The Clenched Fist Injury | Eikenella corrodens
- A 'Fight Bite' is a Septic Arthritis until proven otherwise.
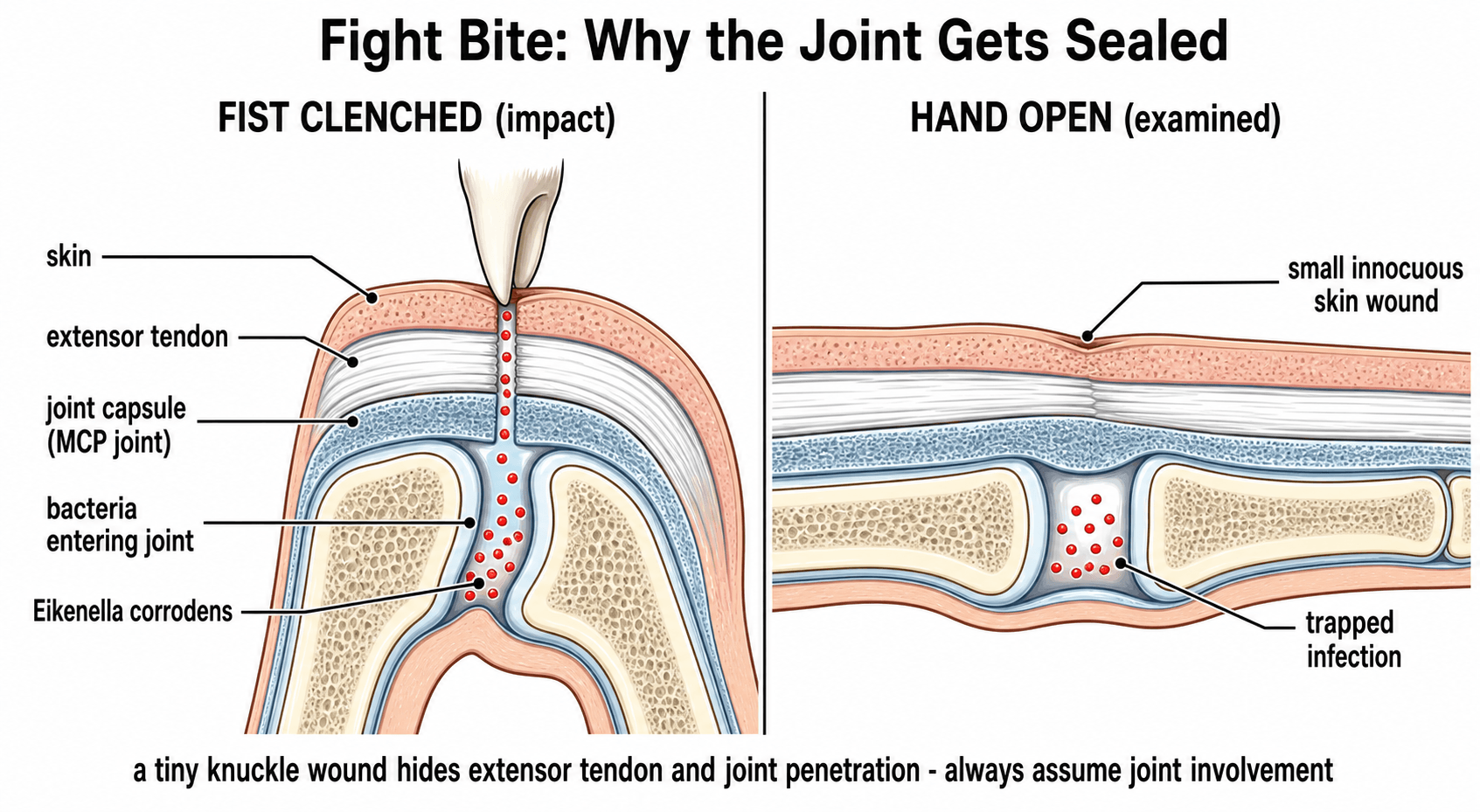
- The tooth penetrates the MCPJ capsule in FLEXION.
