Skier's Thumb | UCL Injury | Stener Lesion | Pinch Grip Stability
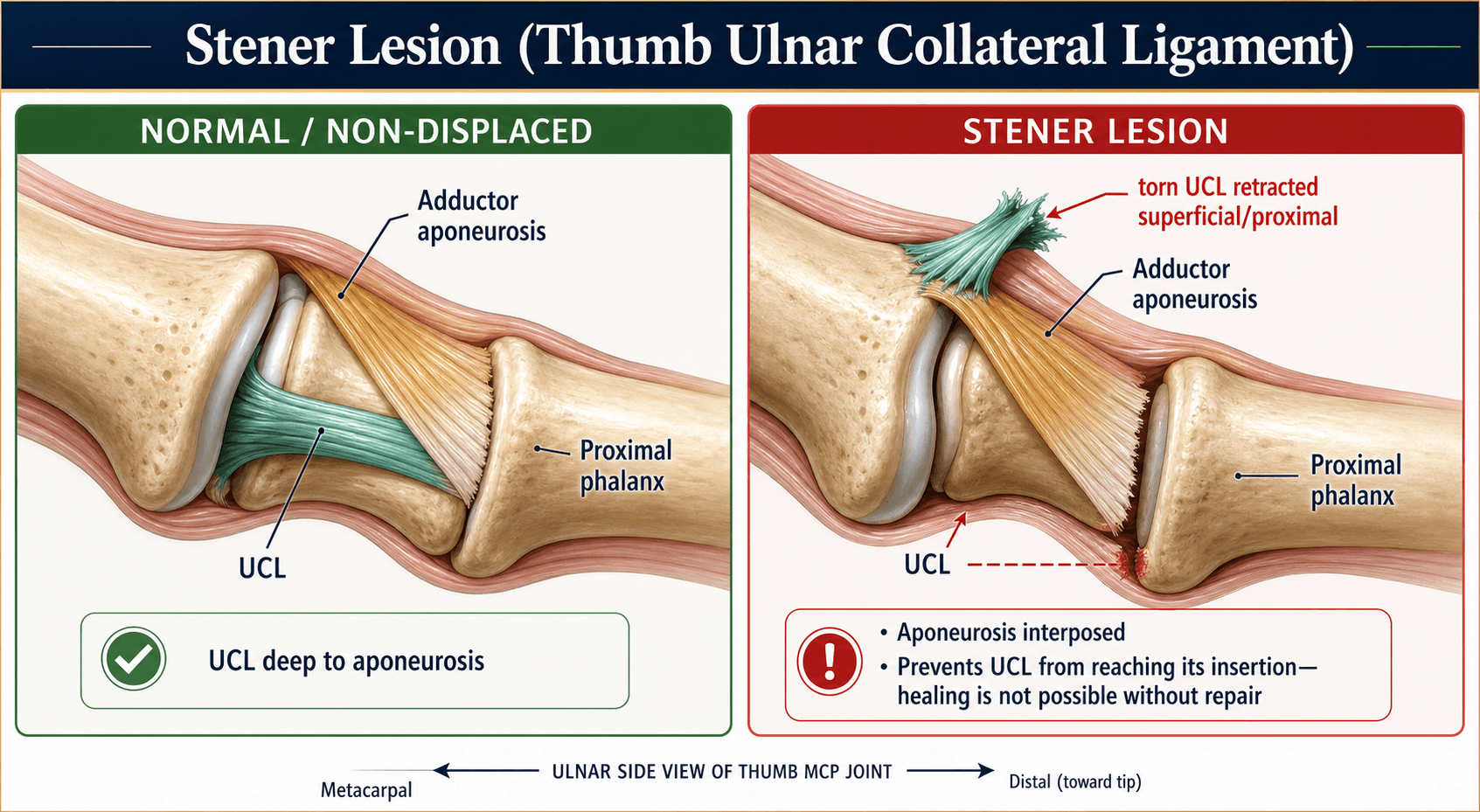
- Stener lesion: UCL stump flips superficial to adductor aponeurosis - aponeurosis blocks healing - MANDATORY surgery
- Test in 30° flexion to isolate proper collateral ligament (main stabiliser). Extension tests accessory UCL + volar plate
- Instability criteria: greater than 30° laxity OR greater than 15° difference to normal side OR no firm endpoint
- X-ray FIRST before stress testing - may have avulsion fracture that stress could displace
- Chronic cases (greater than 6 weeks): Primary repair not possible - requires tendon graft reconstruction or MCP fusion
- “Gamekeeper's = chronic (Scottish rabbit neck-wringing), Skier's = acute (ski pole strap)
- “Palpable mass proximal to MCP = Stener lesion clinically
- “Complete tear conservative treatment failure rate is high because most have Stener lesion
- “Protect radial sensory nerve during surgical repair - runs in surgical field
Gamekeeper's Thumb
Absolute surgical indication. Interposition of Adductor Pollicis aponeurosis prevents healing. Clinically presents as a palpable mass proximal to MCP joint.
