stability (2-10% strain). Mechanism: Enchondral Ossification (Callus).
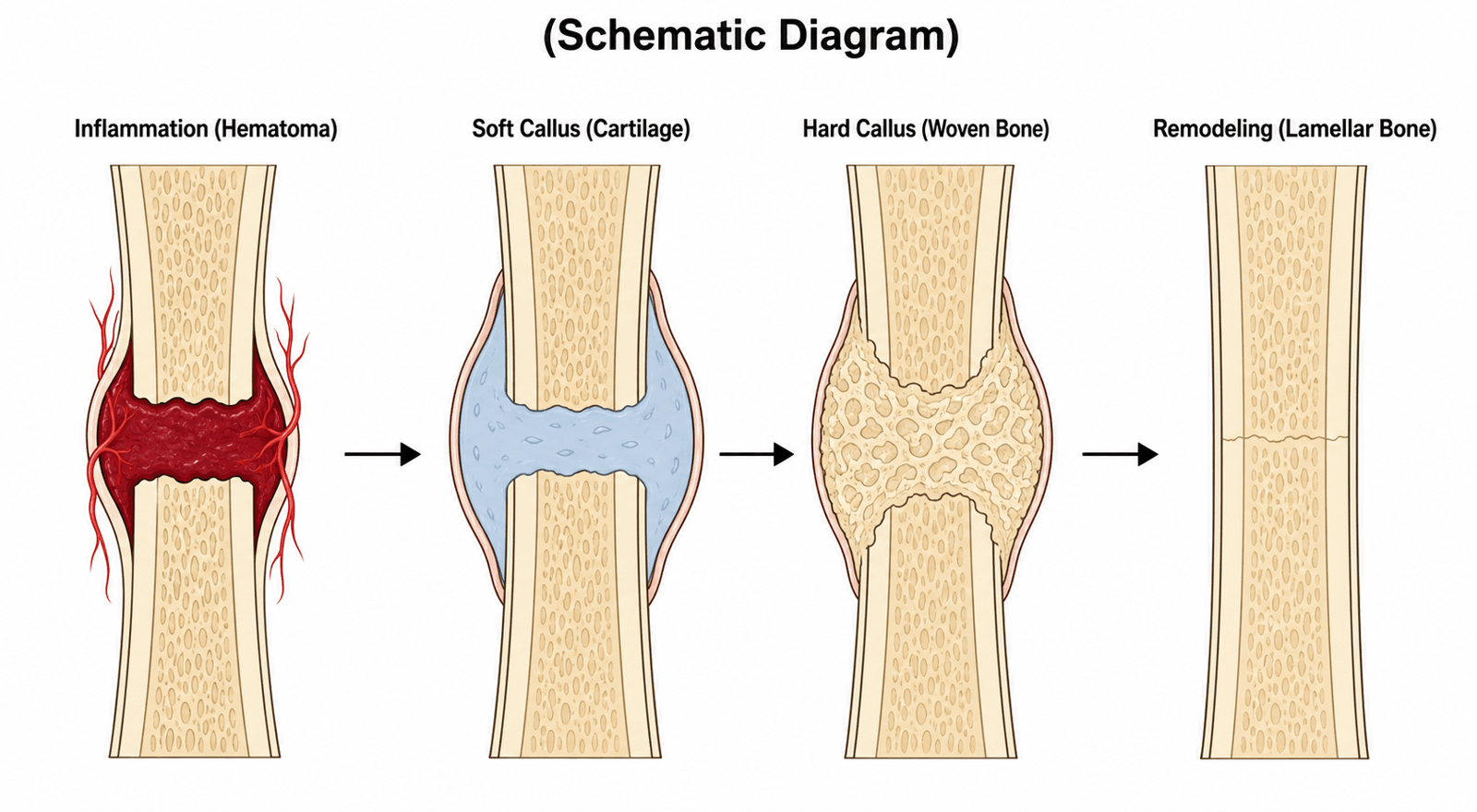
- Phases: Inflammation → Soft → Hard → Remodeling
- Diamond Concept: The holy grail of union = Cells + Scaffold + Signals + Mechanical Stability.
- Perren's Strain Theory: Tissues can only exist if they can withstand the mechanical strain of the environment.
- “Soft Callus = Type II Collagen (Cartilage). Hard Callus = Type I Collagen (Bone).
- “Primary Healing has NO callus.
- “BMP-2 = Open Tibia (INFUSE). BMP-7 = Non-union (OP-1).
- “Nicotine is a potent vasoconstrictor and inhibitor of healing.
Primary Healing. Occurs when strain is less than 2%. Compression plating eliminates micromotion. The bone thinks it is intact and remodels via cutting cones.
