From Alignment Assessment to MRI Cord Evaluation
Radiography: Screening tool, alignment assessment, degenerative changes
CT: Gold standard for fracture characterisation, canal compromise, 3D reconstruction
MRI: Gold standard for soft tissue pathology — disc, cord, infection, tumour, ligaments
CT Myelography: Alternative to MRI when contraindicated — shows cord compression
Bone Scan/SPECT-CT: Facet joint disease, spondylolysis activity, metastatic screening
Key: Radiographs screen, CT characterises fractures, MRI evaluates soft tissues and cord
- Systematic spine radiograph reading follows ABCD: Alignment (3 smooth lines), Bones (vertebral body height/shape), Cartilage/Disc (disc space height), Soft tissues (prevertebral swelling).
- MRI is the gold standard for disc herniation, cord compression, cauda equina syndrome, infection, and tumour assessment.
- CT is the gold standard for fracture characterisation — it reveals fracture lines, posterior column involvement, and canal compromise that radiographs miss.
- Cervical spine clearance: NEXUS criteria or Canadian C-Spine Rule determine the need for imaging after trauma.
- Red flags requiring urgent MRI: cauda equina symptoms, progressive neurological deficit, suspected cord compression, suspected spinal infection, suspected metastatic disease.
- “Prevertebral soft tissue swelling on lateral cervical radiograph: more than 7mm at C2 or more than 21mm at C6 = significant (suspect fracture/haematoma/abscess).
- “Jefferson fracture (C1 burst): lateral mass overhang of more than 7mm (combined bilateral) on AP open-mouth view = transverse ligament disruption (unstable).
- “Hangman fracture (C2 pars): bilateral C2 pedicle fracture — paradoxically often STABLE because the canal enlarges (spinal cord spared).
- “TLICS score guides management: less than 4 = conservative, 4 = borderline, more than 4 = surgical. Components: morphology + posterior ligamentous complex + neurological status.
- “On MRI: loss of T2 high signal in the spinal cord (cord signal change) indicates myelopathy — this is an ominous finding suggesting compressive myelopathy.
Spine imaging is tested extensively across all examination formats. You must know: ABCD systematic radiograph reading, the three alignment lines on lateral view, cervical spine clearance rules (NEXUS/CCR), prevertebral soft tissue thresholds, MRI interpretation for disc herniation and cord signal change, CT characterisation of fractures, TLICS scoring, and red flags requiring urgent MRI (CES, myelopathy, infection, metastases). Classic traps: missing C7-T1 junction injury on lateral radiograph and not recognising cord signal change on MRI.
Overview
Systematic spine imaging is fundamental to orthopaedic practice, encompassing acute trauma (fracture/dislocation), degenerative disease (disc herniation, stenosis), infection (discitis/osteomyelitis), and neoplastic conditions (metastases, primary tumours). The imaging approach follows a logical hierarchy: radiographs for screening and alignment, CT for fracture characterisation, and MRI for soft tissue and cord assessment.
Trauma: (1) Apply NEXUS or CCR to determine need for imaging. (2) If imaging needed: CT is now the primary modality for cervical spine clearance in major trauma (replacing radiographs). (3) If neurological deficit: add MRI for cord, disc, and ligament assessment. Degenerative: radiographs for alignment and deformity, MRI for disc/canal/foraminal assessment if surgical decision-making required. Red flags: urgent MRI for CES, myelopathy, infection, or metastatic disease. Deformity: full-length standing radiographs (scoliosis series) for coronal and sagittal balance.
Cervical lateral radiograph must show C7-T1 junction — failure to visualise this level is the most common cause of missed cervical fractures. If C7-T1 is not visible on lateral radiograph, a swimmer's view or CT is required. On MRI: T2 signal change WITHIN the spinal cord (high signal replacing normal cord) indicates myelopathy — this is an ominous finding that often represents irreversible damage and is a stronger predictor of surgical outcome than the degree of anatomical compression alone.
