Systematic radiographic and MRI evaluation of bone and soft-tissue tumours
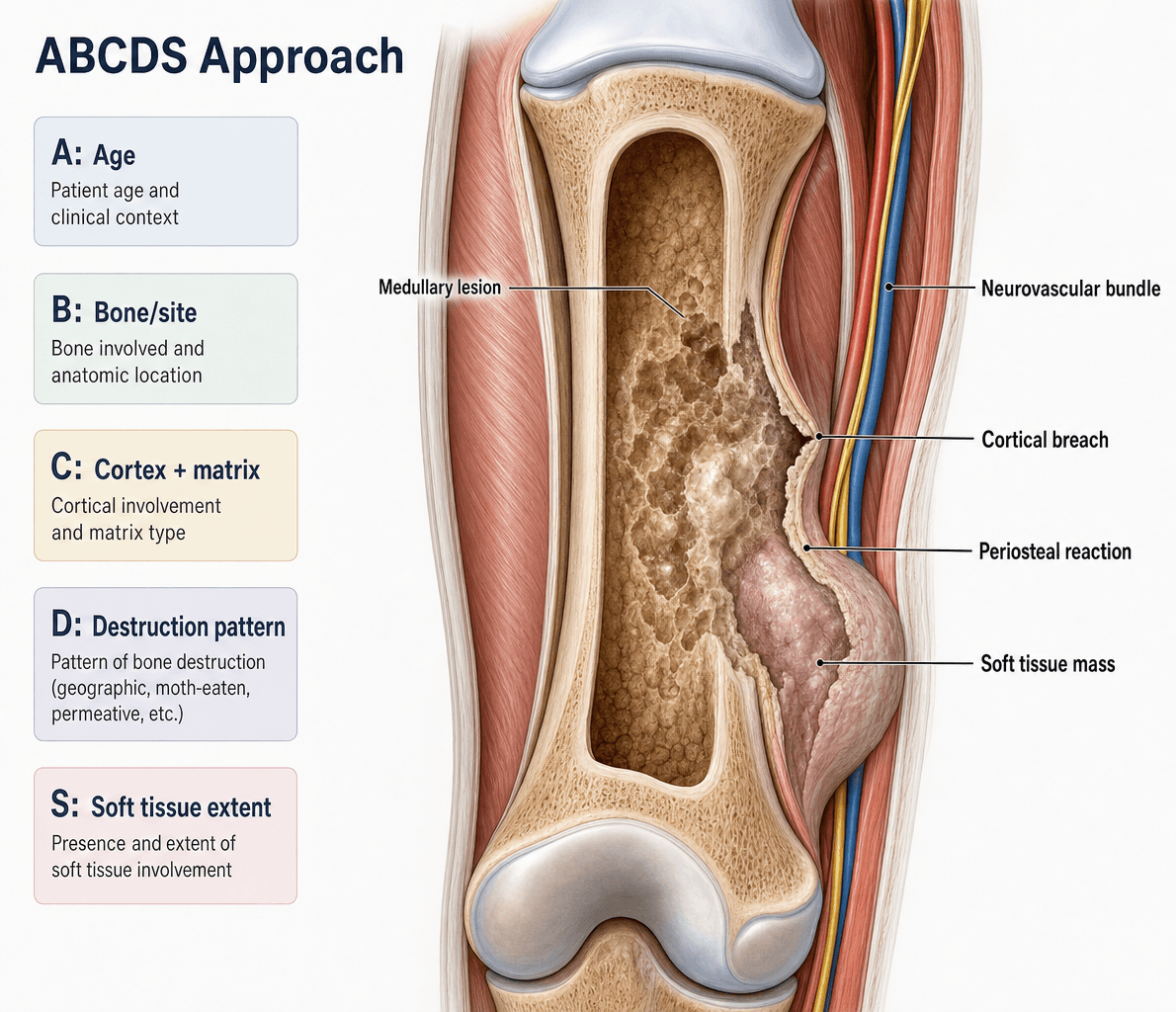
- ABCDS: Age, Border, Cortex, Depth, Soft tissue
- Zone of transition: narrow (benign) vs wide (aggressive)
- Lodwick classification grades aggressiveness (I-III)
- Whole bone MRI mandatory before biopsy for staging
- Biopsy track must be planned with definitive surgeon
- “Age is single most important factor in differential
- “Periosteal reaction: solid (benign) vs interrupted (aggressive)
- “Skip lesions: separate tumour foci in same bone
- “Enneking staging: compartmental vs extracompartmental
- “Don't biopsy before discussing with tumour surgeon
Tumour imaging is a favourite viva topic. You MUST know the ABCDS systematic approach, Lodwick classification, and age-related differentials. Always mention that biopsy track planning requires discussion with the definitive tumour surgeon.