Secondary Healing. Occurs when strain is 2-10%. IM nails allow micromotion. The body responds by throwing down cartilage (callus) to stiffen the gap.
Overview and Epidemiology
Overview Fracture healing is the process of bone regeneration. Unlike other tissues which heal by scar formation, bone heals by regeneration of normal tissue structure. It is a complex cascade of cellular and biochemical events that restores the integrity of the bone.
Primary (Direct) Healing
- Definition: Bone healing without callus formation.
- Prerequisites: Absolute Stability (Strain less than 2%) + Anatomic Reduction.
- Mechanism (Gap less than 0.01 mm): Cutting Cones (Osteoclasts bore tunnels, Osteoblasts fill with osteoid).
- Gap Mechanism (Gap less than 1 mm): Gap healing (Woven bone to Refined by Cutting Cones).
Secondary (Indirect) Healing
- Definition: The natural form of healing involving callus.
- Prerequisites: Relative Stability (Strain 2-10%) + Vitality.
- Phases:
- Inflammation: Hematoma, MSC recruitment.
- Soft Callus: Cartilage formation (Enchondral ossification).
- Hard Callus: Mineralization (Woven bone).
- Remodeling: Wolff's Law (Lamellar bone).
Biology and Core Concepts
Biology of Bone Before understanding healing, one must understand the players.
Cellular Components
- Osteoblasts ("Build"):
- Secrete Osteoid (Type I Collagen) and regulate mineralization.
- Express RANK-L to control osteoclasts.
- Derived from Mesenchymal Stem Cells (MSCs).
- Osteocytes ("Sense"):
- Mechanosensors trapped in lacunae deep within the mineralized matrix.
- Communicate via canaliculi.
- Secrete Sclerostin (inhibits bone formation). Mechanical loading inhibits Sclerostin (allowing bone formation).
- Osteoclasts ("Chew"):
- Multinucleated giant cells derived from Monocyte/Macrophage lineage (Hematopoietic).
- Resorb bone via acid secretion (HCL) and proteases (Cathepsin K).
- Activated by RANK-L. Inhibited by OPG.
The Matrix
- Inorganic (65%): Hydroxyapatite (Calcium Phosphate crystals). Provides compressive strength.
- Organic (35%):
- Collagen Type I (90%): Provides tensile strength. Triple helix structure.
- Non-Collagenous Proteins: Osteocalcin (marker of turnover), Osteopontin (cell attachment), BMPs (growth factors).
Blood Supply
- Centrifugal Flow (Normal): Marrow → Cortex → Periosteum. (Inside to Outside).
- Centripetal Flow (Post-Fx): Periosteum → Cortex → Marrow. (Outside to Inside). The Periosteal blood supply becomes dominant after medullary disruption (e.g., reaming). This highlights the importance of preserving the soft tissue envelope (periosteum) during surgery.
Biophysics of Stimulation
- Piezoelectricity:
- Stress on collagen generates electric potentials.
- Compression side: Electronegative → Stimulates Osteoblasts (Bone Formation).
- Tension side: Electropositive → Stimulates Osteoclasts (Bone Resorption).
- Streaming Potentials: Fluid flow in canaliculi stimulates osteocytes.
Biomechanics (Strain Theory)
Perren's Strain Theory: Tissues can only exist if they can withstand the strain of the gap.
- Strain Formula: Change in Gap / Original Gap.
- Bone: Ruptures at 2% Strain.
- Cartilage/Granulation: Tolerates greater than 10% Strain.
- Conclusion: To form bone (Primary), strain must be less than 2%. To heal via callus (Secondary), granulation tissue first stiffens the gap, reducing strain to allow cartilage, then bone.
The Fracture Hematoma and the Inflammatory Phase
The phases open with "Inflammation: Hematoma, MSC recruitment," but the hematoma is not inert debris - it is the first regenerative signal, and preserving it is a surgical goal rather than an afterthought.
Why the hematoma matters
- The fracture hematoma forms within minutes and provides both a fibrin scaffold and a reservoir of platelet-derived signalling molecules (PDGF, TGF-beta).
- Experimentally, excising or preventing the early hematoma impairs union, whereas a transplanted hematoma can itself induce bone. This is the biological reason to preserve the hematoma with closed/indirect reduction and to avoid over-stripping the fracture ends.
The acute pro-inflammatory burst (first 24-72 hours)
- Neutrophils and then macrophages infiltrate and release a coordinated cytokine wave: TNF-alpha, IL-1, IL-6, IL-11 and IL-18.
- These cytokines are chemotactic for mesenchymal stem cells, promote angiogenesis, and prime the periosteal and marrow progenitors that will build callus.
