Comprehensive Ankle and Foot Assessment
- Mortise view: 15-20° internal rotation shows ankle mortise without overlap. Assesses syndesmosis.
- Ottawa Rules: Clinical decision rule for ankle/foot X-ray - reduces unnecessary imaging.
- Bohler angle: 20-40° normal. Less than 20° suggests calcaneal fracture with posterior facet depression.
- Lisfranc alignment: On AP WB, medial border of 2nd MT aligns with medial border of middle cuneiform.
- OCD stability on MRI: Fluid signal around fragment indicates instability.
- “Tibiofibular clear space greater than 6mm on mortise = syndesmosis injury.
- “Weight-bearing views increase Lisfranc injury detection sensitivity significantly.
- “Gissane angle (crucial angle) 120-145° - flattening suggests calcaneal fracture.
- “Medial malleolus fracture alone is rare - look for associated lateral injury.
- “Maisonneuve fracture: Proximal fibula fracture with medial ankle injury - high syndesmosis injury.
Non-weight-bearing X-rays frequently miss Lisfranc injuries. Always request weight-bearing AP, lateral, and oblique views when Lisfranc injury is suspected. If the patient cannot weight-bear, CT may be needed. Compare to the contralateral foot if in doubt.
Overview & Imaging Principles
The ankle and foot are among the most frequently imaged regions in orthopaedic and emergency practice. Effective interpretation depends less on technology and more on a disciplined search pattern, knowledge of normal measurements, and selecting the right modality for the clinical question. Plain radiography remains the universal first-line investigation worldwide because it is cheap, fast, low-dose and available in every resource setting. CT and MRI are problem-solving tools layered on top.
- Subtle injuries (Lisfranc, Maisonneuve, talar dome lesions) are the commonest medico-legal misses
- A fixed search pattern (ABCS) defeats "satisfaction of search" after the first obvious finding
- Measurements convert subjective impressions into reproducible decisions (operate vs not)
- Always correlate with the clinical question and point of maximal tenderness
- Radiograph: bone, alignment, gross arthritis - always first
- Weight-bearing radiograph: unmasks dynamic instability (Lisfranc, syndesmosis, flatfoot)
- CT: bone architecture, articular comminution, occult/complex fractures, coalition
- MRI: cartilage, marrow, ligament, tendon, occult stress fracture, infection/tumour
- Ultrasound: dynamic soft-tissue (tendon, fascia), guided injection, no ionising radiation
Imaging never replaces examination. The Ottawa Ankle Rules formalise this: radiographs are only indicated with malleolar/midfoot pain PLUS bone tenderness at specified points OR inability to bear weight for four steps. Applied correctly they are close to 100% sensitive for clinically significant fracture and reduce radiography by roughly a third (Stiell, JAMA 1993).
