Imaging in Acute Orthopaedic Trauma
- Two views minimum: At 90° to each other. One view is never enough for fracture assessment.
- Joint above and below: Always include adjacent joints in long bone imaging.
- CT for polytrauma: Pan-scan (C-spine through pelvis) is standard for major trauma.
- Never clear C-spine on X-ray alone: CT is required for obtunded patients.
- Systematic approach: ABCS for every image - Alignment, Bone, Cartilage, Soft tissue.
- “Satisfaction of search: Finding one injury doesn't mean there aren't more. Complete your systematic review.
- “10% of spinal fractures have a second non-contiguous spinal injury.
- “Pelvic ring injuries require two breaks - always look for the second injury.
- “CT reconstructions (sagittal, coronal, 3D) are essential - axial slices alone are insufficient.
- “Occult fractures: If X-ray negative but clinical concern high, CT or MRI is indicated.
A single radiographic view is NEVER adequate for fracture assessment. Fractures can be invisible on one projection but obvious on another. Always obtain a minimum of two views at 90 degrees to each other. This is a fundamental principle that saves missed injuries.
2-2-1Rules of Trauma Radiography
Hook:2 views, 2 joints, 1 system
Systematic Approach: Imaging Pitfalls
Common Missed Injuries
SCALPCommonly Missed Fractures
Hook:Don't let injuries SCALP you
Satisfaction of Search
Definition: Stopping the search after finding one injury
Prevention:
- Complete ABCS for every image even after finding a fracture
- Actively look for associated injuries
- Remember patterns (ACL tear → check meniscus; pelvic ring → find second break)
- Don't anchor on the obvious injury
Example: Finding a displaced distal radius fracture but missing the associated ulnar styloid avulsion or DRUJ disruption
Adequacy Checklist
Ask yourself:
- Are there two views at 90 degrees?
- Are the joints above and below included?
- Is the image quality adequate (penetration, rotation, coverage)?
- Have I completed ABCS systematically?
- Have I looked at all cortices?
- Does the clinical picture match my interpretation?
- If X-rays are normal but clinical concern persists, have I considered CT/MRI?
If any answer is 'no': Obtain additional imaging or review with senior
Principles of Trauma Imaging in the ATLS Framework

Primary Survey Imaging
When to Image
Hemodynamically unstable patient:
- Resuscitation takes priority
- CXR and pelvis X-ray as adjuncts
- May go directly to OR or IR
- CT only if will not delay definitive treatment
Hemodynamically stable patient:
- CT pan-scan indicated for significant mechanism
- Complete secondary survey imaging
- Time for detailed fracture assessment
Plain Radiograph Principles
Why Two Views
- View That May Miss It
- AP
- View That Shows It
- Lateral
- View That May Miss It
- AP
- View That Shows It
- Lateral
- View That May Miss It
- PA
- View That Shows It
- Scaphoid view
- View That May Miss It
- AP
- View That Shows It
- Lateral
- View That May Miss It
- AP ankle
- View That Shows It
- Full-length tibia/fibula
ABCS Systematic Approach
- Joint congruity
- Bone axis/angulation
- Subluxation/dislocation
- Rotational deformity
- Cortical breaks (all cortices)
- Trabecular disruption
- Bone density
- Periosteal reaction
- Joint space width
- Subchondral bone
- Intra-articular fragments
- Effusion
- Swelling (localization)
- Fat pads (effusion signs)
- Foreign bodies
- Gas (open fracture)
Radiation Dose and ALARA in Trauma Imaging
The benefit of rapid, complete CT is weighed against ionising-radiation dose - and the viva will ask the approximate dose of a trauma CT. Effective doses (approximate, for orientation, not exact figures):
- Approx effective dose
- ~0.02 mSv
- Background equivalent
- ~3 days
- Approx effective dose
- ~0.7 mSv
- Background equivalent
- ~4 months
- Approx effective dose
- ~2 mSv
- Background equivalent
- ~8 months
- Approx effective dose
- ~3 mSv
- Background equivalent
- ~1 year
- Approx effective dose
- ~10 mSv
- Background equivalent
- ~3 to 4 years
- Approx effective dose
- ~20 to 30 mSv
- Background equivalent
- ~7 to 10 years
Natural background radiation is roughly 2 to 3 mSv per year for reference.