- When the finger extends, the tract is sealed by the extensor hood gliding proximally.
- This traps bacteria (Eikenella, Strep, Staph) in the joint.
- Eikenella corrodens is resistant to First Gen Cephalosporins (Keflex) and Clindamycin.
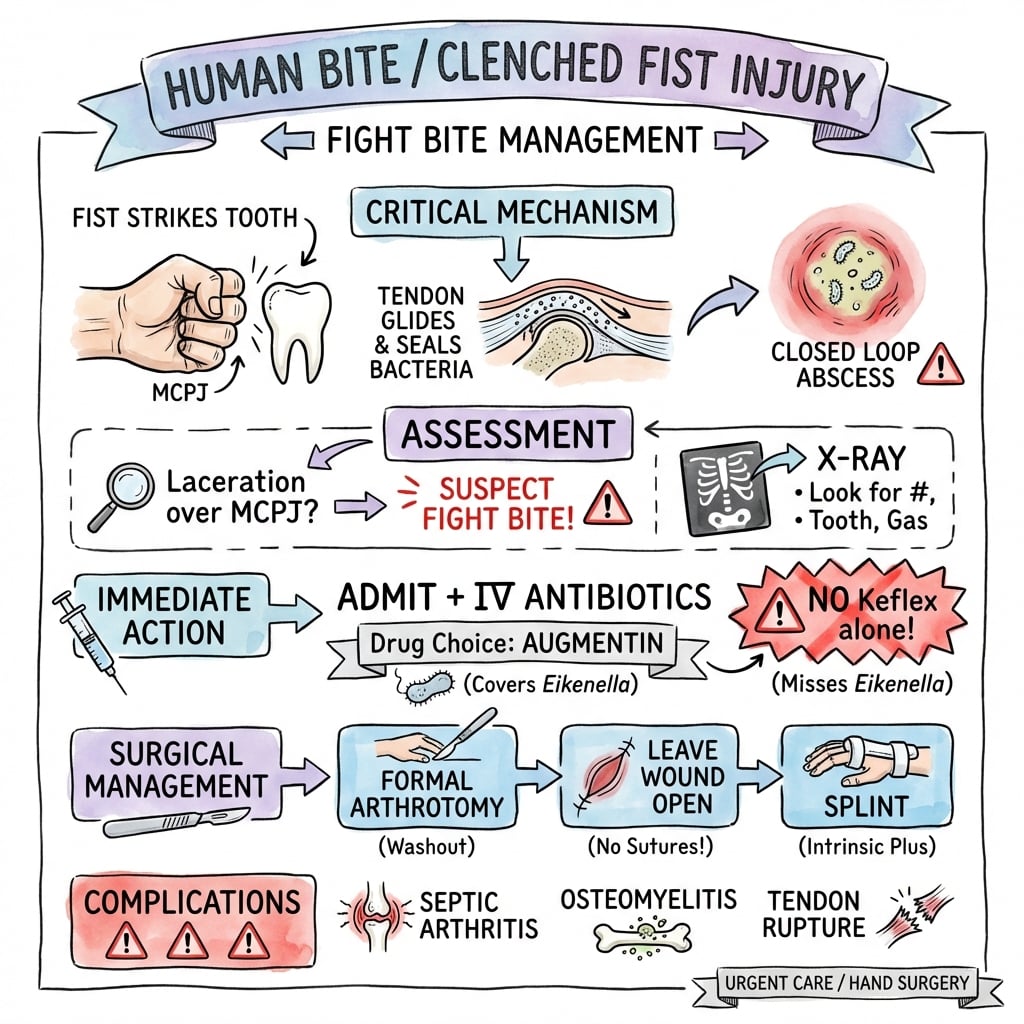
- Treatment is emergent formal arthrotomy and washout.
- “Never trust a 'small cut' over the MCPJ in a young male.