Ankle Radiograph Interpretation
Standard Views
- Technique
- Beam perpendicular to ankle
- Key Assessment
- Distal tibial plafond, medial malleolus
- Technique
- 15-20° internal rotation
- Key Assessment
- Syndesmosis, talar dome, mortise congruity
- Technique
- True lateral
- Key Assessment
- Anterior/posterior malleoli, talus, calcaneus
- Technique
- Forced inversion/eversion/ER
- Key Assessment
- Ligamentous instability (when indicated)
Radiograph Examples


Key Measurements
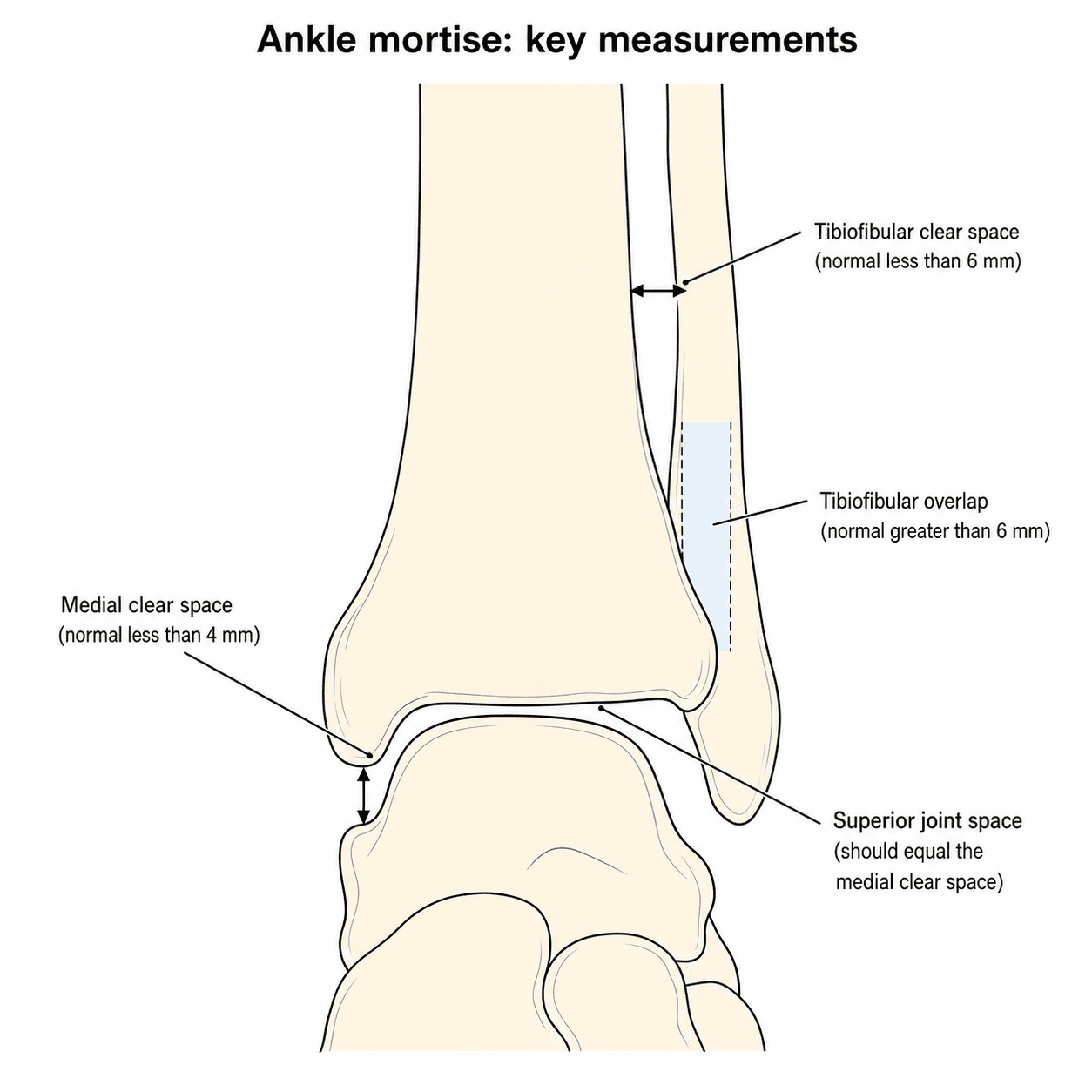
Medial Clear Space: Less than 4mm (talar tilt suggests deltoid injury)
Tibiofibular Clear Space: Less than 6mm (syndesmosis)
Tibiofibular Overlap: Greater than 6mm on AP, greater than 1mm on mortise
Talar Tilt: Asymmetric joint space suggests instability
Anterior talofibular distance: Joint effusion sign
Bohler angle: 20-40° (calcaneus)
Gissane angle (crucial): 120-145° (calcaneus)
Talar dome: Osteochondral lesions
Ankle Fracture Classification
Based on fibular fracture level relative to syndesmosis:
Type A: Below syndesmosis
- Syndesmosis intact
- Stable injury usually
Type B: At level of syndesmosis
- Syndesmosis may be injured
- Assess mortise for widening
Type C: Above syndesmosis
- Syndesmosis disrupted
- Unstable, often requires fixation
Key: Always assess medial side and syndesmosis
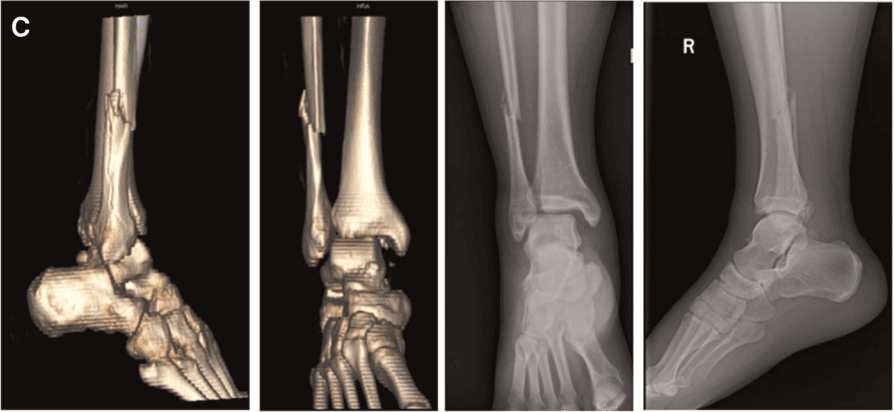
CT of Ankle and Foot
Indications
- Calcaneal fractures (Sanders classification)
- Pilon fractures
- Talus fractures
- Lisfranc injury (if WB X-rays equivocal)
- Tarsal coalitions
- Complex midfoot fractures
- Superior bone detail
- 3D reconstruction for surgical planning
- Fragment size and displacement
- Articular surface assessment
- Subtalar joint involvement
Sanders Classification (Calcaneal Fractures)
- Fracture Lines
- Non-displaced (less than 2mm)
- Prognosis
- Good, non-operative
- Fracture Lines
- 2 fragments (1 fracture line)
- Prognosis
- Fair, operative if displaced
- Fracture Lines
- 3 fragments (2 fracture lines)
- Prognosis
- Guarded, operative
- Fracture Lines
- 4+ fragments (highly comminuted)
- Prognosis
- Poor, may need fusion
Talar Neck Fracture: Hawkins Classification and the Hawkins Sign
The talus is listed above as a CT indication; the Hawkins classification of talar neck fractures and the Hawkins sign are the high-yield imaging points, because the talus is at high risk of avascular necrosis (AVN) from its retrograde, largely intra-osseous blood supply.
- Displacement
- Non-displaced
- Approximate AVN risk
- Low (around 0-15%)
- Displacement
- Displaced with subtalar (talocalcaneal) subluxation/dislocation
- Approximate AVN risk
- Intermediate (around 20-50%)
- Displacement
- Displaced with subtalar AND tibiotalar (ankle) dislocation
- Approximate AVN risk
- High (around 50-90%)