Never stress test before X-ray. Stressing a non-displaced fracture can displace it. Always rule out bony avulsion first.
Test in 30° flexion to isolate the proper collateral ligament (PCL). Extension testing assesses the accessory UCL and volar plate.
Always test the normal side first! Laxity varies. A 'soft end point' is more specific for a tear than the absolute degree of angulation. Test in 30° flexion to isolate the Proper UCL (the critical one).
Clinical Context: If fracture is present on X-ray, do NOT stress test vigorously.
Overview
UCL Injury Overview
- Gamekeeper's thumb: Chronic UCL injury (attritional)
- Skier's thumb: Acute UCL injury (traumatic)
- Both involve ulnar collateral ligament of thumb MCP joint
- Common sports injury (skiing, rugby, AFL)
- Fall on outstretched thumb with forced abduction
- Ski pole strap mechanism classically described
- Skier's Thumb (Acute)
- Single traumatic event
- Gamekeeper's Thumb (Chronic)
- Repetitive stress
- Skier's Thumb (Acute)
- Acute pain, swelling
- Gamekeeper's Thumb (Chronic)
- Gradual weakness, instability
- Skier's Thumb (Acute)
- Repair if Stener lesion
- Gamekeeper's Thumb (Chronic)
- Reconstruction or fusion
Anatomy
UCL Anatomy
- Proper collateral ligament (PCL): Tight in flexion
- Accessory collateral ligament (ACL): Tight in extension
- Adductor pollicis aponeurosis lies superficial to UCL
- In complete tears, UCL can flip outside the aponeurosis
- This is the Stener lesion
- Position
- Dorsal
- Testing Position
- 30° flexion
- Position
- Volar
- Testing Position
- Full extension
- Position
- Superficial to both
- Testing Position
- N/A - covers UCL
Pathophysiology
- Forced radial deviation (abduction) and hyperextension of the thumb metacarpophalangeal (MCP) joint loads the UCL beyond its tensile limit.
- The ligament fails most often at its distal (proximal phalanx) insertion, either as a midsubstance/avulsion tear of soft tissue or as a bony avulsion of the ulnar base of the proximal phalanx.
- Classic mechanisms: ski-pole strap forcing the thumb sideways (acute, "skier's thumb"); repetitive attritional valgus loading (chronic, "gamekeeper's thumb").
- Proper collateral ligament (PCL): dorsal, taut in flexion - the principal restraint to valgus stress at the MCP joint.
- Accessory collateral ligament (ACL): volar, taut in extension, blends with the volar plate.
- The adductor pollicis aponeurosis normally lies superficial to the distal UCL.
- When the UCL avulses distally, the retracted free stump can flip and come to lie superficial to the aponeurosis, while its bony footprint stays deep to it.
- The interposed aponeurosis physically separates ligament from bone ("interposition"), so the torn UCL cannot heal in continuity with immobilisation - hence operative retrieval and repair are required.
- Untreated complete tears progress to chronic instability, weak key pinch, and eventual MCP osteoarthritis.