- “Cephalexin alone effectively TREATS the bacteria it covers but SELECTS OUT Eikenella.
- “Augmentin is the drug of choice.
"I cut it on a fence/can/glass" Patients often lie about the mechanism due to shame or legal reasons. A laceration over the 3rd/4th/5th MCPJ is a fight bite until proven otherwise. X-ray may reveal a tooth fragment or 'Boxer's Fracture' (Neck of 5th MC).
Joint Destruction If treated as a simple laceration (sutured), the septic arthritis proceeds unchecked. Cartilage destruction (chondrolysis) occurs within 24-48 hours. Osteomyelitis and amputation are real risks.
- Animal Bite
- Pasteurella / Capnocytophaga
- Human Bite
- Eikenella / Strep Viridans / Staph
- Animal Bite
- Puncture / Crush
- Human Bite
- Inoculation into Joint (CFI)
- Animal Bite
- Augmentin
- Human Bite
- Augmentin (But Ceph/Clinda fail)
- Animal Bite
- Urgent
- Human Bite
- Emergent (if Joint involved)
HACEKEikenella Corrodens
Hook:Eikenella is part of the HACEK group (Endocarditis risk).
FISTAction Plan
Hook:Don't miss the FIST injury.
AUGAntibiotics
Hook:AUGmentin AUGments the cure.
Overview
A "Human Bite" encompasses two distinct injuries: the Occlusal Bite (direct clamp) and the Clenched Fist Injury (CFI). The CFI is the most dangerous, involving the inoculation of oral flora directly into the MCP joint or extensor apparatus by striking a tooth.
Human saliva contains up to 10 billion (10^9) bacteria per mL, with a diverse mix of aerobes and anaerobes. The unique "gliding" mechanism of the extensor tendon over the MCP joint acts as a one-way valve, sealing the inoculum deep within the joint once the fist is relaxed. This creates a closed-loop abscess within the joint capsule that destroys cartilage (chondrolysis) within 48 hours.
Pathophysiology and Mechanisms
The "Sliding Target"
- Impact: Fist is clenched (MCPJs flexed 90 degrees). Extensor tendon and hood move distally over the metacarpal head.
- Penetration: Tooth penetrates skin, tendon, capsule, and enters joint.
- Relaxation: Fist opens (MCPJs extend). Extensor tendon glides proximally.
- Sealing: The skin wound is now proximal to the capsule wound. They are no longer aligned.
This misalignment creates an anaerobic environment within the joint and prevents drainage.
Microbiology
Eikenella corrodens
- Characteristics: Gram-negative facultative anaerobe.
- Prevalence: Found in 25-30% of human bite infections.
- Synergy: Acts synergistically with Strep viridans to worsen infection.
- Resistance Profile:
- Resistant: Clindamycin, Erythromycin, First Gen Cephalosporins (Cephalexin), Metronidazole (Variable).
- Sensitive: Penicillin, Ampicillin, Augmentin, Ciprofloxacin, Ceftriaxone.
Treating a human bite with Keflex (Cephalexin) is a classic error.
Classification Systems
Injury Types
- Occlusal Bite: Direct clamping. Often finger tip or soft tissue areas. Can cause amputation.
- Clenched Fist Injury (CFI): Indirect inoculation. High risk to joint/tendon.
- Self-Inflicted: Nail biting (Paronychia), psychogenic.
Classification guides urgency. CFI = Urgent Arthrotomy. Occlusal = Debridement.
Depth-Based Staging of the Clenched-Fist Injury
Beyond the injury type (occlusal vs clenched-fist), it is the depth of penetration of a fight bite that drives prognosis and the operation - and it is the basis of the large surgical series quoted in the Evidence Base (Chadaev).
