Benign Vascular Tumor | Phleboliths Pathognomonic | MRI Essential
- Hemangioma is BENIGN - NOT angiosarcoma
- Phleboliths pathognomonic - round calcifications with lucent centers
- MRI essential - radiographs underestimate extent significantly
- Venous type most common in skeletal muscle (60%)
- Incomplete excision leads to high recurrence (up to 40%)
- “Infantile hemangiomas: 50% involute by age 5 - observation first
- “Kasabach-Merritt syndrome with kaposiform hemangioendothelioma, NOT hemangioma
- “MRI: hyperintense T2, flow voids, enhancement
- “Distinguish from vascular malformations - different natural history
Hemangioma (Soft Tissue)

Hemangioma is BENIGN. Do not confuse with angiosarcoma or hemangioendothelioma. No metastatic potential.
Pathognomonic finding - round calcifications with lucent centers. Present in 50% of soft tissue hemangiomas on radiographs.
Radiographs significantly underestimate extent. MRI shows hyperintense T2 signal with flow voids and enhancement.
Incomplete surgical excision leads to 40% recurrence. Complete excision difficult due to infiltrative growth.
Anatomy & Pathophysiology
Histologic Subtypes and Characteristics
Soft tissue hemangiomas represent a spectrum of benign vascular proliferations with distinct histologic patterns that correlate with clinical behavior and imaging characteristics.
- Composed of small, capillary-sized vessels
- Prominent endothelial cells with minimal atypia
- Dense cellularity with little intervening stroma
- Most common type in subcutaneous tissue
- Lobular architecture with feeding vessels
- Usually presents in infants and young children
- High proliferative index in infantile variant
- Associated with GLUT-1 positivity in infantile type
- Large, dilated, blood-filled vascular spaces
- Thin-walled vessels lined by flattened endothelium
- More common in deep soft tissue and muscle
- Significant thrombosis and phlebolith formation
- Slow blood flow with stasis phenomena
- Accounts for most intramuscular hemangiomas
- May cause local mass effect and compression
- Lower proliferative rate than capillary type
- Thick-walled veins with smooth muscle
- Most common type within skeletal muscle (60% of intramuscular)
- Often infiltrates between muscle fibers
- Associated with pain due to venous distension
- Phleboliths present in up to 50% of cases
- Calcifications visible on radiographs
- May cause compartment syndrome-like symptoms
- Difficult to completely excise due to infiltrative growth
- Direct arteriovenous communications without capillary bed
- High-flow lesion with prominent arterial feeders
- Pulsatile mass with audible bruit or palpable thrill
- Risk of bleeding with biopsy or surgery
- May cause distal ischemia via steal phenomenon
- Often requires preoperative embolization
- Higher recurrence rate after incomplete excision
- Can enlarge with hormonal changes or trauma
Molecular and Cellular Mechanisms
Endothelial Proliferation Pathways:
- VEGF (vascular endothelial growth factor) upregulation drives angiogenesis
- FGF-2 (fibroblast growth factor) promotes endothelial cell proliferation
- Angiopoietin-TIE2 system regulates vessel maturation
- GLUT-1 expression distinguishes infantile from congenital hemangiomas
- Hypoxia-inducible factor (HIF) activation in proliferating lesions
- Loss of apoptotic signals allows persistent endothelial growth
- Mast cell infiltration contributes to vascular remodeling
- Pericyte recruitment and smooth muscle differentiation in maturing lesions
Natural History Phases (Infantile Type):
Proliferative Phase (0-12 months):
- Rapid endothelial proliferation with high GLUT-1 expression
- Increased mitotic activity and cellular density
- VEGF and FGF-2 levels peak during this period
- Tumor typically doubles in size during first 5 months
- Minimal apoptosis with net accumulation of vessels
- Bright red appearance due to high blood flow
- May cause functional impairment if near critical structures
Plateau Phase (12-18 months):
- Balance between proliferation and apoptosis
- Stable size with decreased growth velocity
- Beginning of endothelial maturation processes
- Color change from bright red to purple
- Decreased GLUT-1 and proliferation markers
- Structural reorganization of vascular channels
- Opportunity for observation before involution
Involutionary Phase (1-7 years):
- Apoptosis exceeds proliferation with net vessel loss
- Replacement of endothelial cells with fibrofatty tissue
- Progressive decrease in lesion size (50% by age 5)
- Color fades to gray or skin tone
- Decreased vascularity on imaging studies
- May leave residual fibrofatty tissue or skin changes
- Complete involution occurs in 50% by age 5, 70% by age 7
Distribution Patterns
- Lower extremity: 50% (quadriceps, gastrocnemius most common)
- Upper extremity: 25% (deltoid, biceps, forearm flexors)
- Trunk: 15% (paraspinal, abdominal wall muscles)
- Head and neck: 10% (masticatory muscles, tongue)
- Infiltrative growth pattern along fascial planes
- May involve multiple muscle groups in complex cases
- Difficult surgical planes due to muscle infiltration
- High recurrence with incomplete excision
- More common in head and neck region in children
- Superficial location allows easier clinical diagnosis
- Better defined margins than intramuscular types
- More amenable to complete surgical excision
- May respond to laser therapy if purely cutaneous
- Associated with overlying skin discoloration
- Lower recurrence rate after excision
- Better cosmetic outcomes with modern techniques
- Knee joint most frequently affected (40% of joint hemangiomas)
- Causes recurrent hemarthrosis and joint swelling
- Synovial hypertrophy with hemosiderin deposition
- Progressive joint damage if untreated
- May mimic pigmented villonodular synovitis
- Requires synovectomy for definitive treatment
- Arthroscopic evaluation and treatment possible
- Risk of arthrofibrosis post-treatment
Classification
Histologic Classification (Enzinger & Weiss)
Capillary Hemangioma:
Microscopic Features:
- Lobules of closely packed capillaries with narrow lumens
- Prominent plump endothelial cells without significant atypia
- Pericytes present surrounding endothelial tubes
- Minimal intervening stroma between vascular channels
- May have focal mitotic activity in proliferating lesions
- Immunohistochemistry: CD31+, CD34+, factor VIII+
- GLUT-1 positive in infantile variant only
- Ki-67 proliferation index elevated in proliferative phase
Clinical Correlates:
- Most common in subcutaneous tissue and dermis
- Bright red color due to high blood flow
- Soft, compressible mass that blanches with pressure
- May demonstrate rapid growth in infants
- Better defined margins than other subtypes
- More amenable to sclerotherapy or laser treatment
- Lower recurrence rate after complete excision
- 50% of infantile types involute by age 5 years
Cavernous Hemangioma:
Microscopic Features:
- Large, thin-walled vascular spaces filled with blood
- Flattened endothelial lining with minimal cellular atypia
- Fibrous septa separating vascular spaces
- Thrombosis and organization within vascular channels
- Dystrophic calcification forming phleboliths
- Variable smooth muscle in vessel walls
- Hemosiderin deposition from prior hemorrhage
- Immunohistochemistry similar to capillary type
Clinical Correlates:
- Deep soft tissue location, especially muscle
- Bluish discoloration of overlying skin if superficial
- Compressible mass that refills slowly after compression
- Phleboliths visible on radiographs (50% of cases)
- May cause pain from thrombosis or venous distension
- Infiltrative borders make complete excision challenging
- Recurrence rate 20-40% after attempted excision
- Does not involute spontaneously in adults
Arteriovenous Hemangioma:
