Fifth Metatarsal Apophysitis | Peroneus Brevis Traction | Lateral Foot Pain | Often Mistaken For a Fracture
- Traction apophysitis: Repetitive pull of the peroneus brevis on the apophysis at the base of the fifth metatarsal during the growth spurt - an overuse injury, not a joint problem
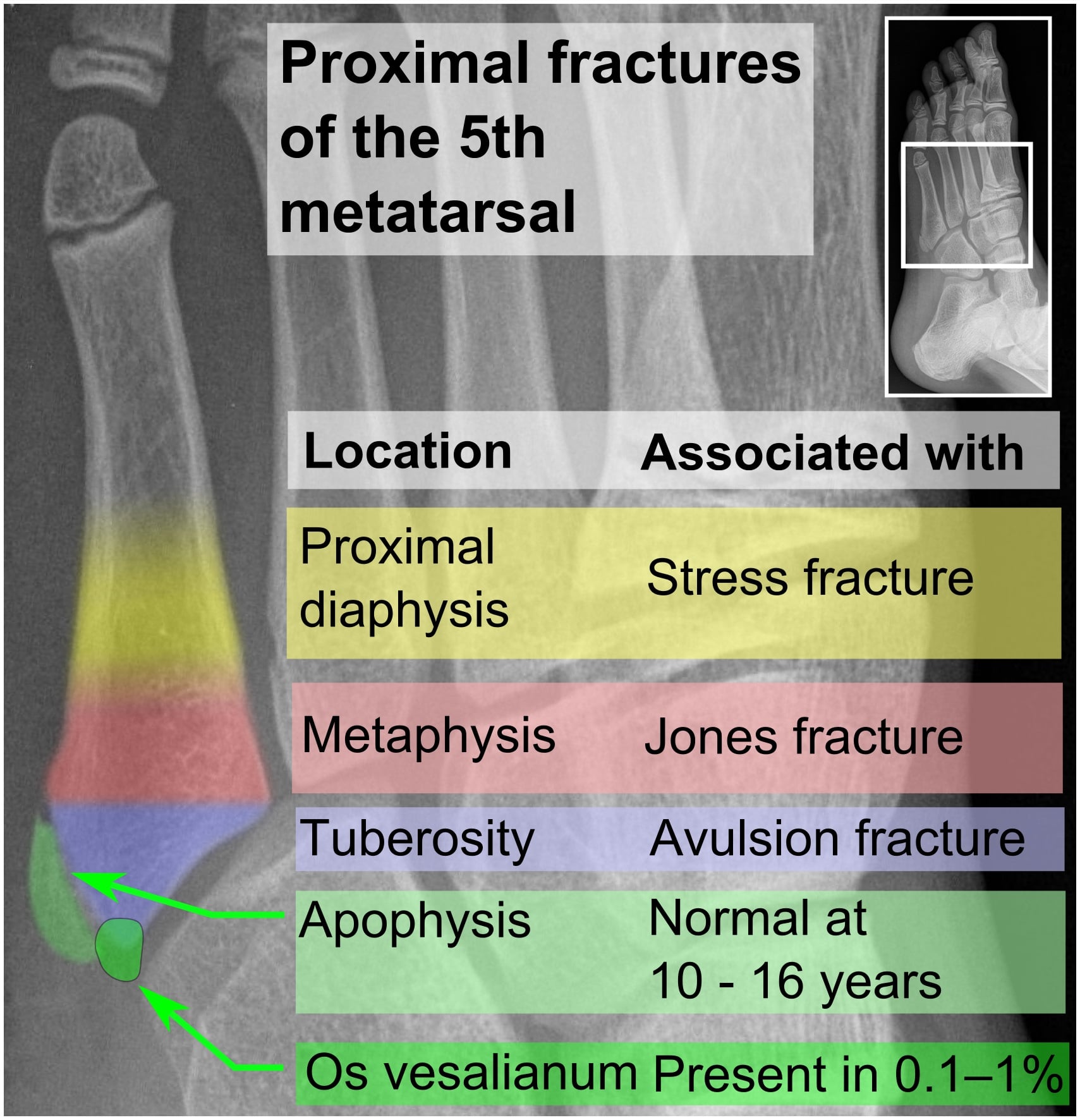
- The fracture trap: The normal apophysis lies roughly PARALLEL to the shaft; an avulsion fracture line runs roughly TRANSVERSE (perpendicular) to it - this orientation is the key to telling them apart
- Clinical diagnosis: Point tenderness and swelling over the base of the fifth metatarsal with activity-related lateral foot pain - imaging is used to exclude fracture, not to confirm apophysitis
- Self-limiting: Settles once the apophysis fuses around skeletal maturity; surgery has essentially no role
- Compare both feet: A symmetrical apophysis on the other foot reassures you the finding is a normal ossification centre, not a fracture
- “Rare but classic FRACS/FRCS exam trap - lateral foot pain in a child, X-ray shows a 'fragment' at the fifth metatarsal base
- “Apophysis parallel to shaft = normal; fracture line transverse to shaft = pathology
- “Peroneus brevis is the culprit tendon (NOT peroneus longus, which inserts on the first ray)
- “Manage like other apophysitides: load modification, stretching, reassurance; image to exclude a fracture
The single biggest pitfall in Iselin disease is misreading the apophysis as an acute fracture - or, just as dangerous, dismissing a genuine avulsion fracture as 'just the apophysis'. The normal apophysis at the base of the fifth metatarsal is a flake of bone that lies roughly parallel to the long axis of the shaft and is separated from it by a smooth, regular lucent line (the physis). A true fracture line typically runs transverse (perpendicular) to the shaft, has sharp non-corticated edges, and is usually accompanied by a clear injury mechanism. According to PubMed, a radiographic review of extremely proximal fifth metatarsal injuries in children found a fracture misdiagnosis rate of around 47%, almost entirely driven by the presence of the normal growth nucleus (DOI). When in doubt, image the other foot - a matching apophysis is reassuring.