- What is involved
- Skin and fat; extensor tendon and capsule intact
- Implication
- Debride and antibiotics; best prognosis
- What is involved
- Tendon laceration or sagittal-band injury, capsule not breached
- Implication
- Explore; watch for tendon subluxation; repair the tendon at a clean second look
- What is involved
- Capsule breached, organisms seeded into the joint
- Implication
- Formal arthrotomy and washout - the classic fight-bite emergency
- What is involved
- Cartilage divots, metacarpal-head erosion, retained tooth fragment
- Implication
- Worst prognosis; thorough debridement, prolonged antibiotics, sometimes joint-spanning distraction
The practical message from the surgical series is that outcome tracks directly with depth: results are excellent when only skin or tendon are involved and deteriorate sharply once the cartilage or bone is breached - exactly why the joint surface must be visualised at operation and a retained tooth fragment actively hunted for and removed.
The skin wound is tiny at every depth - what matters is how far the tooth went. Capsule breach means septic arthritis (formal arthrotomy); cartilage or bone involvement (often with a retained tooth) carries the worst prognosis and may need distraction and prolonged antibiotics. Always inspect the joint surface intra-operatively, because the depth - not the skin - decides the outcome.
Clinical Presentation
The classic patient is a young adult man presenting hours to days after a fight, with a deceptively small (3-5 mm) laceration over the dorsum of the third, fourth or fifth metacarpophalangeal joint. The history is frequently concealed ("I cut it on a fence").
- Early (first 24 hours): Localised tenderness over the MCPJ, minimal swelling, often no erythema. The wound may already be sealed by gliding of the extensor hood. This benign appearance is the trap.
- Established infection (24-72 hours): Increasing dorsal swelling, erythema, throbbing pain, and the cardinal sign of pain on passive movement of the MCP joint, indicating septic arthritis.
- Late / neglected: Spreading dorsal cellulitis, purulent discharge, fixed flexion from joint destruction, and systemic features. Crepitus or pain out of proportion raises the spectre of necrotising infection.
Always assume a wound overlying the MCPJ in this demographic is a clenched-fist injury with joint penetration until surgical exploration proves otherwise.
History
Screening
- The Story: Often vague ("cut on metal").
- Hand Position: Was the hand a fist?
- Time: Delayed presentation is common (pain increases overnight).
- Tetanus/Vaccination: Status.
Assume any laceration over the MCPJ is a fight bite.
Examination
Examination
- Location: Usually 3rd (Middle) or 4th (Ring) MCPJ (prominent heads).
- Wound: Often small (3-5mm). May be sealed.
- ROM: Pain on passive motion (Septic Arthritis).
- Tendons: Assess extensor mechanism stability (sagittal band injury).
- Neurovascular: Digital nerves.
Look for "gas" or crepitus (rare but ominous - necrotizing fasciitis).
Investigations
Radiology
- X-Ray: Mandatory.
- Findings:
- Fracture: 5th Metacarpal Neck (Boxer's Fracture) - suggests punch mechanism.
- Foreign Body: Tooth fragment (radiopaque).
- Air: Gas in the joint (Pathognomonic for penetration).
- Osteomyelitis: Late finding (periosteal reaction, osteopenia, erosions).
MRI is rarely indicated in the acute setting but useful for chronic osteomyelitis. ULTRASOUND can also be used to guide aspiration of joint effusions if the diagnosis is unclear.
Clinical Presentation


Differential Diagnosis
A small, infected, painful wound over the dorsum of the hand has several mimics. The clinical task is to decide which patients have a joint or deep-space process that mandates theatre versus those who can be managed with antibiotics and observation.