Overview and Principles
Musculoskeletal tumours span a vast spectrum from trivial "do-not-touch" lesions (non-ossifying fibroma, bone island) to lethal high-grade sarcomas. The single most important task for the examination candidate is not memorising every entity but applying a reproducible systematic framework to any radiograph, then deciding whether the lesion is non-aggressive (can be observed or treated by a generalist) or aggressive (must be referred to a specialist sarcoma centre before any intervention).
The radiograph remains the cornerstone of bone-tumour assessment: matrix mineralisation, periosteal reaction and zone of transition are best appreciated on plain film and frequently allow a confident diagnosis or a tight differential. Cross-sectional imaging then answers specific questions — MRI for marrow and soft-tissue extent and local staging, CT for cortical detail and pulmonary metastases, and FDG-PET/CT for whole-body staging and response.
A recurring exam theme is the danger of acting before staging. A poorly planned biopsy or an unwary excision of an unsuspected sarcoma can convert a limb-salvageable tumour into an amputation or compromise survival. The candidate who states early that any suspicious lesion is referred intact to a sarcoma multidisciplinary team, fully staged, and biopsied along a planned track demonstrates safe practice.
Systematic ABCDS Approach
A-B-C-D-SABCDS - Tumour Imaging Assessment
Hook:Work through each element systematically in viva - this demonstrates methodical approach and covers all key features
- Benign
- Eosinophilic granuloma, Simple bone cyst, Osteochondroma
- Malignant
- Ewing sarcoma, Neuroblastoma mets
- Benign
- Osteoid osteoma, Chondroblastoma, Aneurysmal bone cyst
- Malignant
- Osteosarcoma, Ewing sarcoma
- Benign
- Giant cell tumour, Enchondroma
- Malignant
- Primary lymphoma, Parosteal osteosarcoma
- Benign
- Fibrous dysplasia (monostotic), Haemangioma
- Malignant
- Metastases, Myeloma, Chondrosarcoma
- Benign
- Paget's disease
- Malignant
- Metastases (most common), Myeloma
Lodwick Classification

- Pattern
- Geographic with sclerotic rim
- Zone of Transition
- Very narrow
- Growth Rate
- Very slow
- Typical Lesions
- NOF, Enchondroma, SBC
- Pattern
- Geographic without sclerosis
- Zone of Transition
- Narrow
- Growth Rate
- Slow
- Typical Lesions
- GCT, ABC, Eosinophilic granuloma
- Pattern
- Geographic with ill-defined margin
- Zone of Transition
- Wide
- Growth Rate
- Moderate
- Typical Lesions
- Low-grade malignancy, Infection
- Pattern
- Moth-eaten
- Zone of Transition
- Wide
- Growth Rate
- Fast
- Typical Lesions
- Aggressive malignancy, Osteomyelitis
- Pattern
- Permeative
- Zone of Transition
- Very wide
- Growth Rate
- Very fast
- Typical Lesions
- Round cell tumours, Ewing, Lymphoma
Periosteal Reaction Patterns
- Appearance
- Smooth, uninterrupted
- Implication
- Slow-growing, benign
- Common Causes
- Stress fracture, Osteoid osteoma
- Appearance
- Multiple parallel layers
- Implication
- Intermittent growth
- Common Causes
- Ewing sarcoma, Osteomyelitis
- Appearance
- Perpendicular striations
- Implication
- Aggressive, rapid growth
- Common Causes
- Osteosarcoma
- Appearance
- Fine perpendicular spicules
- Implication
- Aggressive
- Common Causes
- Ewing, Marrow expansion
- Appearance
- Interrupted periosteum lifted at edge
- Implication
- Very aggressive
- Common Causes
- Osteosarcoma, Ewing, Infection
Solid = Slow, Spiculated = SinisterAggressive vs Non-aggressive Periosteal Reaction
Hook:Infection can mimic aggressive tumour periosteal reaction - always correlate with clinical features
Matrix Mineralisation
- Appearance
- Dense, cloud-like, amorphous
- Tumours
- Osteosarcoma, Osteoid osteoma, Osteoblastoma
- Appearance
- Rings and arcs, popcorn
- Tumours
- Enchondroma, Chondrosarcoma, Chondroblastoma
- Appearance
- Ground-glass, hazy
- Tumours
- Fibrous dysplasia, NOF
- Appearance
- Combination patterns
- Tumours
- Dedifferentiated tumours
Enneking Surgical Staging
The topic repeatedly refers to "Enneking staging" — the examiner expects you to reproduce it. There are two systems, one for benign and one for malignant musculoskeletal tumours, both integrating imaging-defined compartmental anatomy.