Microscopic Features:
- Thick-walled arteries with muscular media
- Direct arteriovenous communications (shunts)
- Absence of normal capillary bed intermediaries
- Variable caliber vessels with high flow
- Reactive intimal thickening in feeding arteries
- May have aneurysmal dilatation of draining veins
- Cellular proliferation in growing lesions
- Hemosiderin and thrombus less common than venous type
Clinical Correlates:
- Pulsatile mass with palpable thrill or audible bruit
- Warm skin temperature over lesion due to arterial flow
- May enlarge with increased cardiac output (pregnancy, exercise)
- Risk of high-output cardiac failure in massive lesions
- Bleeding risk with biopsy or incomplete surgery
- Requires preoperative angiography and possible embolization
- Often invades multiple tissue planes
- Highest recurrence rate of all hemangioma types
Venous Hemangioma:
Microscopic Features:
- Thick-walled veins with prominent smooth muscle
- Dilated vascular spaces with slow blood flow
- Frequent thrombosis with organized thrombi
- Phlebolith formation (dystrophic calcification)
- Infiltration between muscle fibers in intramuscular type
- Variable amounts of fibrous stroma
- Hemosiderin deposition throughout lesion
- Immunoreactive for smooth muscle actin in vessel walls
Clinical Correlates:
- Most common type in skeletal muscle (60% of intramuscular)
- Deep location with ill-defined margins
- Pain with activity (venous distension) or positional changes
- Phleboliths on radiographs (pathognomonic finding)
- MRI shows hyperintense T2 signal with flow voids
- Infiltrative growth makes complete excision difficult
- Recurrence in 30-40% after incomplete excision
- May require preoperative embolization if extensive
Epithelioid Hemangioma:
Microscopic Features:
- Plump epithelioid endothelial cells lining vessels
- Well-formed vascular channels with variable lumens
- Inflammatory infiltrate with eosinophils and lymphocytes
- May have solid areas mimicking angiosarcoma
- Low mitotic activity distinguishes from malignancy
- Immunoreactive for endothelial markers (CD31, ERG)
- Negative for cytokeratin (excludes epithelial tumors)
- May have lymphoid aggregates or germinal centers
Clinical Correlates:
- Previously termed "histiocytoid hemangioma"
- Often occurs in head and neck or distal extremities
- May present as multiple lesions
- Associated with trauma or arteriovenous malformation
- Can recur locally after excision
- Very rarely progresses to angiosarcoma
- Important to distinguish from epithelioid angiosarcoma
- Complete excision curative in most cases
Clinical Classification (Mulliken-Glowacki)
Infantile Hemangioma:
- Not present or minimally present at birth
- Rapid proliferation during first year of life
- GLUT-1 positive (distinguishes from congenital type)
- Female predominance (3:1 ratio)
- 50% involute by age 5, 70% by age 7
- May require propranolol for complicated cases
- Indications for treatment: functional impairment, ulceration, disfigurement
- Observation appropriate for uncomplicated lesions
Congenital Hemangioma:
Rapidly Involuting (RICH):
- Fully formed at birth, then rapidly regresses
- Complete involution by 12-14 months of age
- GLUT-1 negative (key distinguishing feature)
- Equal sex distribution
- Usually solitary lesion
- May leave residual skin changes
- Observation appropriate for most cases
- Surgical excision if symptomatic
Non-Involuting (NICH):
- Fully formed at birth, remains stable
- Does not proliferate or involute over time
- GLUT-1 negative like RICH variant
- Persists into adulthood without treatment
- May require surgical excision for symptoms or cosmesis
- Complete excision usually curative
- Lower recurrence than intramuscular types
- Consider excision in childhood for accessible lesions
Clinical Presentation
Presenting Signs and Symptoms
Asymptomatic Mass (40% of cases):
- Incidental finding during examination for other reasons
- Palpable soft tissue fullness or swelling
- No associated pain, tenderness, or functional limitation
- May have been present for months to years
- Slow growth pattern without recent change
- No overlying skin changes in deep lesions
- Patient or parent notices visible lump
- More common in older children and adults
Pain Syndromes (35% of cases):
Intramuscular Venous Hemangioma Pain:
- Dull, aching pain with activity or muscle contraction
- Venous distension and engorgement during exercise
- Positional pain (worse with dependent positioning)
- Relief with rest and elevation
- Night pain if significant venous stasis
- Tenderness to palpation over lesion
- Exacerbated by Valsalva maneuver
- May mimic chronic compartment syndrome
Acute Thrombosis Pain:
- Sudden onset severe pain in previously asymptomatic lesion
- Firm, tender mass with local inflammation
- Overlying skin warmth and erythema possible
- Usually self-limited episode lasting days to weeks
- May have palpable phleboliths after thrombosis resolves
- Risk of recurrent thrombotic episodes
- Distinguish from deep vein thrombosis or infection
- May require imaging to exclude other pathology
- Restricted range of motion in adjacent joint
- Muscle weakness from infiltration or compression
- Neurologic symptoms if compressing adjacent nerve
- Vascular compromise if compressing major vessels
- Compartment syndrome in rapidly enlarging lesions
- Gait abnormality with lower extremity lesions
- Hand dysfunction with upper extremity involvement
- Cosmetic concerns in exposed areas
- Recurrent hemarthrosis in intra-articular lesions
- Spontaneous bleeding episodes with trauma
- Ecchymosis after minor injury
- Hemarthrosis causes joint swelling and pain
- Progressive joint damage from recurrent bleeding
- Hemosiderin deposition in synovium
- May mimic hemophilia or pigmented villonodular synovitis
- Requires synovectomy for definitive treatment
- Kasabach-Merritt phenomenon (NOT with true hemangiomas)
- Occurs with kaposiform hemangioendothelioma or tufted angioma
- Thrombocytopenia, hypofibrinogenemia, elevated D-dimer
- Petechiae, purpura, or spontaneous bleeding
- Life-threatening complication requiring urgent treatment
- Differentiate true hemangioma from kaposiform type
- Treatment with corticosteroids, vincristine, or sirolimus
- Surgical excision contraindicated during acute phase
Physical Examination Findings
- Visible swelling or fullness in affected region
- Bluish or purple skin discoloration if superficial
- Dilated superficial veins over lesion (venous drainage)
- Skin temperature normal or slightly warm
- No skin ulceration in uncomplicated cases
- Asymmetry compared to contralateral limb
- Muscle atrophy if chronic compression of muscle
- Scars from previous biopsy or surgery attempts
- Soft, compressible mass that refills after compression
- Non-tender in most cases (except thrombosed lesions)
- Ill-defined margins with infiltrative lesions
- Reducible with elevation and compression (venous type)
- May feel phleboliths as hard nodules within soft mass
- Increased size with dependent positioning
- Valsalva maneuver may increase lesion size
- No associated lymphadenopathy
Empty-Refill Test:
- Elevate extremity and compress mass to empty venous spaces
- Lower extremity and release compression
- Slow refilling over 15-30 seconds suggests low-flow venous hemangioma
- Rapid refilling suggests high-flow arteriovenous type
- Helps distinguish hemangioma from solid tumor
- Correlates with venographic findings
- Useful for clinical differentiation of subtypes
- Positive test supports diagnosis of vascular lesion
Auscultation:
- Audible bruit suggests arteriovenous hemangioma or malformation
- Absence of bruit in venous or capillary types
- Palpable thrill with high-flow arteriovenous lesions