- Distinguishing Features
- Small wound over 3rd-5th MCPJ, young adult, fight history (often concealed), pain on passive MCP motion
- Key Discriminator
- Wound overlies MCPJ; air or tooth fragment on X-ray
- Management Implication
- Emergent formal arthrotomy and washout
- Distinguishing Features
- Diffuse erythema, fluctuance away from joint, no joint-line tenderness, full painless passive ROM
- Key Discriminator
- Joint not penetrated; pain not on passive motion
- Management Implication
- Antibiotics +/- bedside incision and drainage
- Distinguishing Features
- Older patient, prior episodes, no wound, raised urate, monosodium urate crystals on aspirate
- Key Discriminator
- No breach of skin; crystals not organisms
- Management Implication
- NSAIDs/colchicine, not surgery
- Distinguishing Features
- Kanavel signs: fusiform swelling, semiflexed digit, pain on passive EXTENSION, tenderness along flexor sheath (volar)
- Key Discriminator
- Volar not dorsal; flexor sheath not MCPJ
- Management Implication
- Surgical sheath irrigation
- Distinguishing Features
- Vesicles on pulp/digit, healthcare or dental exposure, NO frank pus, viral prodrome
- Key Discriminator
- Vesicular, self-limiting; incision is contraindicated
- Management Implication
- Aciclovir; do NOT incise
- Distinguishing Features
- Pain out of proportion, crepitus, skin necrosis/bullae, systemic toxicity, rapid spread
- Key Discriminator
- Crepitus/gas, systemic sepsis
- Management Implication
- Emergent radical debridement, broad-spectrum IV antibiotics
Pain on passive flexion localised to the volar sheath points to flexor tenosynovitis; pain on passive motion of the MCP joint with a dorsal wound points to a fight-bite septic arthritis. Herpetic whitlow is the one infective mimic you must NOT incise.
Management Strategy
Strategic Approach
- Admit: IV Antibiotics.
- Explore: Surgical exploration is mandatory for CFI.
- Wash: Arthrotomy and irrigation.
- Leave Open: Do not suture.
- Rehab: Early motion once infection controlled.
Early mobilization prevents stiffness and tendon adhesion.
Surgical Considerations
Formal Arthrotomy
- Incision: Extend the laceration (usually transverse or Z-plasty). Avoid longitudinal crossing of joint creases.
- Exposure: Expose the extensor tendon. Retract it to inspect the capsule. A longitudinal split of the tendon (splitting the sagittal fibers) may be needed to visualize the joint surface directly.
- Capsulotomy: If a tear is found, open it. If no tear is found but clinical suspicion is high, open it. The joint MUST be visualized.
- Irrigation: Copious saline (e.g. 3-6 Liters). Use a 18G catheter on a syringe for jet lavage within the joint.
- Staging: Inspect the metacarpal head for "divots" (tooth impact) or cartilage loss.
- Closure: Leave skin open. Loose approximation only if very clean.
A strict "No Closure" policy is safest for the junior surgeon.
Antibiotic Protocol
Augmentin (Amoxicillin + Clavulanate). Why? Covers Staph, Strep, Anaerobes, AND Eikenella.
- Ciprofloxacin (Covers Eikenella) OR
- TMP/SMX (Bactrim)
- PLUS Clindamycin or Metronidazole (for Anaerobes/Staph).
Clindamycin ALONE misses Eikenella. Cephalexin ALONE misses Eikenella.
Tetanus and Rabies Prophylaxis
The topic keeps saying "check tetanus status" - here is the actual algorithm, plus the rabies point examiners like.
Tetanus. A human bite is a tetanus-prone wound (contaminated, often with devitalised tissue and delayed presentation). Action depends on the immunisation history:
- Fully immunised with a booster within the last 10 years: no further tetanus action needed.
- Immunised but the last dose was more than 10 years ago, or the course is incomplete/uncertain: give a tetanus toxoid booster.
- Unimmunised/uncertain, or a heavily contaminated wound in an incompletely immunised patient: give toxoid AND human tetanus immunoglobulin (at a separate site) and complete the vaccination course.
Rabies. This is the high-yield discriminator from animal bites: a human bite does NOT require rabies prophylaxis - humans are not a rabies reservoir host. Rabies post-exposure prophylaxis is the concern for many animal bites (dog, bat), not human bites.
Treat every human bite as a tetanus-prone wound: a booster if the last dose was over 10 years ago, and toxoid plus tetanus immunoglobulin if immunisation is absent or uncertain. Unlike an animal bite, a human bite does not need rabies prophylaxis (humans are not a rabies reservoir). The bloodborne viruses to consider for a human bite are hepatitis B, and - only with visible blood - HIV and hepatitis C.