- Displacement
- Type III plus talonavicular dislocation/subluxation
- Approximate AVN risk
- Highest (approaching 100%)
The Hawkins sign (the high-yield positive prognostic sign):
- A subchondral lucency (radiolucent band) in the talar dome on an AP/mortise ankle radiograph at about 6-8 weeks.
- It reflects subchondral osteopenia from disuse hyperaemia in a talus with intact blood supply - so a present Hawkins sign predicts a viable talus (AVN unlikely).
- Its absence (a persistently sclerotic/dense dome) is concerning for AVN, although MRI is the definitive test for established osteonecrosis.
The Hawkins sign - a subchondral lucent band in the talar dome at 6-8 weeks - means the talus is vascularised and AVN is unlikely (a present sign is reassuring). Its absence, or a dense sclerotic dome, suggests AVN. Grade the fracture by the Hawkins classification (I non-displaced through IV with talonavicular dislocation); AVN risk climbs steeply with each grade.
MRI of Ankle and Foot
Sequences
- Best For
- Anatomy, marrow, OCD
- Key Findings
- Low signal = marrow replacement
- Best For
- Edema, fluid, ligaments
- Key Findings
- Bone bruise, soft tissue injury
- Best For
- Tendons, ligaments, cartilage
- Key Findings
- Tendon tears, ligament injury
- Best For
- Cartilage, OCD
- Key Findings
- Cartilage detail, fragment stability
Osteochondral Lesions of Talus (OLT)
Posteromedial talar dome: Most common (inversion injury)
Anterolateral talar dome: Second most common
Location affects approach:
- Medial lesions: Medial malleolar osteotomy may be needed
- Lateral lesions: Often accessible arthroscopically
Tendon Assessment
- Location
- Posterior, superficial
- Common Pathology
- Tendinopathy, rupture (2-6cm from insertion)
- Location
- Posteromedial
- Common Pathology
- Tendinopathy, tears (acquired flatfoot)
- Location
- Posterolateral
- Common Pathology
- Tears, split peroneus brevis, subluxation
- Location
- Anterior
- Common Pathology
- Rupture (drop foot)
Normal: Low signal, approximately 6mm thick
Tendinopathy:
- Thickening (greater than 8mm)
- Increased signal (T2)
- Fusiform swelling
- Intact fibers
Rupture:
- Complete discontinuity
- Gap filled with fluid/hemorrhage (T2 bright)
- Retraction of tendon ends
- Most common 2-6cm from insertion
Plantar Fascia
Normal: Less than 4mm thick at calcaneal insertion, low signal
Plantar fasciitis:
- Thickening greater than 4mm
- Increased T2/STIR signal
- Periplantar edema
- May have calcaneal marrow edema at insertion
Rupture:
- Discontinuity
- Surrounding fluid/hemorrhage
- Associated with prior steroid injection or fluoroquinolone use
Staging Osteochondral Lesions of the Talus
The OLT section above describes location and stability; examiners also want the staging systems, and the topic's own evidence (Orr) is reported in Hepple stages that should be defined.
