Gartland Classification of Supracondylar Humeral Fractures
The Gartland classification
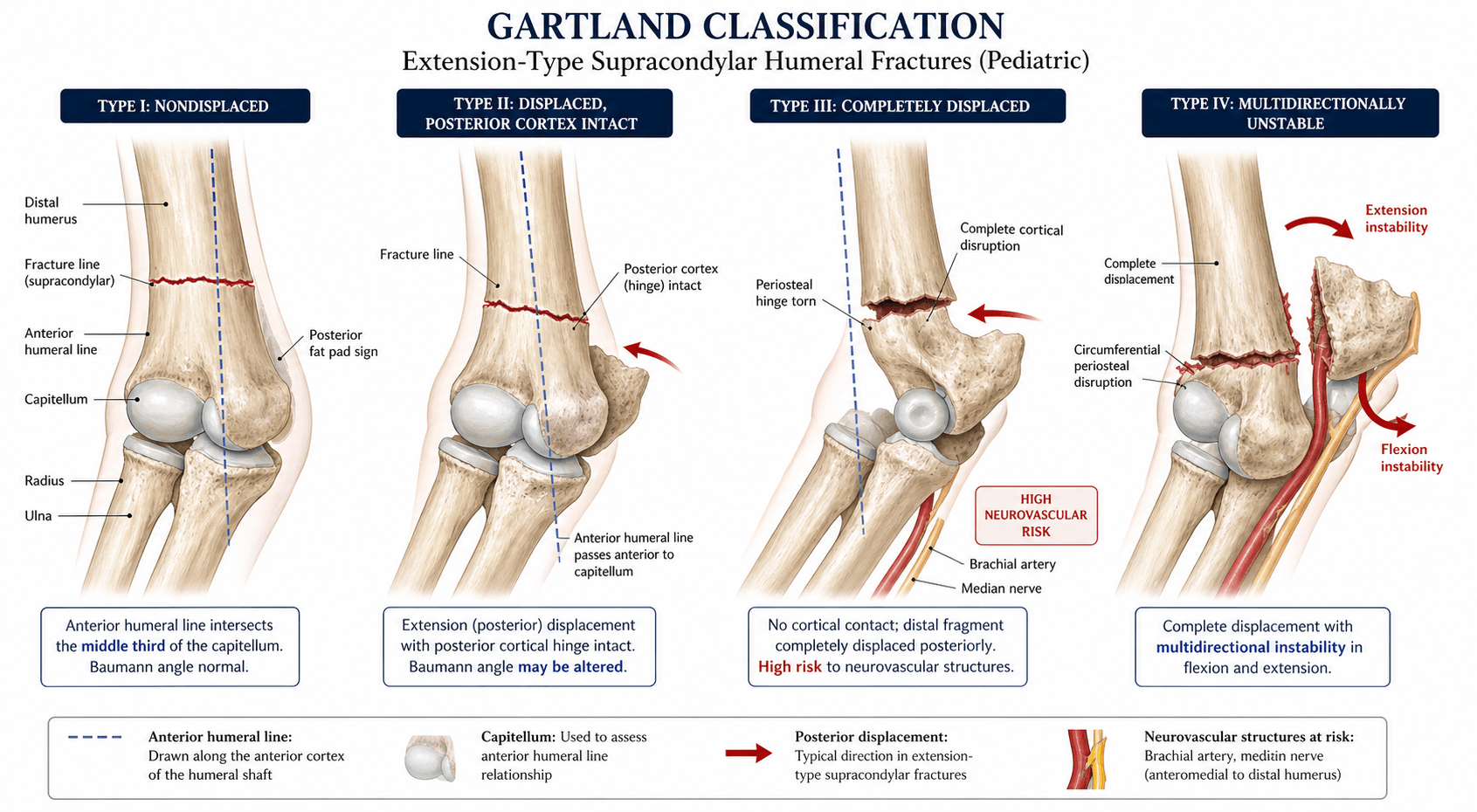
The Gartland system classifies extension-type supracondylar humerus fractures in children (the overwhelming majority — 95 to 98%) by degree of posterior displacement and cortical continuity. The original description had three types; a fourth (multidirectional instability) was added by Leitch.

- Displacement
- Undisplaced
- Posterior cortex
- Intact
- Radiograph
- Anterior humeral line normal — bisects the capitellum
- Management
- Above-elbow backslab/cast, 3–4 weeks
- Displacement
- Angulated, intact posterior hinge
- Posterior cortex
- Intact (hinged)
- Radiograph
- Anterior humeral line passes anterior to the capitellum
- Management
- Reduce if angulation/Baumann angle unacceptable; pin if reduced
- Displacement
- Complete displacement, no cortical contact
- Posterior cortex
- No contact
- Radiograph
- Anterior humeral line misses the capitellum
- Management
- Closed reduction + percutaneous pinning (CRPP)
- Displacement
- Multidirectionally unstable
- Posterior cortex
- No contact; unstable in flexion AND extension
- Radiograph
- Unstable on fluoroscopy in both planes
- Management
- CRPP; harder to hold reduced (may need open reduction)
UHDMThe four Gartland types
Hook:Types I and II have cortical continuity; Types III and IV have none and need operative fixation.