Why it matters: a pan-scan delivers the radiation of several years of background exposure in seconds. Because REACT-2 showed no mortality benefit for indiscriminate pan-scan, the dose is justified by patient selection, not reflex. The concern is greatest in children and young polytrauma survivors, where the lifetime stochastic (cancer) risk is highest - driving an ALARA approach: image only when it will change management, use low-dose and weight/age-adapted CT protocols, and prefer ultrasound (FAST) and MRI where they can answer the question without ionising radiation.
Regional Trauma Imaging
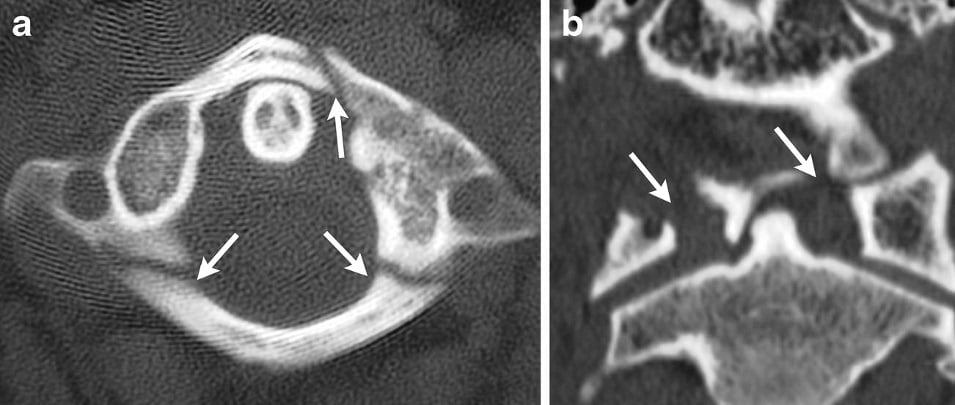
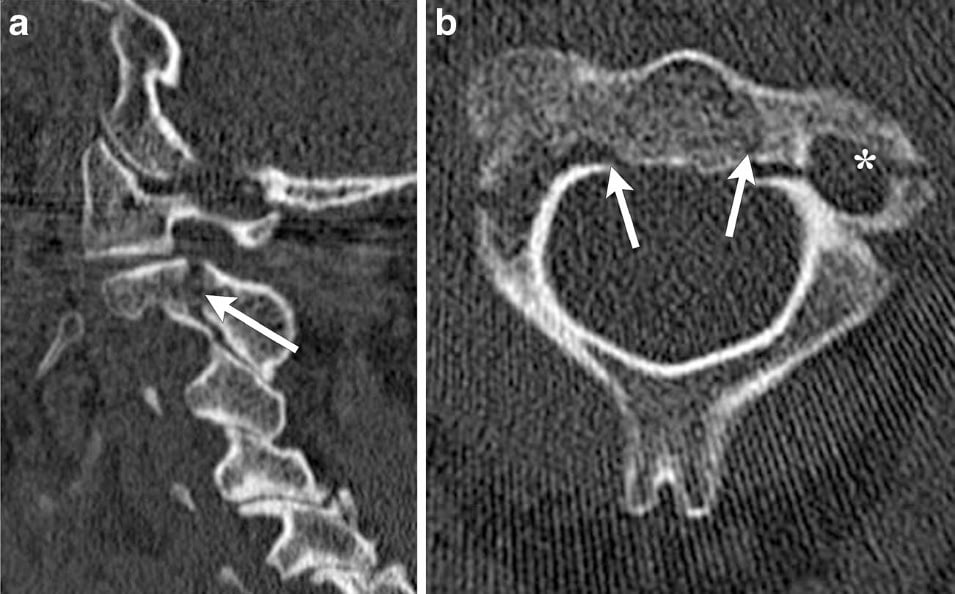
Cervical Spine
Clinical clearance (NEXUS/Canadian C-spine Rules):
- Alert, no midline tenderness, no distracting injury, no intoxication, no neuro deficit
- If criteria met: No imaging needed
If imaging required:
- CT is gold standard (NOT plain films)
- Plain films miss up to 50% of fractures
- MRI if: Neurological deficit, ligamentous injury suspected, obtunded patient with normal CT
Never clear an obtunded patient on plain films alone
Pelvic Ring
AP pelvis X-ray:
- ATLS adjunct in primary survey
- Assess ring integrity, pubic symphysis, SI joints
CT pelvis:
- Essential for all pelvic ring injuries
- Young-Burgess classification
- Acetabular involvement
- Posterior ring assessment
Remember: Ring breaks in two places - find both injuries
Long Bone Fractures
- Application
- AP and lateral minimum
- Why
- Fractures hide on single view
- Application
- Above and below
- Why
- Associated injuries, classify fracture
- Application
- Compare to normal side
- Why
- Rotational malunion prevention
- Application
- Intra-articular extension
- Why
- Surgical planning
Differential Diagnosis: Choosing the Right Modality
Modality Selection by Clinical Problem
When initial radiographs are negative but suspicion persists, the choice between CT, MRI and bone scintigraphy depends on the anatomical region, the urgency, radiation considerations and local availability. Picking the wrong second-line test wastes time and may still miss the injury.
- First-Line
- PA, lateral, scaphoid views
- Best Second-Line
- MRI (or CT)
- Key Reasoning
- MRI sensitivity ~88%, near-perfect specificity; avoids unnecessary casting
- First-Line
- AP pelvis + lateral hip
- Best Second-Line
- MRI
- Key Reasoning
- MRI is gold standard; CT can miss non-displaced femoral neck fractures
- First-Line
- None - go to CT
- Best Second-Line
- CT C-spine
- Key Reasoning
- Plain films miss many fractures; CT sensitivity over 99%