- Stages
- I subchondral compression; II partially detached fragment; III completely detached but undisplaced (in situ); IV displaced loose fragment
- Concept
- The classic radiographic staging of progressive detachment
- Stages
- I cartilage only; IIa subchondral fracture with oedema, IIb without oedema; III detached but undisplaced; IV displaced; V subchondral cyst
- Concept
- Adds marrow/cartilage detail and the subchondral-cyst stage
- Stages
- I intact roof with cyst; II cyst communicating with the surface; III non-displaced fragment with lucency; IV displaced fragment
- Concept
- CT-based, emphasising cyst-surface communication and fragment position
The practical link to the stability assessment above: the higher stages - a detached or displaced fragment (Berndt-Harty III-IV) or a subchondral cyst (Hepple V) - correspond to the instability signs (surrounding fluid, a fluid cleft, a cyst beneath the lesion) that push management toward surgery.
Stage an OLT by modality: Berndt-Harty (radiograph) I-IV from subchondral compression to a displaced loose body; Hepple (MRI) I-V adding the subchondral cyst (stage V); Ferkel (CT) emphasising cyst-surface communication. All describe the same progression from intact cartilage to a detached, displaced or cystic lesion - and the higher stages are the unstable, surgical ones.
Systematic Approach: Interpretation Framework
A reproducible interpretation framework is what separates a consultant-level review from a checklist of "looks normal". Pair a fixed search pattern (ABCS) with a modality-decision mnemonic so the right next test is requested rather than reflexively ordering CT or MRI.
X-FRACTUREChoosing the Right Foot/Ankle Modality
Hook:X-ray first, then problem-solve up the modality ladder
1. Confirm: correct patient, side, projection adequacy, weight-bearing status.
2. Alignment: mortise congruity, talar shift/tilt, syndesmosis, Lisfranc and Chopart lines, hindfoot axis.
3. Bone: trace every cortex - malleoli, plafond, talus, calcaneus, navicular, cuboid, cuneiforms, all five metatarsals and bases (especially 2nd and 5th).
4. Cartilage/joints: tibiotalar, subtalar, talonavicular, calcaneocuboid, TMT joint spaces; osteophytes; erosions.
5. Soft tissue: effusion, focal swelling, Achilles contour, Kager fat pad, calcification/foreign body.
6. Measure: medial clear space, tibiofibular clear space/overlap, Bohler and Gissane angles, Meary angle for arch.
7. Decide next test using the X-FRACTURE ladder, not reflex.
ABCSAnkle X-ray Systematic Review
Hook:Always Be Checking Systematically
Differential Diagnosis & Imaging Pitfalls
Many ankle/foot complaints share overlapping radiographic features. The table below structures the high-yield differentials and the imaging discriminator that resolves each.