Systematic Approach
Systematic Spine Imaging Assessment
- First-Line Imaging
- CT (primary modality in major trauma). NEXUS/CCR for clinical clearance
- Advanced Imaging
- MRI if neurological deficit, cord compression suspected, or ligamentous injury assessment
- First-Line Imaging
- AP + lateral radiographs. CT for any suspected fracture
- Advanced Imaging
- CT for TLICS scoring (morphology, posterior ligament complex). MRI for cord/conus assessment and posterior ligament integrity
- First-Line Imaging
- Radiographs (usually normal or degenerative)
- Advanced Imaging
- MRI: gold standard for disc morphology, nerve root compression, canal stenosis. CT myelography if MRI contraindicated
- First-Line Imaging
- Radiographs (disc space narrowing, endplate irregularity — often delayed)
- Advanced Imaging
- MRI with contrast: gold standard. Shows disc signal change, endplate destruction, paraspinal/epidural abscess. Blood cultures + CRP/ESR
- First-Line Imaging
- Radiographs (may show lytic/blastic lesions, pedicle destruction)
- Advanced Imaging
- Whole-spine MRI: gold standard for metastatic screening. STIR sequence detects marrow infiltration. CT for stability assessment
- First-Line Imaging
- Do NOT delay for radiographs
- Advanced Imaging
- URGENT MRI (within hours): sagittal and axial T2 for compression identification. This is a surgical emergency
ABCDSystematic Spine Radiograph Reading
Hook:ABCD: the systematic approach for spine radiographs — Alignment, Bones, Cartilage/Discs, Dens/Soft tissues.
Differential Diagnosis
Imaging-Based Differential Diagnosis
Two patterns recur in exams: distinguishing the cause of vertebral collapse, and distinguishing the cause of an aggressive disc-level signal change. The MRI features below separate the look-alikes.
- Osteoporotic Fracture
- Band-like oedema, preserved marrow elsewhere; reconstitutes over weeks
- Metastatic / Myeloma
- Complete/convex marrow replacement, often multifocal, pedicle involvement (winking owl)
- Infection (Discitis-Osteomyelitis)
- Confluent endplate signal crossing the disc space
- Osteoporotic Fracture
- Preserved
- Metastatic / Myeloma
- Typically preserved (tumour spares the disc)
- Infection (Discitis-Osteomyelitis)
- Destroyed early — disc is the epicentre
- Osteoporotic Fracture
- Retropulsed but concave fragment
- Metastatic / Myeloma
- Convex posterior bulge, epidural soft-tissue mass
- Infection (Discitis-Osteomyelitis)
- Epidural phlegmon/abscess, paraspinal collection
- Osteoporotic Fracture
- Minimal/linear
- Metastatic / Myeloma
- Solid enhancing soft tissue
- Infection (Discitis-Osteomyelitis)
- Rim-enhancing abscess, marked endplate enhancement
- Osteoporotic Fracture
- Older, low-energy, osteoporosis
- Metastatic / Myeloma
- Known primary, night pain, weight loss
- Infection (Discitis-Osteomyelitis)
- Fever, raised CRP/ESR, IVDU/bacteraemia
Metastatic Spine: Bilsky ESCC Grade and SINS
Grading Metastatic Spinal Disease: Bilsky and SINS
Once metastatic disease is identified, two scores translate the images into a management decision and are favourite viva probes: the Bilsky epidural spinal cord compression (ESCC) grade (how much cord compression?) and the Spinal Instability Neoplastic Score (SINS) (how unstable?). They are complementary - one drives decompression, the other drives stabilisation.
- Axial T2 appearance
- Bone-only disease; no epidural extension
- Axial T2 appearance
- Epidural impingement, thecal sac indentation but no deformation
- Axial T2 appearance
- Thecal sac deformed, cord not abutted
- Axial T2 appearance
- Thecal sac deformed, cord abutted but not compressed
- Axial T2 appearance
- Cord compression but CSF still visible around the cord
- Axial T2 appearance
- Cord compression with NO CSF visible around the cord
SINS sums six components: (1) location (junctional occiput-C2/C7-T2/T11-L1/L5-S1 score highest), (2) mechanical/postural pain, (3) bone lesion quality (lytic worst), (4) spinal alignment (deformity/subluxation), (5) vertebral body collapse, and (6) posterolateral element involvement. Total 0-18: 0-6 = stable, 7-12 = indeterminate / potentially unstable (surgical consultation advised), 13-18 = unstable. A high SINS flags the need for stabilisation regardless of the neurological picture.