- Behaviour
- Inactive, self-limiting, stays within its capsule
- Examples
- Non-ossifying fibroma, bone island
- Behaviour
- Grows and deforms but remains contained
- Examples
- Aneurysmal bone cyst, active simple bone cyst
- Behaviour
- Locally aggressive, breaches the capsule and cortex
- Examples
- Giant cell tumour
For malignant lesions the system combines histological grade (G1 low, G2 high), anatomic site (T1 intracompartmental, T2 extracompartmental) and metastasis (M0 / M1):
- Grade
- G1 (low)
- Site
- T1 (intracompartmental)
- Metastasis
- M0
- Grade
- G1 (low)
- Site
- T2 (extracompartmental)
- Metastasis
- M0
- Grade
- G2 (high)
- Site
- T1 (intracompartmental)
- Metastasis
- M0
- Grade
- G2 (high)
- Site
- T2 (extracompartmental)
- Metastasis
- M0
- Grade
- Any grade
- Site
- Any site
- Metastasis
- M1 (regional or distant)
MRI in Tumour Imaging
- Sequence
- T1, STIR
- Key Information
- Low T1 = tumour replacing marrow
- Sequence
- T2, Gd-enhanced
- Key Information
- Size, relationship to NV structures
- Sequence
- Whole bone T1/STIR
- Key Information
- Separate tumour foci (staging, prognosis)
- Sequence
- All sequences
- Key Information
- Affects surgical planning
- Sequence
- Gd-enhanced, MRA
- Key Information
- Resectability assessment
Classic Tumour Appearances
- Location
- Cortex of long bones
- Age
- 10-25y
- Classic Features
- Less than 1.5cm nidus with reactive sclerosis, nocturnal pain relieved by NSAIDs
- Location
- Metaphysis, away from joint
- Age
- Less than 30y
- Classic Features
- Cortex and medulla continuous with parent bone, pedunculated or sessile
- Location
- Hands, metaphysis long bones
- Age
- 20-40y
- Classic Features
- Central, rings and arcs calcification, Lodwick IA
- Location
- Epiphysis, extends to subchondral
- Age
- 20-40y
- Classic Features
- Eccentric, subarticular, no sclerotic margin (IB), closed physis
- Location
- Proximal humerus, prox femur
- Age
- Less than 20y
- Classic Features
- Central, fallen fragment sign, slightly expansile
- Location
- Metaphysis, eccentric
- Age
- Less than 20y
- Classic Features
- Well-defined, sclerotic rim, asymptomatic, resolves
Soft Tissue Tumour Imaging
- Benign Indicators
- Less than 5 cm
- Malignant Indicators
- Greater than 5 cm
- Benign Indicators
- Superficial to fascia
- Malignant Indicators
- Deep to fascia
- Benign Indicators
- Well-defined, smooth
- Malignant Indicators
- Irregular, infiltrative
- Benign Indicators
- Homogeneous
- Malignant Indicators
- Heterogeneous, necrosis
- Benign Indicators
- Homogeneous signal
- Malignant Indicators
- Mixed signal, haemorrhage, necrosis
- Benign Indicators
- Uniform or none
- Malignant Indicators
- Heterogeneous, peripheral
Imaging-Guided Biopsy
Track in LineBiopsy Planning
Hook:Poorly planned biopsy can convert a limb-salvage case to amputation due to track contamination
Surgical Margins
Imaging does not just diagnose — it defines whether a tumour can be removed with an oncologically adequate margin, which is why MRI assessment of compartmental boundaries is mandatory. Enneking described four margins by the plane of dissection relative to the tumour and its reactive zone.
- Plane of dissection
- Through the tumour itself (e.g. curettage, debulking)
- Oncological result
- Macroscopic tumour left behind
- Plane of dissection
- Through the reactive zone / pseudocapsule (shell-out)
- Oncological result
- Risks residual satellite or reactive-zone tumour
- Plane of dissection
- En bloc with a cuff of normal tissue, within the same compartment
- Oncological result
- Standard for malignant limb salvage
- Plane of dissection
- Removal of the entire involved compartment(s), or amputation above it
- Oncological result
- Whole compartment cleared
Differential Diagnosis: Aggressive vs Non-Aggressive
The decisive radiographic discriminator is the zone of transition combined with periosteal reaction and cortical status, integrated with patient age. The table below collapses the most common pattern-based decisions a candidate must make at the viva.