- Key Differentials
- ATFL tear vs fibular avulsion vs OLT vs peroneal tear
- Discriminating Imaging Finding
- Mortise X-ray for avulsion/talar dome; MRI for ligament/cartilage and bone bruise pattern
- Key Differentials
- Tibialis posterior dysfunction vs deltoid injury vs medial OLT
- Discriminating Imaging Finding
- MRI: tendon signal/thickening and flatfoot alignment vs marrow oedema of talar dome
- Key Differentials
- Lisfranc injury vs cuboid/navicular stress fracture vs midfoot OA
- Discriminating Imaging Finding
- Weight-bearing AP/oblique then CT/MRI; fleck sign and C1-M2 diastasis point to Lisfranc
- Key Differentials
- Calcaneal fracture vs talar fracture vs lumbar burst (associated)
- Discriminating Imaging Finding
- Lateral X-ray Bohler angle then CT Sanders; screen spine given axial-load mechanism
- Key Differentials
- Plantar fasciitis vs calcaneal stress fracture vs Baxter nerve entrapment
- Discriminating Imaging Finding
- MRI/US: fascia thickening over 4mm vs calcaneal marrow oedema/fracture line
Maisonneuve injury: a medial malleolar fracture or deltoid widening with a "normal" ankle fibula should prompt dedicated proximal fibula views - the fracture is at the fibular neck. A flake of bone at the 2nd metatarsal base (fleck sign) is a Lisfranc injury until proven otherwise. An os trigonum, accessory navicular and bipartite sesamoid are normal variants that mimic fractures - look for corticated margins.
Guidelines, Registries & Global Practice
Global Epidemiology
- Ankle sprains are among the most common musculoskeletal injuries globally, with lateral ligament sprains predominating
- Ankle fractures are a high-incidence fracture in adults, rising with an ageing, osteoporotic population
- Calcaneal fractures account for the majority of tarsal fractures and typically follow axial load (fall from height, road trauma)
- Lisfranc injuries are frequently missed at first presentation, a recognised source of long-term disability and litigation
- Plain radiography dominates first-line imaging in every health system
- Decision rules (Ottawa) reduce unnecessary radiographs by roughly a third where implemented
- MRI and CT access varies widely between high- and limited-resource settings, shaping pathways
Side-by-Side Guideline Comparison
- First-Line
- Radiograph for acute trauma; apply Ottawa Rules
- Advanced Imaging Stance
- MRI for chronic pain, OLT, tendon/ligament, occult fracture; CT for complex bone injury
- First-Line
- Radiograph guided by clinical assessment
- Advanced Imaging Stance
- Targeted CT for complex intra-articular fractures; MRI for soft-tissue/occult injury; emphasis on avoiding unnecessary imaging
- First-Line
- Radiograph + classification (Weber/AO, Sanders)
- Advanced Imaging Stance
- CT routine for pilon, calcaneal, talar and complex midfoot fractures to plan reduction and fixation
- First-Line
- Radiograph first; standardised measurements
- Advanced Imaging Stance
- Growing role for weight-bearing CT in instability and deformity assessment
High- vs Limited-Resource Practice Variation
High-resource settings: ready access to CT and MRI lowers the threshold for advanced imaging; weight-bearing CT and standardised reporting are expanding; sub-specialty musculoskeletal radiology input is common.
Limited-resource settings: plain radiography (often with bilateral comparison and stress/weight-bearing views) carries most diagnostic load; clinical decision rules are especially valuable to ration scarce imaging; ultrasound is a cost-effective, radiation-free tool for tendon and fascia pathology where MRI is unavailable.
Universal principle: the imaging pathway should answer a specific clinical question and change management - not generate findings of uncertain significance. This holds regardless of resource level.
Key Exam Points & Practice Pearls
- Medial clear space less than 4mm; tibiofibular clear space less than 6mm
- Tibiofibular overlap over 6mm (AP), over 1mm (mortise)
- Bohler angle 20-40 degrees; Gissane angle 120-145 degrees
- Normal Achilles under 6mm; plantar fascia under 4mm at insertion
- Greater than 2mm diastasis between 1st and 2nd metatarsal bases is abnormal
- "Normal" film with clinical suspicion: request weight-bearing/contralateral views
- High fibular fracture: exclude Maisonneuve and syndesmotic injury
- Fall from height with heel pain: CT for Sanders type and screen the spine
- Lateral talar dome lesion on mortise view: proceed to MRI for stability
- Always state the modality you would request next and why
Controversies & Areas of Uncertainty
The classic teaching of posteromedial and anterolateral talar dome lesions has been questioned. Using a nine-zone MRI grid, operatively treated symptomatic lesions were most often central (central-lateral then central-medial), with medial lesions larger in surface area (Orr, Foot Ankle Int 2012). Describe lesions by zone and size rather than the historical two-location model.