High-grade epidural compression (Bilsky 2-3) with a radioresistant tumour favours surgical decompression ("separation surgery") before radiotherapy, whereas low-grade compression (Bilsky 0-1) of a radiosensitive tumour may be managed with radiotherapy alone. An unstable SINS (13-18) argues for stabilisation even when the cord is not yet compressed. This Bilsky-plus-SINS pairing, alongside the NOMS framework (Neurological, Oncological, Mechanical, Systemic), is the modern decision scaffold for metastatic spine disease.
CRAMSRed Flags Requiring Urgent Spine MRI
Hook:CRAMS: these five scenarios demand URGENT MRI — delay risks permanent neurological damage.
NSAIDNEXUS Criteria for Cervical Spine Clearance
Hook:NSAID: if ALL five criteria are met, cervical spine can be cleared clinically WITHOUT imaging.
Clinical Applications
Cervical Spine Imaging
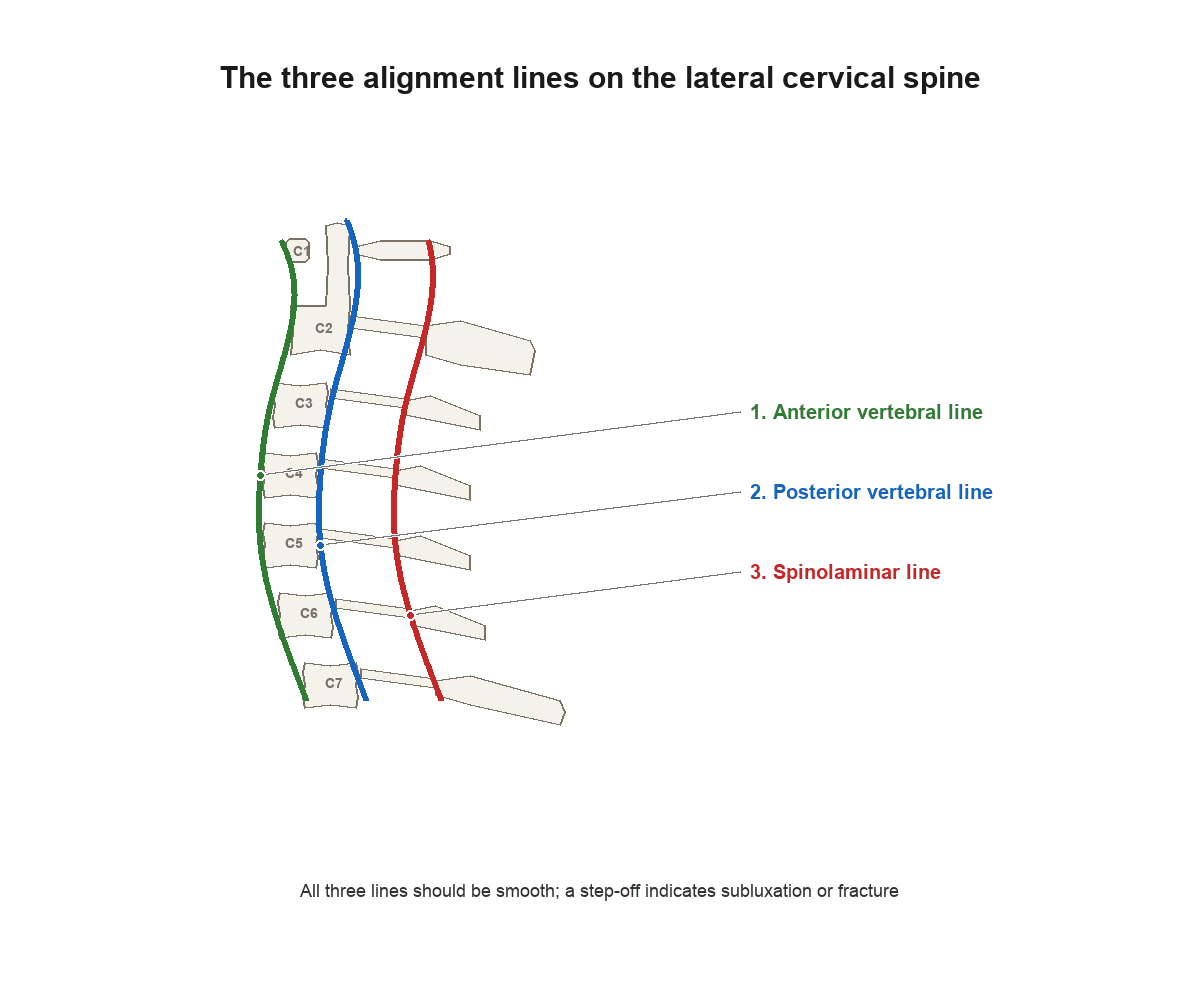
Radiographic assessment (lateral view): Three alignment lines: (1) Anterior vertebral line — follows the anterior cortex of the vertebral bodies. (2) Posterior vertebral line — follows the posterior cortex of the vertebral bodies (the anterior border of the spinal canal). (3) Spinolaminar line — connects the spinolaminar junctions. All three should be smooth lordotic curves. Any step-off suggests subluxation or fracture-dislocation. The atlantodental interval (ADI) should be less than 3mm in adults (less than 5mm in children) — increased ADI suggests transverse ligament disruption or odontoid fracture.
Prevertebral soft tissue width: Measured on the lateral radiograph. At C2: should be less than 7mm (or less than one-third of the vertebral body width). At C6: should be less than 21mm (or less than one full vertebral body width). Widening suggests haematoma from fracture, abscess, or retropharyngeal pathology.
Key cervical fractures: (1) Jefferson fracture (C1 burst): best seen on AP open-mouth view — lateral mass overhang more than 7mm combined (Rule of Spence) = transverse ligament disruption. (2) Hangman fracture (C2 pars): bilateral C2 pedicle fractures — often neurologically intact because canal enlarges. (3) Odontoid fractures (Anderson-D'Alonzo): Type I (tip, rare), Type II (base — most common, highest nonunion risk), Type III (extends into C2 body).
