Rare but Devastating | Immunocompromised Hosts | Prolonged Therapy Required
- Candida and Aspergillus account for 75% of fungal spine infections in immunocompromised patients
- Diagnosis requires tissue biopsy with fungal cultures (blood cultures often negative)
- MRI shows paravertebral abscess and epidural extension more commonly than bacterial infections
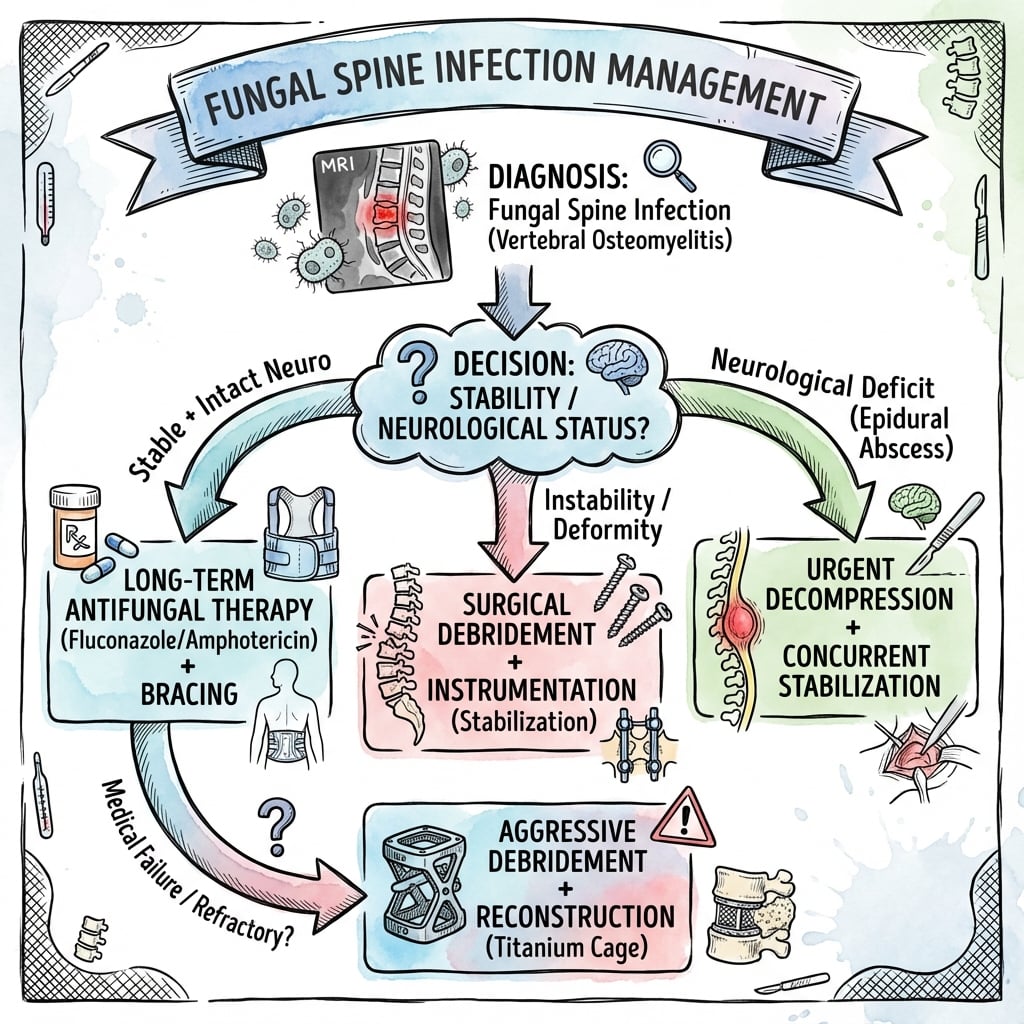
- Treatment requires prolonged antifungal therapy (6-12 months) PLUS surgical debridement if neurological compromise
- Mortality reaches 30-50% in disseminated aspergillosis despite treatment
- “Think fungal in immunocompromised patient with spine infection not responding to antibacterial therapy
- “Beta-D-glucan and galactomannan serum assays help diagnose invasive fungal infection
- “Endemic mycoses (Coccidioides, Histoplasma) occur in specific geographic regions - travel history critical
- “Aspergillus causes bony destruction with less disc involvement compared to bacterial infections
Immunocompromised hosts are primary targets. HIV/AIDS with CD4 less than 100, solid organ transplant recipients on immunosuppression, hematological malignancies undergoing chemotherapy, chronic corticosteroid use (greater than 20mg prednisone daily for over 3 weeks), diabetes mellitus with poor glycemic control.