Classification
UCL Injury Grading
- Microscopic tears, ligament intact
- Less than 15° laxity, firm endpoint
- Treatment: Splint 2-3 weeks
- Partial disruption of ligament fibres
- 15-30° laxity, still has endpoint
- Treatment: Thumb spica 4-6 weeks
- Complete rupture of UCL
- Greater than 30° laxity or greater than 15° difference to normal side
- No firm endpoint
- Treatment: Usually surgical (Stener lesion likely)
- Laxity
- Less than 15°
- Endpoint
- Firm
- Treatment
- Splint 2-3 weeks
- Laxity
- 15-30°
- Endpoint
- Present
- Treatment
- Cast 4-6 weeks
- Laxity
- Greater than 30° or 15° difference
- Endpoint
- Absent
- Treatment
- Surgery
Clinical Assessment
History and Examination
- Mechanism (fall on abducted thumb, ski pole, ball)
- Time since injury
- Weakness of pinch grip
- Previous injuries
- Swelling over ulnar MCP
- Bruising
- Palpable mass (Stener lesion)
- Always test normal side first
- Test in 30° flexion (proper UCL)
- Test in extension (accessory UCL)
- Assess endpoint quality (soft vs firm)
- Interpretation
- Grade I (Strain)
- Treatment
- Splint
- Interpretation
- Grade II (Partial)
- Treatment
- Cast 4-6 weeks
- Interpretation
- Grade III (Complete)
- Treatment
- Consider surgery
Investigations
Imaging Assessment
- AP, lateral, oblique of thumb
- Look for avulsion fracture at proximal phalanx base
- Assess for subluxation or dislocation
- ALWAYS before stress testing
- Valgus stress views
- Compare to normal side
- Can quantify degree of laxity
- Confirm Stener lesion
- Assess ligament integrity
- MRI sensitivity greater than 90% for Stener
- When to Use
- All cases (first)
- Key Finding
- Avulsion fracture
- When to Use
- Quantify laxity
- Key Finding
- Degree of opening
- When to Use
- Suspected Stener
- Key Finding
- Ligament position
- When to Use
- Cost-effective alternative
- Key Finding
- Dynamic assessment
Radial Collateral Ligament (RCL) Injury - The Contrast Diagnosis
The differential table and the figure-of-eight reconstruction evidence both name radial collateral ligament (RCL) injury, and the Classification tab reminds you to "check RCL", but the topic never explains it. It is the examiner's favourite contrast to gamekeeper's thumb.
How common. RCL injuries are considerably less common than UCL injuries - most series report the ulnar side is injured several times more often, so the RCL accounts for only a minority of thumb MCP collateral injuries.
Mechanism and testing. The RCL fails with forced adduction (ulnar/varus deviation) of the thumb MCP joint - the mirror image of the abduction load that tears the UCL. It is assessed with varus (radial-deviation) stress in full extension and in 30° flexion, compared with the normal side; the same laxity thresholds and endpoint-quality principles used for the UCL apply.
The key anatomical contrast (why there is usually no "Stener" on the radial side). The adductor pollicis aponeurosis lies on the ulnar side, which is why a torn UCL can flip superficial to it and become trapped. On the radial side there is no equivalent broad aponeurosis reliably interposing, so a fixed Stener-type interposition is uncommon; a "reverse Stener" is described but is the exception, not the rule. Displacement blocking healing is therefore less characteristic of RCL tears, though complete tears still produce instability.
Deformity pattern - a clinical discriminator. Chronic RCL insufficiency produces volar and ulnar subluxation of the proximal phalanx with a dorsoradial prominence of the metacarpal head, and a supination/rotational deformity - a pattern distinct from the ulnar-sided instability of a UCL injury.
Management mirrors UCL principles: partial or stable injuries are immobilised; complete, displaced, or grossly unstable tears are repaired; chronic irreparable injuries are reconstructed (the Baek et al. figure-of-eight series on this page included 9 RCL reconstructions alongside 7 UCL) or treated by MCP arthrodesis if the joint is arthritic.
If asked "what if the injury were on the other side?", say: RCL injury is much rarer, tested with varus (radial-deviation) stress, and rarely forms a true Stener lesion because the adductor aponeurosis is an ulnar-sided structure. The tell-tale is a chronic volar-ulnar subluxation with dorsoradial metacarpal-head prominence and rotational deformity, and management follows the same repair-versus-reconstruct-versus-fuse ladder.
Differential Diagnosis
A swollen, painful thumb MCP joint after a fall has several mimics. The key is to distinguish UCL injury from radial-sided, bony, and joint pathology, because each changes management.