Complications
Infection-Related Complications
- Risk Factors
- MCP joint penetration, delay
- Prevention
- Early I&D, IV antibiotics
- Management
- Joint washout, may need multiple
- Risk Factors
- Metacarpal head involvement, delay
- Prevention
- Early debridement
- Management
- Prolonged IV antibiotics, debridement
- Risk Factors
- Palmar involvement, immunocompromised
- Prevention
- Aggressive exploration
- Management
- I&D of web space, thenar space
- Risk Factors
- Diabetes, delayed presentation
- Prevention
- High index of suspicion
- Management
- Emergent radical debridement
Structural Complications
- Tendon Rupture: May occur from initial injury or secondary to infection. Extensor tendons most vulnerable at MCP level.
- Extensor Subluxation: Sagittal band disruption allows tendon to sublux between metacarpal heads. May need surgical repair.
- Joint Stiffness: Common after septic arthritis. Early mobilization crucial once infection controlled.
- Contractures: Collateral ligament shortening if immobilized in extension. Splint in intrinsic plus position.
Worst-Case Scenarios
In severely neglected cases with immunocompromise or significant delay:
- Amputation: May be required for uncontrollable infection or extensive tissue loss
- Hand function loss: Permanent grip weakness and finger stiffness
- Systemic sepsis: Life-threatening if infection spreads
Rehabilitation
- Splinting: Volar splint in intrinsic plus (MCPs flexed 70, IPs extended) to prevent collateral ligament shortening.
- Elevation: High elevation in a Bradford sling to reduce edema.
- Dressings: Saline soaked gauze to encourage wicking of purulence.
- Motion: Start Active Range of Motion (AROM) as soon as cellulitis resolves and the wound is clean.
- Tendon: Isolate Extensor Digitorum Communis (EDC) gliding exercises.
- Wound: Secondary intention healing (granulation).
- Scar Management: Desensitization once healed.
- Strengthening: Grip strengthening once soft tissue coverage is complete.
Prognosis
Outcomes by Presentation Time
- Infection Rate
- 10%
- Joint Outcome
- Good if no joint penetration
- Overall Prognosis
- Excellent with appropriate treatment
- Infection Rate
- 30-40%
- Joint Outcome
- Moderate risk of stiffness
- Overall Prognosis
- Fair with aggressive management
- Infection Rate
- 50%+
- Joint Outcome
- High risk of permanent damage
- Overall Prognosis
- Guarded, multiple surgeries likely
Injury Pattern and Prognosis
- Simple bite wound: Good prognosis with early antibiotics
- Clinched fist injury (CFI): Worse prognosis due to joint penetration and contamination
- Joint involvement: Even with treatment, 20-30% develop some permanent stiffness
Factors Predicting Poor Outcome
Negative prognostic factors include:
- Delay in presentation: Greater than 24 hours significantly worsens outcomes
- MCP joint penetration: Risk of septic arthritis and cartilage destruction
- Eikenella corrodens: Often resistant to empiric therapy, may be missed
- Patient comorbidities: Diabetes, immunosuppression, alcoholism
- Incomplete debridement: Retained contamination leads to persistent infection
Long-Term Functional Outcomes
Most patients treated appropriately within 24 hours return to full hand function. Those presenting late or with joint involvement may experience:
- Reduced grip strength (20-40%)
- Limited MCP range of motion
- Cold intolerance
- Persistent pain
Guidelines, Registries & Global Practice
Global Epidemiology
Human bites are the third most common mammalian bite presenting to emergency departments worldwide, after dog and cat bites. They cluster in young adult males, often around interpersonal violence and alcohol, with most injuries to the hand. In the Talan multicentre series, 70% of those involved were young adult men and 56% of injuries were clenched-fist injuries. Under-reporting is common because patients conceal an assault mechanism; delayed presentation (beyond 24 hours) is consistently associated with higher complication rates across published series from Europe, North America, Africa and Asia.