- First-Line
- CT (bone)
- Best Second-Line
- MRI
- Key Reasoning
- MRI shows cord, disc, ligament and SCIWORA in children
- First-Line
- AP pelvis
- Best Second-Line
- CT with reconstructions
- Key Reasoning
- Defines posterior ring, columns, planning
- First-Line
- AP/lateral region
- Best Second-Line
- MRI
- Key Reasoning
- Marrow oedema visible before cortical change
- First-Line
- FAST / CXR
- Best Second-Line
- CT angiography
- Key Reasoning
- Plain films cannot assess; CTA defines active bleeding
For most occult fractures (scaphoid, hip, sacrum, stress fractures), MRI is the most useful single second-line test because it shows marrow oedema before any cortical change and has the best balance of sensitivity and specificity. CT is faster and excellent for cortical/comminuted detail and surgical planning but can miss non-displaced trabecular fractures. Bone scintigraphy is highly sensitive but poorly specific and involves a diagnostic delay - rarely first choice in modern practice.
Guidelines, Registries & Global Practice
Global Epidemiology
Trauma is a leading cause of death and disability worldwide, accounting for roughly 4 to 5 million deaths each year, with road-traffic injury the single largest contributor and a disproportionate burden in low- and middle-income countries. Imaging is central to early decision-making, but access to CT and MRI varies enormously between high-resource trauma systems and limited-resource settings.
Side-by-Side Guideline Comparison
- Cervical Spine
- CXR + pelvis as primary-survey adjuncts; CT for clearance
- Whole-Body CT
- Adjunct once stabilised
- Emphasis
- ABCDE, life-threatening injuries first
- Cervical Spine
- Canadian C-Spine Rule to select CT; CT first-line if indicated
- Whole-Body CT
- Whole-body CT for adults with suspected multiple injuries
- Emphasis
- Selective imaging, avoid plain C-spine films in adults
- Cervical Spine
- CT for moderate/high risk
- Whole-Body CT
- Supports CT for major mechanism
- Emphasis
- Evidence-based modality selection
- Cervical Spine
- CT-led work-up
- Whole-Body CT
- Pan-scan in haemodynamically stable polytrauma
- Emphasis
- FAST in unstable patients, CT when stable
NICE explicitly advises against plain-film (three-view) cervical-spine series as the primary imaging in adults who need imaging, going straight to CT. This contrasts with older or resource-limited protocols where plain films remain the only available first-line test. Be able to justify CT-first on sensitivity grounds while acknowledging that plain radiography retains a role where CT is unavailable.