Blood cultures often negative (60-70% of cases). Requires tissue biopsy via CT-guided needle or open surgical biopsy. Send fresh tissue for fungal culture (NOT formalin) and fungal stains (GMS, PAS). Fungal cultures take 2-6 weeks to grow. Molecular testing (PCR) and serology (beta-D-glucan, galactomannan) aid rapid diagnosis.
Paravertebral and epidural extension more common than bacterial. T2 hyperintense paraspinal masses often with rim enhancement. Subligamentous spread uncommon. Bony destruction may be more prominent than disc involvement especially in Aspergillus. Multiple non-contiguous levels suggest hematogenous dissemination.
Minimum 6-12 months antifungal therapy. Much longer than bacterial infections (6 weeks). Treat until clinical resolution, CRP normalization, and radiographic improvement. Surgical debridement if neurological deficit, spinal instability, or failure of medical therapy. Lifelong suppression may be needed in severe immunosuppression.
CACAOCommon Fungal Pathogens
Hook:Think CACAO when considering fungal spine infection - the sweet (but deadly) pathogens!
Overview and Epidemiology
Fungal spine infections (fungal spondylodiscitis or vertebral osteomyelitis) are rare but serious infections accounting for only 1-2% of all spinal infections. However, incidence is rising due to increasing numbers of immunocompromised patients from HIV, solid organ transplantation, chemotherapy, and chronic immunosuppressive medications.
Fungal spine infections are easily missed because they mimic bacterial infections clinically but do not respond to antibacterial therapy. Delayed diagnosis leads to progressive neurological deficit, spinal instability, and disseminated disease with high mortality (30-50% in aspergillosis). High index of suspicion required in immunocompromised patients with spine infection. Tissue biopsy is gold standard for diagnosis.
Immunocompromised hosts predominate:
- HIV/AIDS with CD4 less than 100 cells/mcL
- Solid organ transplant recipients
- Hematological malignancies (leukemia, lymphoma)
- Chronic corticosteroid use (greater than 20mg/day for more than 3 weeks)
- Diabetes mellitus with HbA1c greater than 9%
- IV drug use (Candida from contaminated needles)
- Recent spine surgery or invasive procedures
Endemic mycoses have specific geography:
- Coccidioides: Southwest USA (California, Arizona, New Mexico)
- Histoplasma: Mississippi and Ohio River valleys
- Blastomyces: Great Lakes region, Mississippi valley
- Cryptococcus: Worldwide but higher in AIDS patients
- Aspergillus and Candida: Worldwide, nosocomial
Pathophysiology and Microbiology
Routes of Infection
- Common Organisms
- Candida, Aspergillus, endemic fungi
- Clinical Scenario
- Disseminated infection from lungs, GI tract, or bloodstream
- Spinal Involvement
- Vertebral body and disc via arterial seeding, often multifocal
- Common Organisms
- Candida, Aspergillus
- Clinical Scenario
- Postoperative infection from contaminated surgical field or implants
- Spinal Involvement
- Localized to surgical site, may involve hardware
- Common Organisms
- Actinomyces (cervical)
- Clinical Scenario
- Extension from adjacent site (retropharyngeal, mediastinal)
- Spinal Involvement
- Progressive involvement of adjacent vertebrae and soft tissues
Specific Fungal Pathogens
Candida Spondylodiscitis
Most common fungal pathogen (50% of cases)
Species: C. albicans most common, but C. glabrata, C. tropicalis, C. parapsilosis increasingly recognized
Risk factors:
- Prolonged ICU stay with central lines
- Total parenteral nutrition (TPN)
- Recent broad-spectrum antibiotics
- Abdominal surgery
- IV drug use
Clinical features:
- Indolent onset over weeks to months
- Back pain with low-grade fever
- Often diagnosed late when neurological deficit develops
Treatment:
- Fluconazole 400-800mg daily PO for susceptible species (C. albicans, C. tropicalis)
- Echinocandin (micafungin 100mg IV daily) for resistant species or critically ill patients
- Duration: minimum 6 months, up to 12 months if extensive disease
Candida has good disc involvement with disc space narrowing on imaging.