- Macrophages are obligatory: their depletion in models markedly impairs callus formation, and the switch from pro-inflammatory (M1) to reparative (M2) macrophages marks the transition out of the inflammatory phase.
Angiogenesis precedes osteogenesis
- The injured, hypoxic fracture site stabilises HIF-1-alpha, driving VEGF and new-vessel ingrowth. No vessels, no bone - revascularisation must precede mineralisation, which is why periosteal blood supply and gentle soft-tissue handling dominate the outcome.
The COX-2 link
- Prostaglandins generated by COX-2 during this inflammatory phase are required for progenitor differentiation and the soft-to-hard callus conversion. This is the mechanistic basis for the NSAID caution developed elsewhere in this topic - blunting the inflammatory signal can blunt healing. (The clinical NSAID evidence is covered in the Controversies and Factors sections; the dedicated
nsaids-in-orthopaedicstopic holds the full drug discussion.)
Q: Why does a well-preserved fracture hematoma help union? A: It is an active signalling depot, not passive clot - a fibrin scaffold plus a cytokine cascade (TNF-alpha, IL-1, IL-6, IL-11, IL-18) from macrophages that recruits MSCs and drives HIF-1-alpha/VEGF angiogenesis. Angiogenesis must precede osteogenesis, so preserving biology (closed reduction, minimal stripping) preserves healing.
Classification Systems
Healing Pathways
- Primary (Direct) Healing:
- Contact Healing: Less than 0.01mm gap. Cutting cones cross directly. Haversian remodeling.
- Gap Healing: Less than 1mm gap. Woven bone fills gap first (scaffold), then cutting cones remodel it.
- Secondary (Indirect) Healing:
- Inflammation → Soft Callus → Hard Callus → Remodeling.
- Requires micromotion.
- Distraction Osteogenesis:
- Intramembranous ossification via tension stress (Ilizarov).
- Requires: Stability, Latency (7 days), Rate (1mm/day), Rhythm (4x 0.25mm).
These pathways exist on a spectrum.
Clinical Assessment
History
- Pain: Resolution of pain is the first sign of union.
- Function: Ability to weight bear. Return to activities of daily living.
- Risk Factors: Ask about smoking, diabetes, steroid use, NSAIDs.
Physical Exam
- Tenderness: No tenderness at fracture site (Clinical Union).
- Motion: No abnormal mobility (Clinical Union).
- Stress: Painless stressing of the fracture.
- Soft Tissue: Assess status of the envelope (healed wounds, skin grafts).
Investigations
Radiographic Assessment (RUST Score)
- Radiographic Union Scale for Tibial fractures (RUST).
- Methodology: Review AP and Lateral X-rays. Identify the 4 cortices (Anterior, Posterior, Medial, Lateral).
- Scoring Per Cortex:
- 1 Point: Fracture line visible, No callus. (Unhealed)
- 2 Points: Fracture line visible, Callus present. (Healing)
- 3 Points: Fracture line invisible, Bridging callus. (Healed)
- Interpretation:
- Minimum Score: 4 (Unhealed).
- Maximum Score: 12 (Fully United).
- Clinical Definition of Union: Score of greater than 10 usually correlates with mechanical stability and ability to weight bear without pain.
- General Signs: Bridging bone on 3 of 4 cortices. Blurring of fracture line. Remember: X-rays lag behind clinical signs.
Assessment of Non-Union
- CT Scan: Gold standard to assess bridging. Can differentiate bony union from fibrous non-union.
- Labs: Vitamin D, PTH, Calcium, ESR/CRP (Infection).
- MRI: Assessing infection (osteomyelitis) vs sterile non-union.
Management Algorithm
- 1Assess fracture healing at 3-6 months
Review clinical signs (resolution of pain, painless stressing) and radiographs for clinical and radiographic union.
Clinical + radiographic union present?
- 2If united: clinical + radiographic union
No tenderness, no abnormal mobility, bridging callus on imaging.
good outcome
- 3If not united: pain or no bridging
Persistent pain or absent bridging callus at the expected time point.
proceed to next step
- 4Determine biologic vs mechanical failure
Assess callus formation on serial imaging to separate a stability problem from a biology problem.
Is callus present (hypertrophic) or absent (atrophic)?
- 5Hypertrophic (callus present)
Good biology (the body is trying to heal) but poor stability - the 'elephant foot' appearance.
warning
- 6Atrophic (no callus)
Poor biology - sclerotic, 'pencil-tip' bone ends with vascular failure.
critical
Management: Conservative
Casting Principles
- Three-Point Molding: To maintain reduction, pressure must be applied at the apex of the curve and counter-pressure at the proximal/distal ends.
- Functional Bracing (Sarmiento):
- Allows joint motion.
- Hydrostatic containment of soft tissues stabilizes the fracture.