The anterior humeral line is the key radiographic sign on the lateral view: drawn down the anterior cortex of the humerus, it should intersect the middle third of the capitellar ossification centre. If it passes anterior to the capitellum, the distal fragment is posteriorly angulated or displaced (Gartland II or III). On the AP view, the Baumann angle (~72–75°, compared with the contralateral side) detects rotational/coronal malalignment.

"Reduce if angulation is unacceptable" begs the question of which type II. The Wilkins modification subdivides Gartland II by whether there is rotational/translational malalignment in addition to the sagittal angulation:
- Type IIA — angulation only: posterior tilt (anterior humeral line off the capitellum) without rotational malalignment, the posterior cortex acting as an intact hinge. Often reducible and stable — minimally angulated IIA can be treated closed (cast), though many surgeons now reduce and pin for reliability.
- Type IIB — angulation PLUS rotation/translation: the added rotational or coronal malalignment (loss of the Baumann angle, a malrotated fragment) makes it less stable and prone to varus malunion — it needs closed reduction and percutaneous pinning, not a cast. This is exactly the distinction the type-II management row turns on: IIA can sometimes be cast; IIB should be reduced and pinned. (Rotational malalignment, not the degree of tilt alone, is the unstable feature.)
Neurovascular assessment
A neurovascular examination before and after manipulation is mandatory (and medicolegally essential). The anterior interosseous nerve (AIN), a motor branch of the median nerve, is the most commonly injured — test flexor pollicis longus and the index FDP ("OK sign"). The brachial artery is the vessel at greatest risk. Most nerve injuries are neuropraxias that recover over 3–6 months.
ARUBNeurovascular structures to check
Hook:Document all four before AND after reduction — a medicolegal must-do.
Management & pinning technique
- 1Examine and gradeDocument the AIN/radial/ulnar nerves and the brachial pulse; grade with Gartland (anterior humeral line, cortical contact). Type I → cast; type II → reduce if angulated/Baumann altered; type III/IV → operative.
- 2Closed reduction + percutaneous pinning for III/IVUrgent CRPP under GA; restore length, alignment and rotation. Type IV has no periosteal hinge so is harder to hold — be ready to convert to open reduction (anterior/Henry approach) if closed reduction fails.
- 3Pin laterallyTwo or three DIVERGENT lateral-entry pins, well-spaced at the fracture site. Avoid a routine medial pin — the ulnar nerve is at risk in the cubital tunnel, especially in a swollen, hyperflexed elbow.
- 4Re-assess the vesselPink pulseless hand (well-perfused, no pulse) → observe (the pulse usually returns). White, cold, pulseless hand → reduce, pin, and EXPLORE the brachial artery (anterior approach). Angiography is not indicated — it only delays reduction.
- Treatment
- Above-elbow backslab/cast at ~90° flexion
- Pinning
- None
- Key consideration
- Review at 1 week with radiographs; ensure no displacement
- Treatment
- Closed reduction if angulation unacceptable; pin if reduced
- Pinning
- If reduced — two lateral-entry pins
- Key consideration
- Baumann-angle loss or rotational malalignment tips toward reduction
- Treatment
- Urgent CRPP
- Pinning
- Two or three divergent lateral-entry pins
- Key consideration
- Admit for overnight NV observation; document NV before and after
- Treatment
- CRPP; convert to open if closed reduction fails
- Pinning
- Two or three divergent lateral-entry pins
- Key consideration
- No periosteal hinge to aid reduction

TDLLateral pin configuration
Hook:Never cross the midline with a pin — the ulnar nerve lives on the medial side.
The pulseless hand. If the hand is well-perfused (pink, warm, good capillary refill) but the radial pulse is absent, observe after reduction — the pulse usually returns within 24–48 hours as swelling subsides. If the hand is white, cold and pulseless, this is a surgical emergency: reduce, pin, and explore the brachial artery (anterior approach). Angiography is not indicated for the pulseless limb — it only delays the reduction that usually fixes the vascular problem. Maintain a high index of suspicion for compartment syndrome (worsening pain on passive finger extension), especially with a co-existing forearm fracture or a median-nerve injury masking symptoms.
Pearls, pitfalls & variations
- Flexion-type fractures (2–5%) are far less common, from a fall on a flexed elbow, with the distal fragment displaced anteriorly — apply Gartland (designed for extension) with caution.
- Medial comminution is a subtle finding that, if treated non-operatively, leads to varus malunion — look for it.
- Cubitus varus (gunstock deformity) is the commonest late complication — from malrotation/medial-column collapse — and may need a corrective supracondylar osteotomy.
- Type IV is easily missed — it appears to reduce in both flexion and extension on fluoroscopy; the clue is instability in both planes under anaesthesia.
- Timing: for a closed injury with a well-perfused hand, multiple studies show no outcome difference between operating overnight and the next morning — swelling and compartment risk, not the clock, dictate urgency.