Mucormycosis of the Spine: the Angioinvasive Emergency
The risk-factor and poor-prognosis lists name mucormycosis (as a diabetic risk and a bad-prognosis pathogen), but it is never developed - a dangerous omission, because it behaves and is treated very differently from Candida and Aspergillus and is a surgical emergency.
- Agents and hosts. Caused by the Mucorales (Rhizopus, Mucor, Rhizomucor, Lichtheimia, Cunninghamella). The classic host is uncontrolled diabetes, especially diabetic ketoacidosis (acidosis impairs neutrophils and frees iron), plus iron overload / deferoxamine therapy (the drug acts as a siderophore that delivers iron to the fungus), haematological malignancy/neutropenia and transplantation, and - for the spine specifically - IV drug use and direct/traumatic inoculation.
- Why it is different: angioinvasion. Mucorales are angioinvasive - they invade blood vessels causing thrombosis, infarction and rapid, extensive tissue necrosis. Disease spreads fast, and antifungals penetrate the dead, thrombosed tissue poorly - which is why surgery is central, not adjunctive.
- On histology. Broad (wide), non-septate (pauci-septate), ribbon-like hyphae with wide-angle (approximately 90-degree), irregular branching - contrast with Aspergillus (narrow, septate hyphae, acute-angle, approximately 45-degree branching). Cultures are frequently negative, so the diagnosis is often made on histology; do not wait for a culture to act.
- Treatment - and the fatal trap. It is a surgical emergency: urgent, aggressive and often repeated surgical debridement of all necrotic tissue, PLUS liposomal amphotericin B (first-line), with isavuconazole or posaconazole for step-down/salvage. Voriconazole, fluconazole and the echinocandins are INEFFECTIVE against Mucorales - so a patient on voriconazole for presumed Aspergillus who deteriorates may in fact have mucormycosis. Reverse the driver (correct DKA/hyperglycaemia, stop deferoxamine, reduce immunosuppression). Mortality is very high.
Q: How does spinal mucormycosis differ from Aspergillus in host, histology and treatment? A: Host = uncontrolled diabetes/DKA, iron overload/deferoxamine, neutropenia. It is angioinvasive (thrombosis, infarction, rapid necrosis). Histology = broad, non-septate, ribbon-like hyphae with wide-angle (~90 degrees) branching (vs Aspergillus's narrow septate ~45-degree hyphae); cultures often negative. Treatment = urgent aggressive surgical debridement + liposomal amphotericin B (then isavuconazole/posaconazole), and crucially voriconazole and echinocandins do NOT cover Mucorales - so worsening on voriconazole should raise the suspicion of mucor.
FUNGALRisk Factors for Fungal Spine Infection
Hook:When spine infection is FUNGAL - look for these key risk factors in patient history!
Actinomyces and Nocardia: the Filamentous Bacteria That Masquerade as Fungi
The CACAO mnemonic and the routes-of-infection table both flag Actinomyces ("technically bacteria but mimics fungus") but never develop it, and its close mimic Nocardia is not mentioned at all. Both are filamentous, branching Gram-positive bacteria that can be mistaken for fungi - but they are treated with antibiotics, not antifungals, so recognising them changes management completely.
- Actinomyces (e.g. A. israelii). An anaerobic/microaerophilic branching Gram-positive filament that is endogenous flora (oropharynx, GI tract, female genital tract). It reaches the spine by contiguous spread - classically cervicofacial ("lumpy jaw") extending to the cervical spine, or thoracic (aspiration) and abdominopelvic (IUD-associated) disease invading adjacent vertebrae. It crosses tissue planes and the disc, forms chronic indurated masses with sinus tracts discharging "sulfur granules", and is NOT acid-fast. Treatment is prolonged high-dose penicillin (IV then oral, often 6-12 months) - not antifungals.