- Increased heart rate or cardiac output with massive lesions
- Bruit accentuated with exercise or increased flow
- Helps identify high-risk lesions requiring embolization
- Important to assess before surgical intervention
- May indicate need for preoperative angiography
Age-Specific Presentations
- Rapidly enlarging red or purple mass
- May not be present at birth (grows after birth)
- Alarming growth rate concerns parents
- Risk of ulceration with rapid proliferation
- Functional impairment if near vital structures
- Airway compromise with head and neck lesions
- Visual obstruction with periorbital location
- Consider propranolol for complicated cases
- Slower growth or stable size after infancy
- Pain with activity in intramuscular lesions
- Functional limitations during sports or play
- Cosmetic concerns in exposed areas
- May have phleboliths visible on radiographs
- School-age children more aware of differences
- Psychological impact of visible deformity
- Optimal time for surgical excision if indicated
- Long-standing stable mass with recent growth
- Pain more prominent than in children
- Hormonal influences may cause enlargement
- Pregnancy-associated growth in females
- Occupational impact from functional limitations
- Diagnostic challenge if first presentation in adulthood
- Higher suspicion for malignancy in adult presentations
- MRI and possible biopsy to exclude sarcoma
Investigations
Mnemonic
Hook:PRIME Imaging
Radiographic Imaging
Plain Radiographs:
Pathognomonic Findings:
- Phleboliths: Round or oval calcifications with radiolucent centers
- Present in 50% of soft tissue hemangiomas
- More common in cavernous and venous subtypes
- Size ranges from 2 mm to greater than 10 mm
- Multiple phleboliths create "grapes in a bag" appearance
- Calcifications follow venous distribution pattern
- May be only radiographic finding in chronic lesions
- Absence does not exclude diagnosis
Associated Findings:
- Soft tissue mass without calcification in 50% of cases
- Periosteal reaction if adjacent to bone (rare)
- Bone remodeling or scalloping from mass effect
- Increased bone density from hyperemia (children)
- Joint space widening with intra-articular lesions
- Osteopenia from disuse if chronic pain present
- Comparison views help assess asymmetry
- Low sensitivity for diagnosis but high specificity if phleboliths present
Ultrasound:
Advantages:
- Non-invasive, no radiation exposure
- Useful in infants and young children
- Real-time assessment of compressibility
- Doppler evaluation of blood flow characteristics
- Differentiates solid from cystic lesions
- Can guide biopsy if needed
- Monitors response to treatment over time
- Readily available and cost-effective
Sonographic Features:
- Heterogeneous echogenicity with mixed solid-cystic areas
- Hyperechoic phleboliths with posterior acoustic shadowing
- Doppler shows low-flow venous signals (venous type)
- High-flow arterial waveforms (arteriovenous type)
- Compressibility confirms vascular nature
- Septations within lesion common
- May demonstrate thrombosed areas as hypoechoic regions
- Limited for deep lesions or extent determination
Magnetic Resonance Imaging
MRI Protocol for Soft Tissue Hemangioma:
- T1-weighted sequences: Isointense to muscle, hyperintense if fat present
- T2-weighted sequences: Markedly hyperintense (diagnostic hallmark)
- Fat-suppressed sequences: Remain hyperintense (confirms fluid, not fat)
- T1 post-contrast: Serpentine or diffuse enhancement pattern
- Dynamic contrast-enhanced: Early enhancement with gradual filling
- Gradient echo sequences: Blooming artifact from phleboliths (flow voids)
- Include entire anatomic compartment to assess extent
- Coronal and sagittal planes for surgical planning
T2-Weighted Signal Characteristics:
Hyperintense Signal:
- Bright signal equal to or greater than fat on T2 sequences
- Reflects slow-flowing blood and vascular spaces
- Serpentine or lobulated hyperintense areas
- Multiple flow voids (signal dropout) from vessels
- Distinguishes hemangioma from solid tumors
- Heterogeneous signal from thrombosis or hemorrhage
- Septations appear as low signal bands
- Surrounding muscle edema if rapid growth or thrombosis
Flow Voids:
- Serpiginous areas of signal dropout on all sequences
- Represent rapidly flowing blood in feeding/draining vessels
- More prominent in arteriovenous subtypes
- Helpful to identify vascular nature of lesion
- Distinguish from cystic lesions (no flow voids)
- May see layering fluid-fluid levels from blood products
- Phleboliths appear as signal voids with GRE blooming
- Number of flow voids correlates with vascularity
Enhancement Patterns:
Venous Hemangioma:
- Gradual progressive enhancement over 5-10 minutes
- Peripheral to central filling pattern
- Enhancement persists on delayed images
- Heterogeneous due to thrombosis and fibrosis
- Septations enhance more than vascular spaces
- Feeding and draining veins enhance prominently
- No rapid arterial phase enhancement
- Correlates with slow-flow venous lesion
Arteriovenous Hemangioma:
- Rapid arterial phase enhancement
- Prominent feeding arteries and draining veins
- Early venous return on dynamic imaging
- Diffuse homogeneous enhancement
- Enlarged feeding vessels with flow voids
- May see arteriovenous shunting on time-resolved MRA
- High-flow characteristics require preoperative planning
- Embolization often needed before surgery
Extent and Margin Assessment:
- Infiltration into multiple muscle groups common
- Follows fascial planes and neurovascular bundles
- Poorly defined margins in 80% of intramuscular cases
- May encase nerves or vessels without invasion
- Involvement of adjacent joints in 10% of cases
- Subcutaneous extension from deep lesions
- Atrophy of infiltrated muscles on chronic imaging
- Compare to contralateral side for subtle findings
Advanced Imaging Studies
Angiography (Conventional or CT/MR Angiography):
Indications:
- Suspected high-flow arteriovenous hemangioma
- Preoperative planning for large or complex lesions
- Embolization treatment planning
- Differentiate from arteriovenous malformation
- Assess feeding vessels before surgery
- Map venous drainage patterns
- Guide sclerotherapy interventions
- Failed prior surgery with recurrence
Angiographic Findings:
- Low-flow lesions: Slow opacification, venous pooling, delayed washout
- High-flow lesions: Early arterial filling, arteriovenous shunting, enlarged feeders
- Phleboliths visible as filling defects
- "Puddle sign" of contrast pooling in cavernous spaces
- Draining veins without capillary blush (AV type)
- Feeding arteries may be hypertrophied
- Distinguish from vascular malformations (dysplastic vessels)
- Embolization coils or particles visible if prior treatment
Computed Tomography:
Limited Role:
- Inferior soft tissue contrast compared to MRI
- Radiation exposure limits use in children
- Useful if MRI contraindicated (pacemaker, metal)
- Excellent for detecting phleboliths
- CT angiography for vascular mapping in select cases
- Three-dimensional reconstruction for surgical planning
- Assess bony involvement adjacent to lesion
- Generally not first-line imaging modality
CT Findings:
- Heterogeneous soft tissue mass
- Calcified phleboliths (easier to detect than on MRI)
- Enhancement with intravenous contrast
- Infiltration of muscle compartments
- Enlarged feeding or draining vessels in high-flow lesions
- Bony remodeling or erosion in chronic cases
- Fluid-fluid levels from hemorrhage or thrombosis
- Similar findings to MRI but less specific
Histopathology and Biopsy
Biopsy Indications:
- Atypical presentation in adults (exclude sarcoma)
- Rapid growth or change in character
- Absence of characteristic imaging features
- Diagnostic uncertainty after MRI
- Solid-appearing lesion without vascular features