- Compartment syndrome / Volkmann contracture — rare but devastating; suspect with escalating pain, anxiety and worsening swelling.
Gartland was designed for the extension pattern; the uncommon flexion-type (about 2–5%) behaves differently in ways that are high-yield:
- Mechanism: a fall onto the point of a flexed elbow (or a direct posterior blow), rather than the FOOSH of extension injuries.
- Displacement: the distal fragment displaces ANTERIORLY (proximal fragment posterior) — the mirror image of extension.
- Radiograph: the anterior humeral line passes POSTERIOR to the capitellum (the opposite of the extension fracture, where it passes anterior).
- Nerve at risk: the ULNAR nerve is the most commonly injured in flexion-type fractures (contrast the AIN/median in extension-type) — examine and document it specifically.
- Stability/treatment: flexion-type fractures are more often irreducible/unstable and reduced in extension (the reverse of the extension fracture, which is held in flexion), so they carry a higher rate of open reduction; pinning principles (divergent lateral-entry) are otherwise the same.
Viva practice
Exam viva
Practise clinical reasoning and management decisions out loud
“A 6-year-old boy fell off a trampoline onto an outstretched hand and now holds his elbow in flexion with marked swelling. Radiographs show a fully displaced extension-type supracondylar fracture with no cortical contact. How do you classify and manage this?”
“You reduce and pin a Gartland Type III supracondylar fracture. During fluoroscopy you note the fracture is unstable in both flexion and extension. What is the diagnosis and how does it change your management?”
Exam & revision
Everything below condenses the Gartland classification for revision and viva practice.
- I undisplaced (cast); II hinged posterior cortex (reduce/pin if angulated); III displaced (CRPP); IV multidirectional (CRPP).
- Anterior humeral line bisects the capitellum; if it passes anterior → type II/III. Baumann angle ~72–75°.
- AIN is the commonest nerve injured (test FPL + index FDP); brachial artery the vessel at risk.
- Lateral-entry pins (two or three, divergent) — a medial pin risks the ulnar nerve.
- Pink pulseless hand → observe; white pulseless hand → explore the brachial artery; angiography not indicated.
- Cubitus varus is the commonest late complication; type IV is the easily-missed multidirectionally unstable pattern.
Exam cheat sheet
Classification (extension type)
- Type I: undisplaced - anterior humeral line normal, cast 3-4 weeks
- Type II: hinged posterior cortex - reduce if angulated, pin if reduced
- Type III: completely displaced - CRPP with lateral-entry pins
- Type IV: multidirectional instability (Leitch) - CRPP, may need open reduction
Neurovascular assessment
- AIN (median branch): most commonly injured nerve - test FPL and index FDP
- Radial nerve: test wrist and finger extension
- Ulnar nerve: at risk from a medial spike or iatrogenic medial pin
- Brachial artery: palpate pulse, check capillary refill, Doppler if absent
Pinning technique
- Two or three divergent lateral-entry pins - the standard of care
- Avoid routine medial pins - ulnar nerve risk in the cubital tunnel
- Separate the pins at the fracture site for stability
- Pink pulseless hand: observe; white pulseless hand: explore the artery (no angiography)
Key radiographic signs
- Anterior humeral line: should bisect the capitellum on the lateral view
- Baumann angle: ~72-75 degrees on AP - compare with the contralateral side
- Posterior fat pad sign: haemarthrosis - suggests an occult fracture if no line is seen
- Type IV: unstable on fluoroscopy in both flexion and extension
Evidence Base
Management of supracondylar fractures of the humerus in children
- Described the original three-type classification of extension supracondylar fractures in children.
- Separated undisplaced (Type I), hinged with an intact posterior cortex (Type II), and completely displaced (Type III) patterns.
- Recommended operative intervention for completely displaced fractures.
Treatment of multidirectionally unstable supracondylar humeral fractures in children. A modified Gartland type-IV fracture
- Identified 9 of 297 displaced supracondylar fractures as completely unstable - displacing into BOTH flexion and extension on fluoroscopy - and named this the Gartland Type IV (modified) pattern.
- All 9 were treated successfully with a new technique of closed reduction and percutaneous pinning, AVOIDING open reduction (7/9 with lateral-entry pins).
- The complication rate of these unstable fractures was no higher than that of the 288 more stable fractures (no nonunion, malunion, cubitus varus or loss of motion).
According to PubMed: the three-type classification comes from Gartland 1959 (PMID 13675986); the type-IV (multidirectionally unstable) pattern from Leitch et al. 2006 (DOI), whose CRPP technique avoided open reduction; the lateral-vs-crossed pin data from Skaggs et al. 2001 (medial pin → 4-15% ulnar injury, PMID 11379744) and the randomised Kocher et al. 2007 (DOI; no ulnar injury in either group, both effective); and the management review (no angiography for a pulseless limb; medial comminution → varus; compartment-syndrome vigilance) from Omid et al. 2008 (DOI). The anterior-humeral-line and AIN points are standard teaching.