- Distinguishing Features
- Ulnar-sided tenderness, valgus laxity, weak key pinch
- Key Discriminator
- Laxity greater on ulnar stress in 30° flexion
- Distinguishing Features
- Radial-sided tenderness, varus laxity, ulnar deviation deformity
- Key Discriminator
- Instability on varus (radial) stress
- Distinguishing Features
- Bony fragment on radiograph at ulnar base
- Key Discriminator
- Visible fracture - X-ray before stress
- Distinguishing Features
- Hyperextension deformity, dorsal subluxation
- Key Discriminator
- Loss of joint congruity on lateral X-ray
- Distinguishing Features
- Pain at thumb base (CMC), not MCP
- Key Discriminator
- Tenderness and fracture at thumb base
- Distinguishing Features
- Chronic basal thumb pain, grind test positive
- Key Discriminator
- Pain at CMC not MCP; degenerative X-ray
Management Algorithm
Surgical Management
- Stener Lesion (Palpable lump + Instability).
- Complete rupture with lack of firm endpoint (greater than 30° laxity).
- Displaced avulsion fracture.
- Chronic instability.
- Approach: Dorsoulnar incision (S-shaped).
- Identify: Superficial Radial Nerve branches (Risk!).
- Stener: Find the stump superficial to adductor, incise adductor hood to reduce it back to bone.
- Repair: Mitek Anchor into base of proximal phalanx.
- Chronic: Tendon graft reconstruction (Palmaris Longus) or MCP Fusion (if arthritic).
Suture-Tape (Internal Brace) Augmentation
The Controversies section flags suture-tape augmentation as an increasingly used adjunct; this is what it means and where it fits.
Concept. A strong non-absorbable suture tape is anchored with knotless anchors spanning the repair - typically from the metacarpal head/neck to the ulnar base of the proximal phalanx - so that it lies alongside the reattached UCL. It acts as a load-sharing "internal brace" or ligament seat-belt that augments the primary anchor repair; it does not replace the native ligament, which still heals to its footprint.
Rationale. The tape carries part of the valgus load during healing, reducing repair-site gapping under early stress. The intended benefit is earlier protected mobilisation and faster return to sport or work than a repair left to heal in a cast, which matters for high-demand athletes.
Evidence status (be honest in the viva). Cadaveric biomechanical work suggests augmented constructs tolerate higher load with less gapping than suture-anchor repair alone, and early clinical case series report reliable stability with accelerated rehabilitation. However, there is no high-quality randomised comparison against conventional anchor repair, and patient-reported superiority is unproven - exactly why the topic lists it as an area of uncertainty.
Cautions.
- The tape must not be over-tensioned: an overconstrained MCP joint loses flexion and can stiffen.
- It adds implant cost and a second set of anchors.
- It is an adjunct, not a shortcut - a Stener lesion must still be reduced by releasing and repairing the adductor aponeurosis; augmentation over an unreduced stump does not restore anatomy.
Frame suture-tape augmentation as a load-sharing adjunct to primary UCL repair that may permit earlier motion, while stating plainly that it is biomechanically supported but not yet proven superior to standard suture-anchor repair on patient-reported outcomes. It never substitutes for reducing a Stener lesion.