- Patient age greater than 40 at first presentation
- Consider core needle biopsy over open biopsy
- Avoid biopsy of high-flow lesions without embolization
Histologic Features:
Capillary Hemangioma:
- Lobules of capillary-sized vessels with narrow lumens
- Plump endothelial cells without significant atypia
- Mitotic figures may be present in proliferating lesions
- Pericytes surrounding endothelial channels
- Minimal intervening stroma
- Immunohistochemistry: CD31+, CD34+, ERG+, GLUT-1+ (infantile)
- Low-grade cytologic atypia acceptable
- Distinguish from angiosarcoma (high-grade atypia, infiltration, necrosis)
Cavernous/Venous Hemangioma:
- Large dilated vascular spaces lined by flat endothelium
- Thrombosis within vascular channels (common)
- Organized thrombi with recanalization
- Dystrophic calcification (phleboliths) in vessel walls
- Smooth muscle in walls of larger vessels
- Hemosiderin deposition from prior hemorrhage
- Fibrous septations between vascular spaces
- Infiltration between muscle fibers in intramuscular type
- CD31 (endothelial marker): Positive in all subtypes
- CD34 (endothelial and stromal): Positive
- ERG (endothelial transcription factor): Positive
- Factor VIII (von Willebrand factor): Variable positive
- GLUT-1 (glucose transporter): Positive only in infantile hemangioma
- Ki-67 (proliferation): Elevated in proliferating infantile type
- Smooth muscle actin: Positive in pericytes and vessel walls
- Cytokeratin: Negative (excludes epithelial tumors)
- Angiosarcoma: High-grade cytologic atypia, infiltration, necrosis, mitoses
- Kaposi sarcoma: Spindle cell proliferation, HHV-8 positive, fascicular pattern
- Intramuscular myxoma: Hypocellular myxoid stroma, no vessels
- Vascular malformation: Dysplastic vessels, no proliferation
- Hemangiopericytoma/Solitary fibrous tumor: Staghorn vessels, STAT6+
- Epithelioid hemangioendothelioma: Epithelioid cells, myxoid stroma, keratin+
- Kaposiform hemangioendothelioma: Infiltrative, glomeruloid vessels
- Synovial sarcoma: Biphasic pattern, SYT-SSX fusion, cytokeratin+
Differential Diagnosis (Quick Reference)
- Discriminating Feature
- Benign, compressible, slow growth
- Imaging Clue
- T2 hyperintense, flow voids, phleboliths
- Key Test / Pitfall
- Phleboliths pathognomonic; benign (no biopsy if classic)
- Discriminating Feature
- Present at birth, grows with child, GLUT-1 negative
- Imaging Clue
- No endothelial proliferation; phleboliths in venous type
- Key Test / Pitfall
- ISSVA: malformation not tumour; never involutes
- Discriminating Feature
- Older adult, rapid growth, may ulcerate
- Imaging Clue
- Ill-defined infiltrative enhancing mass
- Key Test / Pitfall
- High-grade atypia, mitoses, necrosis on biopsy
- Discriminating Feature
- Painless, no vascular features
- Imaging Clue
- T2 hyperintense but NO phleboliths/flow voids
- Key Test / Pitfall
- Hypocellular myxoid stroma; GNAS mutation
- Discriminating Feature
- Infant, firm, NOT compressible
- Imaging Clue
- Infiltrative; ill-defined margins
- Key Test / Pitfall
- Kasabach-Merritt (thrombocytopenia) - EXAM TRAP
- Discriminating Feature
- Recurrent haemarthrosis, joint-based
- Imaging Clue
- Blooming on GRE (haemosiderin)
- Key Test / Pitfall
- Synovial origin; CSF1 rearrangement
Management
Conservative Management
Observation Protocols:
Indications for Observation:
- Asymptomatic small lesions (less than 3 cm)
- Infantile hemangiomas in proliferative phase (first 12 months)
- No functional impairment of adjacent structures
- No rapid growth or concerning features
- Diagnosis confirmed on imaging
- Patient preference for non-surgical approach
- Elderly patients with medical comorbidities
- Lesions in areas where excision would cause significant morbidity
Monitoring Strategy:
- Clinical examination every 3-6 months initially
- Baseline MRI to document size and characteristics
- Repeat MRI at 12 months or if symptoms develop
- Photographic documentation for superficial lesions
- Symptom diary for pain or functional limitations
- Parent/patient education on warning signs
- Expected natural history discussion (involution in infantile type)
- Consider intervention if enlargement or new symptoms
Medical Management:
Propranolol for Infantile Hemangiomas:
- Indications: Rapidly proliferating infantile hemangiomas causing functional impairment, ulceration, or disfigurement
- Mechanism: Beta-blocker causing vasoconstriction, decreased VEGF, increased apoptosis
- Dosing: Start 1 mg/kg/day divided, increase to 2-3 mg/kg/day over 2 weeks
- Duration: Continue through proliferative phase (usually 6-12 months)
- Monitoring: Baseline ECG, blood pressure, heart rate checks
- Side effects: Bradycardia, hypotension, hypoglycemia, bronchospasm
- Efficacy: 60-80% response rate with size reduction
- Timing: Most effective when started before 5 months of age
- Contraindications: Asthma, heart block, hypotension
Topical Timolol (Small, Superficial Infantile Hemangiomas):
- Indication: small, thin, superficial infantile hemangiomas not warranting systemic therapy — the topical counterpart to oral propranolol
- Agent: timolol maleate 0.5% gel-forming solution, a topical beta-blocker; typically one drop applied to the lesion twice daily
- Rationale: targets the same beta-adrenergic pathway as propranolol (vasoconstriction, reduced VEGF, increased apoptosis) while avoiding the systemic risks (bradycardia, hypotension, hypoglycaemia) of oral therapy
- Limitations: little benefit for deep or thick lesions (poor penetration); systemic absorption is low but use caution on ulcerated lesions and in premature/very-low-birth-weight infants
- Evidence: endorsed as an option for select small superficial lesions in the AAP clinical practice guideline (Krowchuk, Pediatrics 2019, PMID 30584062)
Corticosteroids (Second-Line):
- Prednisolone 2-3 mg/kg/day for proliferating infantile hemangiomas
- Less effective than propranolol (30-40% response rate)
- Side effects: Growth suppression, Cushingoid features, infection risk
- Reserved for cases with contraindications to propranolol
- Duration: 4-8 weeks with gradual taper
- Combination with propranolol for refractory cases
- Monitor growth, blood pressure, glucose
- Intralesional steroids for small localized lesions
Compression Therapy:
- Elastic compression garments for superficial lesions
- Reduces venous pooling and discomfort
- May decrease size through chronic compression
- Useful adjunct to other treatments
- Compliance challenging in pediatric patients
- Limited efficacy for deep intramuscular lesions
- Custom-fitted garments provide better results
- Continue for 6-12 months for maximal effect
Minimally Invasive Interventions
Sclerotherapy:
Technique:
- Ultrasound or fluoroscopic guidance
- Percutaneous injection of sclerosant into vascular spaces
- Agents: Ethanol, sodium tetradecyl sulfate, bleomycin, polidocanol, doxycycline
- Multiple sessions usually required (3-5 treatments)
- Interval of 4-6 weeks between treatments
- May combine with compression after treatment
- Performed under sedation or general anesthesia
- Avoid injection into feeding arteries
Indications:
- Low-flow venous or cavernous hemangiomas
- Accessible lesions amenable to percutaneous approach
- Patients preferring non-surgical treatment
- Poor surgical candidates due to comorbidities
- Recurrent lesions after incomplete excision
- Multiple small hemangiomas (diffuse hemangiomatosis)
- Lesions in anatomically challenging locations
- Adjunct to surgery for large lesions
Outcomes and Complications:
- Success rate: 60-80% for appropriately selected lesions
- Complete resolution uncommon (less than 30%)
- Pain and swelling post-procedure (common, self-limited)
- Skin necrosis from extravasation of sclerosant (2-5%)