- Micro-motion stimulates callus (Secondary Healing).
- Common for: Humeral shaft, Tibial shaft.
Biologic Adjuvants
When biology is poor (Atrophic Non-union), we augment it.
Bone Grafts
- Autograft (Self):
- Source: Iliac Crest (Gold Standard), RIA (Reamer Irrigator Aspirator - Femur).
- Properties: Osteogenic (Cells) + Osteoinductive (Signals) + Osteoconductive (Scaffold).
- Cons: Donor site morbidity (pain, infection, nerve injury).
- Allograft (Cadaver):
- Source: Bone bank (structural struts or morcellized chips).
- Properties: Osteoconductive strictly. (No cells, minimal signals).
- Cons: Disease transmission (rare 1 in 1 million), slower incorporation, immune reaction (minor).
- Synthetics (Ceramics/TCP):
- Properties: Osteoconductive (Scaffold).
- Cons: Brittle, expensive, can cause seroma.
Growth Factors
- BMP-2 (Infuse):
- Potent Osteoinductor. Indicated for Acute Open Tibia fractures.
- Mechanism: Recruits MSCs to differentiate into osteoblasts.
- Risks: Swelling (C-spine airway compromise), Heterotopic ossification, Cost.
- BMP-7 (OP-1): Historic use for non-unions.
- PRP/BMAC: Bone Marrow Aspirate Concentrate. Rich in MSCs and growth factors (PDGF, TGF-beta).
Systemic Anabolic Pharmacology to Augment Healing
The biology section noted that osteocytes secrete sclerostin (a brake on bone formation) and that mechanical loading switches it off. That makes sclerostin - and the PTH/Wnt axis - a druggable target for accelerating healing, distinct from the local osteoinductive BMP grafts covered under Biologic Adjuvants (and in the dedicated growth-factors-bone-healing topic).
Teriparatide (recombinant PTH 1-34)
- Intermittent (once-daily) PTH is anabolic - it favours osteoblast survival and enhances callus formation, the opposite of the catabolic effect of continuously elevated PTH seen in hyperparathyroidism.
- Used off-label to support healing in selected fragility fractures and established non-unions (for example pelvic and vertebral insufficiency fractures, and atypical femoral fractures related to bisphosphonates).
- Not licensed for fracture healing: supportive evidence exists but is limited and heterogeneous, so it stays an adjunct in high-risk hosts, not routine care. It is avoided where a bone tumour, skeletal metastasis, Paget disease, or prior skeletal irradiation is a concern.
Anti-sclerostin antibody (romosozumab)
- A monoclonal antibody that neutralises sclerostin, giving a dual effect - increased formation and reduced resorption - and licensed for osteoporosis.
- Mechanistically attractive for healing because loading normally suppresses sclerostin, but dedicated fracture-healing acceleration trials (tibial and hip) have not met their primary endpoints, so it is not established for speeding union.
Do not conflate with anti-resorptives
- Bisphosphonates and denosumab are anti-resorptive, not pro-healing; they do not accelerate union, and bisphosphonates are linked to atypical femoral fractures - a separate problem from augmenting repair.
Q: Why does teriparatide build bone when hyperparathyroidism destroys it? A: Intermittent PTH (once-daily teriparatide) favours osteoblast survival and callus formation, whereas continuously elevated PTH is net catabolic. Teriparatide and anti-sclerostin (romosozumab) target the PTH/Wnt-sclerostin axis this topic introduces, but both remain off-label or unproven for routinely accelerating fracture union.
Factors Affecting Healing
Patient Optimization
- Smoking:
- Nicotine is a vasoconstrictor of microvasculature.
- Carbon Monoxide binds Hemoglobin (hypoxia).
- Increases non-union risk significantly (e.g., Tibia, Fusion, Ankle).
- Diabetes:
- Microvascular disease (ischemia).
- AGEs (Advanced Glycation End-products) inhibit collagen cross-linking.
- Decreased cellular proliferation.
- Medications:
- NSAIDs: Inhibit COX-2, which is needed for Enchondral Ossification (Soft to Hard Callus conversion). Controversial, but generally avoided in high-risk fractures.
- Steroids: Inhibit osteoblasts and calcium absorption.
- Bisphosphonates: Inhibit osteoclasts (remodeling). Long half-life. Can cause atypical fractures.
- Quinolones: Toxic to chondrocytes? (Minor factor).
- Nutrition:
- Albumin less than 3.5 = Malnutrition.
- Vitamin D / Calcium essential for mineralization.
Optimizing the host is as important as the surgery.
History of Fracture Treatment
Historical Evolution
- Ancient Era: Splinting and casting (Egyptians).
- 1950s (AO Foundation):
- Founded by Mueller, Allgower, et al.