Overview and Epidemiology
Iselin disease is a traction apophysitis of the base of the fifth metatarsal - an overuse injury of the secondary ossification centre (apophysis) at the proximal fifth metatarsal, caused by repetitive pull of the peroneus brevis tendon during the growth spurt. It was first described by Hans Iselin in 1912 and, like other apophysitides, is a benign and self-limiting condition of the growing skeleton rather than a true "disease". It is an uncommon but classically under-recognised cause of lateral foot pain in active children and adolescents.
According to PubMed, a systematic review concluded that the condition is "rarely reported and likely to remain undiagnosed, possibly mistaken for a fracture", and exists chiefly as an important differential in any child with fifth metatarsal pain (DOI).
Epidemiology:
- Uncommon and probably under-diagnosed; true incidence is unknown
- Peak age roughly 8 to 13 years, while the apophysis is open
- Tends to appear a little earlier in girls than boys, mirroring earlier skeletal maturation
- Strongly associated with running, jumping, kicking and pivoting sports - soccer, basketball, gymnastics, dance and martial arts
- A described trigger is repetitive lateral loading; according to PubMed, a paediatric case attributed to kickboxing was postulated to arise from traction during side-kicks and round-kicks (DOI)
The apophysis at the base of the fifth metatarsal is a secondary ossification centre onto which the peroneus brevis tendon attaches. During the adolescent growth spurt, bone lengthens faster than the muscle-tendon unit can adapt, so the peroneus brevis becomes relatively tight and applies greater traction across the still-cartilaginous apophyseal plate. Repetitive sport-related loading then produces microtrauma at this junction - the essence of a traction apophysitis, the same mechanism that underlies Sever and Osgood-Schlatter disease at other sites.