- Nerve injury from sclerosant diffusion (rare)
- Compartment syndrome if large volume injected
- Deep vein thrombosis from venous sclerosis
- May require subsequent surgery for residual lesion
Embolization:
Indications:
- High-flow arteriovenous hemangiomas
- Preoperative reduction of blood flow before surgery
- Large lesions with significant bleeding risk
- Failed sclerotherapy or surgical excision
- Lesions not amenable to complete surgical excision
- Symptomatic relief without definitive surgery
- Recurrent bleeding episodes
- Part of multimodal treatment strategy
Technique:
- Selective catheterization of feeding arteries
- Injection of embolic materials (coils, particles, glue, Onyx)
- Proximal and distal embolization to prevent collateral flow
- Staged embolization for extensive lesions
- Perform 24-72 hours before planned surgery (if preoperative)
- General anesthesia or conscious sedation
- Avoid non-target embolization to normal tissues
- Post-procedure angiography confirms occlusion
Complications:
- Skin necrosis from non-target embolization (3-5%)
- Nerve injury from ischemia (rare)
- Post-embolization syndrome: Pain, fever, nausea (common, self-limited)
- Recanalization and recurrence (10-20%)
- Infection of necrotic tissue
- Incomplete embolization requiring repeat procedures
- Distal ischemia if collateral circulation inadequate
- Migration of embolic material
Laser Therapy:
Indications:
- Superficial cutaneous hemangiomas
- Infantile hemangiomas with ulceration or bleeding
- Residual telangiectasias after involution
- Cosmetic improvement of color and texture
- Not effective for deep intramuscular lesions
- Adjunct to other treatments for mixed lesions
- Early treatment may reduce proliferation
- Multiple sessions required for optimal results
Modalities:
- Pulsed dye laser (595 nm): Targets hemoglobin, superficial lesions
- Nd:YAG laser (1064 nm): Greater penetration, thicker lesions
- KTP laser (532 nm): Alternative to pulsed dye laser
- CO2 laser: For ulcerated or friable lesions (resurfacing)
- Settings adjusted based on lesion characteristics
- Cooling devices protect epidermis
- General anesthesia for extensive lesions in children
- Interval of 6-8 weeks between treatments
Surgical Management
Mnemonic
Hook:EXCISE
Surgical Indications:
Absolute Indications:
- Symptomatic compression of neurovascular structures
- Recurrent bleeding or thrombosis causing pain
- Functional impairment limiting activities of daily living
- Diagnostic uncertainty requiring excisional biopsy
- Failed conservative management with progression
- Recurrent hemarthrosis causing joint damage
- Compartment syndrome from rapidly enlarging lesion
- Pathologic fracture through bone involvement (rare)
Relative Indications:
- Cosmetic concerns in visible locations
- Persistent pain despite conservative treatment
- Patient preference for definitive treatment
- Lesion in location amenable to complete excision
- Age appropriate for elective surgery (greater than 1 year)
- Stable lesion unlikely to involute spontaneously
- Psychological impact on patient or family
- Interference with normal development or activities
Preoperative Planning:
Imaging Review:
- MRI assessment of extent in all three planes
- Identify relationship to neurovascular structures
- Determine involvement of muscle groups and compartments
- Plan surgical approach based on anatomic location
- Angiography if high-flow features on MRI
- Mark skin incision and expected extent of resection
- Review images with patient/family to set expectations
- Consider interventional radiology consultation for embolization
Blood Management:
- Type and cross-match blood products (2-4 units for large lesions)
- Cell saver for large resections (if not contaminated)
- Tranexamic acid administration (10-15 mg/kg IV bolus, then infusion)
- Tourniquet use for extremity lesions (tourniquet time limits apply)
- Consider preoperative embolization for high-flow or greater than 5 cm lesions
- Timing of surgery 24-72 hours after embolization optimal
- Hemostatic agents available (thrombin, gelatin, oxidized cellulose)
- Discuss bleeding risk with patient and anesthesia team
Consent Discussion:
- Risk of incomplete excision and recurrence (20-40%)
- Bleeding risk and possible transfusion requirement
- Nerve or vessel injury from dissection (5-10% for large lesions)
- Muscle weakness from sacrifice of involved muscle
- Scar and cosmetic outcome
- Possibility of staged procedures for massive lesions
- Alternative treatments and risks of observation
- Realistic expectations about functional outcome
Surgical Technique:
Approach and Exposure:
- Longitudinal incision along line of limb for extremity lesions
- Extensile approach allowing proximal and distal extension
- Identify and protect neurovascular structures early
- Develop plane between lesion and uninvolved muscle
- Recognize infiltrative nature - often appears worse than imaging
- Use loupe magnification for small vessel ligation
- Tourniquet inflated after exsanguination (extremity)
- Adequate assistant and retraction essential
Resection Principles:
- Complete excision of all involved tissue (most important factor)
- Sacrifice involved muscle if necessary for negative margins
- Follow fascial planes to limit dissection
- Sequential ligation of feeding vessels reduces bleeding
- Preserve major nerves and vessels (may require careful dissection from lesion)
- Remove all phleboliths and thrombosed areas (often at periphery)
- Frozen section if margins unclear (distinguish from normal muscle)
- Accept some muscle dysfunction to achieve complete excision
Hemostasis Techniques:
- Meticulous electrocautery of small vessels
- Suture ligation of larger feeding and draining vessels
- Topical hemostatic agents in resection bed
- Oxidized cellulose or gelatin sponges for oozing
- Avoid excessive cautery (causes muscle necrosis and complications)
- Tourniquet deflation before closure to check hemostasis
- Closed suction drainage (Jackson-Pratt or Blake) for dead space
- Compression dressing postoperatively
Reconstruction and Closure:
- Muscle approximation if possible without tension
- Drain placement in deep dead space (avoid hematoma)
- Layered closure with absorbable sutures
- Skin closure with subcuticular or interrupted sutures
- No role for primary muscle flap reconstruction usually
- Consider skin graft if skin loss from extensive resection
- Splint or immobilize if near joint (allow soft tissue healing)
- Compression dressing for venous hemangiomas
Postoperative Management:
Immediate Postoperative (0-48 hours):
- Monitor drain output (expect 50-200 mL/day initially)
- Pain control with multimodal analgesia
- Check distal neurovascular status frequently
- Elevate extremity to reduce swelling
- Remove drain when output less than 30 mL/day (usually 3-7 days)
- Monitor for signs of compartment syndrome if extensive resection
- Deep vein thrombosis prophylaxis for lower extremity
- Early range of motion of digits to prevent stiffness
Rehabilitation:
- Physical therapy starting postoperative day 1-2
- Gentle active range of motion initially
- Progress to strengthening at 4-6 weeks
- Scar massage starting at 2-3 weeks
- Compression garment if significant edema
- Return to full activities at 3-4 months
- Monitor for delayed complications (seroma, hematoma)
- Long-term surveillance for recurrence (clinical exam every 6 months for 2 years)
Special Surgical Scenarios:
Intra-articular Hemangiomas:
- Arthroscopic versus open synovectomy
- Remove all involved synovium to prevent recurrence
- Hemarthrosis causes hemosiderin deposition and further synovitis
- May require total synovectomy for diffuse involvement
- Postoperative arthrofibrosis risk (aggressive rehabilitation)