Guidelines Side by Side
- Antibiotic of Choice
- Amoxicillin-clavulanate; ampicillin-sulbactam IV
- Wound Closure (Hand)
- Leave open; arthrotomy for CFI
- Notable Stance
- Fight bite over MCPJ treated as septic arthritis
- Antibiotic of Choice
- Co-amoxiclav; clindamycin + ciprofloxacin if penicillin-allergic
- Wound Closure (Hand)
- Open; debride in theatre
- Notable Stance
- Low threshold for surgical exploration of dorsal MCPJ wounds
- Antibiotic of Choice
- Amoxicillin-clavulanate first-line
- Wound Closure (Hand)
- Open for hand/high-risk; closure acceptable for selected facial wounds
- Notable Stance
- Routine prophylaxis advised for human and hand bites
- Antibiotic of Choice
- Cover Eikenella, Strep, Staph, anaerobes
- Wound Closure (Hand)
- Open, delayed closure
- Notable Stance
- Treat associated metacarpal fracture as open/contaminated
The consistent global message: amoxicillin-clavulanate is first-line, cephalexin and clindamycin monotherapy are inadequate, hand bites are left open, and a wound overlying the MCP joint mandates surgical exploration.
Evidence and Registry Notes
There is no implant registry for bite injuries, but the evidence base is anchored by a Cochrane systematic review (Medeiros and Saconato) confirming antibiotic prophylaxis reduces infection after human and hand bites, the Talan microbiology series defining the organisms, and surgical series (Chadaev) showing outcome tracks with depth of joint and bone involvement.
Bloodborne Virus Assessment (Global Principle)
- Hepatitis B: Assess immunisation status of the person bitten; offer vaccination or immunoglobulin where indicated, as HBV can transmit via mucosal or non-intact-skin exposure.
- HIV / Hepatitis C: Transmission requires visible-blood exposure and is negligible from ordinary (blood-free) saliva; reserve testing and post-exposure prophylaxis discussion for bloody-saliva exposures.
- Consent and follow-up: Source and recipient testing requires informed consent; baseline and repeat serology where risk is identified.
High-Resource vs Limited-Resource Practice
- High-resource: 24-hour theatre access, formal arthrotomy under regional/general anaesthesia, IV co-amoxiclav, hand-therapy-led rehabilitation, and structured bloodborne-virus pathways.
- Limited-resource: Emphasis on meticulous bedside debridement and irrigation, oral amoxicillin-clavulanate (oral shown equivalent to IV for uncomplicated early bites in the Zubowicz trial), early referral of any joint-penetrating injury, and tetanus cover, which remains a priority where immunisation coverage is incomplete.
Documentation and Prevention
These injuries carry medicolegal weight: record the time and mechanism, clinical findings (with photographs where consented), treatment given, and the prognosis discussed. Prevention centres on reducing alcohol-related violence and on public awareness that a punch to the mouth is a high-risk inoculation injury, not a trivial graze.
Controversies and Areas of Uncertainty
Much of the surgical dogma for fight bites rests on small retrospective series and a single randomised trial that deliberately excluded joint and tendon injuries. The high-yield exam answers are well established, but several practical questions remain genuinely debated.
- Routine arthrotomy vs selective exploration. Some authors advocate formal arthrotomy for every wound overlying the MCP joint; others reserve it for cases with proven capsular breach, air on imaging, established septic arthritis, or failure of antibiotics. The safe exam position remains: if the joint may be involved, explore it.
- Antibiotic duration. Prophylaxis after a clean early bite (commonly 3-5 days) is distinct from treatment of established septic arthritis or osteomyelitis (often weeks, IV then oral). No high-quality trial defines the optimal duration for the established-infection group.
- Imaging in the clean wound. Plain radiographs are universally recommended to exclude fracture, tooth fragment and intra-articular air. The role of early MRI or ultrasound in the equivocal, apparently clean wound is undefined and rarely changes acute management.