CT for cervical clearance: In major trauma, CT has replaced radiographs as the primary imaging modality for cervical spine clearance. CT sensitivity for cervical fractures is approximately 98% (vs 52-85% for radiographs). MRI is added when there is neurological deficit, suspected ligamentous injury, or persistent clinical concern despite normal CT.
Spondylolysis and the Pars Defect
Spondylolysis and the Pars Interarticularis Defect
A defect of the pars interarticularis (spondylolysis) is the commonest structural cause of low back pain in adolescents and young athletes (especially in hyperextension sports) and the usual cause of isthmic spondylolisthesis. It most often affects L5 (over 85% of cases). Its imaging deserves separate treatment because the modality you choose answers two different questions: is there a defect? and is it active (likely to heal)?
- Role
- Classic teaching view
- Key finding
- The 'Scottie dog' - the pars is the dog's NECK; a defect appears as a collar or a broken neck (decapitated Scottie dog)
- Role
- Detect and grade listhesis
- Key finding
- Anterolisthesis graded by Meyerding (I-IV); flexion-extension films assess dynamic instability
- Role
- Best bony definition
- Key finding
- Directly shows the pars defect, its margins (corticated chronic vs sharp acute), and any contralateral defect
- Role
- Activity and acuity
- Key finding
- Increased uptake (SPECT) or marrow/pars oedema (MRI STIR) indicates an ACTIVE, metabolically hot lesion with the best chance of bony healing; a cold, well-corticated defect is established and unlikely to unite
MRI is increasingly first-line in young patients (no ionising radiation) - a stress reaction with pars oedema but no frank defect can heal with activity restriction/bracing, whereas an established, corticated defect will not. SPECT-CT remains useful where MRI is equivocal. Grading the listhesis (Meyerding) and checking for a high-grade slip or dysplastic posterior elements guides the need for surgical stabilisation.