Etiology and Risk Factors:
- Open apophysis: Skeletal immaturity is the prerequisite
- Peroneus brevis / calf tightness: Increases traction across the apophysis
- Rapid growth: Bone outpaces the soft-tissue envelope
- Foot posture: Cavovarus or a supinated foot increases lateral column loading
- Reduced ankle/subtalar flexibility: A recurring theme across apophysitides
- High-impact, pivoting sport: Running, jumping, kicking, cutting
- Training load: Rapid increases in volume or intensity
- Hard surfaces and poor footwear: Increase peak lateral foot pressures
- Repetitive lateral loading: Side-kicks, sprinting on bends, dance turns
- Multiple concurrent sports: Inadequate recovery between sessions
Natural History:
- Symptoms wax and wane with activity over weeks to months
- Resolves spontaneously once the apophysis fuses (around skeletal maturity)
- No long-term structural sequelae, deformity or arthritis are described
- The clinician's job is accurate diagnosis, exclusion of a fracture, symptom control and reassurance
Pathophysiology and Anatomy
The Fifth Metatarsal Base and Its Apophysis
The base of the fifth metatarsal has a prominent lateral tuberosity (styloid process). A secondary ossification centre (the apophysis) develops here and is the attachment point of the peroneus brevis tendon. The plantar aponeurosis (lateral band) and the lateral band of the plantar fascia also contribute attachments to this region.
- Peroneus brevis - inserts onto the apophysis/tuberosity; everts and plantarflexes the foot. This is the tractioning structure in Iselin disease.
- Peroneus longus - passes plantar to the cuboid to insert on the first metatarsal/medial cuneiform; it does not insert on the fifth metatarsal base, so it is not the culprit (a classic exam point).
- Lateral cord of the plantar fascia - adds a further small tractioning force.
The cartilaginous physis between the apophysis and the metatarsal is the weak link during growth - directly analogous to the tibial tubercle in Osgood-Schlatter disease and the calcaneal apophysis in Sever disease.
- Approx. age (years)
- 0-7
- Description
- Apophysis not yet visible on radiograph
- Clinical Relevance
- Apophysitis does not occur; pain here needs another explanation
- Approx. age (years)
- 7-8
- Description
- Secondary ossification centre becomes radiographically visible as a thin fleck parallel to the shaft
- Clinical Relevance
- Start of the vulnerable period; the fleck is easily mistaken for a fracture
- Approx. age (years)
- 9-12
- Description
- Apophysis ossifying during the growth spurt with high sport load
- Clinical Relevance
- Peak incidence of Iselin disease
- Approx. age (years)
- 10-14+
- Description
- Apophysis fuses to the metatarsal (earlier in girls than boys)
- Clinical Relevance
- Symptoms resolve as fusion completes; persistence is rare
According to PubMed, a CT and radiographic study of an Australian paediatric population found that the fifth metatarsal apophysis begins ossifying as early as 7 years in girls and 8 years in boys, appearing first as a thin fleck of bone that elongates into a crescent. Fusion shows marked sexual dimorphism, commencing at a mean of about 10 years in girls and 12 years in boys (DOI). Knowing this developmental window helps you interpret whether a "fleck" at the base is a normal apophysis for that child's age.
Pathophysiology
Iselin disease is a repetitive microtrauma / overuse phenomenon, not a primary inflammatory or avascular process. Cyclical tensile loading from the peroneus brevis, combined with impact and lateral-column loading, produces microscopic injury and a reparative response at the cartilaginous apophyseal plate. Any radiographic widening, sclerosis or fragmentation reflects loaded ossification rather than a destructive process, which is why imaging changes are subtle and non-specific and why the diagnosis remains clinical.
Lateral foot pain in a child is easily labelled a "sprain", but the base of the fifth metatarsal in this age group hosts a vulnerable apophysis. Persistent, point-tender, activity-related pain at the styloid - especially with normal ankle ligaments - should raise Iselin disease, an avulsion fracture or a stress injury rather than a soft-tissue sprain. Treating it as a trivial sprain risks both missing a fracture and prolonging an apophysitis.