- Consider radiosynovectomy for elderly or high-risk patients
- Recurrence common if incomplete synovectomy (30-50%)
- Joint replacement may be necessary for advanced arthritis
Recurrent Hemangiomas:
- MRI to define extent before reoperation
- Scar tissue makes dissection more challenging
- Higher risk of nerve and vessel injury
- Consider alternatives (sclerotherapy, embolization) before reoperation
- May require more extensive resection at reoperation
- Discuss realistic expectations (may not achieve complete excision)
- Staged procedures for massive recurrent lesions
- Some patients managed with symptom control rather than cure
Outcomes and Prognosis
- Complete excision curative in 60-80% of cases
- Recurrence rate 20-40% with incomplete excision
- Functional outcomes generally good if nerve preserved
- Some muscle weakness expected if muscle sacrificed
- Cosmetic outcomes acceptable with modern techniques
- Patient satisfaction high if expectations managed
- Most patients return to full activities by 4-6 months
- Recurrent bleeding rare after complete excision
- Infantile hemangiomas: 50% involute by age 5, 70% by age 7
- Congenital hemangiomas (RICH): Complete involution by 12-14 months
- Congenital hemangiomas (NICH): Persist without involution
- Intramuscular hemangiomas in adults: Persistent without involution
- Slow growth over years common in adult lesions
- Acute thrombosis episodes may occur intermittently
- Malignant transformation essentially never occurs (benign lesion)
- Quality of life impact depends on symptoms and location
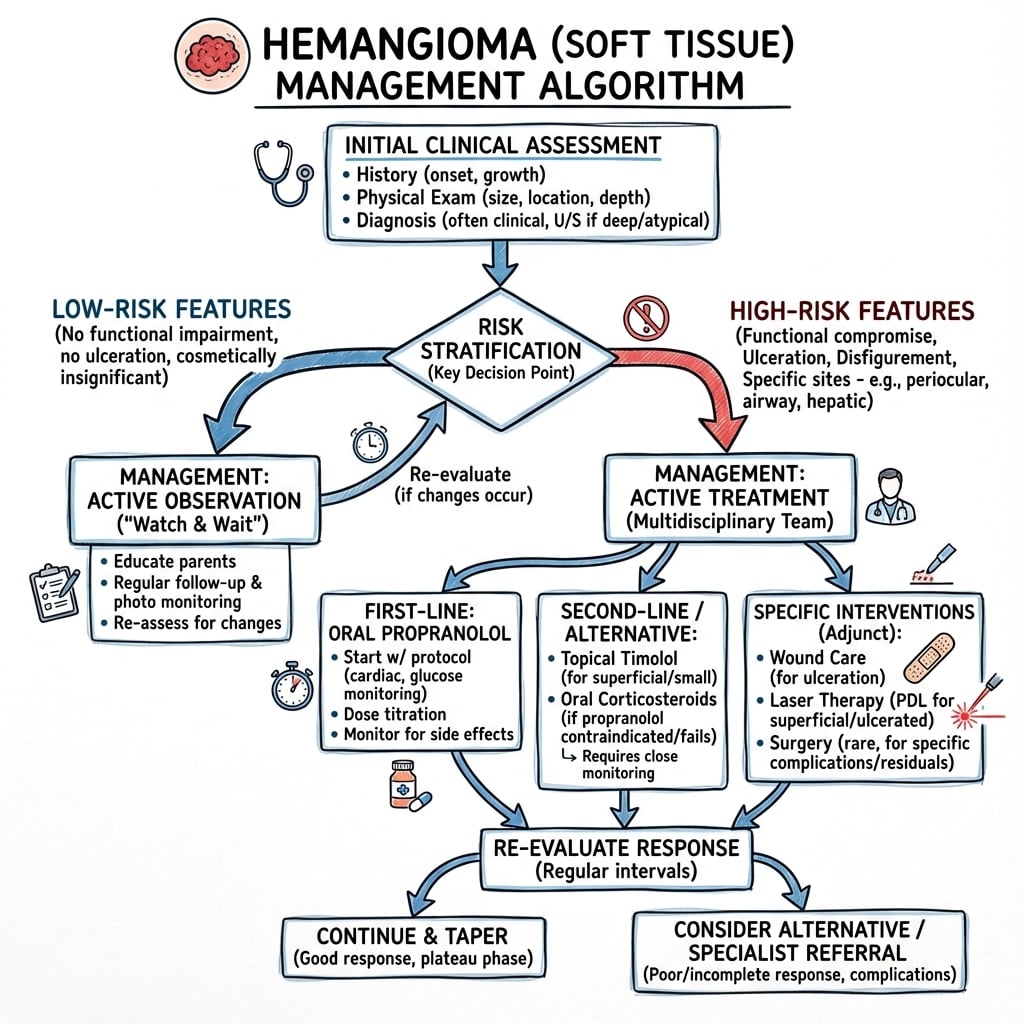
Management Algorithm
Complications
Treatment-Related Complications
Surgical Complications:
Intraoperative Bleeding:
- Incidence: 5-15% require transfusion
- Risk factors: Large lesions (greater than 5 cm), high-flow type, no preoperative embolization
- Presentation: Diffuse oozing from resection bed, tourniquet conceals extent
- Management: Topical hemostatics, suture ligation, tranexamic acid, blood transfusion
- Prevention: Preoperative embolization, meticulous technique, adequate blood available
- Outcome: Rarely causes surgery to be aborted
- Tourniquet use in extremity limits intraoperative blood loss
- Cell saver reduces allogeneic transfusion requirements
Incomplete Excision and Recurrence:
- Incidence: 20-40% with subtotal excision, less than 10% with complete excision
- Cause: Infiltrative margins difficult to identify intraoperatively
- Presentation: Recurrent mass at surgical site months to years later
- Diagnosis: MRI showing recurrent enhancing tissue
- Prevention: Wide margins, sacrifice involved muscle, frozen section guidance
- Management: Observation vs reoperation vs sclerotherapy/embolization
- Some patients managed symptomatically rather than repeat surgery
- Discuss possibility of incomplete excision in preoperative consent
Nerve Injury:
- Incidence: 5-10% for large lesions near neurovascular bundles
- Mechanisms: Stretch injury, iatrogenic transection, ischemia from embolization
- Presentation: Numbness, weakness, neuropathic pain in nerve distribution
- Common nerves at risk: Sciatic (thigh/buttock lesions), radial (arm lesions), median/ulnar (forearm)
- Management: Observation for neurapraxia (6-12 months), exploration and repair if transection
- Prevention: Loupe magnification, meticulous dissection, protect nerves with vessel loops
- Most injuries are neurapraxias that recover over 3-6 months
- Document preoperative neurologic exam for medicolegal protection
Vascular Injury:
- Incidence: Less than 5% clinically significant injuries
- Presentation: Distal ischemia, hematoma, pseudoaneurysm, arteriovenous fistula
- High-risk lesions: Those encasing major vessels, high-flow arteriovenous type
- Management: Vascular surgery consultation, repair or reconstruction as needed
- Prevention: Angiography, careful dissection, vascular instruments available
- May require vein graft reconstruction if vessel sacrificed
- Document distal pulses before and after surgery
- Early recognition and intervention prevents limb loss
Infection:
- Incidence: 2-5% of surgical cases
- Risk factors: Large dead space, hematoma, diabetes, immunosuppression
- Presentation: Erythema, drainage, fever, elevated inflammatory markers
- Organisms: Staphylococcus aureus most common, consider MRSA
- Management: Antibiotics, drainage if abscess or hematoma present
- Prevention: Perioperative antibiotics, sterile technique, drain placement
- Superficial infections managed with oral antibiotics
- Deep infections may require operative debridement
Sclerotherapy Complications:
Skin Necrosis:
- Incidence: 2-5% of sclerotherapy procedures
- Cause: Extravasation of sclerosant, high concentration near skin
- Presentation: Pain, skin discoloration, then ulceration days after procedure
- Management: Wound care, debridement if extensive, skin graft if needed
- Prevention: Careful injection technique, dilute sclerosant concentrations
- Worse with ethanol (most caustic sclerosant)
- Healing by secondary intention acceptable for small areas
- Large areas may require reconstruction
Nerve Injury:
- Incidence: Less than 2% with careful technique
- Mechanism: Direct sclerosant neurotoxicity from diffusion to adjacent nerve
- Presentation: Numbness, dysesthesias, weakness in nerve distribution
- Usually transient with recovery over weeks to months
- Management: Observation, neuropathic pain medications if needed
- Prevention: Avoid injection near major nerves, use image guidance
- Document neurologic exam before procedure
- Permanent injury rare
Deep Vein Thrombosis:
- Risk with sclerotherapy of large venous hemangiomas
- Sclerosant causes thrombosis that may propagate to deep veins
- Symptoms: Calf pain, swelling, positive Homan's sign
- Diagnosis: Duplex ultrasound of deep veins
- Management: Anticoagulation if DVT confirmed
- Prevention: Limit volume of sclerosant, compression after procedure
- Consider prophylactic anticoagulation for high-risk patients
- Monitor for pulmonary embolism if extensive thrombosis
Embolization Complications:
Non-target Embolization:
- Incidence: 3-5% clinically significant events
- Presentation: Skin necrosis, nerve palsy, distal ischemia
- Cause: Reflux of embolic material, collateral flow to normal tissues
- Management: Supportive care, wound care for skin loss, nerve recovery usually complete
- Prevention: Careful catheter placement, avoid overfilling, use appropriate embolic agents
- Most serious complication of embolization
- May require subsequent reconstruction or debridement
Post-embolization Syndrome:
- Incidence: 50-80% after embolization (expected response)
- Symptoms: Pain, fever, nausea, malaise for 3-7 days
- Cause: Tissue ischemia and inflammatory response
- Not infection (cultures negative)
- Management: NSAIDs, antiemetics, hydration, reassurance
- Self-limited with complete resolution
- Distinguish from infection (prolonged course, positive cultures)
- Warn patients preoperatively about expected symptoms
Recanalization and Recurrence:
- Incidence: 10-20% develop collateral flow after embolization
- Presentation: Recurrent symptoms months to years later
- More common with proximal embolization only (allows collateral development)
- Diagnosis: Repeat angiography showing new feeding vessels
- Management: Repeat embolization or surgical excision
- Prevention: Distal and proximal embolization, multiple feeding vessels
- Some lesions require repeated embolizations for symptom control
- Not curative in most cases (palliative treatment)
Disease-Related Complications
- Occurs with kaposiform hemangioendothelioma or tufted angioma, NOT hemangioma
- Consumption coagulopathy with thrombocytopenia, hypofibrinogenemia
- Presentation: Petechiae, purpura, bleeding, rapidly enlarging firm mass