Guidelines, Registries & Global Practice
Spine imaging selection is remarkably consistent across major guideline bodies: clinical decision rules first, CT for fracture characterisation, MRI for cord and soft-tissue pathology. Where guidelines genuinely differ is in the threshold for advanced imaging and the recommended timing of MRI for red-flag presentations.
Global Epidemiology
- Low back pain is the single leading cause of years lived with disability worldwide (Global Burden of Disease), yet the overwhelming majority of acute episodes are non-specific and require no imaging.
- Clinically important cervical spine injury occurs in roughly 2 percent of alert, stable blunt-trauma patients who present for assessment.
- Cauda equina syndrome is rare (incidence on the order of a few per 100,000 per year) but accounts for a disproportionate share of spinal medicolegal claims, almost always for delayed diagnosis.
Side-by-Side Guideline Comparison
- Cervical Trauma Clearance
- CT cervical spine first-line in moderate/high-risk blunt trauma; clinical clearance (NEXUS or CCR) in low risk
- Low Back Pain / Red Flags
- No imaging for non-specific acute LBP without red flags; MRI reserved for neurological deficit, suspected infection, malignancy or CES
- Cervical Trauma Clearance
- NICE NG41 trauma: CT for adults with high-risk factors; MRI added for neurology or suspected ligamentous/cord injury
- Low Back Pain / Red Flags
- NICE NG59: do not image routinely; urgent MRI for suspected CES, metastatic cord compression or infection (whole-spine MRI within 1 week, or emergently for CES)
- Cervical Trauma Clearance
- AO Spine subaxial and upper-cervical classifications standardise CT-based morphology; MRI for discoligamentous complex
- Low Back Pain / Red Flags
- AO Spine thoracolumbar classification (CT morphology + neurology + modifiers) for fracture decision-making
- Cervical Trauma Clearance
- CT-led clearance in major trauma consistent with US/UK; MRI for obtunded patients with persistent concern
- Low Back Pain / Red Flags
- Emphasis on red-flag triage and stewardship to limit low-value spinal MRI
Registry and Audit Evidence
- Spinal trauma is captured in national and regional trauma registries (e.g. the UK Trauma Audit and Research Network and equivalent systems), which have tracked the shift from radiograph-led to CT-led cervical clearance and the reduction in missed injuries.
- Spinal cord injury registries inform the link between timing of decompression and neurological recovery, reinforcing early MRI and surgery in compressive deficits.
High- vs Limited-Resource Practice Variation
- In high-resource settings, multidetector CT and MRI are available around the clock, so CT-led clearance and urgent MRI for red flags are achievable targets.
- In limited-resource settings, MRI access may be delayed or absent; plain radiography and CT myelography retain a larger role, and clinical decision rules (NEXUS, CCR) become even more valuable to ration imaging safely.
- Regardless of setting, the principles are universal: apply a validated rule before imaging, use CT to characterise bony injury, and obtain MRI urgently when cord or cauda equina compromise is suspected.
Controversies & Areas of Uncertainty
Controversies and Areas of Uncertainty
In the obtunded or intubated patient with a normal high-quality CT, the role of additional MRI remains debated. Some protocols clear the collar on negative CT alone, citing the high negative predictive value of modern CT; others mandate MRI to exclude purely ligamentous injury. The balance is between rare missed unstable ligamentous injury and the harms of prolonged collar use and transfer for MRI.
The 48-hour threshold from pooled data is widely quoted, but it does not justify deliberate delay. Many surgeons and medicolegal standards expect decompression as soon as feasible, ideally overnight. The distinction between incomplete CES (CES-I) and CES with retention (CES-R) influences urgency and prognosis more than any single time cut-off.