Registry & System-Level Evidence
National and regional trauma registries (for example the UK Trauma Audit and Research Network and the US National Trauma Data Bank) consistently link the introduction of in-resuscitation-room or rapid-access CT and standardised pan-scan protocols to shorter times to diagnosis and definitive care. These are observational, system-level signals rather than randomised mortality benefit, consistent with REACT-2.
High- vs Limited-Resource Practice Variation
- High-resource trauma centre: CT in or adjacent to the resuscitation bay, rapid pan-scan for major trauma, MRI readily available for cord and occult fracture, formal radiologist reporting.
- Limited-resource setting: Plain radiography and clinical decision rules (NEXUS, Canadian C-Spine Rule, Ottawa rules) become even more valuable to triage scarce CT; FAST ultrasound substitutes for CT in assessing free fluid; transfer pathways and clear documentation matter most.
- Universal principles: ABCDE first, two views minimum, joint above and below, systematic ABCS review, and never clearing the obtunded C-spine clinically - these hold regardless of available technology.
Special Situations
Open Fractures
Foreign body assessment:
- X-ray: Radiopaque foreign bodies (metal, glass)
- May miss wood, plastic, cloth
- CT if X-ray negative but contamination suspected
Gas in soft tissues:
- May indicate open fracture even if wound appears small
- Consider gas gangrene if delayed presentation
Antibiotic administration: Should not be delayed for imaging beyond initial X-rays
Polytrauma Patient
Priorities:
- Life over limb - ATLS approach
- CXR and pelvis X-ray with primary survey
- CT pan-scan when stable
- Extremity X-rays during secondary survey
Temporary measures:
- Splint fractures before moving for CT
- Document neurovascular status before and after
- Photograph open wounds
Communication: Clear handover of imaging findings to receiving team
Pediatric Considerations
Different considerations:
- Growth plates (Salter-Harris)
- Plastic deformation (bowing)
- Greenstick fractures
- Higher radiation sensitivity
Comparison views: May be helpful in children (ossification centers vary)
NAI (Non-accidental injury):
- Consider when injury doesn't match history
- Full skeletal survey if suspected
- Dating fractures (callus, healing stage)
FAST and eFAST Ultrasound
The topic repeatedly defers to "FAST" - here is what it is and where it fits. FAST (Focused Assessment with Sonography in Trauma) is a bedside ultrasound for free fluid (blood) in the dependent spaces, performed in the resuscitation bay without interrupting the primary survey.