- Life-threatening if untreated (mortality historically 20-30%)
- Diagnosis: Platelets less than 25,000, low fibrinogen, elevated D-dimer, MRI showing infiltrative lesion
- Management: Corticosteroids, vincristine, sirolimus (mTOR inhibitor), supportive care
- Surgery contraindicated during acute phase (high bleeding risk)
- Important to distinguish true hemangioma (no Kasabach-Merritt) from kaposiform type
- Biopsy shows infiltrative glomeruloid capillary proliferation in kaposiform type
- Rare complication of rapidly enlarging hemangioma
- Mechanisms: Hemorrhage into lesion, acute thrombosis with swelling, trauma to lesion
- Presentation: Severe pain, tense compartment, pain with passive stretch, sensory changes
- Diagnosis: Clinical, compartment pressure greater than 30 mmHg confirms
- Management: Urgent fasciotomy, do NOT delay for imaging
- Prevention: Early treatment of symptomatic lesions
- Postoperative compartment syndrome risk after extensive resection
- High index of suspicion in perioperative period
- Rare with soft tissue hemangiomas (occurs with bone hemangiomas)
- Vertebral hemangiomas most prone to fracture
- Presentation: Sudden pain, deformity, neurologic deficit if spine
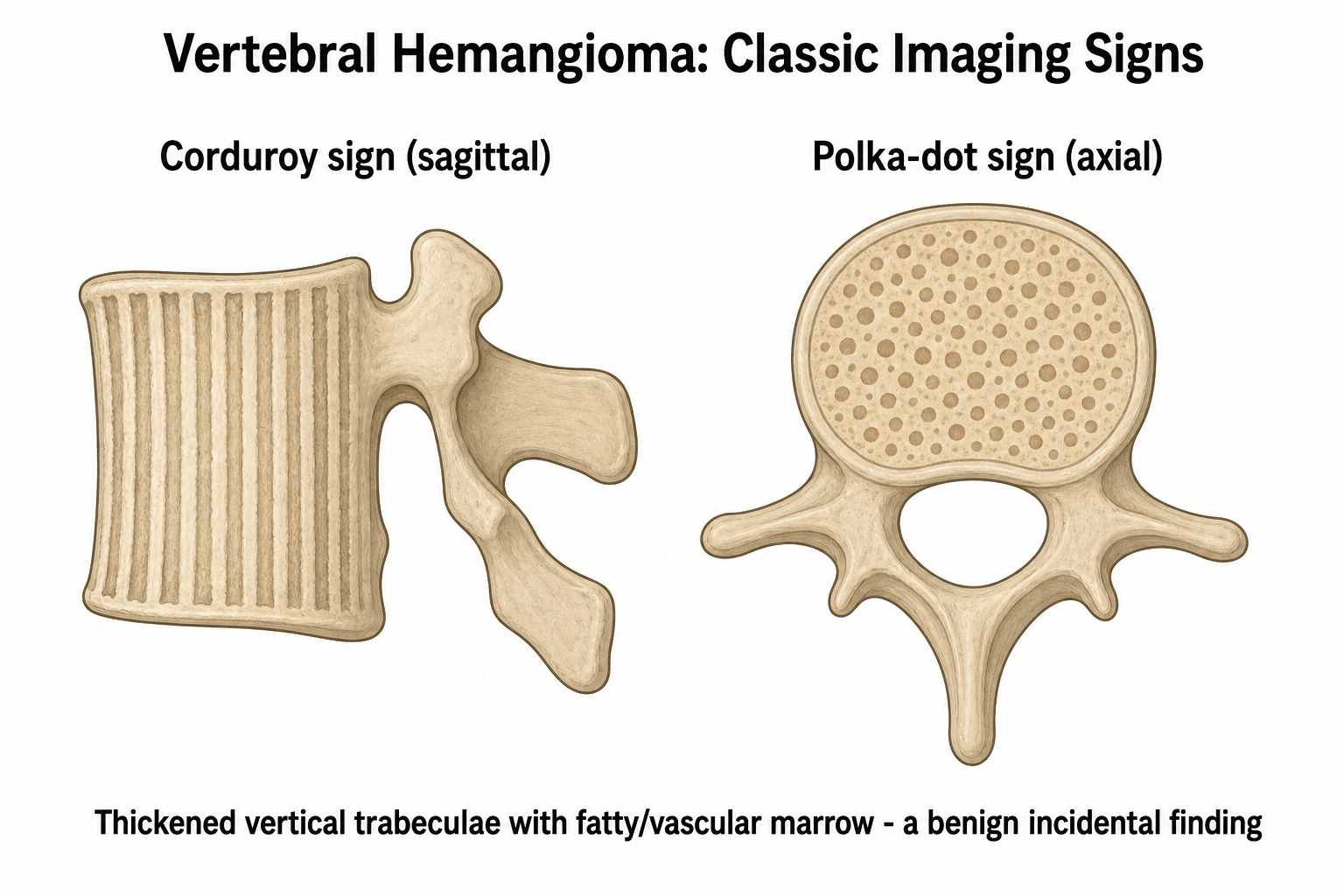
- Imaging: Lytic lesion with trabeculated "corduroy" or "polka dot" appearance
- Management: Stabilization and fixation, embolization, vertebroplasty for spine
- Soft tissue hemangiomas rarely involve bone to degree causing fracture
- Adjacent bone may have remodeling or scalloping from mass effect
- Periosteal reaction suggests aggressive process (reconsider diagnosis)
- Recurrent hemarthrosis causes synovitis and cartilage damage
- Hemosiderin deposition accelerates degenerative changes
- Progression to secondary osteoarthritis if untreated
- Symptoms: Pain, stiffness, limited range of motion, effusions
- Imaging: Joint space narrowing, subchondral sclerosis, osteophytes
- Management: Synovectomy early prevents progression, arthroplasty if end-stage
- Similar pathophysiology to hemophilic arthropathy
- Early treatment prevents irreversible joint damage
Osseous and Vertebral Hemangioma — A Distinct Entity
This page is about the soft-tissue hemangioma, but its complications section (intraosseous/vertebral pathologic fracture) and several MCQ points refer to bone and vertebral hemangioma — a separate, common entity with different behaviour and imaging. It is summarised here so those points make sense; the full detail lives in the dedicated bone hemangioma and vertebral haemangioma topics.
Vertebral hemangioma is the most common benign tumour of the spine and is usually an incidental, asymptomatic intraosseous lesion (thoracic greater than lumbar):
- Imaging (typical/quiescent): vertical "corduroy" or "jail-bar" striations on the lateral radiograph/sagittal images; "polka-dot" pattern of thickened trabeculae in cross-section on axial CT; hyperintense on BOTH T1 and T2 MRI (the combination of intralesional fat and slow-flowing blood) — the high T1 fat signal of a quiescent lesion is reassuring.
- Aggressive features (the exam discriminator): involvement of the whole vertebral body and posterior elements, cortical expansion, an epidural soft-tissue mass, and notably LOW T1 signal (less fat, more vascular stroma). These lesions can cause cord/root compression or pathologic fracture.
- Management: asymptomatic lesions are simply observed; symptomatic or aggressive lesions are treated by vertebroplasty/kyphoplasty (pain and stabilisation), embolisation (vascular control, usually pre-operative), radiotherapy for aggressive lesions, and surgical decompression for neurological deficit. As with soft-tissue lesions, biopsy is generally avoided because of bleeding risk — the diagnosis is made on imaging.
Contrast with the soft-tissue lesion above: the intramuscular soft-tissue hemangioma is an infiltrative, phlebolith-bearing mass treated by complete excision (recurrence if incomplete); the osseous/vertebral lesion is intraosseous, has its own corduroy/polka-dot imaging signature, and is managed predominantly without excision. Detailed coverage of grading, aggressive-lesion management and spinal reconstruction is in the dedicated bone- and vertebral-hemangioma topics.
Guidelines, Registries & Global Practice
Global Epidemiology
- Infantile hemangioma is the most common benign tumour of infancy, occurring in up to 5% of infants (AAP clinical practice guideline). According to PubMed, Krowchuk DP, et al. Pediatrics 2019 DOI.
- Independent risk factors confirmed across large cohorts: female sex (roughly 3:1), low birth weight, prematurity, and multiple gestation. According to PubMed, Hudalla H, et al. Arch Gynecol Obstet 2018 DOI.
- Most rapid proliferation occurs between 1 and 3 months, with growth largely complete by 5 months, defining a narrow window for early referral and treatment of high-risk lesions (AAP 2019).
- Intramuscular (adult-type) hemangiomas are uncommon and benign; the lower limb (especially thigh) predominates, and infiltrative growth drives recurrence. According to PubMed, Allen PW, Enzinger FM. Cancer 1972 DOI.
- No malignant transformation of true hemangioma; the consumption coagulopathy of Kasabach-Merritt phenomenon belongs to kaposiform hemangioendothelioma/tufted angioma, not hemangioma.
Guideline & Classification Framework (Side-by-Side)
- Scope
- Infantile hemangioma
- Core Recommendation
- Risk-stratify; refer high-risk by 1 month; propranolol 2-3 mg/kg/day first-line; topical timolol for small superficial lesions; surgery/laser mainly for residua
- Evidence Basis
- Evidence-based CPG (key/option statements)
- Scope
- All vascular anomalies
- Core Recommendation
- Standardised nomenclature: vascular TUMOURS (e.g. infantile hemangioma) vs MALFORMATIONS; integrate clinical, imaging, histology (GLUT-1), genetics
- Evidence Basis
- Consensus classification
- Scope
- Vascular birthmarks
- Core Recommendation
- Centralised multidisciplinary vascular-anomalies clinics; propranolol via specialist; avoid biopsy of classic lesions
- Evidence Basis
- Service guidance / consensus
- Scope
- Conceptual basis
- Core Recommendation
- Biological dichotomy (proliferative tumour vs structural malformation) underpinning all later schemes
- Evidence Basis
- Landmark cellular study
Treatment Evidence at a Glance
- Indication
- Complicated infantile hemangioma
- Evidence Level
- Level 1 (RCT)
- Key Source
- Léauté-Labrèze, NEJM 2015 (PMID 25693013)
- Indication
- Uncomplicated infantile hemangioma
- Evidence Level
- Guideline (default)
- Key Source
- AAP 2019 (PMID 30584062)
- Indication
- Symptomatic / infiltrative intramuscular hemangioma
- Evidence Level
- Level 4 (case series)
- Key Source
- Allen & Enzinger, Cancer 1972 (PMID 5061701)
- Indication
- Low-flow venous vs high-flow AV lesions
- Evidence Level
- Level 4 (case series)
- Key Source
- Interventional radiology literature
- Indication
- Distinguishing infantile vs congenital/malformation
- Evidence Level
- Level 4 (diagnostic)
- Key Source
- North et al, Hum Pathol 2000 (PMID 10665907)
Practice Variation & Registries
- No dedicated international registry exists for soft-tissue hemangioma; adult intramuscular and complex lesions are captured within soft-tissue tumour / sarcoma services and national soft-tissue tumour databases rather than a hemangioma-specific registry.
- Medical vs interventional vs surgical balance varies by health system: paediatric infantile lesions are predominantly managed medically (propranolol) through dermatology/paediatrics, whereas adult intramuscular lesions are managed by musculoskeletal tumour units, often with interventional-radiology adjuncts (sclerotherapy for low-flow, embolisation for high-flow).