- Emphasis on Anatomic Reduction and Rigid Fixation.
- Result: Primary healing, but high non-union rate due to biological stripping.
- 1990s (Biological Fixation):
- Shift to MIPO (Minimally Invasive Plate Osteosynthesis) and IM Nails.
- Emphasis on Biology (Blood supply) over Anatomy.
- Acceptance of secondary healing (Callus).
- Future: Gene therapy (BMP), 3D printed scaffolds, Stem Cells.
- Gene Therapy: Viral vectors delivering BMP-2 genes to local cells.
- 3D Printing: Custom scaffolds matching the defect, seeded with MSCs.
- Biophysical Stimulation:
- LIPUS: Low Intensity Pulsed Ultrasound. Mechanical vibration stimulates integrins.
- PEMF: Pulsed Electromagnetic Fields. Induces electrical currents (streaming potentials) to stimulate calcification. NOTE: Contraindicated in patients with pacemakers.
Surgical Technique
Compression Plating (Absolute Stability)
- Mechanism: Primary Healing.
- Principles:
- Anatomic Reduction: Essential for articular surfaces.
- Compression: Achieved via Lag Screw (interfragmentary) or DCP Plate (axial).
- Indication:
- Articular fractures (must be perfect).
- Forearm fractures (length/rotation).
- Osteotomy sites.
- Disadvantage: Wide exposure (strips blood supply). High strain if gap remains.
Primary healing is intolerant of gaps.
- Modulus (GPa)
- 200 GPa
- Biological Effect
- Very Rigid. Good for absolute stability.
- Modulus (GPa)
- 110 GPa
- Biological Effect
- Less Rigid (closer to bone). Better for load sharing.
- Modulus (GPa)
- 15-20 GPa
- Biological Effect
- Target stiffness.
- Modulus (GPa)
- 0.1-1 GPa
- Biological Effect
- Spongy.
Biomaterials and Healing The stiffness of the implant dictates the strain at the fracture site.
- Stress Shielding: If an implant is too stiff (e.g., thick steel plate), it takes all the load. The bone beneath it senses no load (strain less than 2%) but also no "need" for strength. This causes bone resorption (Wolff's Law in reverse) and porosis under the plate.
- Titanium: Being less stiff (closer to bone), it allows some load transfer, reducing stress shielding.
- Carbon Fiber: Even closer modulus to bone. Used in oncology (radiolucent).
Complications of Healing
Healing does not always go to plan.
1. Delayed Union
- Definition: Healing that takes longer than expected for the specific fracture and host (typically 3-6 months), but is still progressing.
- Management:
- Conservative: Functional bracing, LIPUS (Low Intensity Pulsed Ultrasound), Nutrition.
- Surgical: Dynamization (remove locking screws) to increase load/strain.
2. Non-Union
- Definition: Failure to heal by 6-9 months, or no progression on X-rays for 3 consecutive months (FDA definition).
- Types:
- Septic Non-Union: Infection until proven otherwise. Check CRP/ESR. MRI.
- Hypertrophic: Good Biology, Poor Stability. (Needs Stability). Elephant Foot appearance.
- Atrophic: Poor Biology. (Needs Biology + Stability). Pencil Tip appearance.
- Oligotrophic: Intermediate.
- Workup:
- History: Smoking, Diabetes, NSAIDs.
- Exam: Mobility at fracture site? Sinus?
- Imaging: CT Scan (Gold Standard for union).
- Labs: Infection markers, Vitamin D, Ca/PO4, PTH.
3. Malunion
- Definition: Healed but in a non-anatomic position.
- Parameters: Shortening, Rotation, Angulation.
- Tolerance:
- Humeral Shaft: Tolerates huge deformity (20 deg angulation, 3cm shortening).
- Forearm: Zero tolerance (loss of pronation/supination).
- Tibia: Tolerates minimal varus/valgus (less than 5 deg).
4. Synostosis
- Definition: Fusion between two adjacent bones (e.g., Radius/Ulna, Tibia/Fibula).
- Cause: Disruption of Interosseous Membrane (IOM) + High Energy + Same approach (single incision).
- Consequence: Loss of rotation (Forearm).
- Timing / Definition
- Slower than expected but still progressing
- Imaging Clue
- Some callus, fracture line persists
- Action
- Optimise host, protected loading, observe
- Timing / Definition
- No progression 3 months; good biology
- Imaging Clue
- Abundant callus, 'elephant foot'
- Action
- Add STABILITY (revise fixation)
- Timing / Definition
- No progression; poor biology
- Imaging Clue
- No callus, sclerotic 'pencil-tip' ends
- Action
- Add BIOLOGY (debride + graft) + stability
- Timing / Definition
- Stalled healing + sepsis markers
- Imaging Clue
- Lysis, sequestrum, periosteal reaction; MRI/labs
- Action
- Treat infection first, then reconstruct
- Timing / Definition
- Healed in non-anatomic position
- Imaging Clue
- Bridged but deformed (angulation/rotation/short)
- Action
- Assess function; osteotomy if symptomatic
Postoperative Care
Early Phase (0-2 weeks)
- Elevation: Reduce edema.