Classification and Severity
There is no universally adopted formal classification for Iselin disease; like other apophysitides it is graded pragmatically by symptom severity and functional impact, which directly guides how much load to remove.
Clinical Severity Grading
- Symptoms
- Lateral foot pain only after sport, settles with rest, no limp
- Impact on Activity
- Completes training and play
- Treatment Emphasis
- Peroneal/calf stretching, footwear advice, continue sport
- Symptoms
- Pain during and after sport, mild limp afterwards
- Impact on Activity
- Performance and participation affected
- Treatment Emphasis
- Reduce load, relative rest, formal physiotherapy
- Symptoms
- Pain on everyday walking, persistent limp, marked tenderness/swelling
- Impact on Activity
- Unable to play sport
- Treatment Emphasis
- Short immobilisation in a boot/cast for a few weeks, then graded return
Grading matters because it dictates how much loading to remove and for how long - not whether to operate (you essentially never do). Milder cases need only stretching and load awareness; more severe or refractory cases may benefit from a short period of immobilisation to break the cycle, followed by a graded return as tenderness settles. All grades share the same favourable endpoint at skeletal maturity.
Clinical Assessment
History:
- Age and growth: Peak 8-13 years, often during a growth spurt
- Sport: Type, frequency, recent increase in load, kicking/pivoting activities
- Pain pattern: Lateral foot, over the base of the fifth metatarsal, activity-related, eases with rest
- Mechanism: Gradual onset (apophysitis) versus an acute twist/inversion (fracture)
- Limp: Present after sport in moderate-to-severe cases
- Footwear: Stiff or poorly cushioned boots on hard surfaces
- Acute injury with sudden onset: Think avulsion or Jones fracture
- Night pain or rest pain: Tumour, infection
- Fever, systemic upset: Osteomyelitis, malignancy
- Marked swelling, warmth or true deformity: Atypical for apophysitis
- Failure to settle with appropriate care: Reconsider the diagnosis (stress injury, non-union)
Physical Examination:
Systematic Examination
- Gait, looking for an antalgic limp or weight-bearing on the medial border to offload the lateral foot
- Compare both feet; look for swelling or prominence at the fifth metatarsal base (often subtle)
- Assess foot posture (cavovarus increases lateral loading) and footwear
- Focal tenderness over the base of the fifth metatarsal / styloid is the hallmark finding
- Localised swelling may be present over the apophysis
- Palpate the lateral ligaments, cuboid and along the shaft to localise the pain and screen for fracture
- Resisted eversion (loads the peroneus brevis) reproduces pain at the apophysis
- Passive inversion / plantarflexion stretches the peroneus brevis and can reproduce pain
- Single-leg stance or hopping may reproduce lateral foot pain
- Ankle and subtalar motion: usually preserved; reduced flexibility of the peroneals/calf is common
- Clear the lateral ankle ligaments (this is not a simple sprain) and the rest of the foot
- Neurovascular check to complete the assessment
Because the peroneus brevis is the tractioning tendon, resisted eversion and passive stretch into inversion load the apophysis and reproduce the child's pain. Combined with focal tenderness at the styloid, the right age and an activity-related history, this functional sign points to Iselin disease - and reminds you it is peroneus brevis, not peroneus longus, that is responsible.
Investigations
Iselin disease is a clinical diagnosis. Investigations are used to exclude a fracture, not to confirm apophysitis.