US vs MRI for Stener Lesion - Meta-analysis
- Systematic review and meta-analysis: 9 ultrasound studies (315 thumbs) and 6 MRI studies (107 thumbs)
- Pooled ultrasound sensitivity 95%, specificity 94% for Stener lesion
- Pooled MRI sensitivity 93%, specificity 98% for Stener lesion
- All included studies were high risk of bias - imaging supports, never replaces, examination
Original Stener Lesion Description
- Classic anatomical description of UCL displacement
- Torn UCL stump flips superficial to adductor aponeurosis
- Aponeurosis blocks ligament-to-bone contact (interposition)
- Healing impossible without surgical retrieval of ligament
Chronic UCL Reconstruction - Free Tendon Graft
- 16 figure-of-eight collateral ligament reconstructions with palmaris longus autograft (7 UCL, 9 RCL), mean 12 months post-injury
- Radial/ulnar deviation laxity improved from 19.3° to 5.3°
- Key pinch improved from 49% to 82% and grip strength from 81% to 87% of contralateral
- Glickel functional grade: 9 excellent, 7 good (all 16 good or excellent)
Ultrasound Criteria for Displaced UCL Tear
- 26 surgically proven UCL tears (17 displaced full-thickness, 7 non-displaced, 2 partial)
- Two ultrasound criteria present in all displaced tears: non-visualisation of the UCL and a heterogeneous mass-like area proximal to the first MCP joint
- Applying these criteria gave 100% sensitivity, specificity and accuracy in differentiating displaced from non-displaced tears
- Displaced (Stener) tears most commonly lay proximal to the adductor aponeurosis
Ultrasound Accuracy for UCL Injury - Meta-analysis
- Systematic review and meta-analysis of 17 studies, 593 UCL injuries
- Ultrasound for Stener lesion: pooled sensitivity 0.96 (95% CI 0.89-0.99), specificity 0.90 (95% CI 0.81-0.94)
- Area under the curve 0.98 for Stener diagnosis - excellent accuracy
- Accuracy lower for non-displaced complete ruptures (sensitivity 0.81)
Collateral Ligament Injuries - Review & Diagnostic Criteria
- Complete tear diagnosed when the proximal phalanx angulates 30° to 35° on the metacarpal head in extension or 30° of flexion
- Lack of a firm endpoint or angulation greater than 15° versus the contralateral thumb also indicates complete tear
- Partial injuries managed nonsurgically; complete tears usually managed surgically
- Chronic injury options: repair, free tendon graft reconstruction, or MCP arthrodesis
Complications
Potential Complications
- Most important complication
- Leads to chronic instability
- Weak pinch grip, pain
- Requires reconstruction or fusion
- Radial sensory nerve injury (neuroma)
- Stiffness
- Re-rupture
- Anchor failure
- Cause
- Missed Stener lesion
- Treatment
- Reconstruction or fusion
- Cause
- Surgical dissection
- Treatment
- Desensitisation, excision
- Cause
- Prolonged immobilisation
- Treatment
- Hand therapy
- Cause
- Chronic instability
- Treatment
- Fusion if severe
Postoperative Care
Rehabilitation Protocol
- Thumb spica cast or splint
- Include IP joint initially
- Elevate to reduce swelling
- Active finger ROM
- Transition to removable splint
- Active ROM exercises
- Hand therapy referral
- Avoid stress on repair
- Progressive pinch strengthening
- Functional activities
- Return to light work
- Activity
- Thumb spica, elevation
- Goal
- Protect repair
- Activity
- Active ROM, removable splint
- Goal
- Restore motion
- Activity
- Strengthening
- Goal
- Functional recovery
- Activity
- Return to sport/work
- Goal
- Full activity
Outcomes
Functional Outcomes
- Greater than 90% good/excellent results
- Stable joint, strong pinch
- Return to full function expected
- Good outcomes if no Stener lesion
- Risk of late instability if undertreated
- 80-85% satisfactory results
- Less predictable than acute repair
- May have some residual laxity
- Good/Excellent
- Greater than 90%
- Main Concern
- Stiffness
- Good/Excellent
- 85-90%
- Main Concern
- Ensure no Stener
- Good/Excellent
- 80-85%
- Main Concern
- Residual laxity
- Good/Excellent
- Pain relief excellent
- Main Concern
- Loss of MCP motion
Guidelines, Registries & Global Practice
Global Epidemiology & Burden
- Thumb UCL injury is among the most common ligamentous hand injuries, accounting for an estimated 50-86% of MCP-joint ligament injuries of the thumb.
- Classic at-risk populations: alpine/skiing (ski-pole strap mechanism) and ball/contact sports (rugby, football codes, basketball, netball, handball).
- Bony avulsion of the ulnar base of the proximal phalanx accompanies roughly 20-30% of cases.
- A Stener lesion is present in the majority of complete ruptures (most series report up to ~80%).
Side-by-Side Guideline & Consensus Comparison
- Position on Stener / complete tear
- Complete tears usually operative; partial tears nonoperative
- Imaging emphasis
- Stress testing primary; imaging adjunct
- Position on Stener / complete tear
- Surgical repair for Stener / unstable complete tear
- Imaging emphasis
- Ultrasound first-line, MRI if equivocal
- Position on Stener / complete tear
- Anatomical repair / suture-anchor to footprint; ORIF for large displaced avulsion
- Imaging emphasis
- Radiograph mandatory before stress
- Position on Stener / complete tear
- Early surgery for complete instability; reconstruction for chronic
- Imaging emphasis
- Dynamic US increasingly standard
There are no randomised trials comparing surgery with immobilisation for complete tears; recommendations rest on anatomical reasoning (the Stener interposition) and consistent case-series outcomes. There is no dedicated implant registry for thumb UCL surgery (unlike arthroplasty registries such as NJR, AJRR or AOANJRR).