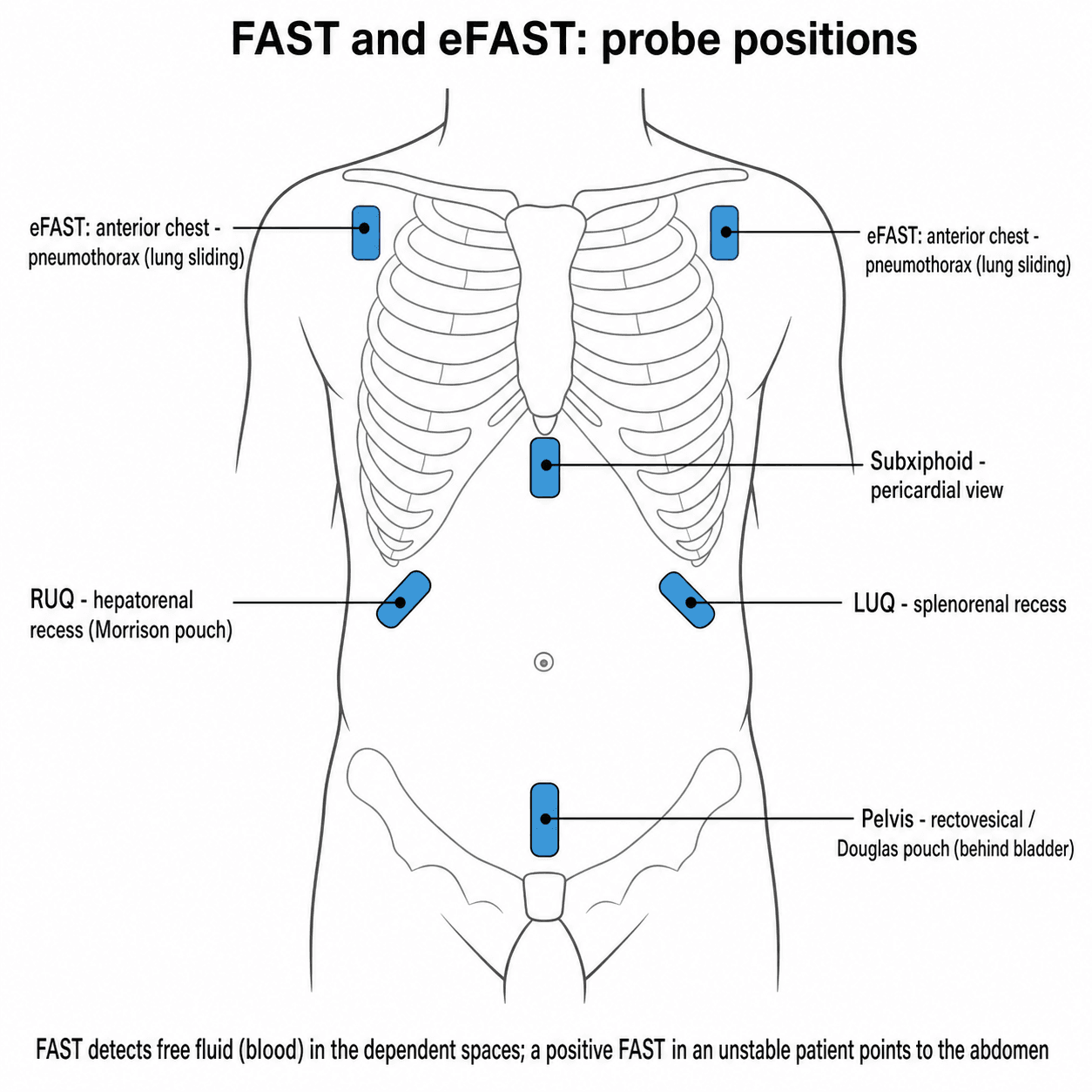
The standard FAST windows:
- Right upper quadrant - the hepatorenal recess (Morrison's pouch), the most sensitive single view for free fluid.
- Left upper quadrant - the splenorenal recess.
- Pelvis - the rectovesical pouch / pouch of Douglas, behind the bladder.
- Subxiphoid (pericardial) - for a pericardial effusion or tamponade.
eFAST (extended FAST) adds the anterior chest views to detect a pneumothorax (loss of lung sliding) and a haemothorax.
Role and limitations:
- The key role is the haemodynamically unstable patient: a positive FAST (free fluid) in an unstable patient points to the abdomen as the bleeding source and mandates laparotomy rather than a trip to the CT scanner.
- It is operator-dependent, detects fluid (not the specific organ injury), needs roughly 200 mL or more to be reliably positive, and misses retroperitoneal bleeding and hollow-viscus injury.
- A negative FAST does NOT exclude significant injury - in the stable patient, CT remains the definitive test.