- Motion: Early ROM (if fixation allows) to prevent stiffness and stimulate blood flow.
- Review: Wound check.
Middle Phase (2-6 weeks)
- Loading: Proprioceptive weight bearing. Wolff's law stimulation.
- X-rays: Check alignment and maintenance of reduction.
Late Phase (6-12 weeks)
- Strengthening: Restore muscle mass.
- Full Weight Bearing: When hard callus visible (3/4 cortices).
- Goal
- Protect Soft Tissue
- Restrictions
- NWB / Elevation
- Biology
- Hematoma Formation
- Goal
- Prevent Stiffness
- Restrictions
- Touch WB / ROM
- Biology
- Soft Callus (Cartilage)
- Goal
- Load the Bone
- Restrictions
- Progressive WB
- Biology
- Hard Callus (Bone)
- Goal
- Return to Sport
- Restrictions
- Full Activity
- Biology
- Haversian Remodeling
Outcomes and Prognosis
Time to Union (Average)
- Upper Limb: 6-8 weeks.
- Lower Limb: 12-16 weeks.
- Tibia: Slowest bone to heal (poor blood supply). 16-20 weeks common for open fractures.
Non-Union Rates
- Tibia: 10-15% (especially open). The most common long bone non-union.
- Femur: 1-2% (with IM nail). Success story of modern orthopaedics.
- Clavicle: 5-10% (conservative).
- Scaphoid: High rate due to retrograde blood supply.
Factors Predicting Poor Outcome
- Smoking (Odds ratio greater than 3).
- Open fracture (Gustilo III).
- Infection.
- NSAID use (Prolonged).
Pediatric Healing
Key Differences
- Speed: Heals twice as fast. High osteogenic potential of thick, vascular periosteum.
- Remodeling Potential:
- Can correct Angulation (in plane of motion).
- Cannot correct Rotation.
- Overgrowth: Femur fractures stimulate growth (1-2cm leg length discrepancy common) due to hyperemia.
- Physeal Injuries:
- Growth arrest (Physeal bar) → Deformity.
- Salter-Harris Classification.
Children are not just small adults.
Guidelines, Registries & Global Practice
Global Epidemiology
- Tibial shaft fracture is the most common long-bone fracture; nonunion affects roughly 5-15% (highest with open injuries and segmental bone loss).
- Smoking, diabetes, NSAID exposure, and high-energy/open injury are consistent risk factors for impaired union worldwide.
Side-by-Side Society Guidance
- Stance on BMP / Stimulators
- BMP-2 an option for selected open tibial fractures; bone stimulators not routinely recommended
- Key Healing Principle
- Early debridement and soft-tissue cover for open fractures
- Stance on BMP / Stimulators
- Stimulators not endorsed; emphasis on biology and stability
- Key Healing Principle
- Combined ortho-plastic fixation and flap within 72h
- Stance on BMP / Stimulators
- Adjuncts reserved for compromised biology
- Key Healing Principle
- Diamond concept: cells + scaffold + signals + stability
- Stance on BMP / Stimulators
- Cautious; reserve BMP for non-union/high-risk
- Key Healing Principle
- Preserve periosteal blood supply; relative stability for diaphysis
Registry & Trial Signals
- Large RCTs (SPRINT, TRUST, BESTT) anchor practice: ream closed tibial nails, LIPUS adds no benefit for fresh fractures, BMP-2 reduces reoperation in open tibiae.
- National trauma/arthroplasty registries (NJR, AOANJRR, Swedish/Norwegian) track reoperation and nonunion as quality metrics rather than implant survival for diaphyseal fixation.
High- vs Limited-Resource Practice
- High-resource: routine IM nailing, CT for suspected nonunion, ortho-plastic flap cover, selective BMP/autograft.
- Limited-resource: external fixation and functional bracing (Sarmiento) remain mainstays; autograft (iliac crest) preferred over costly BMP/synthetics; clinical and plain-radiograph union assessment.
Smoking Cessation (Universal Principle)
- Offer behavioural support plus pharmacotherapy (nicotine replacement, varenicline, or bupropion where available).
- For elective osteotomy/fusion, aim for cessation before surgery; cotinine testing can confirm abstinence.