- To exclude an avulsion (pseudo-Jones) or Jones fracture after an acute injury
- Oblique view best profiles the apophysis
- Comparison views of the contralateral foot are invaluable - a symmetrical apophysis reassures you the finding is normal
- To identify an os vesalianum (accessory bone) as an alternative explanation
- Normal radiographs but persistent, typical symptoms (MRI can confirm apophyseal oedema)
- Diagnostic uncertainty between apophysitis, stress injury and fracture
- Atypical features - night/rest pain, systemic upset, marked swelling
- Failure to respond to appropriate conservative care
- What It Shows
- Apophysis parallel to shaft; excludes transverse fracture line; identifies os vesalianum
- Role in Iselin Disease
- First line - to exclude a fracture and characterise the apophysis
- What It Shows
- Symmetrical apophysis on the asymptomatic side
- Role in Iselin Disease
- Very useful to confirm a normal ossification centre rather than a fracture
- What It Shows
- Bone marrow oedema in/around the apophysis; occult stress injury; soft-tissue detail
- Role in Iselin Disease
- When radiographs are normal but symptoms persist, or to resolve uncertainty
- What It Shows
- Raised in infection or inflammatory arthritis
- Role in Iselin Disease
- Only if infection or systemic illness is suspected
The most reliable discriminator on plain film is orientation: the normal apophysis lies roughly parallel to the long axis of the fifth metatarsal, with a smooth corticated margin, whereas an avulsion fracture line runs transverse (perpendicular) to the shaft with sharp, non-corticated edges. According to PubMed, MRI is especially valuable when radiographs are normal but the clinical picture fits, because it can demonstrate apophyseal oedema and avoid misdiagnosing a fracture (DOI).


Differential Diagnosis
- Distinguishing Features
- 8-13y, gradual activity-related styloid pain, tender base, resisted eversion painful, apophysis parallel to shaft
- Key Action
- Clinical diagnosis; image to exclude fracture; conservative care
- Distinguishing Features
- Acute inversion injury, transverse fracture line at the tuberosity, sharp edges
- Key Action
- Confirm on X-ray; usually conservative (boot/cast), good union
- Distinguishing Features
- Transverse fracture at the metaphyseal-diaphyseal junction, distal to the tuberosity
- Key Action
- Higher non-union risk; consider operative fixation in athletes
- Distinguishing Features
- Insidious lateral pain, periosteal reaction distal to the base
- Key Action
- Offload; watch for non-union; sometimes fixation
- Distinguishing Features
- Accessory bone proximal to the base within peroneus brevis; smooth corticated, may be bilateral
- Key Action
- Usually incidental; rarely symptomatic - differentiate from fracture/apophysis
- Distinguishing Features
- Inversion injury, ligamentous tenderness anterior to the malleolus, base usually non-tender
- Key Action
- Examine ligaments; treat as soft-tissue injury
- Distinguishing Features
- Lateral midfoot pain, cuboid tenderness, peroneal tendon signs
- Key Action
- Clinical; targeted physiotherapy
- Do not miss a fracture - an acute injury with a transverse fracture line at the tuberosity is an avulsion fracture, and one at the metaphyseal-diaphyseal junction is a Jones fracture (higher non-union risk, may need fixation in athletes). Neither is Iselin disease.
- Do not over-call apophysitis as a fracture - a gradual-onset, parallel, smooth-edged apophysis in a child of the right age is normal; comparison views of the other foot settle most arguments.
Management
Management is essentially conservative and built on load management, peroneal/calf flexibility, footwear advice and reassurance. Surgery has essentially no role, and corticosteroid injection is not used.