- Access to propranolol is broad in high-income settings, with specialist initiation (paediatric/dermatology) and cardiovascular monitoring (baseline ECG where indicated, blood pressure and heart rate checks) as the standard pathway across most national health systems, including the NHS (UK) and European equivalents.
- Multidisciplinary vascular-anomalies clinics (combining dermatology, plastic/paediatric surgery, interventional radiology and pathology) are the recommended model internationally for complex or diagnostically uncertain lesions.
Exam Relevance (FRACS / FRCS)
- High-yield differentials for a soft-tissue mass: phlebolith recognition on plain film, MRI interpretation (T2 hyperintensity, flow voids, serpentine enhancement), and surgical principles (complete excision to limit recurrence).
- Classic viva traps: hemangioma (tumour) vs vascular malformation; and the Kasabach-Merritt trap (kaposiform hemangioendothelioma, not hemangioma).
MCQ Practice Points
Q: What is the characteristic radiographic appearance of vertebral hemangioma?
A: Corduroy sign (vertical striations on lateral view) and polka-dot sign (axial CT - thickened trabeculae in cross-section). T1 and T2 hyperintense on MRI due to fat and slow-flowing blood. Most are asymptomatic incidental findings. Located in vertebral body, most common in thoracic and lumbar spine.
Q: What features distinguish aggressive from stable vertebral hemangiomas?
A: Aggressive features: Involves entire vertebral body, extends to posterior elements, epidural extension, cortical expansion, soft tissue mass. T1 hypointense (less fat, more vascular). Low fat signal indicates aggressive behavior. Stable hemangiomas: partial body involvement, T1 hyperintense, no expansion.
Q: What is the ISSVA classification approach to vascular anomalies?
A: ISSVA divides vascular anomalies into: Tumors (proliferative - infantile hemangioma) and Malformations (structural). Malformations subdivided by vessel type: capillary, venous, lymphatic, arterial, or combined. Infantile hemangiomas involute; malformations grow proportionally and don't regress. Critical for treatment planning.
Q: What is the natural history of infantile hemangioma?
A: Proliferative phase: Rapid growth 0-12 months. Plateau: 12-18 months. Involution: Gradual regression over 3-9 years. 90% involute by age 9. Treatment (propranolol) indicated for: airway compromise, visual obstruction, ulceration, disfigurement, or high-output cardiac failure from large lesions.
Q: What are the treatment options for symptomatic vertebral hemangioma?
A: Options include: Vertebroplasty/kyphoplasty for pain and stabilization, embolization for vascular control pre-surgery, radiation therapy for aggressive lesions, surgical decompression for neurological deficit. Alcohol ablation reported. Biopsy contraindicated due to bleeding risk - treat based on imaging diagnosis.
At a Glance
Soft tissue hemangiomas are benign vascular tumours composed of proliferating blood vessels - the most common benign soft tissue tumour of infancy/childhood. Phleboliths (round calcifications with lucent centres) are pathognomonic and visible on plain radiographs in 50% of cases. MRI shows characteristic hyperintense T2 signal with flow voids and enhancement. Management is typically observation for asymptomatic lesions (infantile type: 50% involute by age 5); surgical excision for symptomatic, recurrently bleeding, or functionally impairing lesions. Key trap: incomplete excision results in 40% recurrence rate.
CAVEATHemangioma Classification
Hook:Remember CAVEAT - five histologic subtypes and importance of phleboliths
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 12-year-old girl presents with a 2-year history of a painless mass in her right thigh. On examination, there is a 6 cm soft, compressible mass in the anterior compartment. Radiographs show multiple small rounded calcifications within the soft tissues. MRI demonstrates a lobulated, hyperintense T2 mass infiltrating the quadriceps muscle with serpentine enhancement.”
“A 4-month-old infant presents with a rapidly enlarging bright red mass on the left cheek measuring 4 cm x 3 cm. The lesion was not present at birth but appeared at 3 weeks and has grown significantly. On examination, it is a soft, compressible, non-pulsatile mass with overlying telangiectasias. The mass does not blanch completely with pressure. Parents are very concerned about the alarming growth rate and cosmetic appearance.”
One-Liner Definition
- Hemangioma: Benign vascular tumor composed of proliferating blood vessels
- Most common benign soft tissue tumor of infancy
- Classified as capillary, cavernous, arteriovenous, venous, or epithelioid subtypes
Pathognomonic Finding
- Phleboliths: Rounded calcifications with radiolucent centers on radiographs
- Present in 50% of soft tissue hemangiomas
- Dystrophic calcification in thrombosed venous channels, diagnostic when present
Classification (CAVEAT mnemonic)
- Capillary (small vessels, infants)
- Arteriovenous (high flow, pulsatile)
- Venous (most common intramuscular, phleboliths) - 60% of intramuscular types
- Epithelioid (formerly histiocytoid)
- Acquired (exclude congenital)
- Thrombosis (phleboliths on XR)
Clinical Triad
- Soft compressible mass in muscle (75% intramuscular, thigh most common)
- Hyperintense T2 MRI signal with serpentine enhancement and flow voids
- Phleboliths on radiographs (50% of cases) - this triad is diagnostic
MRI Findings (Must-Know)
- Hyperintense T2 signal (equal to or greater than fat)
- Serpentine or lobulated appearance, multiple flow voids
- Gradual progressive enhancement (venous) or rapid arterial enhancement (AV type)
- Infiltrative margins in 80%, phlebolith blooming on GRE sequences
Infantile Hemangioma Natural History
- Proliferative (0-12 months, rapid growth, GLUT-1 positive)
- Plateau (12-18 months, stable size)
- Involution (1-7 years, gradual regression) - 50% by age 5, 70% by age 7
- NOT present at birth (appears weeks after), distinguish from congenital (GLUT-1 negative)
Medical Management
- Propranolol 2-3 mg/kg/day (first-line for infantile hemangiomas)
- Mechanism: vasoconstriction, decreased VEGF/FGF, increased apoptosis; 60-80% response
- Start before 5 months for best results
- Contraindications: asthma, heart block, hypotension; monitor ECG, BP, HR
- Side effects: bradycardia, hypoglycemia, bronchospasm
Surgical Principles (EXCISE mnemonic)
- Embolize high-flow lesions 24-72 hours preop
- eXtensive exposure (underestimate on exam)
- Complete excision (incomplete → 40% recurrence) - MOST important factor for cure
- Infiltration along fascia, Sacrifice involved muscle if needed
- Expect bleeding (blood available, tourniquet for extremity)
Indications for Surgery
- Absolute: symptomatic compression, recurrent bleeding/thrombosis, functional impairment
- Diagnostic uncertainty, failed conservative Rx, recurrent hemarthrosis
- Relative: cosmetic concerns, persistent pain, patient preference
- Observation for: asymptomatic, infantile type (will involute), less than 3 cm
Sclerotherapy vs Embolization
- Sclerotherapy: low-flow venous/cavernous, percutaneous injection, 60-80% success
- Complications: skin necrosis (2-5%), nerve injury, DVT
- Embolization: high-flow AV types, preop reduction, coils/particles/glue
- Complications: non-target embolization (3-5%), post-embolization syndrome (50-80%)
Critical Exam Trap
- Kasabach-Merritt does NOT occur with hemangiomas
- Occurs with kaposiform hemangioendothelioma and tufted angioma (different entities)
- Thrombocytopenia + hypofibrinogenemia + vascular lesion = kaposiform, not hemangioma
- Treatment: steroids, vincristine, sirolimus; surgery contraindicated
Recurrence Risk
- Incomplete excision → 20-40% recurrence
- Complete excision → less than 10% recurrence
- Infiltrative margins make complete excision challenging
- Sacrifice involved muscle to achieve negative margins
- Frozen section may help assess margins intraoperatively
GLUT-1 Immunostaining
- GLUT-1 positive: Infantile hemangioma (distinguishing feature)
- GLUT-1 negative: Congenital hemangioma (RICH and NICH), vascular malformations
- Gold standard test to differentiate infantile from congenital types
- RICH involutes rapidly (12-14 months), NICH persists without involution
High-Yield Associations
- Location: 75% intramuscular (thigh, upper extremity most common)
- Age: peak less than 5 years; Phleboliths: 50% on XR
- Recurrence: 20-40% incomplete excision; Involution: 50% by age 5 (infantile)
- GLUT-1: positive infantile, negative congenital
- Kasabach-Merritt: kaposiform only, NOT hemangioma