- Nocardia (e.g. N. asteroides complex). An aerobic branching Gram-positive filament that is weakly/partially acid-fast (modified Ziehl-Neelsen / Kinyoun) - the key feature separating it from Actinomyces. It is environmental (soil), affects the immunocompromised (steroids, transplant, malignancy), and typically causes primary pulmonary disease with haematogenous dissemination to brain and bone/spine. Treatment is high-dose co-trimoxazole (TMP-SMX), often with a carbapenem or amikacin for severe disease, and is prolonged.
- Why this matters here. When a "fungal-looking" granulomatous spine infection is actually Actinomyces or Nocardia, the cure is antibiotics. The practical safeguard is to send the biopsy for bacterial (aerobic AND anaerobic), fungal and mycobacterial culture with the right stains (Gram, modified acid-fast) and to avoid anchoring on an "antifungal" plan.
Q: How do you distinguish Actinomyces and Nocardia from fungi, and how does treatment differ? A: Both are filamentous branching Gram-positive BACTERIA treated with antibiotics, not antifungals. Actinomyces = anaerobic, endogenous, contiguous spread (cervicofacial "lumpy jaw"), sulfur granules and sinus tracts, NOT acid-fast - treat with prolonged penicillin. Nocardia = aerobic, environmental, partially acid-fast, immunocompromised host, pulmonary-then-disseminated - treat with co-trimoxazole (TMP-SMX). Always culture the biopsy for bacteria (aerobic and anaerobic), fungi and mycobacteria so these mimics are not missed.
Clinical Presentation
Clinical Features
Indolent onset over weeks to months:
- Back pain (90%) - insidious, progressively worsening
- Low-grade fever (40-60%) - may be absent
- Night sweats and weight loss (40%)
- Radicular pain if nerve root compression (30%)
- Neurological deficit (50-70%) - often presents late
- Constitutional symptoms less prominent than bacterial
Focal findings:
- Spine tenderness at affected level
- Reduced range of motion
- Neurological exam: motor, sensory, reflex deficits
- Assess for epidural abscess: saddle anesthesia, bowel/bladder dysfunction
- Look for other sites: pulmonary (crackles), skin lesions, retinal lesions (Candida endophthalmitis)
Investigations
Diagnostic Approach
Diagnostic Workup for Suspected Fungal Spine Infection
Inflammatory markers: ESR and CRP elevated but less dramatically than bacterial (ESR 40-80mm/hr typical) Complete blood count: Leukocytosis may be absent, anemia of chronic disease common Blood cultures: Positive in only 30-40% of fungal infections (versus 50-60% bacterial) Fungal serology: Beta-D-glucan (Candida, Aspergillus), galactomannan (Aspergillus), Coccidioides serology if endemic exposure HIV testing: All patients with suspected fungal infection should be tested for HIV
MRI spine with contrast (GOLD STANDARD): Shows extent of vertebral involvement, disc involvement, paravertebral abscess, epidural extension, neural compression. T2 hyperintense paraspinal masses with rim enhancement characteristic. Aspergillus shows more bone destruction, less disc involvement. CT spine: Better defines bony destruction and cortical integrity. Useful for surgical planning. Chest/abdominal CT: Evaluate for pulmonary or disseminated fungal infection (aspergillosis, coccidioidomycosis).
CT-guided needle biopsy (initial approach): Send fresh tissue (NOT formalin) for fungal culture and bacterial culture. Also send for fungal stains (GMS, PAS) and AFB stains. Cultures may take 2-6 weeks to grow. Open surgical biopsy if needle biopsy non-diagnostic or neurological deficit requiring decompression: Obtain multiple tissue samples from vertebral body, disc, and abscess. Send fresh tissue for cultures and histopathology. Histopathology: Look for granulomas, fungal elements on GMS or PAS stains. Characteristic morphology helps identify organism (Aspergillus: septate hyphae with acute-angle branching).
PCR testing: Rapid identification of Aspergillus, Candida, endemic fungi from tissue or fluid samples MALDI-TOF mass spectrometry: Rapid species identification from culture isolates Antifungal susceptibility testing: Essential for Candida (resistance to fluconazole common in C. glabrata) and Aspergillus
Blood cultures are negative in 60-70% of fungal spine infections. Empiric antibacterial therapy often started before fungal diagnosis considered. High index of suspicion required when spine infection fails to improve on appropriate antibiotics. Tissue biopsy (CT-guided or open surgical) is MANDATORY for definitive diagnosis. Do NOT send tissue in formalin - send FRESH for culture. Fungal cultures take 2-6 weeks, so maintain suspicion and consider empiric antifungal therapy while awaiting results.