- Most Likely Group
- Benign, slow (NOF, fibrous dysplasia, enchondroma)
- Key Discriminators
- Sharp pencil-traceable margin, no soft-tissue mass
- Common Mimics / Traps
- Low-grade chondrosarcoma can look enchondroma-like
- Most Likely Group
- Giant cell tumour
- Key Discriminators
- Closed physis, subchondral extension
- Common Mimics / Traps
- ABC (fluid-fluid levels), chondroblastoma (open physis)
- Most Likely Group
- Osteosarcoma
- Key Discriminators
- Codman triangle, soft-tissue ossification, age 10-25
- Common Mimics / Traps
- Osteomyelitis and stress fracture can mimic
- Most Likely Group
- Ewing sarcoma / round cell
- Key Discriminators
- Age 5-25, systemic symptoms, fever
- Common Mimics / Traps
- Osteomyelitis, eosinophilic granuloma, lymphoma
- Most Likely Group
- Metastases / myeloma
- Key Discriminators
- Known primary, vertebral body sparing pedicle
- Common Mimics / Traps
- Brown tumours of hyperparathyroidism
- Most Likely Group
- Chondrosarcoma
- Key Discriminators
- Pain, cortical destruction, deep endosteal scalloping
- Common Mimics / Traps
- Enchondroma (asymptomatic, no deep scalloping)
WIDE = WorryAggressive vs Non-Aggressive at a Glance
Hook:Any WIDE feature in an at-risk age group means refer and stage before you touch the lesion.
Guidelines, Registries & Global Practice
Primary bone sarcomas are rare worldwide (osteosarcoma incidence approximately 3-4 per million per year, peaking in adolescence, with a second peak in older adults often related to Paget disease or prior radiation). Ewing sarcoma is rarer still and shows marked geographic and ancestral variation, being notably less common in populations of African ancestry. Soft-tissue sarcomas are commoner than bone sarcomas (roughly 4-5 per 100,000 per year) but still account for under 1% of adult malignancies. Bone metastases vastly outnumber primary bone tumours overall and dominate the differential in patients over 40.
- Region
- UK
- Key Position
- Urgent direct-access radiograph for suspected bone sarcoma; refer suspected sarcoma to a specialist centre BEFORE biopsy; MRI of whole compartment for local staging
- Region
- Europe
- Key Position
- Any deep or over-5cm soft-tissue mass imaged with MRI and referred to a reference centre before biopsy; biopsy planned by the treating sarcoma team
- Region
- US / international
- Key Position
- Cross-sectional local imaging plus chest CT for staging; image-guided core biopsy along a track that can be excised; multidisciplinary review
- Region
- US
- Key Position
- Radiograph first-line for a suspected primary bone lesion; MRI for local extent; bone scan/PET-CT for skeletal and systemic staging
Imaging Atlas
Controversies and Areas of Uncertainty
Clinical Imaging Modalities
- Primary Role
- First-line characterisation
- Strengths
- Matrix, periosteal reaction, zone of transition, aggressiveness
- Limitations
- Insensitive to marrow and soft-tissue extent
- Primary Role
- Cortical detail, matrix, staging chest
- Strengths
- Subtle cortical breach, mineralisation, lung metastases
- Limitations
- Ionising radiation, poor soft-tissue contrast