Stepwise Conservative Management
- Explain the benign, self-limiting natural history to child and parents
- Reduce, do not abolish, impact and pivoting sport - cut volume and intensity to a pain-tolerable level
- Substitute lower-impact cross-training (cycling, swimming) during flares
- Address footwear: a supportive, cushioned shoe; avoid hard, worn-out footwear
- Ice to the lateral foot after activity
- Simple analgesia / short-course NSAIDs for painful flares only
- Relative rest during severe flares
- Peroneal and gastrocnemius-soleus stretching to reduce traction across the apophysis
- Foot and ankle strengthening as tolerated, including the peroneals and intrinsic muscles
- Address cavovarus loading and proprioception where relevant
- Graded return-to-sport programme guided by symptoms and tenderness
- For severe pain or failure of simpler measures, a short period of immobilisation (walking boot or below-knee cast) for a few weeks can break the pain cycle
- According to PubMed, reported cases have settled with rest, NSAIDs and short-term restraint/immobilisation followed by graded return (DOI)
- Reassess and re-image if symptoms do not respond, to exclude a fracture or stress injury
Complications and Prognosis
- Excellent - self-limiting, resolves as the apophysis fuses around skeletal maturity
- No described long-term deformity, growth disturbance or arthritis
- Symptoms may fluctuate for weeks to months while the child is still growing and active
- The main "complication" is missed time from sport and family anxiety - both mitigated by reassurance
- Misdiagnosis as a fracture (or a fracture mislabelled as apophysis) - the central risk
- Deconditioning from unnecessary prolonged rest
- Overtreatment / overinvestigation of a benign condition
- Failure to reassess when symptoms do not follow the expected course (consider stress injury or non-union)
The most therapeutic intervention is accurate reassurance: this is a benign overuse condition of the growing fifth metatarsal base that does not cause lasting damage and reliably resolves with growth, provided a fracture and other mimics have been excluded.
Return to Sport and Graded Loading
The management sections repeatedly promise a "graded return to sport", but Iselin disease is load-driven and self-limiting, so return is criterion-based, not calendar-based - progression is dictated by resolving symptoms and tenderness rather than a fixed number of weeks. There is no trial-derived protocol for this rare condition; the framework below applies the same principles the topic already relies on (relative rest, offloading and staged reloading), which the broader apophysitis literature endorses.
- Pain-free walking and a resolved limp
- Non-tender styloid on direct palpation of the fifth metatarsal base
- Pain-free provocation - resisted eversion and passive inversion stretch no longer reproduce pain (the same manoeuvres used to make the diagnosis)
- Confident single-leg stance and pain-free hopping on the affected side
- Volume before intensity - restore training minutes and impact exposure first, then add sprinting, cutting and kicking (mirrors the prevention advice of progressing volume before intensity)
- Maintain fitness with low-impact cross-training (cycling, swimming) through the restricted phase to avoid deconditioning
- After a boot for a severe flare: protected weight-bearing to full weight-bearing to non-impact to impact to sport-specific drills
- Any recurrence of styloid pain or limp = step back a stage
The single most useful gate for return to play is pain-free resisted eversion - the same peroneus brevis loading manoeuvre used to diagnose the condition. If loading the peroneus brevis still reproduces styloid pain, the apophysis is not ready for sprinting, cutting or kicking. Because there is no evidence-based timeline for this rare condition, examiners want the principle: progress on symptoms and tenderness, reintroduce volume before intensity, and expect fluctuation until skeletal maturity rather than quoting a fixed number of weeks.
Bilaterality and the Limits of the Comparison View
The "compare both feet" rule appears throughout this topic as a key teaching point, so it is worth stating exactly what it does and does not answer. The fifth metatarsal apophysis is a normal, bilateral secondary ossification centre. According to PubMed, a radiographic review identified the growth nucleus in 115 children across 132 feet - present bilaterally in many of them - underscoring that it is an expected paired structure, not a unilateral finding (DOI).
- What a symmetrical apophysis DOES tell you: the finding on the symptomatic side is a normal ossification centre rather than an acute fracture. This is the reassurance the comparison view is meant to provide, because an avulsion fracture is almost always unilateral and asymmetrical.
- What it does NOT tell you: it does not exclude apophysitis. Because both the apophysis and the sporting loads are bilateral, Iselin disease can occur in both feet, so a perfectly symmetrical pair of apophyses can coexist with genuine bilateral symptoms.