Imaging Characteristics
- Bacterial
- Early and prominent
- Fungal (Candida)
- Moderate
- Fungal (Aspergillus)
- Minimal or late
- Bacterial
- Moderate
- Fungal (Candida)
- Moderate
- Fungal (Aspergillus)
- Severe and extensive
- Bacterial
- Common (50-70%)
- Fungal (Candida)
- Very common (70-90%)
- Fungal (Aspergillus)
- Very common (80-90%)
- Bacterial
- 30-50%
- Fungal (Candida)
- 50-70%
- Fungal (Aspergillus)
- 60-80%
- Bacterial
- Common (contiguous levels)
- Fungal (Candida)
- Less common
- Fungal (Aspergillus)
- Rare
- Bacterial
- Rare (unless bacteremia)
- Fungal (Candida)
- Common (hematogenous)
- Fungal (Aspergillus)
- Common (hematogenous)
Management
Treatment Algorithm
Antifungal Therapy by Organism
- First-Line Treatment
- Fluconazole 400-800mg PO daily
- Alternative
- Micafungin 100mg IV daily
- Duration
- 6-12 months
- First-Line Treatment
- Micafungin 100mg IV daily
- Alternative
- Caspofungin 70mg loading, then 50mg daily
- Duration
- 6-12 months
- First-Line Treatment
- Voriconazole 200mg PO BID (after loading)
- Alternative
- Liposomal amphotericin B 5mg/kg IV daily
- Duration
- 12 weeks to 12 months
- First-Line Treatment
- Fluconazole 400-800mg PO daily
- Alternative
- Liposomal amphotericin B (severe cases)
- Duration
- 12-18 months, often lifelong
- First-Line Treatment
- Itraconazole 200mg PO BID
- Alternative
- Liposomal amphotericin B (severe cases)
- Duration
- 12+ months
Fungal spine infections require PROLONGED therapy (minimum 6-12 months, often longer) compared to bacterial infections (6 weeks). Treat until clinical resolution, CRP normalization, and radiographic improvement. Monitor drug levels for voriconazole and itraconazole (significant inter-patient variability). Combination therapy (medical PLUS surgical) often needed for optimal outcomes. Lifelong suppressive therapy may be necessary in patients who remain severely immunosuppressed (AIDS with CD4 less than 100, transplant recipients).
Monitoring and Follow-up
- Clinical response: Monitor pain, fever, neurological status weekly initially
- Inflammatory markers: CRP and ESR monthly - should trend down over 3-6 months
- Drug levels: Voriconazole trough 1-5.5mcg/mL, itraconazole trough greater than 1mcg/mL
- Toxicity monitoring: LFTs monthly (azole hepatotoxicity), creatinine (amphotericin nephrotoxicity), visual changes (voriconazole)
- Imaging: MRI at 3 months and 6 months to assess response - expect slow radiographic improvement
Failure to improve clinically or radiographically at 3 months suggests need for surgical intervention or change in antifungal regimen.
SPORETreatment Principles
Hook:Treat fungal spine infections like SPORES - they take time to eradicate and require comprehensive approach!
Complications and Outcomes
- Incidence
- 20-40% in Aspergillus
- Risk Factors
- Severe immunosuppression, delay in diagnosis
- Management
- Systemic antifungals, manage end-organ dysfunction, high mortality 30-50%
- Incidence
- 30-50% if untreated
- Risk Factors
- Epidural abscess, delayed diagnosis, medical therapy failure
- Management
- Urgent surgical decompression, continue antifungals, outcomes variable
- Incidence
- 40-60% with vertebral collapse
- Risk Factors
- Aspergillus (severe bone destruction), inadequate reconstruction
- Management
- Surgical correction with anterior column support and posterior instrumentation
- Incidence
- 20-30%
- Risk Factors
- Inadequate debridement, premature discontinuation of antifungals, persistent immunosuppression
- Management
- Repeat debridement, change antifungal regimen, prolong therapy, address immune status
- Incidence
- 30-40%
- Risk Factors
- Prolonged therapy, liver disease, drug interactions
- Management
- Monitor LFTs monthly, adjust doses, switch agents if severe hepatotoxicity
Guidelines, Registries & Global Practice
Global Epidemiology
Fungal spine infection accounts for roughly 1-2% of all spinal infections worldwide, with a reported incidence near 2.2 per 100,000 person-years. Distribution is driven by host immunosuppression (HIV, transplantation, haematological malignancy, chronic steroids, diabetes) and by geography for the endemic mycoses. Candida and Aspergillus occur worldwide and are largely healthcare- or immunosuppression-associated, whereas Coccidioides (Southwest USA, parts of Central/South America), Histoplasma (Americas, parts of Africa/Asia) and Blastomyces (North America) are geographically restricted. In published pooled series the lumbar spine is most often affected, with male predominance and a mean age in the mid-50s.