Controversies & Areas of Uncertainty
- Surgery vs immobilisation for complete tears without a confirmed Stener lesion. No RCT exists. Many surgeons trial cast immobilisation when imaging shows the stump is reduced (no Stener), reserving repair for failure; others repair all complete tears in high-demand patients to avoid chronic instability.
- Threshold laxity for "complete tear." Commonly quoted figures (greater than 30°, or 30-35° absolute, or greater than 15° side-to-side difference) vary between sources; endpoint quality (soft vs firm) is arguably more reliable than the absolute angle and should be assessed against the normal side.
- First-line imaging - ultrasound vs MRI. Meta-analytic data show ultrasound is highly accurate for Stener lesions and is increasingly the first-line test, but it is operator-dependent; MRI remains the fallback for equivocal scans.
- Management of small bony avulsions. Fragments too small to fix reliably (often quoted as under 3 mm or comminuted) are usually excised with suture-anchor repair of the ligament rather than ORIF; the size threshold for fixation is not standardised.
- Augmentation / internal brace. Suture-tape augmentation to allow earlier mobilisation is increasingly used, but high-level comparative evidence against conventional anchor repair is limited.
MCQ Practice Points
Q: What is the difference between gamekeeper's thumb and skier's thumb?
A: Gamekeeper's thumb: Chronic attritional injury to the ulnar collateral ligament (UCL) of thumb MCP joint, originally described in Scottish gamekeepers who killed rabbits by neck wringing. Skier's thumb: Acute UCL injury from forced thumb abduction/hyperextension (e.g., ski pole strap, ball handling). Both involve the UCL proper and accessory UCL. The clinical presentation and treatment principles are similar; The distinction is historical/mechanism-based.
Q: What is a Stener lesion and why is it clinically important?
A: Stener lesion: Displaced UCL rupture where the torn ligament end lies superficial to (on top of) the adductor pollicis aponeurosis, preventing healing to bone. Occurs in complete UCL ruptures - the aponeurosis interposes between the ligament and its insertion. Clinical importance: Stener lesions cannot heal with conservative treatment as the ligament cannot reattach to bone. Requires surgical repair. Present in approximately 80% of complete UCL ruptures. Diagnosed by palpable mass at MCP ulnar aspect or MRI.
Q: How do you clinically assess UCL integrity and what constitutes instability?
A: Stress testing: Apply valgus stress to thumb MCP in 30° flexion (tests UCL proper) and full extension (tests accessory UCL). Compare to uninjured side. Instability criteria: Greater than 30° of radial deviation or greater than 15° difference from uninjured side indicates complete rupture. Endpoint: Absent firm endpoint suggests complete tear. Test with local anesthesia if pain limits examination. Caution: Excessive stress may convert partial to complete tear or displace Stener lesion.
Q: What imaging is recommended for suspected UCL injury?
A: Radiographs: AP, lateral, oblique views. Look for: Avulsion fracture at proximal phalanx base (may be rotated/displaced); Joint subluxation. Stress radiographs: Valgus stress views comparing both thumbs (under anesthesia if needed). MRI: Gold standard for soft tissue assessment; Identifies Stener lesion, ligament tears, associated injuries. Ultrasound: Operator-dependent but can assess ligament continuity and Stener lesion dynamically. Imaging helps determine surgical vs. conservative treatment.