In other words, contralateral films answer "is this a fracture or a normal apophysis?", not "is this child's pain apophysitis?". The diagnosis of apophysitis stays clinical - focal styloid tenderness, activity-related pain and painful resisted eversion - however symmetrical the bones look.
A matching apophysis on the asymptomatic foot confirms the bone is normal and argues strongly against a fracture, but it can sit alongside bilateral Iselin disease. Never let a reassuringly symmetrical radiograph talk you out of a clinical diagnosis of apophysitis when the history, focal tenderness and painful resisted eversion all fit - and remember to examine both feet clinically, not just radiographically.
Guidelines, Registries & Global Practice
Global epidemiology. Iselin disease is a worldwide condition of the skeletally immature, running and pivoting athlete and is consistently described as rare and under-recognised. There is no dedicated registry; knowledge comes from case reports, small series and a single systematic review rather than arthroplasty-style national registries. According to PubMed, contemporary anatomical data place the vulnerable window between the appearance of the apophysis (around 7-8 years) and its fusion (mean approximately 10 years in girls and 12 years in boys) (DOI).
Guideline landscape. No major society publishes an Iselin-specific guideline; recommendations are drawn from paediatric overuse-injury and apophysitis guidance, which is strikingly consistent across systems - the diagnosis is clinical and management is conservative, with imaging used to exclude a fracture.
- Position
- Activity modification, peroneal/calf stretching and strengthening; reassurance about the self-limiting course
- Imaging Stance
- Radiograph to exclude a fracture; comparison views useful; MRI if uncertain
- Evidence Basis
- Expert consensus and case-based evidence
- Position
- Primary-care conservative management, load modification, physiotherapy; referral for diagnostic uncertainty
- Imaging Stance
- Imaging mainly to exclude fracture after acute injury or atypical course
- Evidence Basis
- Narrative / consensus guidance
- Position
- Conservative care and family education; avoid mislabelling the normal apophysis
- Imaging Stance
- Selective imaging; emphasise contralateral comparison
- Evidence Basis
- Consensus / practice standards
- Position
- Load management, peroneal flexibility and graded return; flag prolonged or atypical courses
- Imaging Stance
- MRI selectively for normal radiographs with persistent symptoms
- Evidence Basis
- Case-based and anatomical evidence (Level 4-5)
- Position
- Training-load monitoring during growth spurts; gradual return-to-sport progression
- Imaging Stance
- Clinical diagnosis; image to exclude fracture
- Evidence Basis
- Consensus / sports guidance
The main international variation is the threshold for advanced imaging, not the core approach: management is uniformly conservative worldwide. Higher-resource and elite-sport settings reach for MRI sooner to confirm apophyseal oedema and exclude a stress injury, whereas primary-care systems keep the diagnosis clinical and rely on plain radiographs with contralateral comparison to exclude a fracture.
Medicolegal Considerations:
Key documentation points:
- History clarifying gradual overuse onset versus an acute injury
- Documentation of focal tenderness at the fifth metatarsal base and pain on resisted eversion
- Radiographic interpretation noting apophysis orientation (parallel) versus any fracture line (transverse)
- Use and documentation of contralateral comparison views where the diagnosis is uncertain
- Explicit statement that a fracture has been considered and excluded, with a plan for review if symptoms persist
Don't Miss the Fracture: Mislabelling an avulsion or Jones fracture as "Iselin disease" - or vice versa - is the recognised source of harm here. According to PubMed, misdiagnosis rates approaching 47% have been reported in proximal fifth metatarsal injuries in children (DOI). Document the orientation of any lucent line and the comparison views.
Prevention Strategies:
- Training-load management during growth spurts (progress volume before intensity)
- Peroneal and calf flexibility work and attention to footwear and lateral-column loading
- Awareness among coaches and parents that activity-related lateral foot pain in this age group warrants assessment rather than being dismissed as a sprain
Memory Aids
ISELINISELIN - Core Features
Hook:ISELIN = peroneus brevis pulling on a growing fifth metatarsal base in a young athlete - load it less, stretch it, reassure, and it settles.