Side-by-Side Guidance
- Scope
- Candidiasis, aspergillosis, coccidioidomycosis guidelines
- Key Position
- Drug-specific, organism-led: echinocandin then fluconazole step-down for Candida bone disease; voriconazole first-line for Aspergillus; prolonged azole/lifelong suppression for disseminated Coccidioides
- Scope
- Aspergillus and Candida management
- Key Position
- Aligns with voriconazole/isavuconazole first-line for invasive aspergillosis; therapeutic drug monitoring of azoles emphasised
- Scope
- Spinal infection pathways
- Key Position
- Tissue diagnosis before antimicrobials where feasible, MDT (spine + ID + microbiology), surgery for instability or neural compromise
- Scope
- Global prioritisation
- Key Position
- Aspergillus fumigatus and Candida species (incl. C. auris) listed as critical/high priority, underscoring rising resistance and need for susceptibility testing
Registries and Practice Variation
There is no dedicated arthroplasty-style registry for spinal fungal infection; evidence rests on pooled case series and surveillance networks (e.g. ECMM/FungiScope, national antifungal-resistance surveillance such as CDC/EUCAST programmes). High-resource settings emphasise molecular diagnostics (PCR, MALDI-TOF), beta-D-glucan/galactomannan assays, therapeutic drug monitoring of azoles, and ready access to liposomal amphotericin B and newer triazoles. In limited-resource settings, delayed diagnosis, restricted access to voriconazole/isavuconazole and amphotericin formulations, and overlap with tuberculosis (which is far more common and radiographically similar) drive worse outcomes and a lower threshold for empiric anti-tuberculous therapy before fungal disease is considered.
In TB-endemic regions, granulomatous spinal infection is assumed tuberculous until proven otherwise. Fungal disease should be reconsidered when there is failure of anti-tuberculous therapy, an immunocompromised host, relevant travel to mycosis-endemic areas, or negative TB cultures with persistent granulomatous tissue.
Controversies and Areas of Uncertainty
Whether to start empiric antifungals in a deteriorating high-risk patient while awaiting culture (which takes 2-6 weeks) versus holding therapy to preserve culture yield is unresolved. Most authorities favour empiric cover in the immunocompromised, deteriorating patient, accepting reduced culture sensitivity.
Minimum 6-12 months is widely cited but evidence is observational. The endpoint (CRP normalisation, radiographic resolution, or fixed duration) and the role of indefinite suppression in persistent immunosuppression remain debated, with no randomised data.
Unlike high-virulence bacterial infection, instrumentation is generally retained because fungal biofilm behaviour and the need for stability differ. The threshold for hardware removal versus suppression over retained metal is not standardised.
Combination antifungal therapy (e.g. voriconazole plus an echinocandin or amphotericin) for severe or refractory spinal aspergillosis is extrapolated from invasive aspergillosis data; spine-specific evidence is absent and toxicity is additive.
The use of high-dose corticosteroids to reduce cord oedema in fungal epidural compression is controversial: steroids may worsen the underlying fungal infection and immunosuppression. There is no high-quality evidence; decisions are individualised and made with infectious diseases input.
MCQ Practice Points
Q: What is the most common fungal pathogen causing spondylodiscitis? A: Candida species (50% of cases) - Most common fungal pathogen, followed by Aspergillus (25%). Candida spondylodiscitis typically occurs in healthcare-associated settings (ICU, central lines, TPN) or in IV drug users. Treatment is fluconazole 400-800mg daily for 6-12 months.