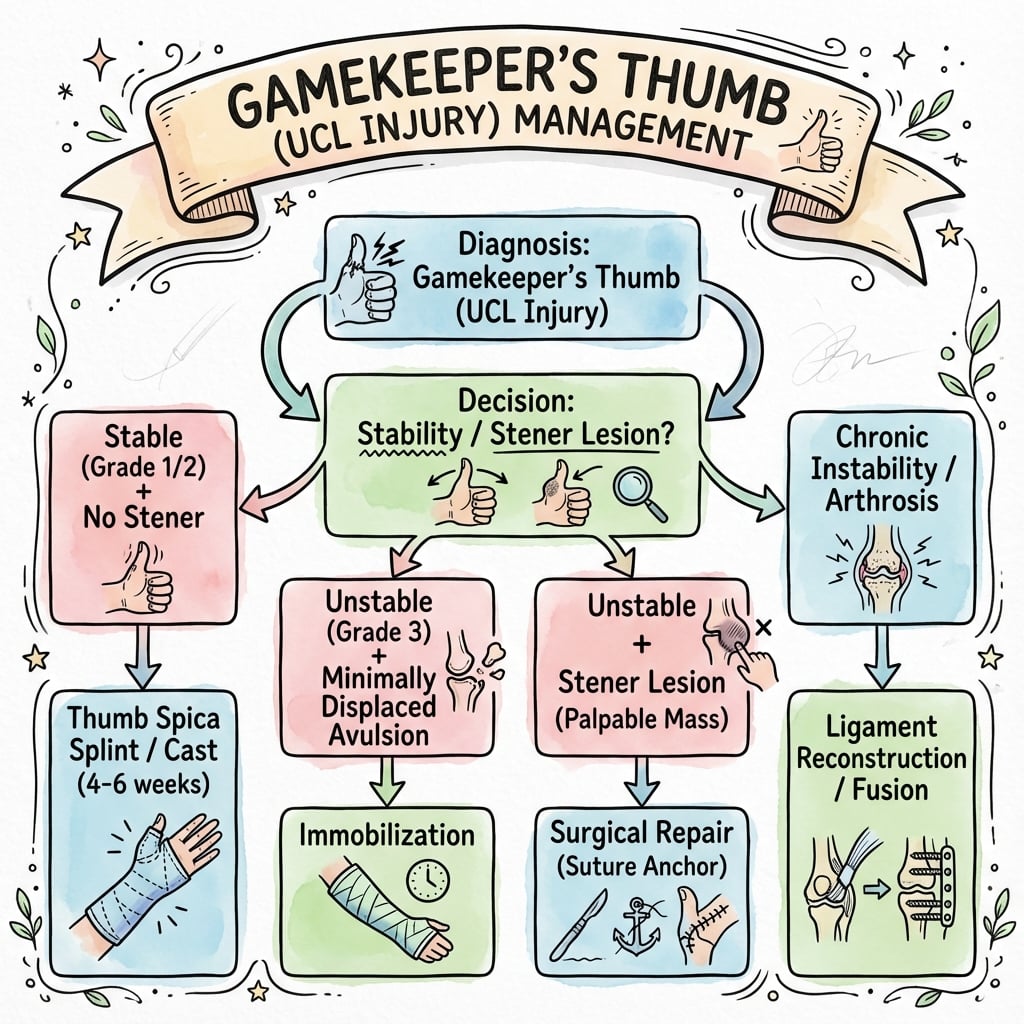
Q: What is the treatment algorithm for UCL injuries?
A: Partial tears / Stable (less than 30° deviation): Thumb spica cast/splint 4-6 weeks, then progressive ROM. Complete tears without Stener lesion: May trial immobilization but high failure rate; Often proceed to repair. Complete tears with Stener lesion: Surgical repair required - direct ligament repair with suture anchors; Avulsion fractures fixed if large enough. Chronic injuries: Ligament reconstruction (palmaris longus tendon graft) if direct repair not possible. Post-op: Immobilization 4-6 weeks, then therapy.
At a Glance
Gamekeeper's thumb refers to chronic UCL injury while Skier's thumb is the acute variant, both involving injury to the ulnar collateral ligament of the thumb MCP joint from forced abduction. The critical pathology is the Stener lesion where the torn UCL flips superficial to the adductor aponeurosis, preventing healing and mandating surgical repair. Stress testing should be performed in 30° flexion to isolate the proper collateral ligament, with greater than 30° laxity or greater than 15° asymmetry indicating complete tear. Partial tears are treated with thumb spica immobilisation for 4-6 weeks, while complete tears with Stener lesion require surgical anchor repair to restore pinch grip strength and prevent chronic instability with CMC arthritis.