Disc bulges, protrusions, Modic changes and mild stenosis are highly prevalent in asymptomatic adults and increase with age. Over-reporting drives unnecessary intervention. Imaging must always be correlated with the clinical syndrome and the relevant nerve root, not treated as a stand-alone diagnosis.
Isolated T2 cord hyperintensity is a weaker prognostic marker than once assumed. Combined T1 hypointensity with T2 hyperintensity, multilevel signal change, and a high signal-intensity ratio carry the worst prognosis, while clinical severity and duration remain the dominant drivers of outcome.


Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 30-year-old man is brought to the emergency department after a motorcycle accident. He is alert, GCS 15, and complains of neck pain. He has no neurological deficit.”
“A 45-year-old woman presents with a 4-week history of progressive bilateral leg weakness, urinary retention, and saddle anaesthesia. Back pain has been present for 6 months.”
“An examiner shows you an MRI of the lumbar spine and asks you to describe your systematic assessment.”
“A 68-year-old man with a history of prostate cancer presents with 3 weeks of progressive thoracic back pain, now with bilateral leg weakness and a sensory level at the umbilicus. He is febrile at 38.2 degrees with a raised CRP.”
ABCD Systematic Reading
- Alignment: 3 smooth lines on lateral (anterior, posterior vertebral, spinolaminar)
- Bones: vertebral body height, pedicles (winking owl = metastasis), cortices
- Cartilage/Disc: disc space height, facet joints, interspinous distance
- Dens/Soft tissues: odontoid fracture, prevertebral width (C2: less than 7mm, C6: less than 21mm)
Red Flags for Urgent MRI (CRAMS)
- Cauda equina syndrome (bladder/bowel dysfunction, saddle anaesthesia)
- Rapidly progressive neurological deficit
- Abscess/infection (fever + back pain + raised inflammatory markers)
- Metastatic disease (cancer history + night pain + weight loss)
- Spinal cord compression/myelopathy (UMN signs)
Key Cervical Fractures
- Jefferson (C1 burst): lateral mass overhang more than 7mm = transverse ligament torn
- Hangman (C2 pars): bilateral C2 pedicle fx — often neurologically intact
- Odontoid: Type II (base) = highest nonunion risk
- ADI more than 3mm (adults) or more than 5mm (children) = transverse ligament disruption
TLICS Score
- Morphology: compression(1), burst(2), translational(3), distraction(4)
- PLC: intact(0), suspected(2), injured(3)
- Neuro: intact(0), root(2), cord incomplete(3), complete(2), cauda equina(3)
- Total: less than 4 = conservative, more than 4 = surgical
Evidence Base
Canadian C-Spine Rule vs NEXUS
- The Canadian C-Spine Rule (CCR) had higher sensitivity (99.4%) than NEXUS (90.7%) for clinically important cervical spine injury.
- CCR was more specific (45.1% vs 36.8%), reducing unnecessary imaging more effectively.
- Both rules were validated for adult blunt trauma patients with GCS 15.
CT vs Radiography for Cervical Spine Clearance
- Pooled sensitivity for cervical fracture was 98% (95% CI 96-99) for CT compared to 52% (95% CI 47-56) for plain radiographs across seven studies.
- The authors recommended CT as the initial screening test in high-risk patients with significantly depressed mental status.
- They found insufficient evidence to replace radiography with CT in lower-risk patients who still require imaging.
SLIC: Subaxial Cervical Spine Injury Classification
- The Subaxial Injury Classification (SLIC) scores subaxial (C3-C7) cervical injuries on three axes: injury morphology, discoligamentous complex integrity, and neurological status.
- Like TLICS, the composite score guides operative versus non-operative care: less than 4 non-operative, equal to 4 surgeon discretion, more than 4 operative.
- The accompanying algorithm directs surgical approach — burst and distraction injuries usually anterior, severe translation/rotation injuries posterior or combined.
Evidence strongly supports CT over radiographs for cervical spine clearance in major trauma, and validated classification scores (SLIC, TLICS) integrate imaging into surgical decision-making.