Static radiographic measurements (clear space, overlap) miss occult instability, and the fibular incisura is highly variable in shape and depth, so absolute numbers can mislead. Bilateral or post-fixation CT is increasingly used to detect malreduction, with the uninjured side as the reference (Liu, J Foot Ankle Surg 2018). Intra-operative dynamic stress and weight-bearing CT remain active research areas.
Cone-beam WBCT provides 3D imaging under physiological load and is gaining traction for subtle Lisfranc and syndesmotic instability, hindfoot alignment and arthritis - but availability is limited and validated thresholds are still maturing.
MRI is the non-invasive standard for staging stability, but it can over- or under-estimate cartilage status versus arthroscopy. CT arthrography or diagnostic arthroscopy may be needed when MRI and symptoms disagree.
Clinical Imaging: Foot, Calcaneus & Lisfranc
Standard Views
- Assessment
- Forefoot, tarsometatarsal joints
- Key Findings
- Lisfranc alignment, MT fractures
- Assessment
- Cuboid, lateral cuneiforms, 4th/5th MT bases
- Key Findings
- Calcaneocuboid, lateral Lisfranc
- Assessment
- Arches, calcaneus, talus
- Key Findings
- Flatfoot, coalitions, Bohler angle
- Assessment
- Sesamoids under 1st MT head
- Key Findings
- Sesamoid fracture, position
Lisfranc Injury Assessment
Weight-bearing AP view critical:
Normal alignment:
- Medial border 2nd MT aligns with medial border middle cuneiform
- Medial border 4th MT aligns with medial border cuboid
Subtle signs of injury:
- Fleck sign: Avulsion at 2nd MT base
- Widening between 1st and 2nd MT bases (greater than 2mm)
- Loss of alignment on any view
- Subtle dorsal subluxation on lateral
If WB not possible: CT or MRI to assess
Calcaneal Fracture Assessment
Lateral view key measurements:
Bohler angle: 20-40° normal
- Formed by lines from anterior process to posterior facet to posterior tuberosity
- Less than 20° suggests posterior facet depression
Gissane angle (Crucial angle): 120-145°
- Angle of posterior facet and calcaneal body
- Altered with intra-articular fractures
CT essential for:
- Classification (Sanders)
- Posterior facet involvement
- Surgical planning
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“How do you assess ankle stability on plain radiographs, and what measurements indicate syndesmotic injury?”
“A patient has midfoot pain after a fall. X-rays are 'normal'. What imaging findings would suggest a Lisfranc injury, and what further imaging would you request?”
“Describe the MRI assessment of an osteochondral lesion of the talus and how you determine if it is stable or unstable.”
Key Ankle Measurements
- Medial clear space: Less than 4mm
- Tibiofibular clear space: Less than 6mm
- Tibiofibular overlap: Greater than 6mm (AP), greater than 1mm (mortise)
- Weber C = above syndesmosis = unstable
Calcaneal Fracture
- Bohler angle: 20-40° (less than 20° = depression)
- Gissane angle: 120-145°
- Sanders classification on CT (I-IV)
- Type IV = comminuted = poor prognosis
Lisfranc Injury
- WEIGHT-BEARING views essential
- 2nd MT medial border = middle cuneiform medial border
- Fleck sign = avulsion at 2nd MT base
- Greater than 2mm between 1st and 2nd MT = abnormal
OLT Stability (MRI)
- Unstable: Fluid around fragment, cysts, displacement
- Stable: No fluid, low signal rim, in situ
- Posteromedial location most common
- Cartilage integrity affects prognosis
Evidence Base & Landmark Literature
Ottawa Ankle Rules - Refinement & Prospective Validation
- 1485 adults studied across validation and refinement stages
- Refined rules 100% sensitive for malleolar and midfoot fractures
- Potential 30-34% reduction in radiographs ordered
- Near-zero fracture probability when the rule is negative
ACR Appropriateness Criteria - Acute Trauma to the Ankle / Chronic Ankle Pain
- Radiographs are the appropriate initial study for acute ankle trauma, guided by the Ottawa Rules
- MRI without contrast usually appropriate for chronic pain, osteochondral lesion, tendon/ligament injury and occult fracture
- CT preferred for complex or occult bony injury and surgical planning