Clinical Imaging: CT in Trauma
CT Trauma Protocol
Consider CT pan-scan for:
- High-energy mechanism (MVA greater than 60 km/h, ejection, rollover)
- Fall greater than 3 meters
- Pedestrian vs vehicle
- Motorcycle accident
- GCS less than 15
- Multiple injuries apparent
- Hemodynamically abnormal (or recently unstable)
- Polytrauma
Standard protocol: Non-contrast head → C-spine through pelvis with IV contrast
CT Advantages
- Plain X-ray
- 50-60%
- CT
- Greater than 99%
- Plain X-ray
- Limited
- CT
- Excellent
- Plain X-ray
- Cannot assess
- CT
- Gold standard
- Plain X-ray
- Faster per image
- CT
- Faster comprehensive assessment
- Plain X-ray
- Lower per image
- CT
- Higher total
- Plain X-ray
- Not possible
- CT
- Excellent for planning
Essential CT Reconstructions
Essential reconstructions:
- Sagittal: Spine alignment, vertebral body height
- Coronal: Pelvic ring, acetabular columns, alignment
- 3D Surface: Complex fracture visualization, surgical planning
Bone and soft tissue windows: Review both for all trauma CT
Common error: Reviewing only axial images and missing fractures obvious on reconstructions
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A patient presents after an MVA with left thigh pain. The AP X-ray shows no obvious fracture. Is this adequate imaging?”
“A 35-year-old pedestrian struck by a car at 50km/h arrives with GCS 13. Describe your imaging approach.”
“What are commonly missed orthopaedic injuries and how do you avoid missing them?”
“An 80-year-old woman cannot weight-bear after a fall, but her AP pelvis and lateral hip radiographs look normal. What is your next step and what is the evidence?”
Fundamental Rules
- TWO views minimum at 90°
- Include joint ABOVE and BELOW
- Complete ABCS for every image
- Don't stop after finding one injury
ATLS Imaging
- Primary survey: CXR + Pelvis X-ray
- CT pan-scan when stable
- Never clear C-spine on X-ray alone
- CT required for GCS less than 15
Commonly Missed (SCALP)
- Scaphoid: MRI/CT if X-ray negative
- C-spine: CT mandatory, not X-ray
- Ankle: Posterior malleolus, syndesmosis
- Lisfranc: Weight-bearing views essential
- Pelvis: Ring breaks twice - find both
CT Essentials
- Review sagittal AND coronal reconstructions
- 3D for complex fractures
- Bone AND soft tissue windows
- CT C-spine sensitivity greater than 99% vs 50% for X-ray
Evidence Base & Landmark Studies
The modern approach to trauma imaging is built on a small number of large, high-quality decision-rule studies and one landmark randomised trial of pan-scan. Knowing these by name, design and headline number is high-yield for vivas.
REACT-2: Immediate Total-Body CT vs Standard Work-Up (RCT)
- International multicentre RCT of 1403 severely injured adults randomised to immediate total-body CT versus conventional imaging with selective CT.
- In-hospital mortality was identical (16% vs 16%, p=0.92), with no benefit in the polytrauma or traumatic brain injury subgroups.
REACT-2: Cost-Effectiveness of Immediate Total-Body CT
- Economic analysis of 928 REACT-2 patients: overall hospital costs were similar between the two strategies.
- Immediate total-body CT had a high probability of being cost-effective specifically in multiple trauma (0.8 to 0.9) and traumatic brain injury (over 0.9).
Areas of Controversy & Uncertainty
- Pan-scan vs selective CT: REACT-2 showed no mortality benefit overall, yet pan-scan is widely used for speed and completeness. The debate centres on radiation stewardship and patient selection rather than diagnostic accuracy.
- Clearing the C-spine in the obtunded patient with a normal CT: Modern multidetector CT has very high sensitivity, and several groups now clear the collar on CT alone. Others still obtain MRI to exclude purely ligamentous injury. Practice varies and guidelines are not unanimous.
- Radiation in young patients: Cumulative dose from repeated CT (especially in children and young polytrauma survivors) drives an ALARA approach and increasing use of MRI and low-dose CT protocols.
- Whole-body MRI and dual-energy CT: Emerging roles for marrow oedema and bone-bruise detection without ionising radiation, but availability, time and cost limit acute use.