Controversies and Areas of Uncertainty
- NSAIDs: Animal data and a meta-analysis (OR ~2.1 overall) suggest impaired union, but the effect is dose- and duration-dependent and absent in children. Short low-dose courses for simple fractures are likely safe; prolonged use is best avoided in high-risk cases. True equipoise persists.
- Bone stimulators (LIPUS/PEMF): The TRUST RCT showed no benefit for fresh tibial fractures. Their role, if any, is debated for established non-union where high-level evidence is lacking.
- BMP use: Reduces reoperation in open tibiae, but cost, swelling, heterotopic ossification and off-label spinal complications have narrowed enthusiasm; reserved for selected high-risk or non-union cases.
- Reaming in open fractures: SPRINT showed benefit only in closed tibial fractures; the closed-vs-open reaming question remains debated, especially in contaminated wounds.
- Optimal definition of union: No universally accepted radiographic threshold exists. RUST improves reliability but CT is often needed; clinical and radiographic union frequently disagree.
- Biologic adjuncts (PRP/BMAC, synthetics): Widely marketed but supported mainly by low-level evidence; routine use is not established.
Preoperative Planning
Planning for Union
- Patient: Stop smoking, Optimize diabetes, Nutrition.
- Implant: Choose load-sharing (Nail) vs load-bearing (Plate) based on fracture pattern and soft tissue.
- Biology: Preserve soft tissue (Open reduction vs Closed).
Mnemonics
CSSMThe Diamond Concept
Hook:What you need for a Union.
I-S-H-RPhases of Healing
Hook:I Shall Heal Right.
N-I-C-O-T-I-N-ENon-Union Risk Factors
Hook:Causes of Non-Union.
MCQ Practice Points
Q: What type of collagen is found in soft callus? A: Type II Collagen. (Think "Two" for "Tissue" / Cartilage). Hard callus replaces it with Type I (Bone).
Q: How do Osteoclasts attach to bone? A: Via the Sealing Zone (Integrins, specifically alpha-v beta-3). They create a "Howship's Lacuna" and secrete H+ ions (acid) to dissolve mineral.
Q: A simple fracture is plated with a bridging plate (long span). Why might it fail? A: Strain Concentration. In a simple gap, all motion is concentrated. Strain = Motion / Gap. Small gap = High Strain. Bridging plates work best in comminuted fractures (Strain = Motion / Long Gap).
Q: What is the odds ratio for non-union in smokers? A: Greater than 3. Smoking is the most significant modifiable risk factor.
Q: What are the 4 pillars of the Diamond Concept for fracture healing? A: C-S-S-M: Cells (osteogenic), Scaffold (osteoconductive), Signals (osteoinductive BMPs), and Mechanical stability.
Specific Fracture Scenarios
The Tibial Shaft (The "Unforgiving Bone")
- Anatomy: One third is subcutaneous (anteromedial surface). Poor blood supply.
- Healing: Slow (16-20 weeks).
- Management: IM Nail (standard) vs Plate (distal/proximal).
- Pearl: Reamed nailing creates a "bonfire" of growth factors and autograft.
The Scaphoid (Retrograde Flow)
- Anatomy: Blood enters distal pole. Proximal pole depends on intraosseous flow.
- Risk: Proximal pole fracture → Avascular Necrosis (AVN).
- Healing: Compression screw (Herbert screw) buried in bone.
The Clavicle (S-Shaped Strut)
- Anatomy: Membranous bone formation (unique).
- Malunion: Shortening greater than 2cm affects shoulder biomechanics (scapular dyskinesis).
- Non-Union: Atrophic common in smokers.
The Femoral Neck (Intracapsular)
- Anatomy: Synovial fluid washes away hematoma (no clot = no callus).
- Result: Must heal by Primary Healing (Compression).
- Risk: AVN due to medial circumflex artery damage.
The Humeral Shaft
- Healing: Typically 8-12 weeks.
- Acceptance: Accepts up to 20 degrees anterior angulation and 30 degrees varus/valgus due to shoulder range of motion compensation.
- Nerve: Radial nerve palsy (Holstein-Lewis fracture in distal third). 90% resolve spontaneously. Watch and wait for 3 months if closed injury.
The Distal Radius (Colles)
- Healing: 6 weeks for bony union.
- Remodeling: Limited in adults. Malunion (shortening) leads to ulnar impaction syndrome.
- Management: Volar locking plate allows early motion.
The Ankle (Weber B)
- Mortise: 1mm shift = 42% decrease in contact area.
- Healing: 6 weeks NWB (Syndesmosis) or 2 weeks NWB then boot (stable).
- Risk: Post-traumatic arthritis if articular step greater than 2mm.
The Pelvis (Ring)
- Healing: Cancellous bone heals fast (6-8 weeks).
- Weight Bearing: Depends on posterior ring stability (Sacrum/SIJ).