Q: What is the gold standard for diagnosing fungal spine infection? A: Tissue biopsy with fungal culture - Blood cultures are negative in 60-70% of fungal spine infections. Tissue biopsy (CT-guided needle or open surgical) is mandatory. Send FRESH tissue (NOT formalin) for fungal culture and fungal stains (GMS, PAS). Cultures take 2-6 weeks to grow. Serology (beta-D-glucan, galactomannan) and PCR can aid rapid diagnosis.
Q: What is the first-line antifungal for invasive aspergillosis including spinal involvement? A: Voriconazole - NEJM 2002 trial showed voriconazole superior to amphotericin B for invasive aspergillosis (71% vs 58% survival at 12 weeks). Dose: 200mg PO BID after loading dose. Monitor drug levels (target trough 1-5.5mcg/mL). Alternative: liposomal amphotericin B 5mg/kg IV daily. Duration: minimum 12 weeks, often 6-12 months for spinal disease.
Q: What MRI finding is more characteristic of fungal versus bacterial spine infection? A: Extensive paravertebral and epidural extension with relative disc sparing (especially Aspergillus) - Fungal infections more commonly have large paraspinal abscesses (70-90% vs 50-70% bacterial) and epidural extension (50-80% vs 30-50% bacterial). Aspergillus preferentially destroys bone with less disc involvement compared to bacterial infections. Multiple non-contiguous levels suggest hematogenous fungal dissemination.
Q: A patient with disseminated coccidioidomycosis and spinal involvement asks how long antifungal therapy will be needed. What do you tell them? A: Lifelong suppressive therapy is often required for disseminated coccidioidomycosis - Unlike localized pulmonary disease (treat 3-6 months), disseminated coccidioidomycosis with spinal involvement requires prolonged therapy (minimum 12-18 months, often lifelong) to prevent relapse. Relapse rates 20-30% if therapy discontinued in disseminated disease. Treatment is fluconazole 400mg daily or higher doses.
Q: What are the absolute indications for surgical intervention in fungal spine infection? A: Progressive neurological deficit, spinal instability, epidural abscess with cord compression, medical treatment failure - Combination therapy (surgery PLUS antifungals) has better outcomes than medical therapy alone; in pooled data, surgery lowered mortality versus medical-only treatment for Aspergillus (26.9% vs 60%) and Candida (0% vs 28.6%). Surgery provides tissue diagnosis, decompresses neural elements, debrides infected tissue, and allows definitive pathogen identification. Medical failure defined as progression despite 4-6 weeks of appropriate antifungal therapy.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 52-year-old renal transplant recipient on tacrolimus and prednisone presents with 6 weeks of progressive low back pain and low-grade fever. He was treated with 2 weeks of IV cefazolin for presumed bacterial spondylodiscitis without improvement. MRI shows L3-L4 spondylodiscitis with large paravertebral abscess and mild epidural extension. Blood cultures are negative. How would you approach this case?”
“A 45-year-old woman with acute myeloid leukemia post-chemotherapy presents with acute onset bilateral lower extremity weakness and urinary retention. She has had 4 weeks of back pain. MRI shows T10-T11 spondylodiscitis with severe vertebral body destruction and epidural abscess causing cord compression. CT-guided biopsy 2 weeks ago grew Aspergillus fumigatus. She has been on voriconazole 200mg BID for 10 days. Exam shows 2/5 bilateral lower extremity strength and T10 sensory level. How do you manage this patient?”
“A 38-year-old previously healthy man who recently relocated from Arizona to a non-endemic country presents with 6 months of progressive back pain, night sweats, and 10kg weight loss. MRI shows multifocal spondylodiscitis at L1-L2 and L4-L5 with extensive paravertebral abscesses bilaterally. He has mild lower extremity weakness (4/5). Coccidioides serology is positive with high titers. How would you counsel and manage this patient?”