- Primary Role
- Local staging (marrow + soft tissue)
- Strengths
- Marrow extent, skip lesions, neurovascular relations
- Limitations
- Cost/access; metal artefact; less specific for matrix
- Primary Role
- Skeletal survey, polyostotic disease
- Strengths
- Whole-skeleton sensitivity
- Limitations
- Low specificity; myeloma often photopenic
- Primary Role
- Whole-body staging, response, recurrence
- Strengths
- Metabolic activity, distant disease, restaging
- Limitations
- False positives (infection, healing); resolution limits
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
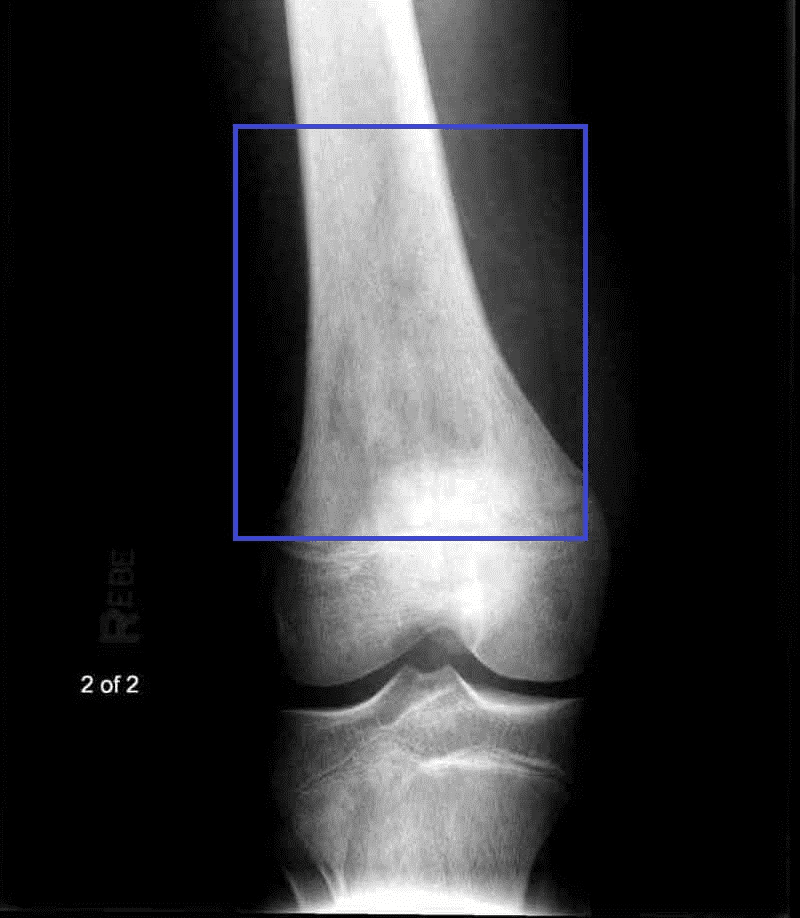
“A 16-year-old presents with a 2-month history of knee pain. X-ray shows a mixed lytic and sclerotic lesion in the distal femoral metaphysis with periosteal reaction.”
“A 55-year-old woman presents with back pain. Spinal X-ray shows a lytic lesion in L3 vertebral body. She has a history of breast cancer 5 years ago.”
“A 30-year-old presents with knee pain. X-ray shows an expansile lytic lesion in the proximal tibial epiphysis extending to the subchondral bone. The lesion has no sclerotic margin.”
ABCDS Framework
- Age: Most important factor - metastases if greater than 40
- Border: Narrow = benign, Wide = aggressive
- Cortex: Intact/expanded vs destroyed
- Depth: Medullary/cortical/surface location
- Soft tissue: Mass indicates aggressive behaviour
Lodwick Classification
- IA: Geographic + sclerotic rim = very benign
- IB: Geographic, well-defined = slow growing
- IC: Geographic, ill-defined = moderate
- II: Moth-eaten = aggressive
- III: Permeative = very aggressive (Ewing, lymphoma)
Periosteal Reaction
- Solid/continuous = slow, benign
- Lamellated (onion-skin) = Ewing, infection
- Sunburst = osteosarcoma
- Codman triangle = aggressive
Pre-Biopsy Rules
- Whole bone MRI BEFORE biopsy (skip lesions)
- CT chest for lung metastases
- Discuss track with tumour surgeon
- Plan track in line with definitive resection
- Poor biopsy can convert salvage to amputation
Evidence Base
Surgical Staging System for Musculoskeletal Sarcoma (Enneking)
- Introduced the GTM staging system stratifying sarcomas by histological grade (G1 low / G2 high), anatomic compartment (T1 intracompartmental / T2 extracompartmental) and metastasis (M0/M1).
- Defined the three surgical stages (I low-grade, II high-grade, III metastatic) each subdivided by compartmental status, and linked them to surgical margins (intralesional, marginal, wide, radical).
- Provided the conceptual basis for relating imaging-defined compartmental anatomy to oncologically appropriate resection.
Lodwick and Enneking Classifications Have Poor Reliability
- Across 48 radiolucent lesion cases rated twice by 20 observers, interobserver agreement was poor for the original Lodwick (39%, kappa 0.23), modified Lodwick (39%, kappa 0.25) and Enneking benign classification (53%, kappa 0.28).
- Intra-observer reproducibility was only fair to moderate (kappa 0.42-0.45), and training level had no measurable effect.
- Lesions were correctly called malignant in only 73%, 59% and 62% of cases respectively across the three systems.