- Negative-pressure wound therapy and distraction fixation. Case reports and small series describe NPWT and joint-spanning distraction for severe established infection, but these are adjuncts, not first-line, and lack comparative evidence.
- Bloodborne-virus testing thresholds. Whether to test asymptomatic recipients of blood-free bites is contested; current synthesis favours universal hepatitis B follow-up but selective HIV/HCV testing based on visible-blood exposure.
MCQ Practice Points
Q: Which bacteria is characteristically resistant to Clindamycin and Cephalexin in human bites? A: Eikenella corrodens.
Q: In a Clenched Fist Injury, the bacterial inoculum is trapped because: A: The extensor tendon glides proximally upon finger extension, sealing the tract.
Q: What is the first-line oral antibiotic for a human bite? A: Amoxicillin + Clavulanate (Augmentin).
Q: What is a 'Honeymoon Period' in flexor tenosynovitis? A: The period (12-24h) where the bacteria are proliferating but signs are subtle, before rapid escalation.
Q: What is the mandatory surgical approach for a confirmed clenched fist injury? A: Formal arthrotomy with copious irrigation (3-6L saline) and the wound left open.
Q: What complication should you suspect if a fight bite patient presents with crepitus? A: Necrotizing fasciitis - requires emergent radical debridement.
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 24-year-old male presents with a 4mm laceration over his right long finger MCPJ. He says he cut it on a tooth during a fight 2 days ago. It is red, swollen, and he cannot extend the finger due to pain. He has been taking Keflex from his GP.”
“X-ray shows a Boxer's fracture (5th MC Neck) with volar angulation. On clinical exam, there is a small scab over the 5th MCPJ. Patient denies a bite.”
“Why is Eikenella corrodens significant in human bites? What is its unique resistance profile?”
“A 40-year-old carer presents 6 hours after being bitten on the dorsum of the hand by a patient with intellectual disability. The skin is broken but there is no erythema, no swelling, the joint is not involved and passive movement is painless. She asks whether she really needs treatment for 'such a tiny bite'.”
Diagnosis
- Small wound over MCPJ = Fight Bite
- Boxer's Fracture + Wound = Open/Infected
- Pain on passive ROM = Septic Arthritis
- X-ray: Look for Air and Tooth
Microbiology
- Polymicrobial
- Eikenella corrodens (Gram Neg Anaerobe)
- Strep viridans
- Staph aureus
Management
- Admit + IV Augmentin
- Formal Arthrotomy + Washout
- Leaves Wounds Open
- Splint in Intrinsic Plus
Evidence Base
Microbiology of Infected Human Bites (Landmark)
- Multicentre prospective study of 50 patients with infected human bites; 56% were clenched-fist injuries, 44% occlusal
- Median 4 isolates per wound (3 aerobes, 1 anaerobe); polymicrobial in the majority
- Key isolates: Streptococcus anginosus 52%, Staphylococcus aureus 30%, Eikenella corrodens 30%, Fusobacterium nucleatum 32%, Prevotella melaninogenica 22%
- Amoxicillin-clavulanate and moxifloxacin showed excellent in-vitro activity against common isolates
Antibiotic Prophylaxis for Mammalian Bites (Cochrane)
- Systematic review of 8 randomised controlled trials of prophylactic antibiotics after mammalian bites
- Prophylactic antibiotics significantly reduced infection after human bites (unlike cat or dog bites)
- For bites of the hand, prophylaxis reduced infection (OR 0.10, 95% CI 0.01 to 0.86; NNT = 4)
Antibiotic Prophylaxis in Early Hand Bites (RCT)
- Prospective randomised trial of 48 patients with early (under 24h) hand bites without joint or tendon involvement
- Placebo (mechanical wound care alone): 7 of 15 (46.7%) became infected
- Oral and parenteral antibiotic groups: zero infections
- Oral antibiotics were equivalent to intravenous for prophylaxis of uncomplicated early bites