- Complication: Venous Thromboembolism (highest risk in orthopaedics).
The Fifth Metatarsal (Jones Fracture)
- Zone 2: Metaphyseal-Diaphyseal junction.
- Physics: Adductor longus traction creates tension side failure.
- Healing: Poor blood supply. High non-union rate.
- Management: Screw fixation often required for athletes.
At a Glance
- Primary (Direct)
- Absolute (No motion)
- Secondary (Indirect)
- Relative (Micromotion)
- Primary (Direct)
- Less than 2%
- Secondary (Indirect)
- 2% - 10%
- Primary (Direct)
- Haversian Remodeling
- Secondary (Indirect)
- Enchondral Ossification
- Primary (Direct)
- NO Callus
- Secondary (Indirect)
- YES Callus (Bridging)
- Primary (Direct)
- Lag Screw + Neutralization Plate
- Secondary (Indirect)
- Intramedullary Nail
Exam Day Cheat Sheet
Primary (Direct)
- Absolute Stability
- less than 2% Strain
- Cutting Cones
- No Callus
Secondary (Indirect)
- Relative Stability
- 2-10% Strain
- Callus (Enchondral)
- IM Nail
PHASES
- Inflammation 0-1wk
- Soft callus 1-3wk
- Hard callus 3-12wk
- Remodeling months-years
Diamond Concept
- Cells
- Scaffold
- Signals
- Stability
Future Directions
The Next Frontier The future of fracture healing lies in targeted biological intervention.
- Personalized Medicine: Genetic profiling for non-union risk.
- Smart Implants: Sensors embedded in plates to measure strain and notify patients when to weight bear.
- Bio-printing: 3D printed vascularized bone grafts.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“Patient with a tibial shaft fracture asks why they need to stop smoking. Convince them.”
“Show me an X-ray of a non-union. How do you classify it and treat it?”
“A simple transverse mid-shaft femoral fracture is fixed with a bridging locked plate and fails to form callus, then breaks the plate. What went wrong, biomechanically?”
Evidence Base
BMP-2 for Open Tibial Fractures (BESTT)
- Prospective, randomized, single-blind RCT of 450 patients with open tibial shaft fractures treated with IM nailing.
- 1.50 mg/mL rhBMP-2 on a collagen sponge gave a 44% reduction in risk of secondary intervention (RR 0.56, 95% CI 0.40-0.78).
- Significantly faster fracture and wound healing, fewer hardware failures, and fewer infections in Gustilo type-III injuries.
- Basis for FDA approval in acute open tibial shaft fractures stabilized with an IM nail.
NSAIDs and Bone Healing (Meta-analysis)
- Random-effects meta-analysis of NSAID exposure and bone healing across adult and pediatric studies.
- NSAID exposure increased delayed union/nonunion (OR 2.07, 95% CI 1.19-3.61).
- No significant effect in children (OR 0.58, 95% CI 0.27-1.21).
- No significant effect with low-dose/short-duration exposure (OR 1.68, 95% CI 0.63-4.46) - effect is dose- and time-dependent.
SPRINT Trial (Reamed vs Unreamed Nailing)
- Multicenter blinded RCT of 1319 adults with a tibial shaft fracture (reamed vs unreamed IM nailing).
- In CLOSED fractures, reamed nailing reduced the primary composite outcome (RR 0.67, 95% CI 0.47-0.96; p=0.03), largely driven by less dynamization.
- In OPEN fractures, no significant difference (RR 1.27, 95% CI 0.91-1.78; p=0.16).
- Delaying reoperation for nonunion until at least 6 months substantially reduced the need for reoperation.
The Diamond Concept
- Reframed bone regeneration around four equally weighted pillars rather than the older triangular tissue-engineering model.
- Pillars: osteogenic cells, osteoconductive scaffold, osteoinductive signals, and mechanical stability.
- Argued the mechanical environment is consistently underweighted in non-union strategy.
- Provides the framework for systematically assessing and treating non-unions.
TRUST Trial (LIPUS)
- Concealed, blinded, sham-controlled RCT of 501 operatively managed tibial fractures.
- No difference in time to radiographic healing (HR 1.07, 95% CI 0.86-1.34; p=0.55).
- No difference in SF-36 physical component score or other functional measures.
- Postoperative LIPUS did not accelerate healing or improve functional recovery.
Smoking and Tibial Fracture Healing (Global Meta-analysis)
- Systematic review and meta-analysis of 12 observational studies conducted worldwide.
- Smoking associated with increased non-union, delayed union, and longer time to union of tibial shaft fractures.
- 8 of 12 studies reported increased non-union rates with smoking.
- Reinforces smoking cessation counselling as a core part of fracture care globally.