Key Pathogens and Epidemiology
- Candida (50%) - healthcare-associated, IV drug use, immunocompromised
- Aspergillus (25%) - hematological malignancies, transplant, high mortality 30-50% if disseminated
- Coccidioides - endemic Southwest USA, disseminated disease requires lifelong therapy
- Histoplasma/Blastomyces - endemic mycoses, Mississippi/Ohio valleys and Great Lakes region
- Only 1-2% of all spine infections but rising incidence due to more immunocompromised patients
Clinical Recognition
- Think fungal if spine infection fails to respond to appropriate antibacterial therapy
- Indolent onset over weeks to months with low-grade fever (or absent)
- Neurological deficit in 50-70% (often late presentation)
- Risk factors: HIV CD4 less than 100, transplant, chemotherapy, chronic steroids greater than 20mg daily, diabetes
- Blood cultures negative in 60-70% - tissue biopsy is MANDATORY
Diagnostic Approach
- MRI: extensive paravertebral/epidural extension more than bacterial, disc sparing in Aspergillus
- Tissue biopsy (CT-guided or surgical) is gold standard - send FRESH (NOT formalin) for culture
- Fungal stains: GMS (Grocott methenamine silver), PAS (periodic acid-Schiff)
- Serology: beta-D-glucan (Candida/Aspergillus), galactomannan (Aspergillus), Coccidioides titers
- Fungal cultures take 2-6 weeks to grow - consider empiric therapy in high-risk patients
Treatment by Organism
- Candida albicans: fluconazole 400-800mg daily PO × 6-12 months
- Candida glabrata (resistant): micafungin 100mg IV daily × 6-12 months
- Aspergillus: voriconazole 200mg BID PO (monitor levels) × 12 weeks to 12 months
- Coccidioides disseminated: fluconazole 400-800mg daily, often lifelong suppression
- Surgery if neurological deficit, instability, medical failure, or extensive destruction
Surgical Indications and Approach
- Absolute: progressive neuro deficit, spinal instability, epidural abscess with cord compression, medical failure
- Combination therapy (surgery + antifungals) superior to medical alone (lower mortality: Aspergillus 26.9% vs 60%, Candida 0% vs 28.6% in pooled review)
- Posterior decompression for epidural abscess, laminectomy, instrumentation if instability
- Anterior corpectomy for vertebral body destruction, reconstruct with cage (avoid autograft)
- Combined anterior-posterior for severe destruction, maximum debridement and stability
Outcomes and Prognosis
- Candida: 70-80% cure rate with combination therapy, good neurological recovery if early surgery
- Aspergillus disseminated: 30-50% mortality despite treatment, localized spinal 70-80% survival
- Coccidioides disseminated: requires lifelong therapy, relapse 20-30% if discontinued
- Treatment failure/relapse 20-30% overall - inadequate debridement, early discontinuation, persistent immunosuppression
- Monitor CRP/ESR monthly (should trend down), MRI at 3 and 6 months, drug levels for voriconazole/itraconazole
Evidence Base
Fungal Infections of the Spine: Literature Review
- Review of 130 articles representing 157 cases of fungal spine infection (1948-2010)
- Aspergillus (38.2%) was the single most common pathogen, followed by Candida (22.9%)
- Surgery plus antifungals carried lower mortality than medical therapy alone for Aspergillus (26.9% vs 60%) and Candida (0% vs 28.6%)
- Overall mortality 19.3% and overall recurrence 7.4%
- Amphotericin use was associated with higher mortality than newer azoles
Voriconazole for Invasive Aspergillosis
- Randomized trial of 277 patients with invasive aspergillosis: voriconazole vs amphotericin B deoxycholate
- 12-week survival higher with voriconazole (70.8% vs 57.9%; hazard ratio 0.59, 95% CI 0.40-0.88)
- Successful (complete or partial) response higher with voriconazole (52.8% vs 31.6%)
- Fewer severe drug-related adverse events with voriconazole; transient visual disturbance in 44.8%
IDSA Clinical Practice Guideline for Candidiasis (2016)
- For Candida osteomyelitis, recommended fluconazole 400mg (6mg/kg) daily, or an echinocandin/lipid amphotericin B for 2 weeks followed by fluconazole step-down
- Total duration 6-12 months for osteomyelitis (longer than soft-tissue candidiasis)
- Echinocandin (micafungin, caspofungin, anidulafungin) preferred for azole-resistant species or critically ill patients
- Surgical debridement recommended for extensive disease, hardware involvement or neurological compromise