LINEPARALLEL - Apophysis vs Fracture
Hook:Read the LINE: parallel and smooth is the apophysis; transverse and sharp is a fracture.
RESTREST - Conservative Management
Hook:REST the fifth metatarsal base - relative rest, peroneal exercise, settle flares, teach the family - and growth does the rest.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 12-year-old boy who plays a lot of football presents with a 4-week history of pain on the outer border of his right foot. The pain is worse during and after matches and he occasionally limps off. There was no specific injury. He is otherwise well.”
“A 13-year-old is brought to the emergency department after twisting her ankle playing netball. She has pain and swelling over the outer border of the foot. The radiograph shows a lucent line near the base of the fifth metatarsal, and the on-call doctor is unsure whether this is Iselin disease or a fracture.”
“An 11-year-old competitive dancer has clinically confirmed Iselin disease. Despite peroneal and calf stretching and activity advice over 6 weeks she still has limiting lateral foot pain and is missing classes. Her parents ask whether she needs surgery.”
Key Anatomy
- Apophysis = secondary ossification centre at the base of the fifth metatarsal
- Peroneus brevis inserts here and provides the traction (NOT peroneus longus)
- Cartilaginous physis is the weak link during growth
- Apophysis lies roughly PARALLEL to the shaft
Diagnosis
- Clinical diagnosis - focal styloid tenderness, activity-related lateral foot pain
- Pain on resisted eversion and passive inversion (loads peroneus brevis)
- Age 8-13 years, gradual overuse onset, often a young athlete
- Image to EXCLUDE a fracture; comparison views of the other foot
Apophysis vs Fracture
- Apophysis = PARALLEL to shaft, smooth corticated edge
- Fracture = TRANSVERSE to shaft, sharp non-corticated edge
- Avulsion fracture at tuberosity; Jones fracture more distal
- Comparison views resolve most cases; MRI if still unclear
Treatment
- Load MODIFICATION, not complete rest
- Peroneal and calf stretching and strengthening
- Ice and short-course NSAIDs for flares
- Short boot/cast immobilisation for severe or refractory cases
- No surgery, no injection
Differentials (NOT Iselin)
- Avulsion (pseudo-Jones) fracture - acute, transverse at tuberosity
- Jones fracture - metaphyseal-diaphyseal, higher non-union risk
- Proximal diaphyseal stress fracture
- Os vesalianum accessory bone; lateral ankle sprain
Prognosis
- Excellent - self-limiting with skeletal maturity
- No long-term deformity or arthritis
- Symptoms may fluctuate for weeks to months while growing
- Reassurance is a key part of treatment
Evidence Base
Iselin disease is rare, so the literature is dominated by case reports, small series and a single systematic review, supplemented by anatomical and imaging studies of the apophysis. Each card below is verified against PubMed. Some management principles are shared with the broader paediatric apophysitis literature and labelled where relevant.
Iselin's Disease: A Systematic Review
- Systematic review of the available published data on Iselin's disease, a traction apophysitis of the fifth metatarsal base
- Predominantly affects adolescents, especially those in regular sporting activity
- Rarely reported and likely to remain undiagnosed, with frequent confusion with a fracture
- Investigation, treatment and outcomes are summarised to support diagnosis and management
Apophysitis and Osteochondrosis: Common Causes of Pain in Growing Bones
- Narrative review of apophysitis and osteochondrosis across the growing skeleton
- Lists Iselin disease (base of the fifth metatarsal) among the recognised apophysitides alongside Sever, Osgood-Schlatter and Sinding-Larsen-Johansson
- Apophysitis is an overuse traction injury, typically with tight or inflexible muscle-tendon units
- Treatment includes stretching, relative rest, offloading, icing and limited NSAID use; surgery is rarely needed