PAVUCL Components
Hook:Proper = Primary = test in Flexion (Proper Flexes)
SAILStener Lesion Criteria
Hook:The ligament SAILs outside the aponeurosis and can't get back in
S-P-CUCL Injury Grading
Hook:S-P-C: Severity Progressively Climbs
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 30-year-old skier presents with a painful thumb after falling on his ski pole. X-ray is normal. On examination, he has tenderness over the ulnar aspect of the MCPJ and 45 degrees of valgus laxity in flexion (compared to 15 on normal side). There is no end point. How do you manage this?”
“A 25-year-old rugby player presents 3 days after injuring his thumb during a tackle. X-rays show a small (2mm) minimally displaced bony fragment at the ulnar base of the proximal phalanx. Clinical examination shows 25 degrees of laxity in 30 degrees flexion (15 degrees on normal side) with a soft endpoint. He asks whether he needs surgery. How would you counsel him?”
“A 45-year-old manual laborer presents with chronic thumb MCP instability 2 years after an untreated UCL injury. He has weakness in pinch grip affecting his work. X-rays show moderate MCP joint arthritis with joint space narrowing and osteophytes. Clinical exam shows 40 degrees of valgus laxity with no endpoint. He is frustrated his initial injury was missed and wants definitive treatment. What are your options and what would you recommend?”
Anatomy
- Proper UCL: Flexion stabiliser
- Accessory UCL: Extension stabiliser
- Stener: Stump superficial to adductor
Testing Criteria
- Greater than 30 degrees laxity
- Greater than 15 degrees difference side-to-side
- No end point
Management Rules
- Partial: Cast 6w
- Complete/Stener: Surgery
- Fx non-displaced: Cast
- Fx displaced: Surgery
Evidence Base
Key Studies
- Stener (1962): Described interposition of adductor aponeurosis
- Established the anatomical basis for surgical treatment
- Miller (2008): MRI sensitivity greater than 90% for Stener lesion
- Clinical exam alone may miss Stener lesion
- Key Finding
- Aponeurosis blocks healing
- Clinical Impact
- Surgery for Stener lesion
- Key Finding
- MRI greater than 90% for Stener
- Clinical Impact
- Get imaging if complete tear
- Key Finding
- Reconstruction techniques
- Clinical Impact
- Options for chronic cases
References
- Stener B. Displacement of the ruptured ulnar collateral ligament of the metacarpophalangeal joint of the thumb. J Bone Joint Surg Br. 1962;44-B:869-879. (Landmark anatomical description - predates PubMed indexing.)
- Tang P. Collateral ligament injuries of the thumb metacarpophalangeal joint. J Am Acad Orthop Surg. 2011;19(5):287-296. PMID 21536628. doi:10.5435/00124635-201105000-00006
- Qamhawi Z, Shah K, Kiernan G, Furniss D, Teh J, Azzopardi C. Diagnostic accuracy of ultrasound and MRI in detecting Stener lesions of the thumb: systematic review and meta-analysis. J Hand Surg Eur Vol. 2021;46(9):946-953. PMID 33596684. doi:10.1177/1753193421993015
- Raheman FJ, Rojoa DM, Dhingra M, Siddiqui S, Macdonald CR. The role of ultrasonography in the assessment of UCL injury of the thumb - a diagnostic test accuracy meta-analysis. J Plast Surg Hand Surg. 2020;55(2):83-95. PMID 33156740. doi:10.1080/2000656X.2020.1838295
- Melville D, Jacobson JA, Haase S, Brandon C, Brigido MK, Fessell D. Ultrasound of displaced ulnar collateral ligament tears of the thumb: the Stener lesion revisited. Skeletal Radiol. 2012;42(5):667-673. PMID 23001117. doi:10.1007/s00256-012-1519-x
- Baek JH, Lee JH, Ku KH. Novel figure-of-eight reconstruction with free tendon graft for unrepairable collateral ligament of the thumb MCP joint. Hand Surg Rehabil. 2024;43(3):101696. PMID 38657737. doi:10.1016/j.hansur.2024.101696
- Başar H, Başar B, Kaplan T, Erol B, Tetik C. Comparison of results after surgical repair of acute and chronic ulnar collateral ligament injury of the thumb. Chir Main. 2014;33(6):384-389. PMID 25458468. doi:10.1016/j.main.2014.10.003